
Prognostic Value of PCSK9 Levels in Premenopausal Women at Risk of Breast Cancer—Evidence from a 17-Year Follow-Up Study

 , ,
, ,  , , , , ,
, , , , ,  , , , , , and
, , , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Assay Methods
2.3. Statistical Analysis
3. Results
3.1. Baseline Patient Characteristics
3.2. Correlation Analyses
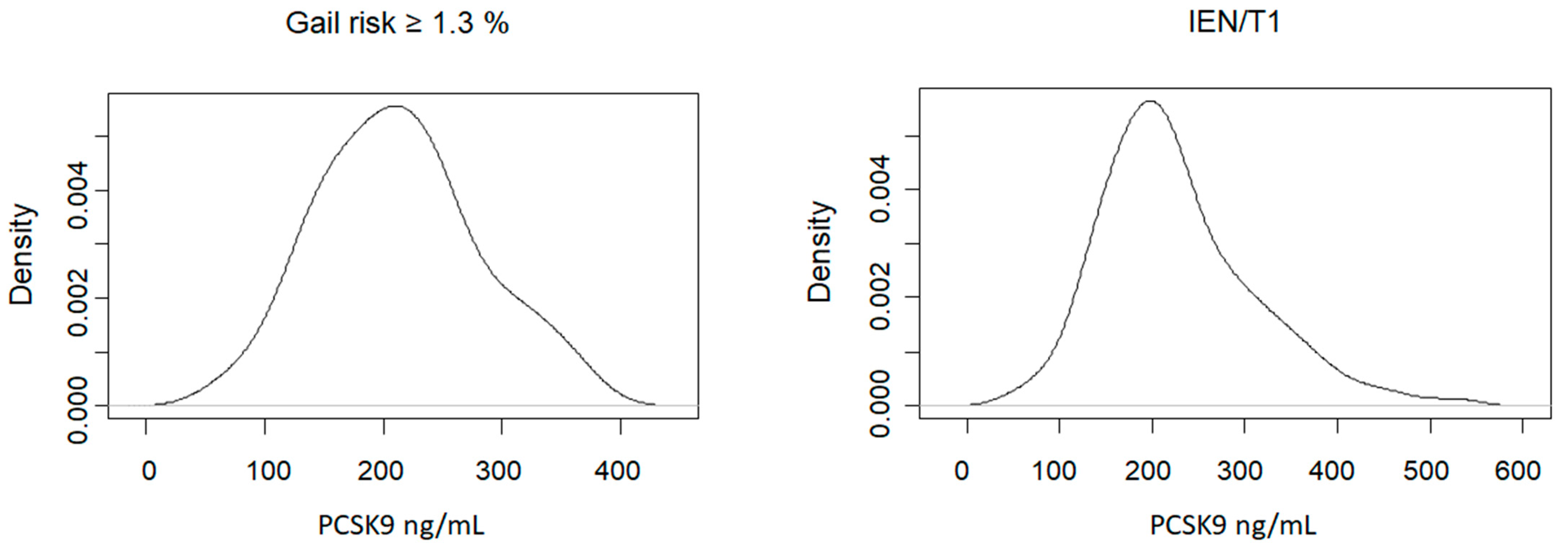
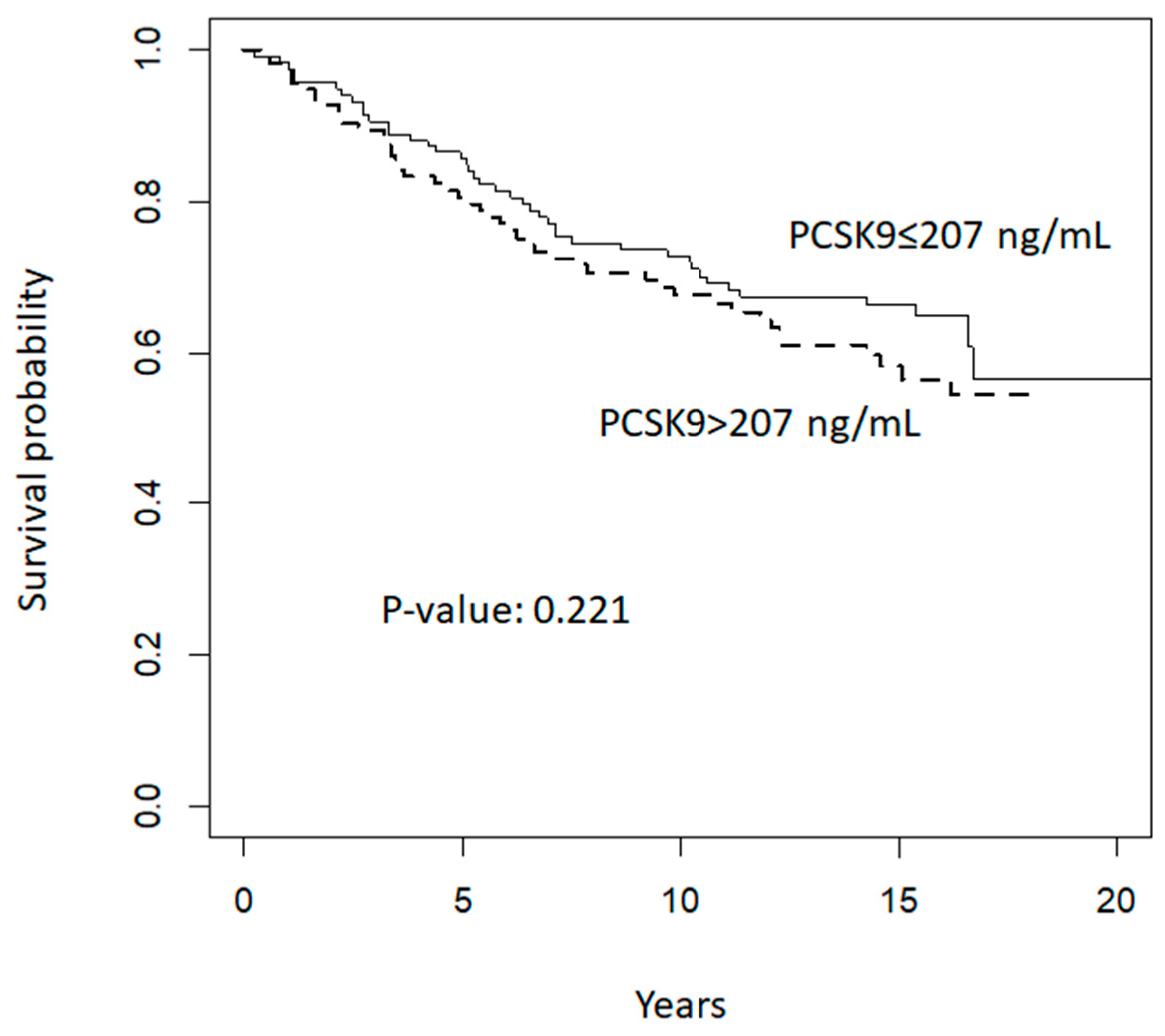
3.3. Prognostic Value of Plasma Levels of PCSK9
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Heer, E.; Harper, A.; Escandor, N.; Sung, H.; McCormack, V.; Fidler-Benaoudia, M.M. Global burden and trends in premenopausal and postmenopausal breast cancer: A population-based study. Lancet Glob. Health 2020, 8, e1027–e1037. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Lv, M.; Zhang, W.; Zhan, Q. Dysregulation of cholesterol metabolism in cancer progression. Oncogene 2023, 42, 3289–3302. [Google Scholar] [CrossRef]
- Gomaraschi, M. Role of Lipoproteins in the Microenvironment of Hormone-Dependent Cancers. Trends Endocrinol. Metab. 2020, 31, 256–268. [Google Scholar] [CrossRef] [PubMed]
- Cruz, P.M.; Mo, H.; McConathy, W.J.; Sabnis, N.; Lacko, A.G. The role of cholesterol metabolism and cholesterol transport in carcinogenesis: A review of scientific findings, relevant to future cancer therapeutics. Front. Pharmacol. 2013, 4, 119. [Google Scholar] [CrossRef] [PubMed]
- Touvier, M.; Fassier, P.; His, M.; Norat, T.; Chan, D.S.; Blacher, J.; Hercberg, S.; Galan, P.; Druesne-Pecollo, N.; Latino-Martel, P. Cholesterol and breast cancer risk: A systematic review and meta-analysis of prospective studies. Br. J. Nutr. 2015, 114, 347–357. [Google Scholar] [CrossRef]
- Borgquist, S.; Butt, T.; Almgren, P.; Shiffman, D.; Stocks, T.; Orho-Melander, M.; Manjer, J.; Melander, O. Apolipoproteins, lipids and risk of cancer. Int. J. Cancer 2016, 138, 2648–2656. [Google Scholar] [CrossRef]
- Seidah, N.G.; Garcon, D. Expanding Biology of PCSK9: Roles in Atherosclerosis and Beyond. Curr. Atheroscler. Rep. 2022, 24, 821–830. [Google Scholar] [CrossRef]
- Seidah, N.G.; Benjannet, S.; Wickham, L.; Marcinkiewicz, J.; Jasmin, S.B.; Stifani, S.; Basak, A.; Prat, A.; Chretien, M. The secretory proprotein convertase neural apoptosis-regulated convertase 1 (NARC-1): Liver regeneration and neuronal differentiation. Proc. Natl. Acad. Sci. USA 2003, 100, 928–933. [Google Scholar] [CrossRef]
