
Radiation Dose-Induced Carotid Artery Stenosis and Brain Necrosis in Head and Neck Cancer—A Real World Cohort Study

Abstract
Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Data Source and Study Design
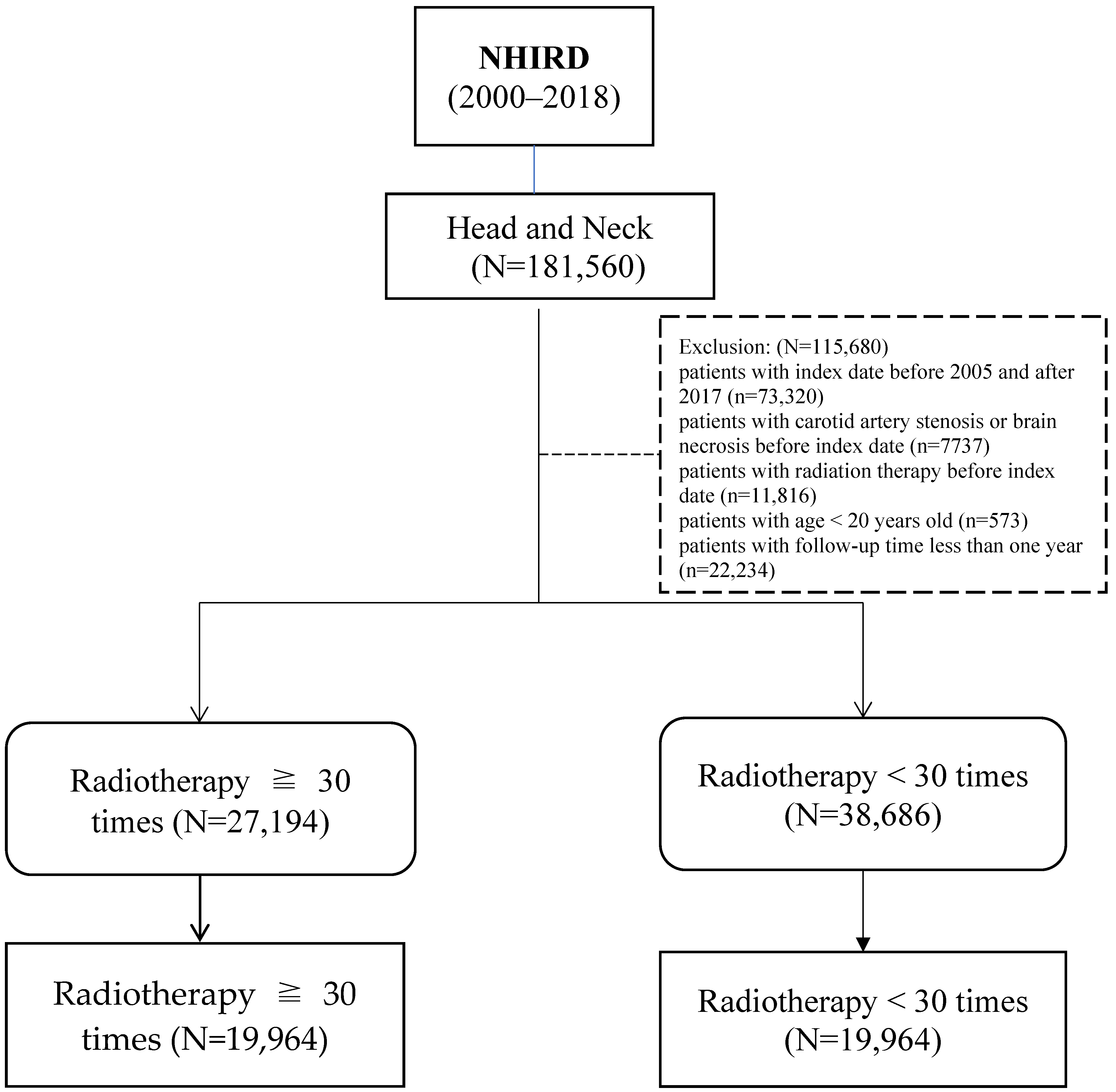
2.2. Study Population
2.3. Main Outcome and Potential Confounding Factors
2.4. Statistical Analysis
2.5. Sensitivity Analyses
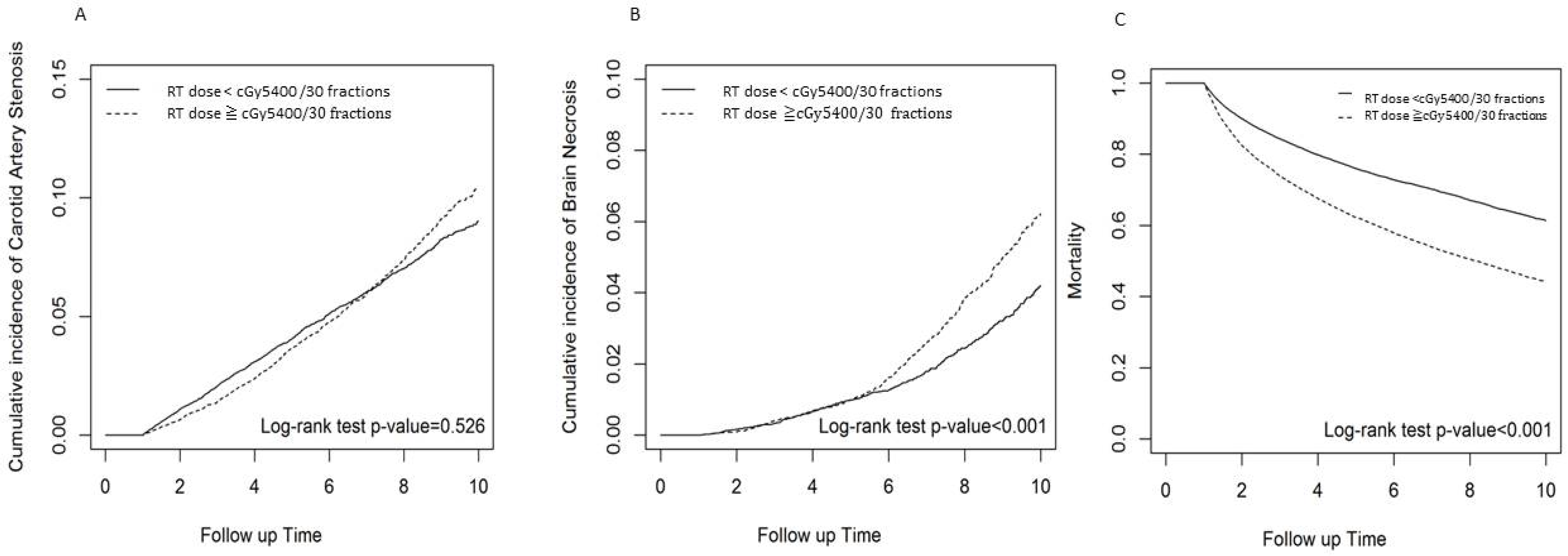
3. Results
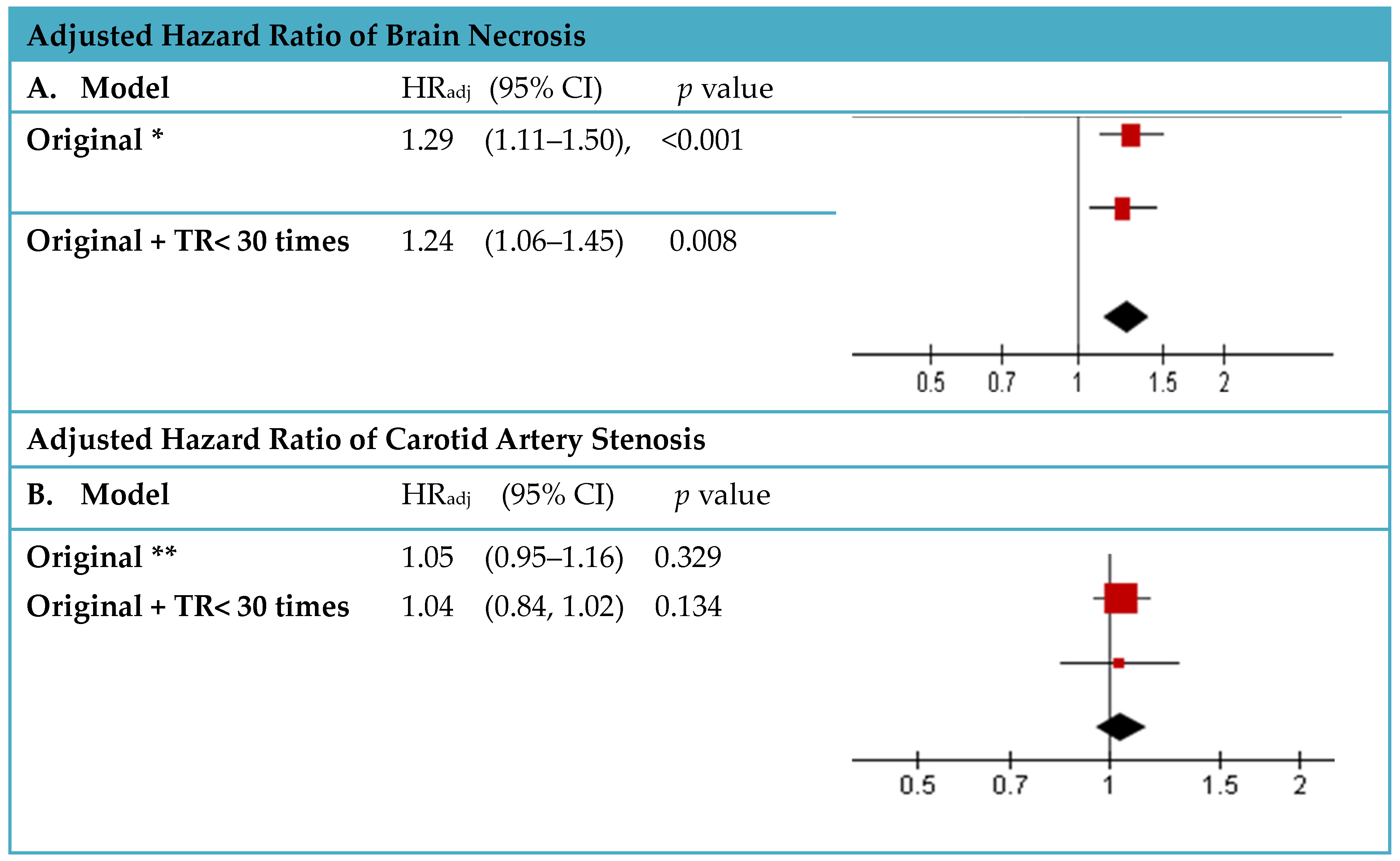
4. Sensitivity Analysis
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| RT | Radiation therapy |
| HNC | Head and neck cancer |
| CAS | Carotid artery stenosis |
| RIBN | Radiation-induced brain necrosis |
| HR | Hazard ratio |
| CI | Confidence interval |
References
- Global Cancer Observatory; International Agency for Research on Cancer; World Health Organization. Available online: https://gco.iarc.fr/today/home (accessed on 20 December 2023).
- Taiwan Cancer Registry Center. 2020. Available online: https://twcr.tw/?page_id=1855&lang=en (accessed on 23 June 2023).
- Vigneswaran, N.; Williams, M.D. Epidemiologic trends in head and neck cancer and aids in diagnosis. Oral. Maxillofac Surg. Clin. N. Am. 2014, 26, 123–141. [Google Scholar] [CrossRef]
- Chi, A.C.; Day, T.A.; Neville, B.W. Oral cavity and oropharyngeal squamous cell carcinoma—An update. CA Cancer J. Clin. 2015, 65, 401–421. [Google Scholar] [CrossRef]
- Alfouzan, A.F. Radiation therapy in head and neck cancer. Saudi Med. J. 2021, 42, 247–254. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network. Head and Neck Cancers (Version 3.2021). 2021. Available online: https://www.nccn.org/professionals/physician_gls/pdf/head-and-neck.pdf (accessed on 1 December 2022).
- Arboleda, L.P.A.; de Carvalho, G.B.; Santos-Silva, A.R.; Fernandes, G.A.; Vartanian, J.G.; Conway, D.I.; Virani, S.; Brennan, P.; Kowalski, L.P.; Curado, M.P. Squamous Cell Carcinoma of the Oral Cavity, Oropharynx, and Larynx: A Scoping Review of Treatment Guidelines Worldwide. Cancers 2023, 15, 4405. [Google Scholar] [CrossRef] [PubMed]
- Anderson, G.; Ebadi, M.; Vo, K.; Novak, J.; Govindarajan, A.; Amini, A. An Updated Review on Head and Neck Cancer Treatment with Radiation Therapy. Cancers 2021, 13, 4912. [Google Scholar] [CrossRef] [PubMed]
- Barton, M.B.; Jacob, S.; Shafiq, J.; Wong, K.; Thompson, S.R.; Hanna, T.P.; Delaney, G.P. Estimating the demand for radiotherapy from the evidence: A review of changes from 2003 to 2012. Radiother. Oncol. 2014, 112, 140–144. [Google Scholar] [CrossRef]
