
T-Cell Subtypes and Immune Signatures in Cutaneous Immune-Related Adverse Events in Melanoma Patients under Immune Checkpoint Inhibitor Therapy

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Plasma Analysis and PBMC Isolation
2.3. Flow Cytometry
2.4. Statistics
3. Results
3.1. Clinical Characteristics of the Patient Cohort
3.2. Shift towards Th1 Cells in PBMCs during ICI Is Not Associated with a Favorable Clinical Response
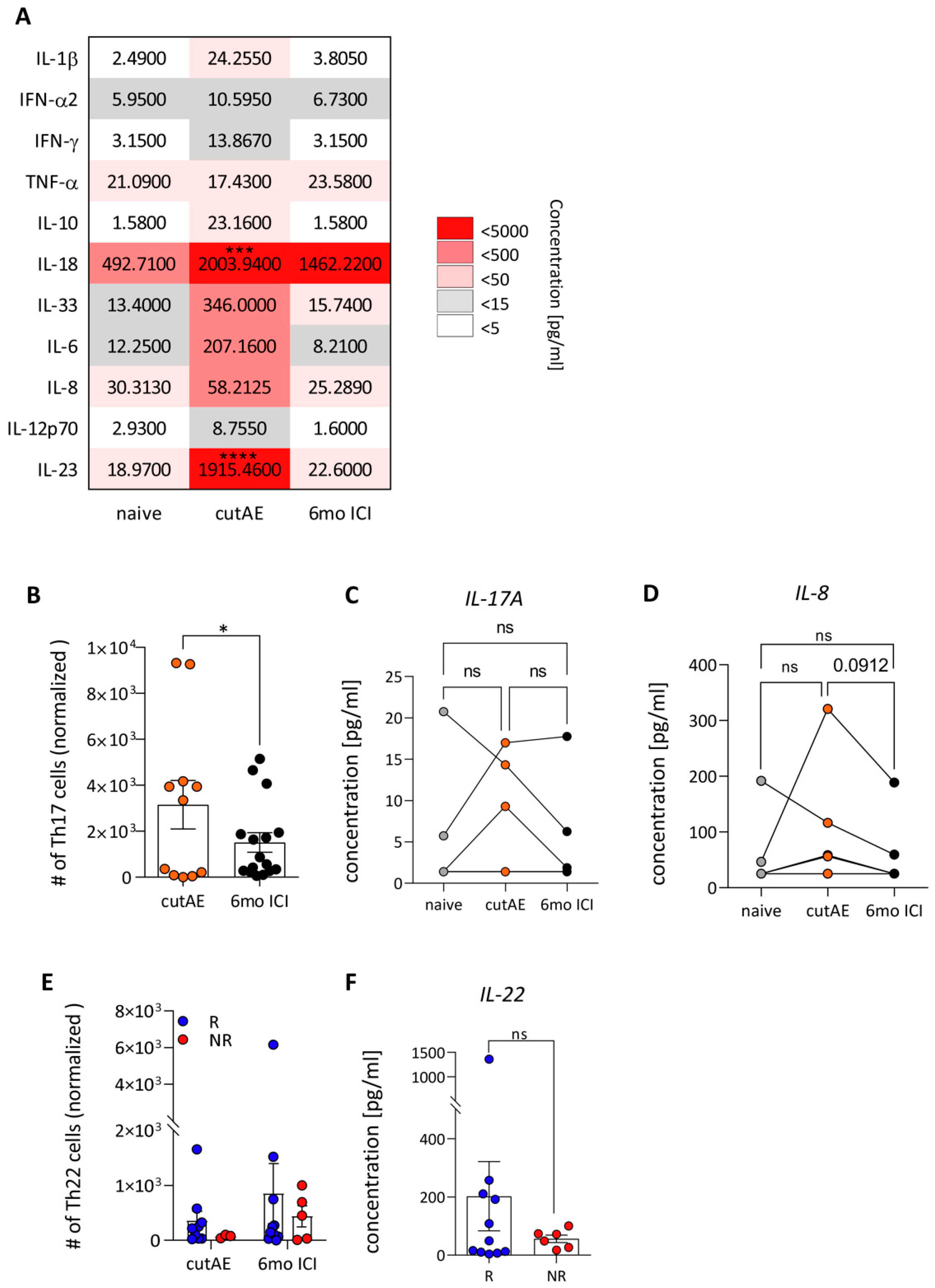
3.3. CutAEs Show a Th17/Th22-Related Immune Profile
3.4. Increase in Inflammatory Cytokines at the Occurrence of cutAEs
3.5. Pro-Inflammatory IL-10 Is Associated with cutAEs and Increased in Non-Responders
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CLA | cutaneous lymphocyte-associated antigen |
| CT | computer tomography |
| CTLA-4 | cytotoxic T-lymphocyte-associated protein 4 |
| cutAE | cutaneous immune-related adverse event |
| DMSO | dimethylsulfoxide |
| EDTA | ethylenediaminetetraacetic acid |
| FCS | fetal calf plasma |
| ICI | immune checkpoint inhibition |
| irAE | immune-related adverse event |
| NK | natural killer cell |
| NR | non-responder |
| NSCLC | non-small cell lung cancer |
| PBMC | peripheral blood mononuclear cell |
| PBS | phosphate-buffered saline |
| PD1 | programmed cell death protein 1 |
| PET | positron emission tomography |
| PFS | progression-free survival |
| R | responder |
| RECIST | response evaluation criteria in solid tumors |
References
- Robert, C.; Long, G.V.; Brady, B.; Dutriaux, C.; Maio, M.; Mortier, L.; Hassel, J.C.; Rutkowski, P.; McNeil, C.; Kalinka-Warzocha, E.; et al. Nivolumab in Previously Untreated Melanoma without Braf Mutation. N. Engl. J. Med. 2015, 372, 320–330. [Google Scholar] [CrossRef]
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.J.; Cowey, C.L.; Lao, C.D.; Schadendorf, D.; Dummer, R.; Smylie, M.; Rutkowski, P.; et al. Combined Nivolumab and Ipilimumab or Monotherapy in Untreated Melanoma. N. Engl. J. Med. 2015, 373, 23–34. [Google Scholar] [CrossRef] [PubMed]
- Sibaud, V. Dermatologic Reactions to Immune Checkpoint Inhibitors. Am. J. Clin. Dermatol. 2018, 19, 345–361. [Google Scholar] [CrossRef] [PubMed]
- Luke Jason, J.; Ott, P.A. Pd-1 Pathway Inhibitors: The Next Generation of Immunotherapy for Advanced Melanoma. Oncotarget 2015, 6, 3479. [Google Scholar] [CrossRef] [PubMed]
- Postow Michael, A.; Sidlow, R.; Hellmann, M.D. Immune-Related Adverse Events Associated with Immune Checkpoint Blockade. N. Engl. J. Med. 2018, 378, 158–168. [Google Scholar] [CrossRef]
