
The Impact of Radiofrequency Ablation on Survival Outcomes and Stent Patency in Patients with Unresectable Cholangiocarcinoma: A Systematic Review and Meta-Analysis of Randomized Controlled Trials

 , , , , ,
, , , , ,  , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy and Selection Criteria
2.2. Data Extraction and Statistical Analysis
2.3. Risk-of-Bias Assessment and Sensitivity Analysis
3. Results
3.1. Study Selection and Baseline Characteristics
3.2. Pooled Analysis of All Studies
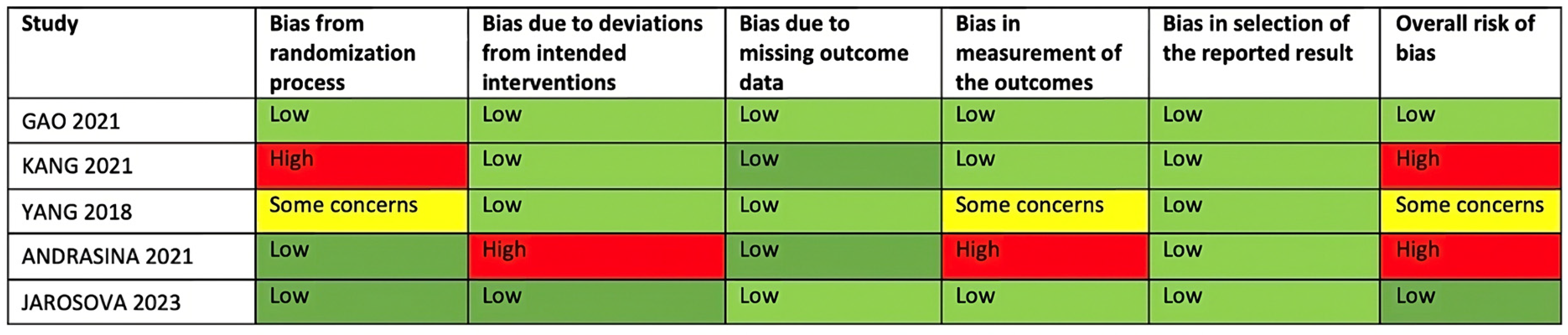
3.3. Quality Assessment
3.4. Sensitivity Analyses and Investigation of Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- Razumilava, N.; Gores, G.J. Classification, Diagnosis, and Management of Cholangiocarcinoma. Clin. Gastroenterol. Hepatol. 2013, 11, 13–21.e1. [Google Scholar] [CrossRef]
- Almadi, M.A.; Barkun, A.; Martel, M. Plastic vs. Self-Expandable Metal Stents for Palliation in Malignant Biliary Obstruction: A Series of Meta-Analyses. Am. J. Gastroenterol. 2017, 112, 260–273. [Google Scholar] [CrossRef]
- Walter, D.; Van Boeckel, P.G.A.; Groenen, M.J.M.; Weusten, B.L.A.M.; Witteman, B.J.; Tan, G.; Brink, M.A.; Nicolai, J.; Tan, A.C.; Alderliesten, J.; et al. Higher Quality of Life after Metal Stent Placement Compared with Plastic Stent Placement for Malignant Extrahepatic Bile Duct Obstruction: A Randomized Controlled Trial. Eur. J. Gastroenterol. Hepatol. 2017, 29, 231–237. [Google Scholar] [CrossRef]
- Shah, T.; Desai, S.; Haque, M.; Dakik, H.; Fisher, D. Management of Occluded Metal Stents in Malignant Biliary Obstruction: Similar Outcomes with Second Metal Stents Compared to Plastic Stents. Dig. Dis. Sci. 2012, 57, 2765–2773. [Google Scholar] [CrossRef]
- Inoue, T.; Yoneda, M. Recent Updates on Local Ablative Therapy Combined with Chemotherapy for Extrahepatic Cholangiocarcinoma: Photodynamic Therapy and Radiofrequency Ablation. Curr. Oncol. 2023, 30, 2159. [Google Scholar] [CrossRef]
- Uyanık, S.A.; Öğüşlü, U.; Yılmaz, B.; Çevik, H.; Atlı, E.; Gümüş, B. Percutaneous Intraductal Microwave Ablation of Malignant Biliary Strictures: Initial Experience. Am. J. Roentgenol. 2020, 215, 753–759. [Google Scholar] [CrossRef]
- Iasiello, M.; Andreozzi, A.; Bianco, N.; Vafai, K. Effects of Pulsed Radiofrequency Source on Cardiac Ablation. Bioengineering 2023, 10, 227. [Google Scholar] [CrossRef]
- Gupta, P.R.; Ghosh, P.; Sarkar, J. Effects of Probe Parameters on Radio-Frequency Ablation of Localized Liver Cancer Using a Personalized Patient Treatment Planning. Therm. Sci. Eng. Prog. 2023, 46, 102236. [Google Scholar] [CrossRef]
- Owen, M.; Makary, M.S.; Beal, E.W. Locoregional Therapy for Intrahepatic Cholangiocarcinoma. Cancers 2023, 15, 2384. [Google Scholar] [CrossRef] [PubMed]