- Saloura, V.; Langerman, A.; Rudra, S.; Chin, R.; Cohen, E.E.W. Multidisciplinary care of the patient with head and neck cancer. Surg. Oncol. Clin. N. Am. 2013, 22, 179–215. [Google Scholar] [CrossRef] [PubMed]
- van der Molen, L.; van Rossum, M.A.; Burkhead, L.M.; Smeele, L.E.; Hilgers, F.J.M. Functional outcomes and rehabilitation strategies in patients treated with chemoradiotherapy for advanced head and neck cancer: A systematic review. Eur. Arch. Otorhinolaryngol. 2009, 266, 889–900. [Google Scholar] [CrossRef]
- Kuo, D.-Y.; Wu, Y.-W.; Hsieh, C.-H.; Liao, L.-J.; Shueng, P.-W. Application of Carotid Duplex Ultrasonography in the Surveillance of Carotid Artery Stenosis after Neck Irradiation. Rev. Cardiovasc. Med. 2022, 23, 240. [Google Scholar] [CrossRef]
- Yao, C.-Y.; Zhou, G.-R.; Wang, L.-J.; Xu, J.-H.; Ye, J.-J.; Zhang, L.-F.; He, X.; Chen, Z.-Z.; Huang, S.-F. A retrospective dosimetry study of intensity-modulated radiotherapy for nasopharyngeal carcinoma: Radiation-induced brainstem injury and dose-volume analysis. Radiat. Oncol. 2018, 13, 194. [Google Scholar] [CrossRef]
- Huang, X.-D.; Li, Y.-C.; Chen, F.-P.; Zheng, W.-H.; Zhou, G.-Q.; Lin, L.; Hu, J.; He, W.-J.; Zhang, L.-L.; Kou, J.; et al. Evolution and Dosimetric Analysis of Magnetic Resonance Imaging-Detected Brain Stem Injury After Intensity Modulated Radiation Therapy in Nasopharyngeal Carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2019, 105, 124–131. [Google Scholar] [CrossRef]
- Fan, X.; Huang, Y.; Xu, P.; Min, Y.; Li, J.; Feng, M.; Xu, G.-H.; Lang, J. Dosimetric analysis of radiation-induced brainstem necrosis for nasopharyngeal carcinoma treated with IMRT. BMC Cancer 2022, 22, 178. [Google Scholar] [CrossRef] [PubMed]
- Wu, V.W.C.; Tam, S.Y. Radiation induced temporal lobe necrosis in nasopharyngeal cancer patients after radical external beam radiotherapy. Radiat. Oncol. 2020, 15, 112. [Google Scholar] [CrossRef]
- Zhou, X.; Liu, P.; Wang, X. Temporal Lobe Necrosis Following Radiotherapy in Nasopharyngeal Carcinoma: New Insight into the Management. Front. Oncol. 2021, 10, 593487. [Google Scholar] [CrossRef]
- Registry for Catastrophic Illness Patients (HV), National Health Insurance Database. Available online: https://nhird.nhri.edu.tw/en/Data_Files.html (accessed on 20 December 2023).