- Artenstein, A.W.; Opal, S.M. Proprotein convertases in health and disease. N. Engl. J. Med. 2011, 365, 2507–2518. [Google Scholar] [CrossRef]
- Luo, Y.; Warren, L.; Xia, D.; Jensen, H.; Sand, T.; Petras, S.; Qin, W.; Miller, K.S.; Hawkins, J. Function and distribution of circulating human PCSK9 expressed extrahepatically in transgenic mice. J. Lipid Res. 2009, 50, 1581–1588. [Google Scholar] [CrossRef]
- Bordicchia, M.; Spannella, F.; Ferretti, G.; Bacchetti, T.; Vignini, A.; Di Pentima, C.; Mazzanti, L.; Sarzani, R. PCSK9 is Expressed in Human Visceral Adipose Tissue and Regulated by Insulin and Cardiac Natriuretic Peptides. Int. J. Mol. Sci. 2019, 20, 245. [Google Scholar] [CrossRef]
- Bhattacharya, A.; Chowdhury, A.; Chaudhury, K.; Shukla, P.C. Proprotein convertase subtilisin/kexin type 9 (PCSK9): A potential multifaceted player in cancer. Biochim. Biophys. Acta Rev. Cancer 2021, 1876, 188581. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Bao, X.; Hu, M.; Chang, H.; Jiao, M.; Cheng, J.; Xie, L.; Huang, Q.; Li, F.; Li, C.Y. Inhibition of PCSK9 potentiates immune checkpoint therapy for cancer. Nature 2020, 588, 693–698. [Google Scholar] [CrossRef]
- Wong Chong, E.; Joncas, F.H.; Seidah, N.G.; Calon, F.; Diorio, C.; Gangloff, A. Circulating levels of PCSK9, ANGPTL3 and Lp(a) in stage III breast cancers. BMC Cancer 2022, 22, 1049. [Google Scholar] [CrossRef]
- Nowak, C.; Arnlov, J. A Mendelian randomization study of the effects of blood lipids on breast cancer risk. Nat. Commun. 2018, 9, 3957. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Ding, H.; Jia, Y.; Shi, M.; Guo, D.; Yang, P.; Wang, Y.; Liu, F.; Zhang, Y.; Zhu, Z. Associations of genetically proxied inhibition of HMG-CoA reductase, NPC1L1, and PCSK9 with breast cancer and prostate cancer. Breast Cancer Res. 2022, 24, 12. [Google Scholar] [CrossRef]
- Decensi, A.; Robertson, C.; Guerrieri-Gonzaga, A.; Serrano, D.; Cazzaniga, M.; Mora, S.; Gulisano, M.; Johansson, H.; Galimberti, V.; Cassano, E.; et al. Randomized double-blind 2 × 2 trial of low-dose tamoxifen and fenretinide for breast cancer prevention in high-risk premenopausal women. J. Clin. Oncol. 2009, 27, 3749–3756. [Google Scholar] [CrossRef]
