Simple Summary
Sensorineural hearing loss is a common late complication among nasopharyngeal cancer survivors, primarily due to the close proximity of the auditory apparatus to the treatment volume and the use of cisplatin-based chemotherapy. The incidence of hearing loss in the era of intensity-modulated radiation therapy varies widely, influenced by factors such as patient demographics, auditory assessment methods, and the duration of follow-up. While guidelines have provided recommendations on radiation dose constraints to the cochlea to mitigate hearing loss, significant risks remain. To improve hearing outcomes, strategies such as radiotherapy de-escalation, personalized treatment planning, and the consideration of alternative systemic agents in localized nasopharyngeal cancer are being investigated. This review discusses the context and relevant evidence regarding potential strategies to improve hearing outcomes in this patient population.
Abstract
Intensity-modulated radiation therapy (IMRT) improves disease control and reduces treatment-related toxicity in patients with localized nasopharyngeal carcinoma (NPC). However, due to the proximity of the auditory apparatus to the treatment volume and the frequent incorporation of cisplatin-based chemotherapy, treatment-related sensorineural hearing loss (SNHL) remains a common debilitating complication among NPC survivors. The reported crude incidence of SNHL following IMRT for NPC varies widely at 1–46% due to differences in auditory assessment methods and thresholds, follow-up durations, chemotherapy usage, and patient compositions. International guidelines and radiation dosimetric studies have recommended constraining the cochlear mean dose to less than 44–50 Gy, but the risk of SNHL remains high despite adherence to these constraints. Potential strategies to improve hearing outcomes in NPC survivors include cautious de-escalation of radiotherapy dose and volume, individualization of cochlear constraints, optimization of radiotherapy planning techniques, and the use of substitutes or alternative schedules for cisplatin-based chemotherapy. The addition of immune checkpoint inhibitors to chemoradiotherapy did not impact ototoxicity. Prospective studies that employ both objective and patient-reported auditory outcomes are warranted to test the long-term benefits of various approaches. This article aims to provide a comprehensive review of the incidence and radiation dose–toxicity relationship of SNHL in NPC survivors and to summarize potential strategies to optimize hearing outcomes in relation to nuances in radiotherapy planning and the selection of systemic therapy.
1. Introduction
Modern radiotherapy techniques, such as intensity-modulated radiation therapy (IMRT), have significantly improved the treatment outcomes of localized nasopharyngeal carcinoma (NPC) by enhancing disease control and reducing toxicity [1]. However, due to the proximity of the auditory apparatus to the nasopharynx, sensorineural hearing loss (SNHL) remains a major late complication in NPC survivors. Radiation-induced SNHL arises from direct damage to non-regenerating cochlear hair cells, as well as an indirect radiation-induced bystander effect triggered by oxidative stress and the inflammatory response [2]. The higher frequency hearing range is particularly susceptible to radiation-induced damage due to the low levels of the antioxidant glutathione in the basal outer hair cells, which are responsible for processing high-frequency sounds [3].
The incorporation of cisplatin as part of the definitive treatment regimens for NPC also contributes to ototoxicity. Cisplatin-induced ototoxicity is primarily driven by mitochondrial and DNA damage to the outer hair cells, spiral ganglion neurons, and stria vascularis of the cochlea, as well as the generation of reactive oxygen species that leads to inflammation and apoptotic cell death [4,5]. Importantly, these detrimental effects to the cochlea occur in a dose-dependent manner. Along with the increasing use of contemporary cisplatin-based induction or adjuvant therapy in locoregionally advanced NPC, the risk of ototoxicity in NPC survivors is further exacerbated.
During the era of conventional 2-dimensional (2D) radiotherapy for NPC, the reported incidence of SNHL was substantially high, ranging from 24% to 54% [6,7,8,9]. The advent of IMRT has enabled the delivery of highly conformal radiation to the planning target volume, thereby lowering the incidence of SNHL by better sparing the auditory apparatus (Figure 1). Over the past decade, there has been a growing body of literature on the dose–toxicity relationship of radiation-induced cochlear damage, allowing for the practical application of appropriate constraints during radiotherapy planning. Hearing outcomes may also be improved through cautious de-escalation in radiotherapy dose and volume, along with careful considerations of dosage, scheduling, and potential substitutes for cisplatin as a radiosensitizer.
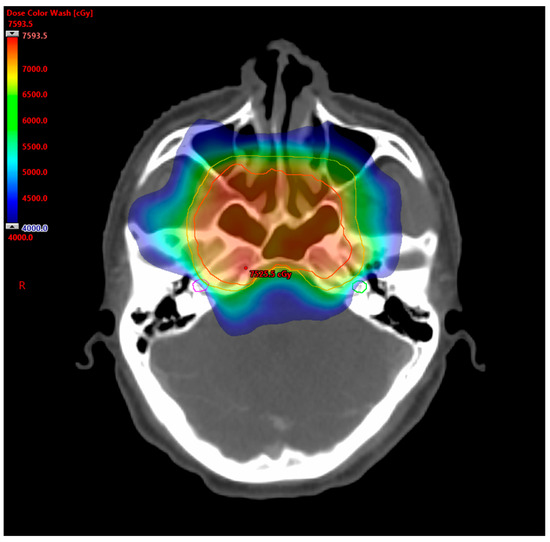
Figure 1.
Cochlear-sparing IMRT for NPC. This was a VMAT plan for a patient with T3N2M0 NPC. The radiation dose color wash was set to depict 40–75.9 Gy. The following structures are delineated: PTV70 (red line), PTV60 (orange line), right cochlea (purple line), and left cochlea (green line). The mean doses of right and left cochlea were 44.8 Gy and 39.8 Gy, respectively.
This review aims to summarize the incidence and radiation dose–toxicity relationship of SNHL in NPC survivors treated with modern radiotherapy and systemic therapy. Potential strategies for optimizing hearing outcomes in relation to radiotherapy planning and the selection of systemic therapy are also discussed.
2. Incidence of SNHL after IMRT for NPC
Several observational studies have reported the incidence of SNHL after IMRT for NPC, most of which had a retrospective design (Table 1) [10,11,12,13,14,15,16,17,18,19,20,21,22,23,24]. The median age of the patients was approximately 50 years, although two studies specifically recruited younger populations, with one enrolling patients under 20 years of age [18] and the other under 30 years of age [24]. Cisplatin was used as a concurrent radiosensitizer in most studies. The mean follow-up period varied significantly from 1.3 years to 9.9 years.

Table 1.
Summary of studies reporting incidence of SNHL in NPC patients who underwent IMRT.
Across the studies conducted in the era of IMRT, the reported incidence of SNHL ranged from 1.0% to 46.0% [10,11,12,13,14,15,16,17,18,19,20,21,22,23,24]. Heterogeneous assessment methods and thresholds have been used to define SNHL. Table 2 shows the various definitions of hearing impairment outlined in commonly employed grading scales [25,26,27]. Most studies utilized either pure tone audiometry (PTA) or the Common Terminology Criteria for Adverse Events (CTCAE) to define SNHL. For PTA, hearing impairment was defined as an increase in the bone conduction threshold (BCT) at low frequencies (0.5–2 kHz) or high frequency (4 kHz) compared to baseline values. CTCAE, on the other hand, allows for both audiometry-based assessments and physicians’ grading of limitations in activities of daily living (ADL) or the need for therapeutic intervention.
Table 2.
Ototoxicity grading scale for hearing impairment.
In addition to these physician-based assessment tools, there appears to be an emerging trend toward subjective assessment to define hearing impairment. For instance, in a recent study [24], post-radiation hearing impairment was assessed using the Hearing Handicap Inventory for Adult (HHIA)-Screening version, a self-administered questionnaire. This study found that nearly 30% of NPC survivors experienced self-perceived severe hearing impairment after IMRT. HHIA has been validated to correlate with pure tone sensitivity [28] and has been demonstrated to be a more robust indicator of social and emotional well-being when compared to the measured hearing loss [29]. Integrating patient-reported outcomes into the evaluation of hearing loss assessment may facilitate the development of management strategies that are targeted to clinically meaningful endpoints.