- Steele, S.R.; Martin, M.J.; Mullenix, P.S.; Crawford, J.V.; Cuadrado, D.S.; Andersen, C.A. Focused high-risk population screening for carotid arterial stenosis after radiation therapy for head and neck cancer. Am. J. Surg. 2004, 187, 594–598. [Google Scholar] [CrossRef]
- Nieder, C.; Grant, D.M. Considerations regarding carotid artery dose in radiotherapy of the cervical spine. Clin. Transl. Radiat. Oncol. 2022, 38, 77–80. [Google Scholar] [CrossRef] [PubMed]
- Pfister, D.G.; Spencer, S.; Adelstein, D.; Adkins, D.; Anzai, Y.; Brizel, D.M.; Bruce, J.Y.; Busse, P.M.; Caudell, J.J.; Cmelak, A.J.; et al. Head and Neck Cancers, Version 2.2020, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc. Netw. 2020, 18, 873–898. [Google Scholar] [CrossRef]
- Taiwan Cancer Registration Database. Available online: https://cris.hpa.gov.tw/EngPages/home (accessed on 16 August 2024).
- Biologically Effective Dose (BED) and Equivalent Dose (EQD2) Calculators. Available online: https://www.eviq.org.au/clinical-resources/eviq-calculators/3197-biologically-effective-dose-bed-and-equival (accessed on 8 August 2024).
- Cheng, S.W.; Wu, L.L.; Ting, A.C.; Lau, H.; Lam, L.K.; Wei, W.I. Irradiation-induced extracranial carotid stenosis in patients with head and neck malignancies. Am. J. Surg. 1999, 178, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, D.J.; Mowery, Y.M.; Broadwater, G.; Rodrigues, A.; Wisdom, A.J.; Dorth, J.A.; Patel, P.R.; Shortell, C.K.; Clough, R.; Brizel, D.M. The risk of carotid stenosis in head and neck cancer patients after radiation therapy. Oral Oncol. 2018, 80, 9–15. [Google Scholar] [CrossRef]
- Lin, D.; Lapen, K.; Sherer, M.V.; Kantor, J.; Zhang, Z.; Boyce, L.M.; Bosch, W.; Korenstein, D.; Gillespie, E.F. A Systematic Review of Contouring Guidelines in Radiation Oncology: Analysis of Frequency, Methodology, and Delivery of Consensus Recommendations. Int. J. Radiat. Oncol. Biol. Phys. 2020, 107, 827–835. [Google Scholar] [CrossRef]
- Marks, L.B.; Yorke, E.D.; Jackson, A.; Ten Haken, R.K.; Constine, L.S.; Eisbruch, A.; Bentzen, S.M.; Nam, J.; Deasy, J.O. Use of normal tissue complication probability models in the clinic. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76 (Suppl. 3), S10–S19. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Ren, H.; Fu, J. Treatment of Radiation-Induced Brain Necrosis. Oxid. Med. Cell Longev. 2021, 2021, 4793517. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.H.; Chang, J.T.; Lee, T.H.; Chang, P.Y.; Chang, C.H.; Wu, H.C.; Chang, T.Y.; Huang, K.L.; Lin, C.Y.; Fan, K.H.; et al. Total plaque score helps to determine follow-up strategy for carotid artery stenosis progression in head and neck cancer patients after radiation therapy. PLoS ONE 2021, 16, e0246684. [Google Scholar] [CrossRef] [PubMed]