- Fausto, P.; Grizzi, G.; Ghidini, M.; Ghidini, A.; Ratti, M.; Panni, S.; Cabiddu, M.; Ghilardi, M.; Borgonovo, K.; Parati, M.C. Immune-Related Adverse Events and Survival in Solid Tumors Treated with Immune Checkpoint Inhibitors: A Systematic Review and Meta-Analysis. J. Immunother. 2020, 43, 1–7. [Google Scholar]
- Horvat, T.Z.; Adel, N.G.; Dang, T.O.; Momtaz, P.; Postow, M.A.; Callahan, M.K.; Carvajal, R.D.; Dickson, M.A.; D’Angelo, S.P.; Woo, K.M.; et al. Immune-Related Adverse Events, Need for Systemic Immunosuppression, and Effects on Survival and Time to Treatment Failure in Patients with Melanoma Treated with Ipilimumab at Memorial Sloan Kettering Cancer Center. J. Clin. Oncol. 2015, 33, 3193–3198. [Google Scholar] [CrossRef]
- Geisler, A.N.; Phillips, G.S.; Barrios, D.M.; Wu, J.; Leung, D.Y.M.; Moy, A.P.; Kern, J.A.; Lacouture, M.E. Immune Checkpoint Inhibitor-Related Dermatologic Adverse Events. J. Am. Acad. Dermatol. 2020, 83, 1255–1268. [Google Scholar] [CrossRef]
- Habre, M.; Habre, S.B.; Kourie, H.R. Dermatologic Adverse Events of Checkpoint Inhibitors: What an Oncologist Should Know. Immunotherapy 2016, 8, 1437–1446. [Google Scholar] [CrossRef]
- Said, J.T.; Talia, J.; Wei, E.; Mostaghimi, A.; Semenov, Y.; Giobbie-Hurder, A.; Chen, S.T.; LeBoeuf, N.R. Impact of Biologic Therapy on Cancer Outcomes in Patients with Immune Checkpoint Inhibitor-Induced Bullous Pemphigoid. J. Am. Acad. Dermatol. 2023, 88, 670–671. [Google Scholar] [CrossRef]
- Lu, W.; Zhang, H.; Guo, Q.; Gou, Z.; Yao, J. Selected Cutaneous Adverse Events in Patients Treated with Ici Monotherapy and Combination Therapy: A Retrospective Pharmacovigilance Study and Meta-Analysis. Front. Pharmacol. 2023, 14, 1076473. [Google Scholar] [CrossRef]
- Wongvibulsin, S.; Pahalyants, V.; Kalinich, M.; Murphy, W.; Yu, K.H.; Wang, F.; Chen, S.T.; Reynolds, K.; Kwatra, S.G.; Semenov, Y.R. Epidemiology and Risk Factors for the Development of Cutaneous Toxicities in Patients Treated with Immune-Checkpoint Inhibitors: A United States Population-Level Analysis. J. Am. Acad. Dermatol. 2022, 86, 563–572. [Google Scholar] [CrossRef] [PubMed]
- Celine, B.; Tarhini, A.; Routier, E.; Lambotte, O.; Ladurie, F.L.; Carbonnel, F.; Izzeddine, H.; Marabelle, A.; Champiat, S.; Berdelou, A. Safety Profiles of Anti-Ctla-4 and Anti-Pd-1 Antibodies Alone and in Combination. Nat. Rev. Clin. Oncol. 2016, 13, 473–486. [Google Scholar]