Across the observational studies, the incidence of PTA-defined SNHL among post-IMRT NPC survivors ranged from 7.7% to 46.0%, which appeared to be higher than those defined by CTCAE (7.0–27.5% for G2, 1.7–17.2% for ≥ G3). There are several possible explanations for this numerical difference. First, the PTA-defined SNHL incidence was typically reported on a per-ear basis, whereas the CTCAE-defined incidence was reported on a per-patient basis, which may have counted bilateral hearing loss as a single event. In addition, PTA-defined SNHL focuses on specific hearing frequencies, which may not fully correlate with a patient’s ADL. For example, all studies that used PTA included high-frequency hearing loss at 4 kHz, as it is known to be more susceptible to the detrimental effects of radiation [3,30]. However, this measurement may not accurately reflect the impact on patients’ ADL, as the normal speech range occurs at a lower frequency range of 0.5–2 kHz [7].
It is worth noting that the reported risk of SNHL could also be influenced by the concurrent use of cisplatin, which was not accounted for by all studies. For instance, a study by Wang et al. demonstrated a significantly higher incidence of SNHL in patients who received a cumulative cisplatin dose exceeding 200 mg/m2 [15]. Over the recent decade, there has been a paradigm shift toward the use of extended chemotherapy in locoregionally advanced NPC. Both the ASCO and ESMO guidelines have recommended the adoption of either induction or adjuvant chemotherapy in addition to standard chemoradiotherapy [31,32]. These approaches, albeit effective, are associated with high cumulative cisplatin doses of up to 480 mg/m2 to 540 mg/m2. Given the heightened risk of compounded ototoxicity, more stringent radiation dose constraints for the cochlea may be required to adequately protect NPC patients from SNHL.
Another important consideration when examining the incidence of SNHL is the duration of follow-up. Early-onset hearing impairment is common among NPC patients who undergo definitive radiotherapy, but it may be unrelated to cochlear injury. Early prospective studies during the conventional 2D RT era indicated that a substantial proportion of patients developed otitis media as an acute adverse effect of irradiation, which is typically transient and resolves spontaneously within two years [7,8]. This finding is supported by modern IMRT cohorts, which also showed that radiation to the cochlea and inner ear was associated with late-onset high-frequency SNHL (24 months after RT completion) but not early-onset SNHL (within 12 months of RT completion) [22]. Considering this latency period, long-term follow-up for at least two years is necessary to accurately determine the incidence of radiation-induced SNHL. Notably, two studies [23,24] had an extended follow-up period of more than 8 years, reporting incidences of hearing impairment as high as 40%. In the absence of non-irradiated controls, their interpretations must be taken with caution, as age-related hearing loss and patients lost to follow-up may confound the incidence of SNHL.
3. Radiation Dose–Toxicity Relationship of SNHL
The radiation dose to several components of the auditory apparatus may be relevant to radiation-induced SNHL. A contouring atlas was developed to promote standardized delineation of organs at risk in patients with NPC receiving IMRT [33]. It was recommended that four auditory sub-structures should be contoured, namely, the internal auditory canal (IAC), cochlea, tympanic cavity, and bony part of the Eustachian tube. Their boundaries should be delineated on the bone window of simulation computer tomography images.
Despite the meticulous auditory OARs proposed for NPC radiotherapy planning, most studies have focused on the cochlea when evaluating the dose–response relationship of radiation ototoxicity. Given the small size of the cochlea (approximately 0.2 mL), it is reasonable that mean dose was the most commonly investigated parameter for establishing constraints.
Table 3 summarizes the studies on auditory constraints proposed for NPC radiotherapy planning and the corresponding incidence of SNHL stratified according to these constraints [11,15,20,21,22,24,34,35,36,37]. The proposed cochlear constraints were consistently set in the range of Dmean <44–50 Gy. These proposals are in line with the recommendations from QUANTEC and current international guidelines [38,39], which suggest limiting the cochlear Dmean to under 45 Gy. Understanding that this target may not be realistically achievable in locally advanced NPC, guidelines have also set a second constraint of cochlear Dmean <55 Gy for radiotherapy planning [39].
Table 3.
Summary of studies on dosimetric constraints of the auditory apparatus in radiotherapy planning for NPC.
Other than the cochlea, few studies have suggested the use of the IAC as a key auditory OAR. Two studies proposed IAC constraints of 32.7 Gy and 50 Gy, below which the SNHL rates were <21.6% and <25.8%, respectively [11,20]. In another study with a longer follow-up period, IAC V50 <40% and V60 <40% were recommended as dose constraints to limit self-reported hearing impairment. Two nomograms have been constructed using these metrics to assist with probability prediction in radiotherapy planning [24].
Instead of using a single constraint to dichotomize the risk of SNHL, studies have attempted to establish a quantitative relationship between cochlear dose and hearing loss in NPC survivors. In a recent retrospective study, Yip et al. estimated that each 10 Gy increase in cochlear Dmean would result in a 5 dB increase in BCT at 4 kHz [22]. Similarly, Peuker et al. developed a normal tissue complication probability model for the inner ear, estimating predicted toxicity rates of 25% and 50% at mean doses of 44 Gy and 65 Gy, respectively [37]. These findings highlight the merit of minimizing cochlear dose beyond the standard constraints to further reduce the risk of permanent hearing loss.
4. Prevention Strategy
4.1. De-Escalating Radiotherapy
In the era of IMRT, standard radiation doses of 70 Gy have demonstrated high local control rates of over 80–90% [40,41]. In radiotherapy planning, the clinical target volume (CTV), encompassing the gross tumor volume (GTV) along with a margin for potential subclinical disease extension, is of utmost significance as it is the volume that must be adequately treated to achieve a cure. The international guidelines on CTV delineation for NPC proposed by Lee et al. [42] recommend including the entire nasopharynx within either the full therapeutic volume (70 Gy) or prophylactic volume (lower dose), rather than relying on geometric expansion from the gross tumor. In addition, the petrous apex is routinely included within the prophylactic volume regardless of the local tumor extent. This blanket target delineation approach, when indiscriminately applied to all primary tumors, may result in unnecessarily high radiation doses to the auditory apparatus, particularly in patients with early lateralized diseases. Alternative target delineation methods to individualize the primary CTV according to T-stage and tumor topography have been proposed (Table 4) [43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60].
Table 4.
Potential strategies to prevent SNHL in patients with NPC.
The local extension of NPC typically follows a stepwise spread pattern, with over 70% of primary tumors exhibiting asymmetrical infiltration into the skull base structures [61]. This raises the potential of sparing the contralateral organs at risk in lateralized tumors. In a retrospective study conducted by Xie et al. focusing on unilateral NPC (defined as tumors not crossing the midline according to endoscopy and MRI), the primary CTV was delineated using 1.5–2 cm geometric expansion from the GTV without prophylactic inclusion of the contralateral skull base structures [43]. After a median follow-up of 7 years, no out-of-field local recurrence was observed in the contralateral unirradiated structures. Importantly, this approach resulted in a low average Dmean of the contralateral middle ear of 24.1 Gy. No high-grade acute hearing loss was observed, and only 1 out of 95 contralateral ears developed late hearing impairment.
A more recent study by Wang et al. proposed an individualized method for delineating the CTV that combines geometric expansion and the consideration of anatomical structures [45]. This approach involves the division of the adjacent structures of the nasopharynx into different tiers, taking into account the pattern of tumor spread. The CTV was then delineated using a combination of geometric expansion and the inclusion of at-risk structures based on the extent of the primary tumor. Specifically, only the ipsilateral petrous apex was included in primary CTV. With a median follow-up period of 66.6 months, both the 5-year local recurrence-free survival and overall survival (OS) rates exceeded 90%, and the incidence of grade 3 hearing impairment was remarkably low (0.2%).