- Bentzen, S.M.; Constine, L.S.; Deasy, J.O.; Eisbruch, A.; Jackson, A.; Marks, L.B.; Ten Haken, R.K.; Yorke, E.D. Quantitative analyses of normal tissue effects in the clinic (QUANTEC): An introduction to the scientific issues. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, S3–S9. [Google Scholar] [CrossRef]
- Fionda, B.; Bussu, F.; Placidi, E.; Rosa, E.; Lancellotta, V.; Parrilla, C.; Zinicola, T.; De Angeli, M.; Greco, F.; Rigante, M.; et al. Interventional Radiotherapy (Brachytherapy) for Nasal Vestibule: Novel Strategies to Prevent Side Effects. J. Clin. Med. 2023, 12, 6154. [Google Scholar] [CrossRef]
- Van den Bosch, L.; van der Schaaf, A.; van der Laan, H.P.; Hoebers, F.; Wijers, O.; van den Hoek, J.G.; Moons, K.; Reitsma, J.; Steenbakkers, R.; Schuit, E.; et al. Comprehensive toxicity risk profiling in radiation therapy for head and neck cancer: A new concept for individually optimised treatment. Radiother. Oncol. 2021, 157, 147–154. [Google Scholar] [CrossRef]
- Majeed, H.; Gupta, V. Adverse Effects of Radiation Therapy. 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK563259/ (accessed on 10 August 2023).

{kind=link}
{kind=link}
{kind=link}
| Radiotherapy | * Dose < 30 Fractions | * Dose ≥ 30 Fractions | |||
|---|---|---|---|---|---|
| N = 19,964 | N = 19,964 | ||||
| Variables | n | % | n | % | p-Value |
| Gender | 0.562 | ||||
| female | 2943 | 14.74 | 2902 | 14.54 | |
| male | 17,021 | 85.26 | 17,062 | 85.46 | |
| Age, years | 0.756 | ||||
| 20–59 | 13,524 | 67.74 | 13,495 | 67.60 | |
| 60+ | 6440 | 32.26 | 6469 | 32.40 | |
| Mean, (SD) | 54.86 | (11.46) | 54.89 | (11.43) | 0.782 |
| Primary site specified | <0.001 | ||||
| Oropharynx | 108 | 0.54 | 280 | 1.40 | |
| Nasopharyngeal | 1144 | 5.73 | 3494 | 17.50 | |
| Hypopharynx | 257 | 1.29 | 891 | 4.46 | |
| Larynx | 188 | 0.94 | 351 | 1.76 | |
| Oral cavity | 7 | 0.04 | 18 | 0.09 | |
| Sinus/Nasal cavity | 29 | 0.15 | 69 | 0.35 | |
| Parotid | 191 | 0.96 | 196 | 0.98 | |
| Submandibular | 71 | 0.36 | 78 | 0.39 | |
| Primary site unspecified | 17,969 | 90.01 | 14,587 | 73.07 | |
| Comorbidities | |||||
| Hyperlipidemia | 5733 | 28.72 | 5696 | 28.53 | 0.682 |
| Cerebrovascular events | 176 | 0.88 | 200 | 1.00 | 0.214 |