- Macis, D.; Gandini, S.; Guerrieri-Gonzaga, A.; Johansson, H.; Magni, P.; Ruscica, M.; Lazzeroni, M.; Serrano, D.; Cazzaniga, M.; Mora, S.; et al. Prognostic effect of circulating adiponectin in a randomized 2 × 2 trial of low-dose tamoxifen and fenretinide in premenopausal women at risk for breast cancer. J. Clin. Oncol. 2012, 30, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Johansson, H.; Bonanni, B.; Gandini, S.; Guerrieri-Gonzaga, A.; Cazzaniga, M.; Serrano, D.; Macis, D.; Puccio, A.; Sandri, M.T.; Gulisano, M.; et al. Circulating hormones and breast cancer risk in premenopausal women: A randomized trial of low-dose tamoxifen and fenretinide. Breast Cancer Res. Treat. 2013, 142, 569–578. [Google Scholar] [CrossRef]
- Macchi, C.; Iodice, S.; Persico, N.; Ferrari, L.; Cantone, L.; Greco, M.F.; Ischia, B.; Dozio, E.; Corsini, A.; Sirtori, C.R.; et al. Maternal exposure to air pollutants, PCSK9 levels, fetal growth and gestational age—An Italian cohort. Environ. Int. 2021, 149, 106163. [Google Scholar] [CrossRef]
- Decensi, A.; Bonanni, B.; Baglietto, L.; Guerrieri-Gonzaga, A.; Ramazzotto, F.; Johansson, H.; Robertson, C.; Marinucci, I.; Mariette, F.; Sandri, M.T.; et al. A two-by-two factorial trial comparing oral with transdermal estrogen therapy and fenretinide with placebo on breast cancer biomarkers. Clin. Cancer Res. 2004, 10, 4389–4397. [Google Scholar] [CrossRef] [PubMed]
- Johansson, H.; Gandini, S.; Guerrieri-Gonzaga, A.; Iodice, S.; Ruscica, M.; Bonanni, B.; Gulisano, M.; Magni, P.; Formelli, F.; Decensi, A. Effect of fenretinide and low-dose tamoxifen on insulin sensitivity in premenopausal women at high risk for breast cancer. Cancer Res. 2008, 68, 9512–9518. [Google Scholar] [CrossRef] [PubMed]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Sun, C.; Zhu, G.; Shen, C.; Huang, S.; Li, R.; Li, J.; Ma, Z.; Wang, Z. Identification and validation of PCSK9 as a prognostic and immune-related influencing factor in tumorigenesis: A pan-cancer analysis. Front. Oncol. 2023, 13, 1134063. [Google Scholar] [CrossRef] [PubMed]
- Momtazi-Borojeni, A.A.; Nik, M.E.; Jaafari, M.R.; Banach, M.; Sahebkar, A. Effects of immunization against PCSK9 in an experimental model of breast cancer. Arch. Med. Sci. 2019, 15, 570–579. [Google Scholar] [CrossRef] [PubMed]
- Bao, X.; Liang, Y.; Chang, H.; Cai, T.; Feng, B.; Gordon, K.; Zhu, Y.; Shi, H.; He, Y.; Xie, L. Targeting proprotein convertase subtilisin/kexin type 9 (PCSK9): From bench to bedside. Signal Transduct. Target. Ther. 2024, 9, 13. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Guo, Q.; Wang, M.; Liu, C.; Tian, Z. PCSK9 promotes tumor cell proliferation and migration by facilitating CCL25 secretion in esophageal squamous cell carcinoma. Oncol. Lett. 2023, 26, 500. [Google Scholar] [CrossRef] [PubMed]