- Inoue, T.; Naitoh, I.; Kitano, R.; Ibusuki, M.; Kobayashi, Y.; Sumida, Y.; Nakade, Y.; Ito, K.; Yoneda, M. Endobiliary Radiofrequency Ablation Combined with Gemcitabine and Cisplatin in Patients with Unresectable Extrahepatic Cholangiocarcinoma. Curr. Oncol. 2022, 29, 2240–2251. [Google Scholar] [CrossRef] [PubMed]
- Montori, M.; Scorzoni, C.; Argenziano, M.E.; Balducci, D.; De Blasio, F.; Martini, F.; Buono, T.; Benedetti, A.; Marzioni, M.; Maroni, L. Cancer-Associated Fibroblasts in Cholangiocarcinoma: Current Knowledge and Possible Implications for Therapy. J. Clin. Med. 2022, 11, 6498. [Google Scholar] [CrossRef]
- Inoue, T.; Yoneda, M. Updated Evidence on the Clinical Impact of Endoscopic Radiofrequency Ablation in the Treatment of Malignant Biliary Obstruction. Dig. Endosc. 2022, 34, 345–358. [Google Scholar] [CrossRef]
- Cho, J.H.; Jeong, S.; Kim, E.J.; Kim, J.M.; Kim, Y.S.; Lee, D.H. Long-Term Results of Temperature-Controlled Endobiliary Radiofrequency Ablation in a Normal Swine Model. Gastrointest. Endosc. 2018, 87, 1147–1150. [Google Scholar] [CrossRef]
- Rustagi, T.; Jamidar, P.A. Intraductal Radiofrequency Ablation for Management of Malignant Biliary Obstruction. Dig. Dis. Sci. 2014, 59, 2635–2641. [Google Scholar] [CrossRef]
- Wadsworth, C.A.; Westaby, D.; Khan, S.A. Endoscopic Radiofrequency Ablation for Cholangiocarcinoma. Curr. Opin. Gastroenterol. 2013, 29, 305–311. [Google Scholar] [CrossRef]
- Kang, H.; Han, S.Y.; Cho, J.H.; Kim, E.J.; Kim, D.U.; Yang, J.K.; Jeon, S.; Park, G.; Lee, T.H. Efficacy and Safety of Temperature-Controlled Intraductal Radiofrequency Ablation in Advanced Malignant Hilar Biliary Obstruction: A Pilot Multicenter Randomized Comparative Trial. J. Hepatobiliary Pancreat. Sci. 2022, 29, 469–478. [Google Scholar] [CrossRef]
- Yang, J.; Wang, J.; Zhou, H.; Zhou, Y.; Wang, Y.; Jin, H.; Lou, Q.; Zhang, X. Efficacy and Safety of Endoscopic Radiofrequency Ablation for Unresectable Extrahepatic Cholangiocarcinoma: A Randomized Trial. Endoscopy 2018, 50, 751–760. [Google Scholar] [CrossRef]
- Gao, D.J.; Yang, J.F.; Ma, S.R.; Wu, J.; Wang, T.T.; Jin, H.B.; Xia, M.X.; Zhang, Y.C.; Shen, H.Z.; Ye, X.; et al. Endoscopic Radiofrequency Ablation plus Plastic Stent Placement versus Stent Placement Alone for Unresectable Extrahepatic Biliary Cancer: A Multicenter Randomized Controlled Trial. Gastrointest. Endosc. 2021, 94, 91–100.e2. [Google Scholar] [CrossRef]
- Jarosova, J.; Zarivnijova, L.; Cibulkova, I.; Mares, J.; Macinga, P.; Hujova, A.; Falt, P.; Urban, O.; Hajer, J.; Spicak, J.; et al. Endoluminal Radiofrequency Ablation in Patients with Malignant Biliary Obstruction: A Randomised Trial. Gut 2023, 72, 2286–2293. [Google Scholar] [CrossRef] [PubMed]