Another potential strategy is response-adaptive de-escalation of radiotherapy. The use of induction chemotherapy before concurrent chemoradiotherapy has shown significant improvements in OS in patients with advanced NPC [62]. However, the optimal CTV following response to induction chemotherapy remains controversial. Current international guidelines suggest that the pre-induction chemotherapy volume should ideally receive the full therapeutic dose regardless of any shrinkage that may occur after induction chemotherapy [42]. In a randomized controlled trial, Xiang et al. [44] tested the feasibility of radiation volume de-escalation, with the post-induction chemotherapy volume receiving the full therapeutic dose and the pre-induction chemotherapy volume treated with a lower prophylactic dose. Compared with the control group, in which patients received a full therapeutic dose to the pre-induction chemotherapy volume, patients who underwent de-escalated radiotherapy had similar 5-year locoregional relapse-free survival. While differences in cochlear dose have not been reported, patients in the reduced-volume group had a significantly lower incidence of late hearing loss (52.2% vs. 69.1%), suggesting potential merits in preserving auditory function with this de-escalation approach.
In addition to restricting high-dose radiation to the post-induction chemotherapy tumor volume, several studies have proposed dose de-escalation in patients who exhibit tumor responses. In a retrospective, propensity score-matched cohort analysis conducted by Yao et al. [46], the impact of reducing the radiation dose to the high-risk CTV was evaluated in adolescent patients with locally advanced NPC who achieved complete or partial response after two to four cycles of induction chemotherapy. Compared with patients who received standard doses (66–70 Gy), patients in the reduced-dose (60–65.9 Gy) group had similar survival outcomes but a lower incidence of severe late toxicity, including grade 3–4 hearing loss (10.6% vs. 5.9%). This response-adaptive approach was tested in a phase II single-arm prospective trial by Luo et al. [47]. The trial stratified patients based on their response to induction chemotherapy: for patients whose tumors achieved complete response (CR) or partial response (PR), a lower dose of 60 Gy was given to the GTV, 54 Gy to the high-risk CTV, and 48 Gy to the low-risk CTV, whereas standard doses of 70 Gy, 60 Gy, and 54 Gy were given for static or progressed tumors. This approach resulted in excellent 3-year progression-free survival (PFS) and OS rates of 91% and 100%, respectively. The incidence of grade 1–2 hearing impairment was low at 14%, and no high-grade event was reported.
Apart from using tumor responses to stratify patients for treatment de-escalation, there is also growing interest in individualizing radiation doses based on biomarker responses. Guo et al. investigated the role of de-escalating the radiation dose in low-risk stage III NPC with low pre-treatment plasma EBV DNA levels [48]. After two cycles of induction chemotherapy, patients who achieved tumor responses and had undetectable plasma EBV DNA received 60–66 Gy, whereas those who did not meet these criteria were treated with 70 Gy. This approach resulted in an encouraging 3-year PFS rate of 88.8%. Importantly, the incidence of grade 1–2 hearing impairment in patients treated with a reduced dose was low at 14.7%, in contrast to 41.4% in patients who received standard radiotherapy dose.
Ultimately, given the prevailing importance of local tumor control over the risk of radiation-induced SNHL, de-escalation in radiotherapy volume or dose should be carefully approached with individualized considerations of the anatomic relationships between the tumor and cochlea, baseline auditory function, and patient preference. Prospective clinical trials that incorporate auditory outcomes as secondary endpoints will help to ensure safety and provide valuable insight into the magnitude of the benefit.
4.2. Individualizing Cochlea Dose Constraints
In the current international dose prioritization guidelines for NPC, each OAR was assigned a “goal” constraint and a “maximum acceptance” constraint [39]. The Dmean constraints for the cochlea were set to ≤45 Gy and ≤55 Gy, respectively. Among the list of OARs, the cochlea was assigned the lowest dosimetric priority (priority 4).
Instead of using a one-size-fits-all constraint on the cochlea, a risk-stratified approach has been proposed to achieve better cochlea sparing across different T stages. In a dosimetric study by Zhang et al. using step-and-shoot IMRT, various strategies to reduce cochlear dose were attempted [49]. These included setting tiered cochlear constraints, upgrading the protection priority for the cochlea, and modification of the radiation beam angle. For T1 tumors, the maximal cochlear dose was set to <45 Gy. For T2 or T3 tumors of which the PTV overlapped with the cochlea, a constraint of V50 < 50% was applied. For T3 or T4 tumors where the PTV encircled the cochlea, the maximum cochlear dose was limited to <103% of the prescription dose. In addition, during plan optimization, the dosimetric priority of the cochlea was upgraded to the same level as the salivary glands. Compared to the control plans, the above approach achieved a significantly lower cochlear Dmean without compromising target coverage parameters or other important OARs. The average ipsilateral and contralateral cochlear Dmeans were reduced from 50.6 Gy to 46.2 Gy and 50.0 Gy to 43.9 Gy, respectively.
4.3. Selection of Radiotherapy Techniques
Compared with standard step-and-shoot IMRT, volumetric modulated arc therapy (VMAT) may achieve superior dose homogeneity and lower doses to the OARs through modulation of the multileaf collimator (MLC) pattern, as well as gantry rotation speed and dose rate [63]. In the context of NPC, several investigators have examined the benefit of VMAT on cochlear dose [50,51,52,53]. In a planning study that compared the dosimetric outcomes between VMAT and step-and-shoot IMRT, jaw tracking was employed in VMAT plans to ensure the cochlea was kept outside the treatment field during gantry rotation, thereby reducing the interleaf leakage from MLC [52]. This technique resulted in significantly lower average cochlear Dmeans (right: 18.5 Gy vs. 26.1 Gy; left: 15.0 Gy vs. 24.1 Gy). In another large retrospective study that included 627 NPC patients, the use of VMAT also resulted in significantly lower rates of grade 1–2 (16.4% vs. 25.1%) and grade 3–4 (0.9% vs. 3.1%) ototoxicity than step-and-shoot IMRT, suggesting that VMAT may be the preferred radiotherapy planning technique for NPC [51].
The use of proton therapy in the treatment of NPC has gained attention due to its dosimetric advantages in minimizing the dose to normal structures, which are particularly important when the primary tumor and OARs are in close proximity. Several studies have reported the auditory outcomes of proton therapy for NPC [54,55,56]. In cohorts that utilized modern pencil-beam proton radiotherapy, the reported cochlear Dmean ranged from 31 Gy to 42 Gy. No high-grade hearing impairment was reported, with a low incidence of grade 2 events of 4–7% at 2 years after treatment [54,55]. In another retrospective dosimetric study, Anderson et al. showed that proton therapy could achieve a significantly lower cochlear Dmean (25.5–33.2 Gy) when compared to treatment with photon-based IMRT (31.5–41.8 Gy) [56]. These data support clear dosimetric advantages of proton therapy on the cochlea in NPC radiotherapy planning. Prospective studies that compare with proton- and photon-based IMRT are warranted to quantify the magnitude of the benefits in auditory outcomes.
4.4. De-Escalating Systemic Therapy
Since the risk of SNHL is compounded by the use of cisplatin, de-escalating systemic therapy in carefully selected patient subgroups may also reduce the risk of SNHL in patients with localized NPC.
For stage II NPC, recommendations from international guidelines suggest that concurrent chemoradiotherapy with cisplatin may be considered in selected patients [31,32,64,65], based on the survival benefit shown in a randomized clinical trial that used 2DRT [66]. However, in the era of IMRT, increasing evidence suggests that radiotherapy alone can achieve excellent clinical outcomes [67,68,69]. In a recent randomized controlled trial, Tang et al. [57] examined the feasibility of omitting concurrent cisplatin in low-risk NPC, defined as stage II or T3N0M0 (AJCC 7th edition) without adverse features, namely, lymph nodes larger than 3 cm, level IV, or VB nodal involvement, extracapsular extension, and plasma EBV DNA levels higher than 4000 copies/mL. With a median follow-up of 46 months, radiotherapy alone has led to survival outcomes that are non-inferior to those of chemoradiotherapy. The omission of concurrent cisplatin appeared to have a small benefit in reducing the risk of hearing impairment (grades 1–2, 40% vs. 47%).