- Plachouri, K.M.; Florou, V.; Georgiou, V.; Georgiou, S. Cutaneous Side Effects of Modern Targeted Therapy and Immunotherapy in Patients with Dermatological Malignancies. Cancers 2023, 15, 3126. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Cho, D.H.; Park, H.J. Il-18 and Cutaneous Inflammatory Diseases. Int. J. Mol. Sci. 2015, 16, 29357–29369. [Google Scholar] [CrossRef]
- Helmby, H.; Grencis, R.K. Il-18 Regulates Intestinal Mastocytosis and Th2 Cytokine Production Independently of Ifn-Gamma During Trichinella Spiralis Infection. J. Immunol. 2002, 169, 2553–2560. [Google Scholar] [CrossRef] [PubMed]
- He, S.H. Key Role of Mast Cells and Their Major Secretory Products in Inflammatory Bowel Disease. World J. Gastroenterol. 2004, 10, 309–318. [Google Scholar] [CrossRef]
- Hsu, P.; Santner-Nanan, B.; Hu, M.; Skarratt, K.; Lee, C.H.; Stormon, M.; Wong, M.; Fuller, S.J.; Nanan, R. Il-10 Potentiates Differentiation of Human Induced Regulatory T Cells via Stat3 and Foxo1. J. Immunol. 2015, 195, 3665–3674. [Google Scholar] [CrossRef]
- Christian, G.; Franco, P.A.V.; Arosio, P.; Hersey, P. Immunosuppressive Effects of Melanoma-Derived Heavy-Chain Ferritin Are Dependent on Stimulation of Il-10 Production. Int. J. Cancer 2001, 92, 843–850. [Google Scholar]
- Khoja, L.; Day, D.; Chen, T.W.-W.; Siu, L.L.; Hansen, A.R. Tumour- and Class-Specific Patterns of Immune-Related Adverse Events of Immune Checkpoint Inhibitors: A Systematic Review. Ann. Oncol. 2017, 28, 2377–2385. [Google Scholar] [CrossRef]
- Alexander, L.; Aadel, X.; Chaudhuri, A.; Nene, A.; Bacchiocchi, A.; Earland, N.; Vesely, M.D.; Usmani, A.; Turner, B.E.; Steen, C.B.; et al. T Cell Characteristics Associated with Toxicity to Immune Checkpoint Blockade in Patients with Melanoma. Nat. Med. 2022, 28, 353–362. [Google Scholar]
- Lim, S.Y.; Lee, J.H.; Gide, T.N.; Menzies, A.M.; Guminski, A.; Carlino, M.S.; Breen, E.J.; Yang, J.Y.H.; Ghazanfar, S.; Kefford, R.F.; et al. Circulating Cytokines Predict Immune-Related Toxicity in Melanoma Patients Receiving Anti-Pd-1-Based Immunotherapy. Clin. Cancer Res. 2019, 25, 1557–1563. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.; Kishimoto, T. Interplay between Interleukin-6 Signaling and the Vascular Endothelium in Cytokine Storms. Exp. Mol. Med. 2021, 53, 1116–1123. [Google Scholar] [CrossRef]
- Gieseck Richard, L.; Wilson, M.S.; Wynn, T.A. Type 2 Immunity in Tissue Repair and Fibrosis. Nat. Rev. Immunol. 2018, 18, 62–76. [Google Scholar] [CrossRef] [PubMed]
- Sun, Q.; Hong, Z.; Zhang, C.; Wang, L.; Han, Z.; Ma, D. Immune Checkpoint Therapy for Solid Tumours: Clinical Dilemmas and Future Trends. Signal Transduct. Target. Ther. 2023, 8, 320. [Google Scholar] [CrossRef] [PubMed]