| Hypertension | 7839 | 39.27 | 7793 | 39.04 | 0.637 |
| Coronary artery disease | 3172 | 15.89 | 3132 | 15.69 | 0.583 |
| Atrial Fibrillation | 211 | 1.06 | 236 | 1.18 | 0.234 |
| Myocardial infarction | 367 | 1.84 | 346 | 1.73 | 0.427 |
| Peripheral artery disease | 265 | 1.33 | 294 | 1.47 | 0.217 |
| Smoking | 868 | 4.35 | 865 | 4.33 | 0.941 |
| Charlson comorbidity index, CCI | 0.136 | ||||
| 0–2 | 13,821 | 69.23 | 13,958 | 69.92 | |
| 3+ | 6143 | 30.77 | 6006 | 30.08 | |
| Tumor Grade | <0.001 | ||||
| 1 | 3036 | 15.21 | 1727 | 8.65 | |
| 2 | 4398 | 22.03 | 5594 | 28.02 | |
| 3 | 808 | 4.05 | 1847 | 9.25 | |
| 4 | 834 | 4.18 | 2453 | 12.29 | |
| X | 10,888 | 54.54 | 8343 | 41.79 | |
| Carotid Artery Stenosis | ||||||
|---|---|---|---|---|---|---|
| Variable | N | PY | IR | aHR | (95% CI) | p-Value |
| Radiotherapy dose | ||||||
| <cGy 5400/30 fractions | 965 | 112,077.72 | 8.61 | 1.00 | (reference) | - |
| ≥cGy 5400/30 fractions | 863 | 100,648.57 | 8.57 | 1.05 | (0.95, 1.16) | 0.329 |
| female | 250 | 35,636.74 | 7.02 | 1.00 | (reference) | - |
| male | 1578 | 177,089.55 | 8.91 | 1.44 | (1.26, 1.65) | <0.001 |
| 20–59 | 950 | 147,311.82 | 6.45 | 1.00 | (reference) | - |
| 60+ | 878 | 65,414.46 | 13.42 | 1.66 | (1.51, 1.83) | <0.001 |
| Mean, (SD) | 1.03 | (1.03, 1.04) | <0.001 | |||
| Primary site | ||||||
| Oropharynx | 13 | 1525.20 | 8.52 | 1.00 | (reference) | - |
| Nasopharyngeal | 181 | 22,256.50 | 8.13 | 1.05 | (0.58, 1.90) | 0.862 |
| Hypopharynx | 37 | 4449.10 | 8.32 | 0.94 | (0.50, 1.76) | 0.836 |
| Larynx | 13 | 1934.67 | 6.72 | 0.67 | (0.31, 1.44) | 0.299 |
| Oral cavity | 8 | 3047.80 | 2.62 | 0.32 | (0.13, 0.78) | 0.012 |
| Other | 1576 | 179,513.01 | 8.78 | 0.85 | (0.49, 1.47) | 0.561 |
| Comorbidities | ||||||
| Hyperlipidemia | 694 | 58,765.59 | 11.81 | 1.17 | (1.06, 1.30) | 0.002 |
| Cerebrovascular events | 35 | 1887.18 | 18.55 | 1.37 | (0.98, 1.92) | 0.065 |
| Hypertension | 1035 | 78,685.54 | 13.15 | 1.71 | (1.55, 1.90) | <0.001 |
| Coronary artery disease | 456 | 32,478.67 | 14.04 | 1.12 | (0.99, 1.26) | 0.070 |
| Atrial fibrillation | 35 | 1952.30 | 17.93 | 1.26 | (0.90, 1.78) | 0.177 |
| Myocardial infarction | 26 | 2589.32 | 10.04 | 0.80 | (0.53, 1.18) | 0.260 |
| Peripheral artery disease | 35 | 2717.43 | 12.88 | 1.10 | (0.79, 1.54) | 0.574 |
| Smoking | 56 | 7481.59 | 7.49 | 0.97 | (0.74, 1.27) | 0.838 |
| Charlson comorbidity index | ||||||
| 0–2 | 1251 | 157,356.67 | 7.95 | 1.00 | (reference) | - |