- Yang, Q.C.; Wang, S.; Liu, Y.T.; Song, A.; Wu, Z.Z.; Wan, S.C.; Li, H.M.; Sun, Z.J. Targeting PCSK9 reduces cancer cell stemness and enhances antitumor immunity in head and neck cancer. iScience 2023, 26, 106916. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.Z.; Zhu, X.D.; Feng, L.H.; Li, X.L.; Liu, X.F.; Sun, H.C.; Tang, Z.Y. PCSK9 promotes tumor growth by inhibiting tumor cell apoptosis in hepatocellular carcinoma. Exp. Hematol. Oncol. 2021, 10, 25. [Google Scholar] [CrossRef]
- Wang, L.; Li, S.; Luo, H.; Lu, Q.; Yu, S. PCSK9 promotes the progression and metastasis of colon cancer cells through regulation of EMT and PI3K/AKT signaling in tumor cells and phenotypic polarization of macrophages. J. Exp. Clin. Cancer Res. 2022, 41, 303. [Google Scholar] [CrossRef]
- Xu, B.; Li, S.; Fang, Y.; Zou, Y.; Song, D.; Zhang, S.; Cai, Y. Proprotein Convertase Subtilisin/Kexin Type 9 Promotes Gastric Cancer Metastasis and Suppresses Apoptosis by Facilitating MAPK Signaling Pathway Through HSP70 Up-Regulation. Front. Oncol. 2020, 10, 609663. [Google Scholar] [CrossRef] [PubMed]
- Ruscica, M.; Ricci, C.; Macchi, C.; Magni, P.; Cristofani, R.; Liu, J.; Corsini, A.; Ferri, N. Suppressor of Cytokine Signaling-3 (SOCS-3) Induces Proprotein Convertase Subtilisin Kexin Type 9 (PCSK9) Expression in Hepatic HepG2 Cell Line. J. Biol. Chem. 2016, 291, 3508–3519. [Google Scholar] [CrossRef] [PubMed]
- Seidah, N.G. The PCSK9 discovery, an inactive protease with varied functions in hypercholesterolemia, viral infections, and cancer. J. Lipid Res. 2021, 62, 100130. [Google Scholar] [CrossRef]
- Ooi, T.C.; Raymond, A.; Cousins, M.; Favreau, C.; Taljaard, M.; Gavin, C.; Jolly, E.E.; Malone, S.; Eapen, L.; Chretien, M.; et al. Relationship between testosterone, estradiol and circulating PCSK9: Cross-sectional and interventional studies in humans. Clin. Chim. Acta 2015, 446, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, M.; Galman, C.; Rudling, M.; Angelin, B. Influence of physiological changes in endogenous estrogen on circulating PCSK9 and LDL cholesterol. J. Lipid Res. 2015, 56, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Persson, L.; Henriksson, P.; Westerlund, E.; Hovatta, O.; Angelin, B.; Rudling, M. Endogenous estrogens lower plasma PCSK9 and LDL cholesterol but not Lp(a) or bile acid synthesis in women. Arterioscler. Thromb. Vasc. Biol. 2012, 32, 810–814. [Google Scholar] [CrossRef] [PubMed]