- Mübeccel, A.; Palomares, O.; van de Veen, W.; van Splunter, M.; Akdis, C.A. Th17 and Th22 Cells: A Confusion of Antimicrobial Response with Tissue Inflammation Versus Protection. J. Allergy Clin. Immunol. 2012, 129, 1438–1449. [Google Scholar]
- Liu, X.; Xiao, Y.; Pan, Y.; Li, H.; Zheng, S.G.; Su, W. The Role of the Il-33/St2 Axis in Autoimmune Disorders: Friend or Foe? Cytokine Growth Factor. Rev. 2019, 50, 60–74. [Google Scholar] [CrossRef]
- von Euw, E.; Chodon, T.; Attar, N.; Jalil, J.; Koya, R.C.; Comin-Anduix, B.; Ribas, A. Ctla4 Blockade Increases Th17 Cells in Patients with Metastatic Melanoma. J. Transl. Med. 2009, 7, 35. [Google Scholar] [CrossRef]
- Ahmad, A.T.; Zahoor, H.; Lin, Y.; Malhotra, U.; Sander, C.; Butterfield, L.H.; Kirkwood, J.M. Baseline Circulating Il-17 Predicts Toxicity While Tgf-Β1 and Il-10 Are Prognostic of Relapse in Ipilimumab Neoadjuvant Therapy of Melanoma. J. ImmunoTherapy Cancer 2015, 3, 39. [Google Scholar]
- Dudakov, J.A.; Hanash, A.M.; van den Brink, M.R. Interleukin-22: Immunobiology and Pathology. Annu. Rev. Immunol. 2015, 33, 747–785. [Google Scholar] [CrossRef]
- Liang, S.C.; Tan, X.Y.; Luxenberg, D.P.; Karim, R.; Dunussi-Joannopoulos, K.; Collins, M.; Fouser, L.A. Interleukin (Il)-22 and Il-17 Are Coexpressed by Th17 Cells and Cooperatively Enhance Expression of Antimicrobial Peptides. J. Exp. Med. 2006, 203, 2271–2279. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Su, Y.; Jiao, A.; Wang, X.; Zhang, B. T Cells in Health and Disease. Signal Transduct. Target. Ther. 2023, 8, 235. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.; ATheron, J.; Rapoport, B.L. Immunopathogenesis of Immune Checkpoint Inhibitor-Related Adverse Events: Roles of the Intestinal Microbiome and Th17 Cells. Front. Immunol. 2019, 10, 2254. [Google Scholar] [CrossRef] [PubMed]
- Puxeddu, I.; Italiani, P.; Giungato, P.; Pratesi, F.; Panza, F.; Bartaloni, D.; Rocchi, V.; Del Corso, I.; Boraschi, D.; Migliorini, P. Free Il-18 and Il-33 Cytokines in Chronic Spontaneous Urticaria. Cytokine 2013, 61, 741–743. [Google Scholar] [CrossRef] [PubMed]
- Kurt, E.; Aktas, A.; Aksu, K.; Keren, M.; Dokumacioglu, A.; Goss, C.H.; Alatas, O. Autologous Serum Skin Test Response in Chronic Spontaneous Urticaria and Respiratory Diseases and Its Relationship with Serum Interleukin-18 Level. Arch. Dermatol. Res. 2011, 303, 643–649. [Google Scholar] [CrossRef] [PubMed]
- de Waal Malefyt, R.; Abrams, J.; Bennett, B.; Figdor, C.G.; de Vries, J.E. Interleukin 10(Il-10) Inhibits Cytokine Synthesis by Human Monocytes: An Autoregulatory Role of Il-10 Produced by Monocytes. J. Exp. Med. 1991, 174, 1209–1220. [Google Scholar] [CrossRef] [PubMed]