| 3+ | 577 | 55,369.61 | 10.42 | 1.09 | (0.99, 1.21) | 0.088 |
| Tumor Grade | ||||||
| 1 | 144 | 24,243.78 | 5.94 | 1.00 | (reference) | - |
| 2 | 298 | 47,113.45 | 6.33 | 1.08 | (0.88, 1.32) | 0.450 |
| 3 | 88 | 12,068.65 | 7.29 | 1.20 | (0.92, 1.58) | 0.179 |
| 4 | 121 | 15,524.15 | 7.79 | 1.36 | (0.98, 1.88) | 0.063 |
| X | 1177 | 113,776.25 | 10.34 | 1.60 | (1.34, 1.91) | <0.001 |
| Brain Necrosis | ||||||
| Variable | N | PY | IR | aHR | (95% CI) | p-Value |
| Radiotherapy dose | ||||||
| <cGy 5400/30 fractions | 359 | 114,571.10 | 3.13 | 1.00 | (reference) | - |
| ≥cGy 5400/30 fractions | 435 | 102,141.31 | 4.26 | 1.29 | (1.11, 1.5) | <0.001 |
| Sex | ||||||
| female | 124 | 36,211.08 | 3.42 | 1.00 | (reference) | - |
| male | 670 | 180,501.34 | 3.71 | 1.28 | (1.06, 1.56) | 0.012 |
| Age, years | ||||||
| 20–59 | 503 | 149,255.57 | 3.37 | 1.00 | (reference) | - |
| 60+ | 291 | 67,456.84 | 4.31 | 1.16 | (0.99, 1.35) | 0.067 |
| Mean, (SD) | 1.01 | (1.01, 1.02) | <0.001 | |||
| Primary site specified | ||||||
| Oropharynx | 7 | 1545.29 | 4.53 | 1.00 | (reference) | - |
| Nasopharyngeal | 111 | 22,413.71 | 4.95 | 0.88 | (0.39, 2.00) | 0.760 |
| Hypopharynx | 18 | 4470.40 | 4.03 | 0.83 | (0.35, 1.99) | 0.679 |
| Larynx | 6 | 1948.32 | 3.08 | 0.73 | (0.24, 2.17) | 0.565 |
| Oral cavity + Sinus/Nasal cavity + Parotid + Submandibular | 10 | 3051.79 | 3.28 | 0.77 | (0.29, 2.02) | 0.591 |
| Primary site unspecified | 642 | 183,282.91 | 3.50 | 0.56 | (0.26, 1.18) | 0.124 |
| Comorbidities | ||||||
| Diabetes | 280 | 60,331.79 | 4.56 | 1.16 | (1.01, 1.37) | 0.040 |
| Hyperlipidemia | 281 | 60,341.79 | 4.66 | 1.18 | (1.01, 1.39) | 0.041 |
| Cerebrovascular events | 9 | 1968.25 | 4.57 | 0.93 | (0.48, 1.79) | 0.822 |
| Hypertension | 395 | 81,100.88 | 4.87 | 1.60 | (1.37, 1.88) | <0.001 |
| Coronary artery disease | 156 | 33,592.77 | 4.64 | 0.94 | (0.77, 1.14) | 0.519 |
| Atrial fibrillation | 16 | 2013.67 | 7.95 | 1.89 | (1.14, 3.14) | 0.014 |
| Myocardial infarction | 10 | 2635.58 | 3.79 | 1.01 | (0.53, 1.92) | 0.984 |
| Peripheral artery disease | 14 | 2793.47 | 5.01 | 1.23 | (0.72, 2.09) | 0.451 |
| Smoking | 32 | 7541.60 | 4.24 | 1.47 | (1.03, 2.11) | 0.033 |
| Charlson comorbidity index, CCI | ||||||
| 0–2 | 570 | 160,208.35 | 3.56 | 1.00 | (reference) | - |
| 3+ | 224 | 56,504.06 | 3.96 | 1.17 | (0.99, 1.37) | 0.064 |
| Tumor Grade | ||||||
| 1 | 66 | 24,566.41 | 2.69 | 1.00 | (reference) | - |
| 2 | 157 | 47,527.17 | 3.30 | 1.20 | (0.90, 1.61) | 0.215 |