- Lakoski, S.G.; Lagace, T.A.; Cohen, J.C.; Horton, J.D.; Hobbs, H.H. Genetic and metabolic determinants of plasma PCSK9 levels. J. Clin. Endocrinol. Metab. 2009, 94, 2537–2543. [Google Scholar] [CrossRef]
- Peticca, P.; Raymond, A.; Gruslin, A.; Cousins, M.; Adetola, E.; Abujrad, H.; Mayne, J.; Ooi, T.C. Human Serum PCSK9 Is Elevated at Parturition in Comparison to Nonpregnant Subjects While Serum PCSK9 from Umbilical Cord Blood is Lower Compared to Maternal Blood. ISRN Endocrinol. 2013, 2013, 341632. [Google Scholar] [CrossRef] [PubMed]
- Maarouf, N.; Chen, Y.X.; Shi, C.; Deng, J.; Diao, C.; Rosin, M.; Shrivastava, V.; Batulan, Z.; Liu, J.; O’Brien, E.R. Unlike estrogens that increase PCSK9 levels post-menopause HSP27 vaccination lowers cholesterol levels and atherogenesis due to divergent effects on PCSK9 and LDLR. Pharmacol. Res. 2020, 161, 105222. [Google Scholar] [CrossRef]
- Blom, D.J.; Djedjos, C.S.; Monsalvo, M.L.; Bridges, I.; Wasserman, S.M.; Scott, R.; Roth, E. Effects of Evolocumab on Vitamin E and Steroid Hormone Levels: Results From the 52-Week, Phase 3, Double-Blind, Randomized, Placebo-Controlled DESCARTES Study. Circ. Res. 2015, 117, 731–741. [Google Scholar] [CrossRef]
- Blom, D.J.; Chen, J.; Yuan, Z.; Borges, J.L.C.; Monsalvo, M.L.; Wang, N.; Hamer, A.W.; Ge, J. Effects of evolocumab therapy and low LDL-C levels on vitamin E and steroid hormones in Chinese and global patients with type 2 diabetes. Endocrinol. Diabetes Metab. 2020, 3, e00123. [Google Scholar] [CrossRef] [PubMed]
- Nomura, D.K.; Long, J.Z.; Niessen, S.; Hoover, H.S.; Ng, S.W.; Cravatt, B.F. Monoacylglycerol lipase regulates a fatty acid network that promotes cancer pathogenesis. Cell 2010, 140, 49–61. [Google Scholar] [CrossRef] [PubMed]
- Menendez, J.A.; Lupu, R. Fatty acid synthase and the lipogenic phenotype in cancer pathogenesis. Nat. Rev. Cancer 2007, 7, 763–777. [Google Scholar] [CrossRef] [PubMed]
- Narii, N.; Zha, L.; Komatsu, M.; Kitamura, T.; Sobue, T.; Ogawa, T. Cholesterol and breast cancer risk: A cohort study using health insurance claims and health checkup databases. Breast Cancer Res. Treat. 2023, 199, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Johnson, K.E.; Siewert, K.M.; Klarin, D.; Damrauer, S.M.; Program, V.A.M.V.; Chang, K.M.; Tsao, P.S.; Assimes, T.L.; Maxwell, K.N.; Voight, B.F. The relationship between circulating lipids and breast cancer risk: A Mendelian randomization study. PLoS Med. 2020, 17, e1003302. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Yang, X.; Li, Q.; Zeng, P.; Liu, Y.; Liu, L.; Chen, Y.; Yu, M.; Ma, C.; Li, X.; et al. Activation of Adiponectin Receptor Regulates Proprotein Convertase Subtilisin/Kexin Type 9 Expression and Inhibits Lesions in ApoE-Deficient Mice. Arterioscler. Thromb. Vasc. Biol. 2017, 37, 1290–1300. [Google Scholar] [CrossRef] [PubMed]