- Del Prete, G.; De Carli, M.; Almerigogna, F.; Giudizi, M.G.; Biagiotti, R.; Romagnani, S. Human Il-10 Is Produced by Both Type 1 Helper (Th1) and Type 2 Helper (Th2) T Cell Clones and Inhibits Their Antigen-Specific Proliferation and Cytokine Production. J. Immunol. 1993, 150, 353–360. [Google Scholar] [CrossRef]
- Taga, K.; Tosato, G. Il-10 Inhibits Human T Cell Proliferation and Il-2 Production. J. Immunol. 1992, 148, 1143–1148. [Google Scholar] [CrossRef]
- Cassatella, M.A.; Meda, L.; Bonora, S.; Ceska, M.; Constantin, G. Interleukin 10 (Il-10) Inhibits the Release of Proinflammatory Cytokines from Human Polymorphonuclear Leukocytes. Evidence for an Autocrine Role of Tumor Necrosis Factor and Il-1 Beta in Mediating the Production of Il-8 Triggered by Lipopolysaccharide. J. Exp. Med. 1993, 178, 2207–2211. [Google Scholar] [CrossRef]
- Ralph, P.; Nakoinz, I.; Sampson-Johannes, A.; Fong, S.; Lowe, D.; Min, H.Y.; Lin, L. Il-10, T Lymphocyte Inhibitor of Human Blood Cell Production of Il-1 and Tumor Necrosis Factor. J. Immunol. 1992, 148, 808–814. [Google Scholar] [CrossRef]
- Tripp, C.S.; Wolf, S.F.; Unanue, E.R. Interleukin 12 and Tumor Necrosis Factor Alpha Are Costimulators of Interferon Gamma Production by Natural Killer Cells in Severe Combined Immunodeficiency Mice with Listeriosis, and Interleukin 10 Is a Physiologic Antagonist. Proc. Natl. Acad. Sci. USA 1993, 90, 3725–3729. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Zhou, F.; Zhao, C.; Cheng, L.; Zhou, C.; Qiao, M.; Li, X.; Chen, X. Interleukin-10 Is a Promising Marker for Immune-Related Adverse Events in Patients with Non-Small Cell Lung Cancer Receiving Immunotherapy. Front. Immunol. 2022, 13, 840313. [Google Scholar] [CrossRef] [PubMed]
- Nemunaitis, J.; Fong, T.; Shabe, P.; Martineau, D.; Ando, D. Comparison of Serum Interleukin-10 (Il-10) Levels between Normal Volunteers and Patients with Advanced Melanoma. Cancer Invest. 2001, 19, 239–247. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Garza, M.T.; Elva, C.-V.D.; Carmen, M.-B. Il10 as Cancer Biomarker. In Translational Research in Cancer; Sivapatham, S., Yeun-Hwa, G., Eds.; IntechOpen: Rijeka, Croatia, 2020. [Google Scholar]
- Tyan, K.; Baginska, J.; Brainard, M.; Giobbie-Hurder, A.; Severgnini, M.; Manos, M.; Haq, R.; Buchbinder, E.I.; Ott, P.A.; Hodi, F.S.; et al. Cytokine Changes During Immune-Related Adverse Events and Corticosteroid Treatment in Melanoma Patients Receiving Immune Checkpoint Inhibitors. Cancer Immunol. Immunother. 2021, 70, 2209–2221. [Google Scholar] [CrossRef] [PubMed]