- Andrasina, T.; Rohan, T.; Panek, J.; Kovalcikova, P.; Kunovsky, L.; Ostrizkova, L.; Valek, V. The Combination of Endoluminal Radiofrequency Ablation and Metal Stent Implantation for the Treatment of Malignant Biliary Stenosis—Randomized Study. Eur. J. Radiol. 2021, 142, 109830. [Google Scholar] [CrossRef] [PubMed]
- de Jong, D.M.; Fritzsche, J.A.; Audhoe, A.S.; Yi, S.S.L.; Bruno, M.J.; Voermans, R.P.; van Driel, L.M.J.W. Comparison of Intraductal RFA Plus Stent versus Stent-Only Treatment for Unresectable Perihilar Cholangiocarcinoma-A Systematic Review and Meta-Analysis. Cancers 2022, 14, 2079. [Google Scholar] [CrossRef] [PubMed]
- Song, S.; Jin, H.; Cheng, Q.; Gong, S.; Lv, K.; Lei, T.; Tian, H.; Li, X.; Lei, C.; Yang, W.; et al. Local Palliative Therapies for Unresectable Malignant Biliary Obstruction: Radiofrequency Ablation Combined with Stent or Biliary Stent Alone? An Updated Meta-Analysis of Nineteen Trials. Surg. Endosc. 2022, 36, 5559–5570. [Google Scholar] [CrossRef]
- Cha, B.H.; Jang, M.J.; Lee, S.H. Survival Benefit of Intraductal Radiofrequency Ablation for Malignant Biliary Obstruction: A Systematic Review with Meta-Analysis. Clin. Endosc. 2021, 54, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Sofi, A.A.; Khan, M.A.; Das, A.; Sachdev, M.; Khuder, S.; Nawras, A.; Lee, W. Radiofrequency Ablation Combined with Biliary Stent Placement versus Stent Placement Alone for Malignant Biliary Strictures: A Systematic Review and Meta-Analysis. Gastrointest. Endosc. 2018, 87, 944–951.e1. [Google Scholar] [CrossRef] [PubMed]
- Rebhun, J.; Shin, C.M.; Siddiqui, U.D.; Villa, E. Endoscopic Biliary Treatment of Unresectable Cholangiocarcinoma: A Meta-Analysis of Survival Outcomes and Systematic Review. World J. Gastrointest. Endosc. 2023, 15, 177. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. BMJ 2009, 339, 332–336. [Google Scholar] [CrossRef] [PubMed]
- Parmar, M.K.; Torri, V.; Stewart, L. Extracting Summary Statistics to Perform Meta-analyses of the Published Literature for Survival Endpoints. Stat. Med. 1998, 17, 2815–2834. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in Meta-Analysis Detected by a Simple, Graphical Test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Hänsler, J.; Wissniowski, T.T.; Schuppan, D.; Witte, A.; Bernatik, T.; Hahn, E.G.; Strobel, D. Activation and Dramatically Increased Cytolytic Activity of Tumor Specific T Lymphocytes after Radio-Frequency Ablation in Patients with Hepatocellular Carcinoma and Colorectal Liver Metastases. World J. Gastroenterol. 2006, 12, 3716–3721. [Google Scholar] [CrossRef]