- Macchi, C.; Greco, M.F.; Botta, M.; Sperandeo, P.; Dongiovanni, P.; Valenti, L.; Cicero, A.F.G.; Borghi, C.; Lupo, M.G.; Romeo, S.; et al. Leptin, Resistin, and Proprotein Convertase Subtilisin/Kexin Type 9: The Role of STAT3. Am. J. Pathol. 2020, 190, 2226–2236. [Google Scholar] [CrossRef]
- Levenson, A.E.; Haas, M.E.; Miao, J.; Brown, R.J.; de Ferranti, S.D.; Muniyappa, R.; Biddinger, S.B. Effect of Leptin Replacement on PCSK9 in ob/ob Mice and Female Lipodystrophic Patients. Endocrinology 2016, 157, 1421–1429. [Google Scholar] [CrossRef] [PubMed]
- Gaskill, B.N.; Garner, J.P. Power to the People: Power, Negative Results and Sample Size. J. Am. Assoc. Lab. Anim. Sci. 2020, 59, 9–16. [Google Scholar] [CrossRef]
- Cohen, J.C.; Boerwinkle, E.; Mosley, T.H., Jr.; Hobbs, H.H. Sequence variations in PCSK9, low LDL, and protection against coronary heart disease. N. Engl. J. Med. 2006, 354, 1264–1272. [Google Scholar] [CrossRef]
- Park, S.W.; Moon, Y.A.; Horton, J.D. Post-transcriptional regulation of low density lipoprotein receptor protein by proprotein convertase subtilisin/kexin type 9a in mouse liver. J. Biol. Chem. 2004, 279, 50630–50638. [Google Scholar] [CrossRef] [PubMed]
- Ferri, N.; Ruscica, M.; Coggi, D.; Bonomi, A.; Amato, M.; Frigerio, B.; Sansaro, D.; Ravani, A.; Veglia, F.; Capra, N.; et al. Sex-specific predictors of PCSK9 levels in a European population: The IMPROVE study. Atherosclerosis 2020, 309, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Ruscica, M.; Macchi, C.; Giuliani, A.; Rizzuto, A.S.; Ramini, D.; Sbriscia, M.; Carugo, S.; Bonfigli, A.R.; Corsini, A.; Olivieri, F.; et al. Circulating PCSK9 as a prognostic biomarker of cardiovascular events in individuals with type 2 diabetes: Evidence from a 16.8-year follow-up study. Cardiovasc. Diabetol. 2023, 22, 222. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | 5-Year Gail Risk ≥ 1.3% (n = 54) | IEN, T1 (n = 181) | p-Value |
|---|---|---|---|
| Age, y | 46 (43, 49) | 46 (42, 49) | 0.868 |
| BMI, kg/m2 | 22 (21, 25) | 23 (21, 25) | 0.524 |
| Percentage mammographic density | 49.9 (38.4, 61.1) | 46.3 (35.3, 58.3) | 0.312 |
| PCSK9, ng/mL | 206 (161–250) | 207 (172–263) | 0.554 |