Treatment with fewer concurrent cisplatin cycles has also been investigated. Traditionally, concurrent cisplatin in chemoradiotherapy for NPC consists of 3 tri-weekly cycles at a dose of 100 mg/m2 [40,70]. In a phase II randomized non-inferiority trial, Li et al. [58] compared 2 cycles versus 3 cycles of concurrent cisplatin in stage III to IVB NPC patients with plasma EBV DNA <4000 copies/mL. While the 3-year survival outcomes were similar between the two groups, patients who underwent 2 cycles of concurrent cisplatin had a lower incidence of hearing impairment of any grade (22.9% vs. 35.2%) and a trend toward lower severe hearing impairment (0.6% vs. 3.6%), suggesting that 200 mg/m2 of cisplatin may be a sufficient dose for low-risk loco-regionally advanced diseases.
Traditionally, fractionated cisplatin delivery schedules, such as the weekly regimen, have been thought to be less ototoxic [71]. A recent randomized controlled trial compared 2 cycles of concurrent once-every-3-weeks cisplatin (100 mg/m2) to 6 cycles of weekly cisplatin (40 mg/m2) in NPC patients [72]. Surprisingly, while the 3-year failure-free survival rates were similar between the two groups, the rate of late grade 3–4 hearing impairment was significantly lower in patients treated with once-every-3-weeks cisplatin (9.6% vs. 16.5%). This finding may be attributable to the higher cumulative cisplatin dose in the weekly than the once-every-3-weeks group (median, 220 mg/m2 vs. 200 mg/m2), further supporting the clinical merit of safe de-escalation of cisplatin dose in the treatment for NPC.
In search of alternative concurrent agents to cisplatin, researchers have developed platinum derivatives to mitigate the toxicity associated with cisplatin. Tang et al. showed that nedaplatin-based concurrent chemoradiotherapy is non-inferior to standard cisplatin-based concurrent chemoradiotherapy in terms of 2-year PFS, with a significantly lower rate of any grade (14% vs. 23%) and grade 3 hearing impairment (2% vs. 6%) [59]. On the other hand, Lv et al. [60] showed that S-1, a 5-fluorouracil prodrug, can be used as a concurrent agent with IMRT in NPC treatment. Its combination with IMRT resulted in a favorable 3-year PFS of 87.4%, with grade 1 hearing impairment observed in only 2.3% of patients, without grade 2 or above events.
A substantial body of research is currently exploring the integration of immune checkpoint inhibitors with radiotherapy for NPC. A recent randomized phase III trial has indicated that the addition of sintilimab, a PD-1 inhibitor, to standard induction-concurrent chemoradiotherapy significantly improved event-free survival in patients with loco-regionally advanced disease [73]. Importantly, this intensification of treatment did not adversely affect auditory outcomes, as evidenced by the comparable rates of all-grade hearing impairment between the sintilimab group and the standard therapy group (35% vs. 34%). Additionally, ongoing clinical trials are investigating the efficacy of adjuvant immune checkpoint inhibitors following standard chemoradiotherapy (NCT03544099, NCT04910347). Should these approaches demonstrate non-inferiority relative to standard induction or adjuvant chemotherapy, they may help to reduce the cumulative cisplatin dose from extended chemotherapy cycles, thereby reducing the risk of SNHL in patients with advanced NPC. This approach may hold particular relevance for those high-risk patients who might otherwise be undertreated without the use of induction or adjuvant cisplatin-based chemotherapy.
5. Management
Radiation- or cisplatin-induced SNHL is an irreversible complication for which no standard treatment is currently available. Among the available options, hearing aids offer a non-surgical and accessible treatment for patients with serviceable hearing [74]. For patients with severe SNHL, sound amplification by hearing aids would be ineffective, and cochlear implantation may be considered.
Cochlear implants transduce acoustic energy into electrical signals that stimulate the surviving spiral ganglion cells of the auditory nerve [75]. Although whether the retro-cochlear auditory pathway is damaged following chemoradiotherapy remains controversial [76,77], retrospective studies and case series have demonstrated the efficacy and safety of cochlear implants in terms of improving hearing and speech performance in NPC survivors with severe SNHL [77,78,79]. Co-existing radiation-induced complications, such as chronic suppurative otitis media (CSOM) and temporal bone osteonecrosis, can complicate the candidacy for cochlear implants. In these situations, concurrent surgeries including mastoidectomy, temporal bone resection, and external auditory canal elimination may be required [79,80]. The bone-anchored implantable hearing aid system may represent a potential solution for post-irradiation patients with CSOM, recurrent ear discharge, and osteoradionecrotic bony ear canal ulcers. The system utilizes an osseointegrated titanium implant to directly transmit sound to the functioning cochlea, bypassing the external and middle ear mechanism. A prospective longitudinal study showed that NPC patients had improved subjective hearing clarity and reduced otorrhea rate with this system [81]. These surgical options may be particularly beneficial for those high-risk NPC patients who are not eligible for treatment de-escalation.
Emerging therapies, such as signal pathway inhibitors, antioxidant drugs, and gene therapy, are currently under investigation as potential treatment options, although none are currently approved for the treatment of SNHL in NPC survivors [2]. For example, AM-111, a c-Jun N-terminal kinase (JNK) inhibitor, was found to significantly improve hearing outcomes in patients with profound idiopathic sudden SNHL [82]; it is expected to be useful in radiation-induced SNHL, which also involves the JNK signaling pathway in its pathogenesis [83]. As radiation-induced SNHL is closely associated with oxidative stress and the inflammatory response, antioxidant drugs appear to be reasonable agents in treatment. Many antioxidants, such as melatonin and amifostine, have been tested in animals but not humans. Methylprednisolone use during RT has been shown to reduce SNHL one year after RT in a small prospective trial, but larger studies with longer follow-up are needed [84]. On the other hand, cochlear hair cell regeneration using induced pluripotent stem cells and epigenetic drugs has emerged as a promising treatment option, although many of them are still in their preclinical phases of drug development [85].
6. Conclusions
SNHL is a debilitating and irreversible late complication in NPC survivors. The reviewed studies reported a wide range of SNHL incidence following contemporary radiotherapy and systemic treatments for NPC, which can be attributed to the heterogeneity in assessment methods, auditory endpoints, cumulative cisplatin dose, and follow-up durations. There is an emerging trend toward incorporating patient-reported outcomes to evaluate hearing impairment, highlighting the importance of a comprehensive approach that encompasses both objective and subjective measures.
In terms of prevention, constraining the cochlear Dmean to under 44–50 Gy may reduce radiation ototoxicity, but the incidence of SNHL remained relatively high even when these constraints were met. Other potential strategies to mitigate the risk of SNHL in NPC survivors include response-adaptive de-escalation of radiotherapy volume and dose, individualization of cochlear constraints according to tumor stage, employing specific radiotherapy planning techniques, and cautious de-escalation of systemic therapy. Prospective studies are warranted to evaluate the long-term outcomes of these approaches.
Author Contributions
Conceptualization, J.C.S.H., B.B.Y.M. and J.C.H.C.; writing—original draft preparation, J.C.H.C.; writing—review and editing, J.C.S.H., B.B.Y.M. and J.C.H.C.; supervision, B.B.Y.M. and J.C.H.C. All authors have read and agreed to the published version of the manuscript.