| 3 | 30 | 12,242.17 | 2.45 | 0.81 | (0.52, 1.26) | 0.343 |
| 4 | 88 | 15,598.74 | 5.64 | 1.76 | (1.12, 2.78) | 0.015 |
| X | 453 | 116,777.93 | 3.88 | 1.08 | (0.83, 1.40) | 0.563 |
| Carotid Artery Stenosis | |||||
|---|---|---|---|---|---|
| Radiotherapy Dose | <cGY5400/30 Fractions | ≥cGY5400/30 Fractions | |||
| Variables | N | N | aHR | (95% CI) | p-Value |
| Sex | |||||
| female | 153 | 97 | 0.70 | (0.54, 0.9) | 0.006 |
| male | 812 | 766 | 1.10 | (1.00, 1.22) | 0.054 |
| Age, years | |||||
| 20–59 | 474 | 476 | 1.17 | (1.03, 1.33) | 0.015 |
| 60+ | 491 | 387 | 0.89 | (0.78, 1.02) | 0.095 |
| Primary site specified | |||||
| Oropharynx + Oral cavity + Sinus/Nasal cavity + Parotid + Submandibular | 5 | 16 | 1.40 | (0.50, 3.91) | 0.516 |
| Nasopharyngeal | 39 | 142 | 0.70 | (0.48, 1.00) | 0.050 |
| Hypopharynx | 6 | 31 | 1.22 | (0.51, 2.92) | 0.663 |
| Larynx | 5 | 8 | 0.73 | (0.24, 2.24) | 0.581 |
| Primary site unspecified | 910 | 666 | 1.03 | (0.94, 1.14) | 0.502 |
| Comorbidities | |||||
| Diabetes | 358 | 334 | 1.08 | (0.91, 1.23) | 0.366 |
| Hyperlipidemia | 359 | 335 | 1.04 | (0.90, 1.21) | 0.608 |
| Cerebrovascular events | 19 | 16 | 0.82 | (0.42, 1.59) | 0.552 |
| Hypertension | 556 | 479 | 0.98 | (0.87, 1.11) | 0.754 |
| Coronary artery disease | 259 | 197 | 0.84 | (0.70, 1.01) | 0.066 |
| Atrial fibrillation | 14 | 21 | 1.51 | (0.77, 2.97) | 0.234 |
| Myocardial infarction | 18 | 8 | 0.53 | (0.23, 1.23) | 0.140 |
| Peripheral artery disease | 23 | 12 | 0.52 | (0.26, 1.04) | 0.066 |
| Smoking | 23 | 33 | 1.54 | (0.90, 2.65) | 0.113 |
| Charlson comorbidity index, CCI | |||||
| 0–2 | 651 | 600 | 1.05 | (0.94, 1.18) | 0.364 |
| 3+ | 314 | 263 | 0.99 | (0.84, 1.17) | 0.925 |
| Tumor Grade | |||||
| 1 | 75 | 69 | 1.52 | (1.10, 2.11) | 0.012 |
| 2 | 110 | 188 | 1.29 | (1.02, 1.63) | 0.035 |
| 3 | 26 | 62 | 0.96 | (0.61, 1.52) | 0.853 |
| 4 | 28 | 93 | 0.71 | (0.46, 1.09) | 0.117 |
| X | 726 | 451 | 0.99 | (0.88, 1.12) | 0.900 |
| Follow-up time | |||||
| <6 years | 707 | 558 | 0.89 | (0.79, 1.00) | 0.051 |
| 6+ years | 258 | 305 | 1.48 | (1.24, 1.76) | <0.001 |
| Brain Necrosis | |||||
| Variables | N | N | aHR | (95% CI) | p-Value |
| Sex | |||||
| female | 57 | 67 | 1.33 | (0.94, 1.90) | 0.112 |
| male | 302 | 368 | 1.5 | (1.29, 1.75) | <0.001 |
| Age, years | |||||
| 20–59 | 210 | 293 | 1.69 | (1.42, 2.02) | <0.001 |
| 60+ | 149 | 142 | 1.15 | (0.91, 1.44) | 0.244 |
| Primary site specified | |||||