- Liu, X.; Qin, S. Immune Checkpoint Inhibitors in Hepatocellular Carcinoma: Opportunities and Challenges. Oncologist 2019, 24, S3–S10. [Google Scholar] [CrossRef] [PubMed]
- Albers, D.; Schmidt, A.; Schiemer, M.; Caca, K.; Wannhoff, A.; Sauer, P.; Wiesweg, M.; Schumacher, B.; Dechene, A. Impact of Endobiliary Radiofrequency Ablation on Biliary Drainage in Patients with Malignant Biliary Strictures Treated with Uncovered Self-Expandable Metal Stents: A Randomized Controlled Multicenter Trial. Gastrointest. Endosc. 2022, 96, 970–979. [Google Scholar] [CrossRef]
- Sharaiha, R.Z.; Natov, N.; Glockenberg, K.S.; Widmer, J.; Gaidhane, M.; Kahaleh, M. Comparison of Metal Stenting with Radiofrequency Ablation versus Stenting Alone for Treating Malignant Biliary Strictures: Is There an Added Benefit? Dig. Dis. Sci. 2014, 59, 3099–3102. [Google Scholar] [CrossRef] [PubMed]
- Kallis, Y.; Phillips, N.; Steel, A.; Kaltsidis, H.; Vlavianos, P.; Habib, N.; Westaby, D. Analysis of Endoscopic Radiofrequency Ablation of Biliary Malignant Strictures in Pancreatic Cancer Suggests Potential Survival Benefit. Dig. Dis. Sci. 2015, 60, 3449–3455. [Google Scholar] [CrossRef] [PubMed]
- Bokemeyer, A.; Matern, P.; Bettenworth, D.; Cordes, F.; Nowacki, T.M.; Heinzow, H.; Kabar, I.; Schmidt, H.; Ullerich, H.; Lenze, F. Endoscopic Radiofrequency Ablation Prolongs Survival of Patients with Unresectable Hilar Cholangiocellular Carcinoma—A Case-Control Study. Sci. Rep. 2019, 9, 13685. [Google Scholar] [CrossRef]
- Matheus de Oliveira Veras, A.; Turiani Hourneaux de Moura, D.; McCarty, T.R.; Henrique Peixoto de Oliveira, G.; Sérgio Araújo Gomes, R.; Lucena Landim, D.; Giacobo Nunes, F.; Antônio Prince Franzini, T.; Eduardo Lera dos Santos, M.; Marques Bernardo, W.; et al. Intraductal Radiofrequency Ablation plus Biliary Stent versus Stent Alone for Malignant Biliary Obstruction: A Systematic Review and Meta-Analysis. Endosc. Int. Open 2024, 12, E23–E33. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Country | Number of Patients | Age † (years) | Female Sex, n (%) | Tumor Location, n (%) | Type of Stent | Technique |
|---|---|---|---|---|---|---|---|
| Yang, 2018 [17] | China | 65 | 62 | 32 (49) | Bismuth I–II: 19 (29) Distal: 46 (71) | Plastic | Endoscopic |
| Andrasina, 2021 [20] | Czech Republic | 43 | 66 | 17 (40) | Bismuth II: 7 (16) IIIa: 15 (35) IIIb: 3 (7) IV: 18 (42) | Metal | Percutaneous |
| Gao, 2021 [18] | China | 147 | 68 * | 85 (49) * | Bismuth I: 18 (12) II: 16 (11) III: 13 (9) Distal: 100 (68) | Plastic | Endoscopic |
| Kang, 2022 [16] | South Korea | 30 | 72 | 10 (33) | Bismuth II: 5 (16) IIIa: 8 (27) IIIb: 6 (20) IV: 11 (37) | Plastic | Endoscopic |