Funding
This study is supported by Hong Kong Research Grant Council General Research Grant: 14108923.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Peng, G.; Wang, T.; Yang, K.Y.; Zhang, S.; Zhang, T.; Li, Q.; Han, J.; Wu, G. A prospective, randomized study comparing outcomes and toxicities of intensity-modulated radiotherapy vs. conventional two-dimensional radiotherapy for the treatment of nasopharyngeal carcinoma. Radiother. Oncol. 2012, 104, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Shi, W.; Hou, X.; Bao, X.; Hou, W.; Jiang, X.; Ma, L.; Jiang, X.; Dong, L. Mechanism and Protection of Radiotherapy Induced Sensorineural Hearing Loss for Head and Neck Cancer. Biomed. Res. Int. 2021, 2021, 3548706. [Google Scholar] [CrossRef] [PubMed]
- Low, W.K.; Tan, M.G.; Chua, A.W.; Sun, L.; Wang, D.Y. 12th Yahya Cohen Memorial Lecture: The cellular and molecular basis of radiation-induced sensori-neural hearing loss. Ann. Acad. Med. Singap. 2009, 38, 91–94. [Google Scholar] [CrossRef] [PubMed]
- Tan, W.J.T.; Vlajkovic, S.M. Molecular Characteristics of Cisplatin-Induced Ototoxicity and Therapeutic Interventions. Int. J. Mol. Sci. 2023, 24, 16545. [Google Scholar] [CrossRef] [PubMed]
- Chattaraj, A.; Syed, M.P.; Low, C.A.; Owonikoko, T.K. Cisplatin-Induced Ototoxicity: A Concise Review of the Burden, Prevention, and Interception Strategies. JCO Oncol. Pract. 2023, 19, 278–283. [Google Scholar] [CrossRef]
- Oh, Y.T.; Kim, C.H.; Choi, J.H.; Kang, S.H.; Chun, M. Sensory neural hearing loss after concurrent cisplatin and radiation therapy for nasopharyngeal carcinoma. Radiother. Oncol. 2004, 72, 79–82. [Google Scholar] [CrossRef]
- Ho, W.K.; Wei, W.I.; Kwong, D.L.; Sham, J.S.; Tai, P.T.; Yuen, A.P.; Au, D.K. Long-term sensorineural hearing deficit following radiotherapy in patients suffering from nasopharyngeal carcinoma: A prospective study. Head. Neck 1999, 21, 547–553. [Google Scholar] [CrossRef]
- Kwong, D.L.; Wei, W.I.; Sham, J.S.; Ho, W.K.; Yuen, P.W.; Chua, D.T.; Au, D.K.; Wu, P.M.; Choy, D.T. Sensorineural hearing loss in patients treated for nasopharyngeal carcinoma: A prospective study of the effect of radiation and cisplatin treatment. Int. J. Radiat. Oncol. Biol. Phys. 1996, 36, 281–289. [Google Scholar] [CrossRef]
- Moretti, J.A. Sensori-neural hearing loss following radiotherapy to the nasopharynx. Laryngoscope 1976, 86, 598–602. [Google Scholar] [CrossRef]
- Hsin, C.H.; Chen, T.H.; Young, Y.H.; Liu, W.S. Comparison of otologic complications between intensity-modulated and two-dimensional radiotherapies in nasopharyngeal carcinoma patients. Otolaryngol. Head. Neck Surg. 2010, 143, 662–668. [Google Scholar] [CrossRef]
- Petsuksiri, J.; Sermsree, A.; Thephamongkhol, K.; Keskool, P.; Thongyai, K.; Chansilpa, Y.; Pattaranutaporn, P. Sensorineural hearing loss after concurrent chemoradiotherapy in nasopharyngeal cancer patients. Radiat. Oncol. 2011, 6, 19. [Google Scholar] [CrossRef] [PubMed]
- Leung, S.W.; Lee, T.F. Treatment of nasopharyngeal carcinoma by tomotherapy: Five-year experience. Radiat. Oncol. 2013, 8, 107. [Google Scholar] [CrossRef]
- Lee, A.W.; Ng, W.T.; Chan, L.L.; Hung, W.M.; Chan, C.C.; Sze, H.C.; Chan, O.S.; Chang, A.T.; Yeung, R.M. Evolution of treatment for nasopharyngeal cancer--success and setback in the intensity-modulated radiotherapy era. Radiother. Oncol. 2014, 110, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Ou, X.; Zhou, X.; Shi, Q.; Xing, X.; Yang, Y.; Xu, T.; Shen, C.; Wang, X.; He, X.; Kong, L.; et al. Treatment outcomes and late toxicities of 869 patients with nasopharyngeal carcinoma treated with definitive intensity modulated radiation therapy: New insight into the value of total dose of cisplatin and radiation boost. Oncotarget 2015, 6, 38381–38397. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Chen, Y.Y.; Tai, A.; Chen, X.L.; Huang, S.M.; Yang, C.; Bao, Y.; Li, N.W.; Deng, X.W.; Zhao, C.; et al. Sensorineural Hearing Loss after Combined Intensity Modulated Radiation Therapy and Cisplatin-Based Chemotherapy for Nasopharyngeal Carcinoma. Transl. Oncol. 2015, 8, 456–462. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Han, F.; Xiao, W.; Xiang, Y.; Lu, L.; Deng, X.; Cui, N.; Zhao, C. Analysis of late toxicity in nasopharyngeal carcinoma patients treated with intensity modulated radiation therapy. Radiat. Oncol. 2015, 10, 17. [Google Scholar] [CrossRef]
- Huang, T.L.; Chien, C.Y.; Tsai, W.L.; Liao, K.C.; Chou, S.Y.; Lin, H.C.; Dean Luo, S.; Lee, T.F.; Lee, C.H.; Fang, F.M. Long-term late toxicities and quality of life for survivors of nasopharyngeal carcinoma treated with intensity-modulated radiotherapy versus non-intensity-modulated radiotherapy. Head Neck 2016, 38 (Suppl. S1), E1026–E1032. [Google Scholar] [CrossRef]
- Qiu, W.Z.; Peng, X.S.; Xia, H.Q.; Huang, P.Y.; Guo, X.; Cao, K.J. A retrospective study comparing the outcomes and toxicities of intensity-modulated radiotherapy versus two-dimensional conventional radiotherapy for the treatment of children and adolescent nasopharyngeal carcinoma. J. Cancer Res. Clin. Oncol. 2017, 143, 1563–1572. [Google Scholar] [CrossRef]
- Chan, S.L.; Ng, L.S.; Goh, X.; Siow, C.H.; Goh, H.L.; Goh, B.C.; Cheo, T.; Loh, K.S.; Brunham, L.R. Time course and clinical characterization of cisplatin-induced ototoxicity after treatment for nasopharyngeal carcinoma in a South East Asian population. Head Neck 2018, 40, 1425–1433. [Google Scholar] [CrossRef]
- Zhu, W.; Chen, F.; Li, J.; Wang, W.; Zhang, H.; Yang, G.; Zou, L.; Zhu, Y.; Yuan, W.; Ding, H.; et al. Dosimetric parameters associated with conductive or sensorineural hearing loss 5 years after intensity-modulated radiation therapy in nasopharyngeal carcinoma. Acta Otolaryngol. 2019, 139, 263–268. [Google Scholar] [CrossRef]
- Inada, M.; Nishimura, Y.; Ishikura, S.; Ishikawa, K.; Murakami, N.; Kodaira, T.; Ito, Y.; Tsuchiya, K.; Murakami, Y.; Saito, J.; et al. Organs-at-risk dose constraints in head and neck intensity-modulated radiation therapy using a dataset from a multi-institutional clinical trial (JCOG1015A1). Radiat. Oncol. 2022, 17, 133. [Google Scholar] [CrossRef] [PubMed]
- Yip, P.L.; Mok, K.C.J.; Ho, H.S.; Lee, W.Y.V.; Wong, A.C.L.; Lau, C.T.; Wong, F.C.S.; Yeung, K.W.; Lee, S.F. Sensorineural Hearing Loss in Nasopharyngeal Carcinoma Survivors in the Modern Treatment Era—The Early and Late Effects of Radiation and Cisplatin. Clin. Oncol. (R. Coll. Radiol.) 2022, 34, e160–e167. [Google Scholar] [CrossRef] [PubMed]