| Oropharynx + Larynx + Oral cavity + Sinus/Nasal cavity + Parotid + Submandibular | 3 | 20 | 2.94 | (0.87, 9.94) | 0.083 |
| Nasopharyngeal | 19 | 92 | 0.85 | (0.52, 1.41) | 0.532 |
| Hypopharynx | 3 | 15 | 1.22 | (0.35, 4.24) | 0.751 |
| Primary site unspecified | 334 | 308 | 1.33 | (1.14, 1.55) | <0.001 |
| Comorbidities | |||||
| Diabetes | 130 | 148 | 1.17 | (0.90, 1.50) | 0.206 |
| Hyperlipidemia | 131 | 150 | 1.35 | (1.06, 1.7) | 0.013 |
| Cerebrovascular events | 4 | 5 | 1.46 | (0.39, 5.46) | 0.577 |
| Hypertension | 190 | 205 | 1.29 | (1.06, 1.57) | 0.012 |
| Coronary artery disease | 81 | 75 | 1.09 | (0.79, 1.49) | 0.608 |
| Atrial fibrillation | 13 | 3 | 0.22 | (0.06, 0.78) | 0.019 |
| Myocardial infarction | 5 | 5 | 1.29 | (0.36, 4.62) | 0.700 |
| Peripheral artery disease | 6 | 8 | 1.83 | (0.63, 5.35) | 0.270 |
| Smoking | 15 | 17 | 1.41 | (0.70, 2.84) | 0.335 |
| Charlson comorbidity index, CCI | |||||
| 0–2 | 248 | 322 | 1.57 | (1.33, 1.85) | <0.001 |
| 3+ | 111 | 113 | 1.25 | (0.96, 1.63) | 0.092 |
| Tumor Grade | |||||
| 1 | 31 | 35 | 1.72 | (1.06, 2.80) | 0.028 |
| 2 | 54 | 103 | 1.46 | (1.05, 2.02) | 0.026 |
| 3 | 9 | 21 | 0.87 | (0.40, 1.89) | 0.719 |
| 4 | 17 | 71 | 0.77 | (0.45, 1.31) | 0.335 |
| X | 248 | 205 | 1.33 | (1.10, 1.60) | 0.003 |
| Follow-up time | |||||
| <6 years | 165 | 174 | 0.89 | (0.71, 1.12) | 0.333 |
| 6+ years | 194 | 261 | 1.67 | (1.38, 2.03) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leung, H.W.C.; Wang, S.-Y.; Lin, C.-L.; Chan, A.L.F. Radiation Dose-Induced Carotid Artery Stenosis and Brain Necrosis in Head and Neck Cancer—A Real World Cohort Study. Cancers 2024, 16, 2982. https://doi.org/10.3390/cancers16172982
Leung HWC, Wang S-Y, Lin C-L, Chan ALF. Radiation Dose-Induced Carotid Artery Stenosis and Brain Necrosis in Head and Neck Cancer—A Real World Cohort Study. Cancers. 2024; 16(17):2982. https://doi.org/10.3390/cancers16172982
Chicago/Turabian StyleLeung, Henry W. C., Shyh-Yau Wang, Cheng-Li Lin, and Agnes L. F. Chan. 2024. "Radiation Dose-Induced Carotid Artery Stenosis and Brain Necrosis in Head and Neck Cancer—A Real World Cohort Study" Cancers 16, no. 17: 2982. https://doi.org/10.3390/cancers16172982
APA StyleLeung, H. W. C., Wang, S.-Y., Lin, C.-L., & Chan, A. L. F. (2024). Radiation Dose-Induced Carotid Artery Stenosis and Brain Necrosis in Head and Neck Cancer—A Real World Cohort Study. Cancers, 16(17), 2982. https://doi.org/10.3390/cancers16172982