| Jarosova, 2023 [19] | Czech Republic | 85 | 70 | 33 (39) | Bismuth I: 9 (11) II: 14 (16) III: 28 (33) IV: 22 (26) Distal: 12 (14) | Metal/plastic | Endoscopic |
| Participants (Studies) Follow-Up | Risk of Bias | Inconsistency | Indirectness | Imprecision | Publication Bias | Overall Certainty of Evidence | Relative Effect (95% CI) | Comments |
|---|---|---|---|---|---|---|---|---|
| Overall survival | ||||||||
| 370 (5 RCTs) | very serious a | not serious | not serious | serious b | none | ⨁◯◯◯ Very low | HR 0.62 (0.36 to 1.07) | The evidence about the effect of RFA is very uncertain. The RFA has little to no effect on overall survival, but the evidence is very uncertain. |
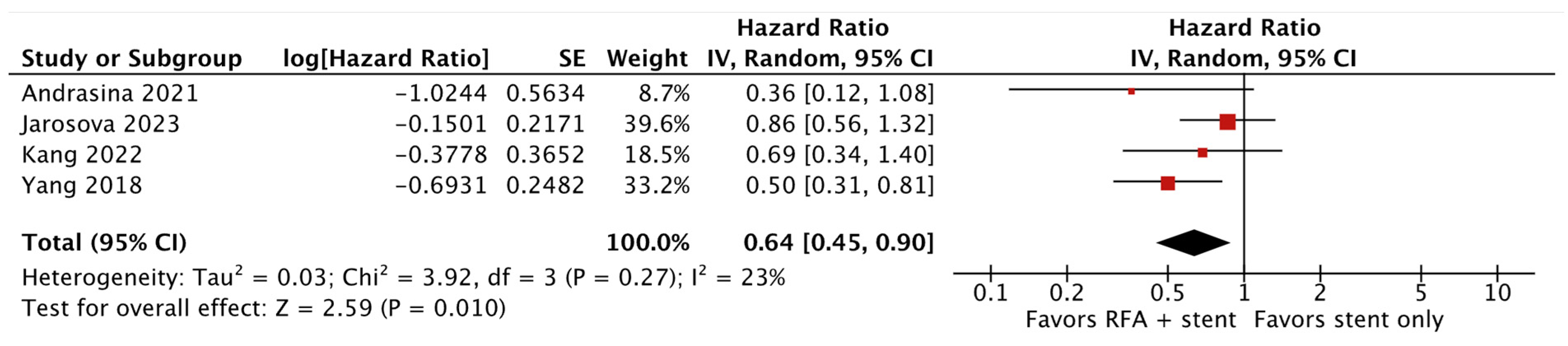
| Patency | ||||||||
| 222 (4 RCTs) | very serious a | not serious | not serious | not serious | none | ⨁⨁◯◯ Low | HR 0.64 (0.45 to 0.90) | The evidence suggests that RFA results in a slight increase in stent patency. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balducci, D.; Montori, M.; Martini, F.; Valvano, M.; De Blasio, F.; Argenziano, M.E.; Tarantino, G.; Benedetti, A.; Bendia, E.; Marzioni, M.; et al. The Impact of Radiofrequency Ablation on Survival Outcomes and Stent Patency in Patients with Unresectable Cholangiocarcinoma: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Cancers 2024, 16, 1372. https://doi.org/10.3390/cancers16071372
Balducci D, Montori M, Martini F, Valvano M, De Blasio F, Argenziano ME, Tarantino G, Benedetti A, Bendia E, Marzioni M, et al. The Impact of Radiofrequency Ablation on Survival Outcomes and Stent Patency in Patients with Unresectable Cholangiocarcinoma: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Cancers. 2024; 16(7):1372. https://doi.org/10.3390/cancers16071372
Chicago/Turabian StyleBalducci, Daniele, Michele Montori, Francesco Martini, Marco Valvano, Federico De Blasio, Maria Eva Argenziano, Giuseppe Tarantino, Antonio Benedetti, Emanuele Bendia, Marco Marzioni, and et al. 2024. "The Impact of Radiofrequency Ablation on Survival Outcomes and Stent Patency in Patients with Unresectable Cholangiocarcinoma: A Systematic Review and Meta-Analysis of Randomized Controlled Trials" Cancers 16, no. 7: 1372. https://doi.org/10.3390/cancers16071372
APA StyleBalducci, D., Montori, M., Martini, F., Valvano, M., De Blasio, F., Argenziano, M. E., Tarantino, G., Benedetti, A., Bendia, E., Marzioni, M., & Maroni, L. (2024). The Impact of Radiofrequency Ablation on Survival Outcomes and Stent Patency in Patients with Unresectable Cholangiocarcinoma: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Cancers, 16(7), 1372. https://doi.org/10.3390/cancers16071372