| 17 β-estradiol, pg/mL | 142.3 (94.4, 232.7) | 121.7 (72.3, 188) | 0.118 |
| Total cholesterol, mg/dL | 216 (198, 236) | 208 (185, 234) | 0.158 |
| LDL-C, mg/dL | 130.6 (109.8, 152.4) | 122.3 (103.4, 145.5) | 0.183 |
| HDL-C, mg/dL | 66.5 (61, 79) | 69 (58, 78) | 0.587 |
| Non-HDL-C, mg/dL | 144.5 (125, 168) | 137 (118, 166) | 0.272 |
| Remnant cholesterol, mg/dL | 14 (10.2, 18.6) | 14.4 (11.6, 18.8) | 0.261 |
| Triglycerides, mg/dL | 70 (51, 93) | 72 (58, 94) | 0.258 |
| Leptin, ng/mL | 10.01 (6.16, 16.0) | 10.8 (7.3, 15.6) | 0.497 |
| Adiponectin, μg/mL | 11.99 (8.62, 16.1) | 9.8 (6.9, 13.5) | 0.006 |
| CRP, mg/L | 0.07 (0.04, 0.18) | 0.1 (0.04, 0.21) | 0.192 |
| Glucose, mg/dL | 89 (83, 93) | 88 (83, 94) | 0.927 |
| Insulin, μU/mL | 12.32 (10.38, 15.12) | 14.00 (10.72, 17.5) | 0.048 |
| HOMA-IR | 2.65 (2.14, 3.26) | 3.05 (2.31, 3.80) | 0.047 |
| Univariate Spearman Analysis R Coefficient | |
|---|---|
| BMI, kg/m2 | 0.080 |
| Percentage mammographic density | −0.045 |
| 17 β-estradiol, pg/mL | −0.294 |
| Total cholesterol, mg/dL | 0.277 |
| LDL-C, mg/dL | 0.217 |
| HDL-C, mg/dL | 0.037 |
| Non-HDL-C, mg/dL | 0.256 |
| Remnant cholesterol, mg/dL | 0.237 |
| Triglycerides, mg/dL | 0.238 |
| Leptin, ng/mL | 0.171 |
| Adiponectin, μg/mL | 0.003 |
| CRP, mg/L | 0.166 |
| Glucose, mg/dL | 0.164 |
| Insulin, μU/mL | 0.066 |
| HOMA-IR | 0.092 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruscica, M.; Macchi, C.; Gandini, S.; Macis, D.; Guerrieri-Gonzaga, A.; Aristarco, V.; Serrano, D.; Lazzeroni, M.; Rizzuto, A.S.; Gaeta, A.; et al. Prognostic Value of PCSK9 Levels in Premenopausal Women at Risk of Breast Cancer—Evidence from a 17-Year Follow-Up Study. Cancers 2024, 16, 1411. https://doi.org/10.3390/cancers16071411
Ruscica M, Macchi C, Gandini S, Macis D, Guerrieri-Gonzaga A, Aristarco V, Serrano D, Lazzeroni M, Rizzuto AS, Gaeta A, et al. Prognostic Value of PCSK9 Levels in Premenopausal Women at Risk of Breast Cancer—Evidence from a 17-Year Follow-Up Study. Cancers. 2024; 16(7):1411. https://doi.org/10.3390/cancers16071411
Chicago/Turabian StyleRuscica, Massimiliano, Chiara Macchi, Sara Gandini, Debora Macis, Aliana Guerrieri-Gonzaga, Valentina Aristarco, Davide Serrano, Matteo Lazzeroni, Alessandra Stefania Rizzuto, Aurora Gaeta, and et al. 2024. "Prognostic Value of PCSK9 Levels in Premenopausal Women at Risk of Breast Cancer—Evidence from a 17-Year Follow-Up Study" Cancers 16, no. 7: 1411. https://doi.org/10.3390/cancers16071411