- Doi, H.; Ri, A.; Inada, M.; Tatsuno, S.; Uehara, T.; Matsuura, T.; Ishikawa, K.; Nakamatsu, K.; Hosono, M.; Nishimura, Y. Clinical course of longer than five years after definitive radiotherapy for nasopharyngeal carcinoma. Int. J. Clin. Oncol. 2023, 28, 1607–1615. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Li, J.; Li, K.; Hu, J.; Li, Q.; Huang, C.; Wang, G.; Liu, N.; Tang, L. Evaluation and analysis of risk factors of hearing impairment for nasopharyngeal carcinoma treated using intensity-modulated radiotherapy. Radiother. Oncol. 2024, 190, 109985. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute (US). Common Terminology Criteria for Adverse Events (CTCAE), 4th ed.; U.S. Department of Health and Human Services, National Institutes of Health, National Cancer Institute: Bethesda, MD, USA, 2009. [Google Scholar]
- LENT SOMA scales for all anatomic sites. Int. J. Radiat. Oncol. Biol. Phys. 1995, 31, 1049–1091. [CrossRef]
- Cox, J.D.; Stetz, J.; Pajak, T.F. Toxicity criteria of the Radiation Therapy Oncology Group (RTOG) and the European Organization for Research and Treatment of Cancer (EORTC). Int. J. Radiat. Oncol. Biol. Phys. 1995, 31, 1341–1346. [Google Scholar] [CrossRef]
- Newman, C.W.; Weinstein, B.E.; Jacobson, G.P.; Hug, G.A. Test-retest reliability of the hearing handicap inventory for adults. Ear Hear. 1991, 12, 355–357. [Google Scholar] [CrossRef]
- Bass, J.K.; Wang, F.; Thaxton, M.E.; Warren, S.E.; Srivastava, D.K.; Hudson, M.M.; Ness, K.K.; Brinkman, T.M. Association of hearing loss with patient-reported functional outcomes in adult survivors of childhood cancer. J. Natl. Cancer Inst. 2024, 116, 596–605. [Google Scholar] [CrossRef]
- Lau, S.K.; Wei, W.I.; Sham, J.S.; Choy, D.T.; Hui, Y. Early changes of auditory brain stem evoked response after radiotherapy for nasopharyngeal carcinoma--a prospective study. J. Laryngol. Otol. 1992, 106, 887–892. [Google Scholar] [CrossRef]
- Chen, Y.P.; Ismaila, N.; Chua, M.L.K.; Colevas, A.D.; Haddad, R.; Huang, S.H.; Wee, J.T.S.; Whitley, A.C.; Yi, J.L.; Yom, S.S.; et al. Chemotherapy in Combination With Radiotherapy for Definitive-Intent Treatment of Stage II-IVA Nasopharyngeal Carcinoma: CSCO and ASCO Guideline. J. Clin. Oncol. 2021, 39, 840–859. [Google Scholar] [CrossRef]
- Bossi, P.; Chan, A.T.; Licitra, L.; Trama, A.; Orlandi, E.; Hui, E.P.; Halamkova, J.; Mattheis, S.; Baujat, B.; Hardillo, J.; et al. Nasopharyngeal carcinoma: ESMO-EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up(dagger). Ann. Oncol. 2021, 32, 452–465. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Yu, X.L.; Luo, W.; Lee, A.W.; Wee, J.T.; Lee, N.; Zhou, G.Q.; Tang, L.L.; Tao, C.J.; Guo, R.; et al. Recommendation for a contouring method and atlas of organs at risk in nasopharyngeal carcinoma patients receiving intensity-modulated radiotherapy. Radiother. Oncol. 2014, 110, 390–397. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.C.; Jackson, A.; Budnick, A.S.; Pfister, D.G.; Kraus, D.H.; Hunt, M.A.; Stambuk, H.; Levegrun, S.; Wolden, S.L. Sensorineural hearing loss in combined modality treatment of nasopharyngeal carcinoma. Cancer 2006, 106, 820–829. [Google Scholar] [CrossRef]
- Chan, S.H.; Ng, W.T.; Kam, K.L.; Lee, M.C.; Choi, C.W.; Yau, T.K.; Lee, A.W.; Chow, S.K. Sensorineural hearing loss after treatment of nasopharyngeal carcinoma: A longitudinal analysis. Int. J. Radiat. Oncol. Biol. Phys. 2009, 73, 1335–1342. [Google Scholar] [CrossRef] [PubMed]
- Wei, Y.; Zhou, T.; Zhu, J.; Zhang, Y.; Sun, M.; Ding, X.; Wang, D.; Li, H.; Li, B. Long-term outcome of sensorineural hearing loss in nasopharyngeal carcinoma patients: Comparison between treatment with radiotherapy alone and chemoradiotherapy. Cell Biochem. Biophys. 2014, 69, 433–437. [Google Scholar] [CrossRef] [PubMed]
- Peuker, L.; Rolf, D.; Oertel, M.; Peuker, A.; Scobioala, S.; Hering, D.; Rudack, C.; Haverkamp, U.; Eich, H.T. Definition of an Normal Tissue Complication Probability Model for the Inner Ear in Definitive Radiochemotherapy of Nasopharynx Carcinoma. Cancers 2022, 14, 3422. [Google Scholar] [CrossRef]
- Bhandare, N.; Jackson, A.; Eisbruch, A.; Pan, C.C.; Flickinger, J.C.; Antonelli, P.; Mendenhall, W.M. Radiation therapy and hearing loss. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, S50–S57. [Google Scholar] [CrossRef]
- Lee, A.W.; Ng, W.T.; Pan, J.J.; Chiang, C.L.; Poh, S.S.; Choi, H.C.; Ahn, Y.C.; AlHussain, H.; Corry, J.; Grau, C.; et al. International Guideline on Dose Prioritization and Acceptance Criteria in Radiation Therapy Planning for Nasopharyngeal Carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2019, 105, 567–580. [Google Scholar] [CrossRef]
- Lee, N.; Harris, J.; Garden, A.S.; Straube, W.; Glisson, B.; Xia, P.; Bosch, W.; Morrison, W.H.; Quivey, J.; Thorstad, W.; et al. Intensity-modulated radiation therapy with or without chemotherapy for nasopharyngeal carcinoma: Radiation therapy oncology group phase II trial 0225. J. Clin. Oncol. 2009, 27, 3684–3690. [Google Scholar] [CrossRef]
- Au, K.H.; Ngan, R.K.C.; Ng, A.W.Y.; Poon, D.M.C.; Ng, W.T.; Yuen, K.T.; Lee, V.H.F.; Tung, S.Y.; Chan, A.T.C.; Sze, H.C.K.; et al. Treatment outcomes of nasopharyngeal carcinoma in modern era after intensity modulated radiotherapy (IMRT) in Hong Kong: A report of 3328 patients (HKNPCSG 1301 study). Oral Oncol. 2018, 77, 16–21. [Google Scholar] [CrossRef]
- Lee, A.W.; Ng, W.T.; Pan, J.J.; Poh, S.S.; Ahn, Y.C.; AlHussain, H.; Corry, J.; Grau, C.; Gregoire, V.; Harrington, K.J.; et al. International guideline for the delineation of the clinical target volumes (CTV) for nasopharyngeal carcinoma. Radiother. Oncol. 2018, 126, 25–36. [Google Scholar] [CrossRef] [PubMed]
- Xie, D.H.; Wu, Z.; Li, W.Z.; Cheng, W.Q.; Tao, Y.L.; Wang, L.; Lv, S.W.; Lin, F.F.; Cui, N.J.; Zhao, C.; et al. Individualized clinical target volume delineation and efficacy analysis in unilateral nasopharyngeal carcinoma treated with intensity-modulated radiotherapy (IMRT): 10-year summary. J. Cancer Res. Clin. Oncol. 2022, 148, 1931–1942. [Google Scholar] [CrossRef] [PubMed]
- Xiang, L.; Rong, J.F.; Xin, C.; Li, X.Y.; Zheng, Y.; Ren, P.R.; Lin, S.; Wen, Q.L.; He, L.J.; Zhang, J.W.; et al. Reducing Target Volumes of Intensity Modulated Radiation Therapy After Induction Chemotherapy in Locoregionally Advanced Nasopharyngeal Carcinoma: Long-Term Results of a Prospective, Multicenter, Randomized Trial. Int. J. Radiat. Oncol. Biol. Phys. 2023, 117, 914–924. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Huang, N.; Yip, P.L.; Wang, J.; Huang, R.; Sun, Z.; Kang, D.; He, Q.; Deng, X.; Zhao, C.; et al. The individualized delineation of clinical target volume for primary nasopharyngeal carcinoma based on invasion risk of substructures: A prospective, real-world study with a large population. Radiother. Oncol. 2024, 194, 110154. [Google Scholar] [CrossRef] [PubMed]