- Siegel, J.; Totonchy, M.; Damsky, W.; Berk-Krauss, J.; Castiglione, F., Jr.; Sznol, M.; Petrylak, D.P.; Fischbach, N.; Goldberg, S.B.; Decker, R.H.; et al. Bullous Disorders Associated with Anti-Pd-1 and Anti-Pd-L1 Therapy: A Retrospective Analysis Evaluating the Clinical and Histopathologic Features, Frequency, and Impact on Cancer Therapy. J. Am. Acad. Dermatol. 2018, 79, 1081–1088. [Google Scholar] [CrossRef]
- Nelson, C.A.; Singer, S.; Chen, T.; Puleo, A.E.; Lian, C.G.; Wei, E.X.; Giobbie-Hurder, A.; Mostaghimi, A.; LeBoeuf, N.R. Bullous Pemphigoid after Anti-Programmed Death-1 Therapy: A Retrospective Case-Control Study Evaluating Impact on Tumor Response and Survival Outcomes. J. Am. Acad. Dermatol. 2022, 87, 1400–1402. [Google Scholar] [CrossRef]
- Bui, A.N.; Singer, S.; Hirner, J.; Cunningham-Bussel, A.C.; Larocca, C.; Merola, J.F.; Lian, C.G.; LeBoeuf, N.R. De Novo Cutaneous Connective Tissue Disease Temporally Associated with Immune Checkpoint Inhibitor Therapy: A Retrospective Analysis. J. Am. Acad. Dermatol. 2021, 84, 864–869. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Gender/Age a | Melanoma Subtype/Site/Breslow in mm b | BRAF/PD-L1 c | Involved Sites d | Pre-Treatment e | Treatment Group f | Response g | cutAE h | cutAE Subtype i | cutAE Grade j |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 83/F | snSSM/T/1.1 | V600E/unk | CUT | none | PD1-a | R | + | lichenoid dermatitis | 1 |
| 2 | 80/M | NM/HN/1.9 | WT/7% | LN | none | PD1-a | R | + | acantholytic dermatosis | 1 |
| 3 | 81/F | NM/UE/6.8 | WT/2% | CUT, LN | none | PD1-t | R | − | ||
| 4 | 39/M | NM/AN/>8 | V600E/<1% | LN | none | PD1-a | R | − | ||
| 5 | 57/M | uNM/T/2.1 | V600K/1% | LN | none | PD1-a | R | − | ||
| 6 | 66/M | unk/T/1 | WT/<1% | LN, PUL, ST | none | combi | NR | + | acantholytic dermatosis | 1 |
| 7 | 65/M | uNM/HN/1.9 | G466E/2% | CUT, LN | none | combi | R | + | psoriasis | 1 |
| 8 | 38/M | unk/UE/7 | V600E/unk | LN, ST, PUL, HEP, OSS, CUT | DTIC, TT | combi | NR | − | ||
| 9 | 81/M | unk/LE/>8 | WT/0% | LN, OSS | none | PD1-t | NR | − | ||
| 10 | 77/F | snSSM/LE/1.6 | V600K/15% | CUT, LN, ADR, INT | RT, TT | PD1-t | NR | − | ||
| 11 | 68/M | unk/T/>8 | V600E/2% | LN, CUT, HEP, OSS | none | PD1-a | NR | − | ||
| 12 | 64/F | unk/T/0.7 | V600E/6% | LN, PUL | TT | PD1-t | R | − | ||
| 13 | 62/F | ALM/UE/8 | V600E/2% | LN | IFN | PD1-a | NR | − | ||
| 14 | 62/M | PM/T/>8 | V600E/0% | ST, HEP, ADR, PAN, LN, OSS | TT | combi | NR | + | maculopapular exanthema | 2 |