- Yao, J.J.; Jin, Y.N.; Lin, Y.J.; Zhang, W.J.; Marks, T.; Ryan, I.; Zhang, H.Y.; Xia, L.P. The feasibility of reduced-dose radiotherapy in childhood nasopharyngeal carcinoma with favorable response to neoadjuvant chemotherapy. Radiother. Oncol. 2023, 178, 109414. [Google Scholar] [CrossRef]
- Luo, D.H.; Li, X.Y.; Guo, S.S.; Guo, W.P.; Liu, L.T.; Mo, H.Y.; Guo, L.; Lv, X.F.; Liu, L.Z.; Li, J.B.; et al. Paclitaxel liposome, cisplatin and 5-fluorouracil-based induction chemotherapy followed by de-escalated intensity-modulated radiotherapy with concurrent cisplatin in stage IVA-IVB childhood nasopharyngeal carcinoma in endemic area: A phase II, single-arm trial. Lancet Reg. Health West. Pac. 2023, 40, 100895. [Google Scholar] [CrossRef]
- Guo, S.S.; Yang, J.H.; Sun, X.S.; Liu, L.Z.; Yang, Z.C.; Liu, L.T.; Liu, S.L.; Li, X.Y.; Lv, X.F.; Luo, D.H.; et al. Reduced-dose radiotherapy for Epstein-Barr virus DNA selected staged III nasopharyngeal carcinoma: A single-arm, phase 2 trial. Eur. J. Cancer 2023, 194, 113336. [Google Scholar] [CrossRef]
- Zhang, C.; Liu, L.X.; Li, W.Z.; Liang, W.; Chen, Z.H.; Huang, X.H.; Qi, J.; Chen, X.H.; Liang, J.G.; Cao, X.L. Cochlea sparing with a stratified scheme of dose limitation employed in intensity-modulated radiotherapy for nasopharyngeal carcinoma: A dosimetry study. Med. Dosim. 2019, 44, 226–232. [Google Scholar] [CrossRef]
- Gao, J.; Qian, T.L.; Tao, C.Z.; Zhang, Y.H.; Zhou, Y.; Yang, J.; He, J.; Wang, R.; Zhou, P.J. SmartArc-based volumetric modulated arc therapy can improve the middle ear, vestibule and cochlea sparing for locoregionally advanced nasopharyngeal carcinoma: A dosimetric comparison with step-and-shoot intensity-modulated radiotherapy. Br. J. Radiol. 2015, 88, 20150052. [Google Scholar] [CrossRef]
- He, L.; Xiao, J.; Wei, Z.; He, Y.; Wang, J.; Guan, H.; Mu, X.; Peng, X. Toxicity and dosimetric analysis of nasopharyngeal carcinoma patients undergoing radiotherapy with IMRT or VMAT: A regional center’s experience. Oral Oncol. 2020, 109, 104978. [Google Scholar] [CrossRef]
- Lamaj, E.; Vu, E.; van Timmeren, J.E.; Leonardi, C.; Marc, L.; Pytko, I.; Guckenberger, M.; Balermpas, P. Cochlea sparing optimized radiotherapy for nasopharyngeal carcinoma. Radiat. Oncol. 2021, 16, 64. [Google Scholar] [CrossRef] [PubMed]
- Nanda, S.; Parida, S.; Ahirwar, M.K. A Dosimetric Comparison of Volumetric-modulated Arc Therapy and IMRT for Cochlea-sparing Radiation Therapy in Locally Advanced Nasopharyngeal Cancer. J. Med. Phys. 2023, 48, 248–251. [Google Scholar] [CrossRef] [PubMed]
- Jiri, K.; Vladimir, V.; Michal, A.; Matej, N.; Silvia, S.; Pavel, V.; Katerina, D.; Jana, P.; Barbora, O.; Eliska, R.; et al. Proton pencil-beam scanning radiotherapy in the treatment of nasopharyngeal cancer: Dosimetric parameters and 2-year results. Eur. Arch. Otorhinolaryngol. 2021, 278, 763–769. [Google Scholar] [CrossRef] [PubMed]
- Williams, V.M.; Parvathaneni, U.; Laramore, G.E.; Aljabab, S.; Wong, T.P.; Liao, J.J. Intensity-Modulated Proton Therapy for Nasopharynx Cancer: 2-year Outcomes from a Single Institution. Int. J. Part. Ther. 2021, 8, 28–40. [Google Scholar] [CrossRef]
- Anderson, J.L.; Schreibmann, E.; Bates, J.E.; Rudra, S.; Hall, B.; Neunuebel, A.; Remick, J.S.; Stokes, W.A.; McDonald, M.W. Photon vs. Proton Radiotherapy in the Definitive Treatment of Nasopharyngeal Cancer: Single Institution Experience. Int. J. Radiat. Oncol. Biol. Phys. 2023, 117, e562. [Google Scholar] [CrossRef]
- Tang, L.L.; Guo, R.; Zhang, N.; Deng, B.; Chen, L.; Cheng, Z.B.; Huang, J.; Hu, W.H.; Huang, S.H.; Luo, W.J.; et al. Effect of Radiotherapy Alone vs Radiotherapy With Concurrent Chemoradiotherapy on Survival Without Disease Relapse in Patients With Low-risk Nasopharyngeal Carcinoma: A Randomized Clinical Trial. JAMA 2022, 328, 728–736. [Google Scholar] [CrossRef]
- Li, X.Y.; Luo, D.H.; Guo, L.; Mo, H.Y.; Sun, R.; Guo, S.S.; Liu, L.T.; Yang, Z.C.; Yang, J.H.; Qiu, F.; et al. Deintensified Chemoradiotherapy for Pretreatment Epstein-Barr Virus DNA-Selected Low-Risk Locoregionally Advanced Nasopharyngeal Carcinoma: A Phase II Randomized Noninferiority Trial. J. Clin. Oncol. 2022, 40, 1163–1173. [Google Scholar] [CrossRef]
- Tang, L.Q.; Chen, D.P.; Guo, L.; Mo, H.Y.; Huang, Y.; Guo, S.S.; Qi, B.; Tang, Q.N.; Wang, P.; Li, X.Y.; et al. Concurrent chemoradiotherapy with nedaplatin versus cisplatin in stage II-IVB nasopharyngeal carcinoma: An open-label, non-inferiority, randomised phase 3 trial. Lancet Oncol. 2018, 19, 461–473. [Google Scholar] [CrossRef]
- Lv, T.; Wang, Y.; Ou, D.; Liu, P.; Qin, S.; Liu, L.; Lou, P.; Wang, X. IMRT combined with S-1 concurrent chemoradiotherapy in locally advanced nasopharyngeal carcinoma: A prospective phase II study. Investig. New Drugs 2019, 37, 352–359. [Google Scholar] [CrossRef]
- Wu, Z.; Qi, B.; Lin, F.F.; Zhang, L.; He, Q.; Li, F.P.; Wang, H.; Han, Y.Q.; Yin, W.J. Characteristics of local extension based on tumor distribution in nasopharyngeal carcinoma and proposed clinical target volume delineation. Radiother. Oncol. 2023, 183, 109595. [Google Scholar] [CrossRef]
- Zhang, Y.; Chen, L.; Hu, G.Q.; Zhang, N.; Zhu, X.D.; Yang, K.Y.; Jin, F.; Shi, M.; Chen, Y.P.; Hu, W.H.; et al. Final Overall Survival Analysis of Gemcitabine and Cisplatin Induction Chemotherapy in Nasopharyngeal Carcinoma: A Multicenter, Randomized Phase III Trial. J. Clin. Oncol. 2022, 40, 2420–2425. [Google Scholar] [CrossRef] [PubMed]
- Lee, F.K.; Yip, C.W.; Cheung, F.C.; Leung, A.K.; Chau, R.M.; Ngan, R.K. Dosimetric difference amongst 3 techniques: TomoTherapy, sliding-window intensity-modulated radiotherapy (IMRT), and RapidArc radiotherapy in the treatment of late-stage nasopharyngeal carcinoma (NPC). Med. Dosim. 2014, 39, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Tang, L.L.; Chen, Y.P.; Chen, C.B.; Chen, M.Y.; Chen, N.Y.; Chen, X.Z.; Du, X.J.; Fang, W.F.; Feng, M.; Gao, J.; et al. The Chinese Society of Clinical Oncology (CSCO) clinical guidelines for the diagnosis and treatment of nasopharyngeal carcinoma. Cancer Commun. 2021, 41, 1195–1227. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network. Head and Neck Cancers (Version 4.2024). Available online: https://www.nccn.org/professionals/physician_gls/pdf/head-and-neck.pdf (accessed on 20 May 2024).
- Chen, Q.Y.; Wen, Y.F.; Guo, L.; Liu, H.; Huang, P.Y.; Mo, H.Y.; Li, N.W.; Xiang, Y.Q.; Luo, D.H.; Qiu, F.; et al. Concurrent chemoradiotherapy vs radiotherapy alone in stage II nasopharyngeal carcinoma: Phase III randomized trial. J. Natl. Cancer Inst. 2011, 103, 1761–1770. [Google Scholar] [CrossRef] [PubMed]
- Su, S.F.; Han, F.; Zhao, C.; Chen, C.Y.; Xiao, W.W.; Li, J.X.; Lu, T.X. Long-term outcomes of early-stage nasopharyngeal carcinoma patients treated with intensity-modulated radiotherapy alone. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Zhang, Y.; Li, W.F.; Liu, X.; Guo, R.; Sun, Y.; Lin, A.H.; Chen, L.; Ma, J. Efficacy of Concurrent Chemotherapy for Intermediate Risk NPC in the Intensity-Modulated Radiotherapy Era: A Propensity-Matched Analysis. Sci. Rep. 2015, 5, 17378. [Google Scholar] [CrossRef]
- Huang, X.; Chen, X.; Zhao, C.; Wang, J.; Wang, K.; Wang, L.; Miao, J.; Cao, C.; Jin, T.; Zhang, Y.; et al. Adding Concurrent Chemotherapy to Intensity-Modulated Radiotherapy Does Not Improve Treatment Outcomes for Stage II Nasopharyngeal Carcinoma: A Phase 2 Multicenter Clinical Trial. Front. Oncol. 2020, 10, 1314. [Google Scholar] [CrossRef]
- Al-Sarraf, M.; LeBlanc, M.; Giri, P.G.; Fu, K.K.; Cooper, J.; Vuong, T.; Forastiere, A.A.; Adams, G.; Sakr, W.A.; Schuller, D.E.; et al. Chemoradiotherapy versus radiotherapy in patients with advanced nasopharyngeal cancer: Phase III randomized Intergroup study 0099. J. Clin. Oncol. 1998, 16, 1310–1317. [Google Scholar] [CrossRef]
- Teft, W.A.; Winquist, E.; Nichols, A.C.; Kuruvilla, S.; Richter, S.; Parker, C.; Francis, P.; Trinnear, M.; Lukovic, J.; Bukhari, N.; et al. Predictors of cisplatin-induced ototoxicity and survival in chemoradiation treated head and neck cancer patients. Oral Oncol. 2019, 89, 72–78. [Google Scholar] [CrossRef]
- Xia, W.X.; Lv, X.; Liang, H.; Liu, G.Y.; Sun, R.; Zeng, Q.; Li, S.W.; Mo, H.Y.; Han, F.; Luo, D.H.; et al. A Randomized Controlled Trial Comparing Two Different Schedules for Cisplatin Treatment in Patients with Locoregionally Advanced Nasopharyngeal Cancer. Clin. Cancer Res. 2021, 27, 4186–4194. [Google Scholar] [CrossRef]
- Liu, X.; Zhang, Y.; Yang, K.Y.; Zhang, N.; Jin, F.; Zou, G.R.; Zhu, X.D.; Xie, F.Y.; Liang, X.Y.; Li, W.F.; et al. Induction-concurrent chemoradiotherapy with or without sintilimab in patients with locoregionally advanced nasopharyngeal carcinoma in China (CONTINUUM): A multicentre, open-label, parallel-group, randomised, controlled, phase 3 trial. Lancet 2024, 403, 2720–2731. [Google Scholar] [CrossRef] [PubMed]
- Ishak, E.M.; Gallitto, M.; Golub, J.S.; Sisti, M.B.; Wang, T.J.C. Radiation-Induced Sensorineural Hearing Loss and Potential Management. Pract. Radiat. Oncol. 2024, 14, 212–215. [Google Scholar] [CrossRef] [PubMed]
- Deep, N.L.; Dowling, E.M.; Jethanamest, D.; Carlson, M.L. Cochlear Implantation: An Overview. J. Neurol. Surg. B Skull Base 2019, 80, 169–177. [Google Scholar] [CrossRef] [PubMed]
- Li, J.J.; Guo, Y.K.; Tang, Q.L.; Li, S.S.; Zhang, X.L.; Wu, P.A.; Yang, X.M. Prospective study of sensorineural hearing loss following radiotherapy for nasopharyngeal carcinoma. J. Laryngol. Otol. 2010, 124, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Chang, W.W.; Yeung, K.N.; Luk, B.P.; Leung, K.K.; Sung, J.K.; Tong, M.C. Cochlear implantation in postirradiated ears: A case-control comparative study. Laryngoscope Investig. Otolaryngol. 2020, 5, 1163–1167. [Google Scholar] [CrossRef]
- Lee, C.Y.; Lin, W.C.; Lin, C.C.; Hsu, C.J.; Wu, H.P. Management Options for Patients With Nasopharyngeal Carcinoma Undergoing Cochlear Implantation. Ear Nose Throat J. 2020, 145561320947274. [Google Scholar] [CrossRef]
- Huang, Y.; Wang, X.; Huang, H.; Ge, R.; Liu, X.; Huang, D.; Huang, Y.; Mo, Y.; Lin, X.; Liu, T.; et al. Long-Term Outcomes of Cochlear Implantation in Irradiated Ears of Nasopharyngeal Carcinoma Patients. Laryngoscope 2021, 131, 649–655. [Google Scholar] [CrossRef]
- Alahmadi, A.; Abdelsamad, Y.; Al-Zuraiqi, B.; Alghamdi, S.; Hagr, A.; Saleh, E. Cochlear Implantation in Radiation-Induced Hearing Loss: A Systematic Review. Otol. Neurotol. 2023, 44, 767–774. [Google Scholar] [CrossRef]
- Soo, G.; Tong, M.C.; Tsang, W.S.; Wong, T.K.; To, K.F.; Leung, S.F.; van Hasselt, C.A. The BAHA hearing system for hearing-impaired postirradiated nasopharyngeal cancer patients: A new indication. Otol. Neurotol. 2009, 30, 496–501. [Google Scholar] [CrossRef]
- Staecker, H.; Jokovic, G.; Karpishchenko, S.; Kienle-Gogolok, A.; Krzyzaniak, A.; Lin, C.D.; Navratil, P.; Tzvetkov, V.; Wright, N.; Meyer, T. Efficacy and Safety of AM-111 in the Treatment of Acute Unilateral Sudden Deafness-A Double-blind, Randomized, Placebo-controlled Phase 3 Study. Otol. Neurotol. 2019, 40, 584–594. [Google Scholar] [CrossRef]
- Tan, P.X.; Du, S.S.; Ren, C.; Yao, Q.W.; Yuan, Y.W. Radiation-induced Cochlea hair cell death: Mechanisms and protection. Asian Pac. J. Cancer Prev. 2013, 14, 5631–5635. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Zhao, Y.; Zhou, X.; Tan, L.; Ou, Z.; Yu, Y.; Wang, Y. Methylprednisolone use during radiotherapy extenuates hearing loss in patients with nasopharyngeal carcinoma. Laryngoscope 2016, 126, 100–103. [Google Scholar] [CrossRef] [PubMed]
- Khalaily, L.; Avraham, K.B. Insights into the regulation of hearing regeneration. Front. Audiol. Otol. 2024, 2, 1404617. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).