| 15 | 88/F | uALM/UE/>8 | WT/<1% | LN, ADR | RT | PD1-t | R | − | ||
| 16 | 78/M | LMM/HN/0.7 | V600K/2% | LN, SC | none | PD1-t | NR | − | ||
| 17 | 48/M | ALM/UE/2.1 | V600E/20% | LN, CUT | none | PD1-t | NR | − | ||
| 18 | 59/F | ALM/UE/4.9 | WT/unk | CUT | none | PD1-a | NR | − | ||
| 19 | 62/M | uNM/UE/2.5 | WT/1% | CUT | none | PD1-a | R | + | maculopapular exanthema | 1 |
| 20 | 81/M | unk/T/2 | WT/unk | SC, LN, PUL | RT, IFN | PD1-t | R | + | urticaria | 1 |
| 21 | 77/M | uNM/UE/>8 | WT/0% | LN | none | combi | NR | + | acantholytic dermatosis | 1 |
| 22 | 51/F | SSM/T/1.1 | V600E/unk | LN | IFN | PD1-a | R | + | urticaria | 1 |
| 23 | 64/M | SSM/T/2 | WT/0% | LN | none | PD1-a | R | − | ||
| 24 | 51/F | SSM/HN/1.5 | V600E/<1% | LN, SC, ADR, BIL, OSS, ST | IFN | combi | NR | − | ||
| 25 | 84/M | snSSM/T/>8 | WT/2% | PUL | none | combi | NR | − | ||
| 26 | 59/F | NM/T/>8 | V600E/<1% | LN | none | PD1-a | NR | + | lichenoid dermatitis | 1 |
| 27 | 76/M | uNM/T/4.9 | WT/0% | LN | none | PD1-a | R | − | ||
| 28 | 74/M | NM/T/1.3 | V600E/30% | LN | none | PD1-a | NR | − | ||
| 29 | 55/F | NM/UE/1.2 | V600E/0% | LN, CUT, PUL, CER | IFN | combi | R | + | urticaria, maculopapular exanthema | 2, 2 |
| 30 | 68/F | uNM/T/3.2 | WT/60% | LN | none | PD1-a | R | + | psoriasis | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Absmaier-Kijak, M.; Iuliano, C.; Kaesler, S.; Biedermann, T.; Posch, C.; Brockow, K. T-Cell Subtypes and Immune Signatures in Cutaneous Immune-Related Adverse Events in Melanoma Patients under Immune Checkpoint Inhibitor Therapy. Cancers 2024, 16, 1226. https://doi.org/10.3390/cancers16061226
Absmaier-Kijak M, Iuliano C, Kaesler S, Biedermann T, Posch C, Brockow K. T-Cell Subtypes and Immune Signatures in Cutaneous Immune-Related Adverse Events in Melanoma Patients under Immune Checkpoint Inhibitor Therapy. Cancers. 2024; 16(6):1226. https://doi.org/10.3390/cancers16061226
Chicago/Turabian StyleAbsmaier-Kijak, Magdalena, Caterina Iuliano, Susanne Kaesler, Tilo Biedermann, Christian Posch, and Knut Brockow. 2024. "T-Cell Subtypes and Immune Signatures in Cutaneous Immune-Related Adverse Events in Melanoma Patients under Immune Checkpoint Inhibitor Therapy" Cancers 16, no. 6: 1226. https://doi.org/10.3390/cancers16061226
APA StyleAbsmaier-Kijak, M., Iuliano, C., Kaesler, S., Biedermann, T., Posch, C., & Brockow, K. (2024). T-Cell Subtypes and Immune Signatures in Cutaneous Immune-Related Adverse Events in Melanoma Patients under Immune Checkpoint Inhibitor Therapy. Cancers, 16(6), 1226. https://doi.org/10.3390/cancers16061226