


Growth Charts for Shwachman–Diamond Syndrome at Ages 0 to 18 Years
 , ,
, ,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Recruitment
2.2. Statistical Analysis
3. Results
3.1. Study Population
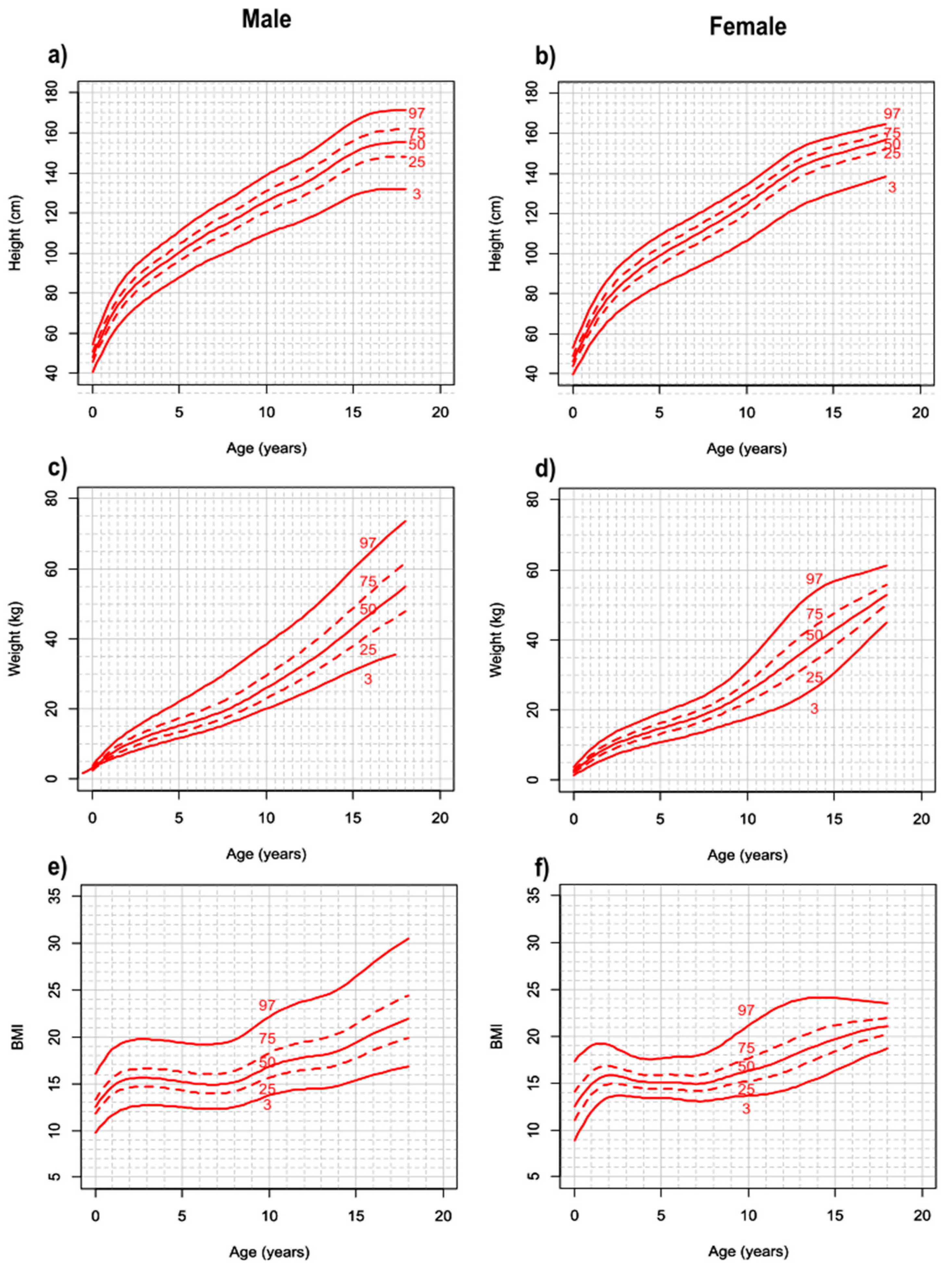
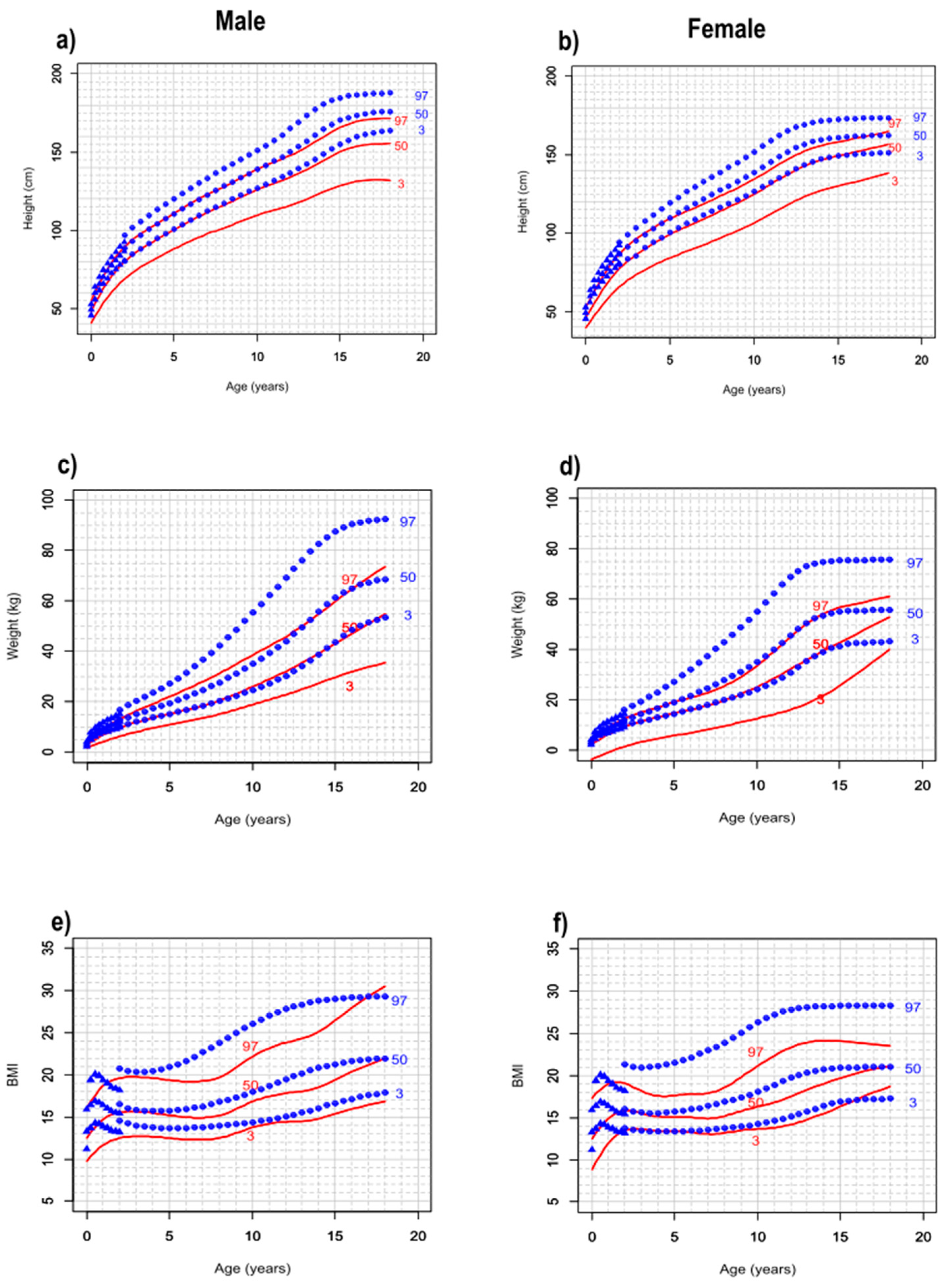
3.2. SDS Percentiles and Growth Charts
3.3. Percentage Changes in Height, Weight, and BMI
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dokal, I.; Vulliamy, T. Inherited bone marrow failure syndromes. Haematologica 2010, 95, 1236–1240. [Google Scholar] [CrossRef] [PubMed]
- Savage, S.A.; Dufour, C. Classical inherited bone marrow failure syndromes with high risk for myelodysplastic syndrome and acute myelogenous leukemia. Semin. Hematol. 2017, 54, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Warren, A.J. Molecular basis of the human ribosomopathy Shwachman-Diamond syndrome. Adv. Biol. Regul. 2018, 67, 109–127. [Google Scholar] [CrossRef] [PubMed]
- Finch, A.J.; Hilcenko, C.; Basse, N.; Drynan, L.F.; Goyenechea, B.; Menne, T.F.; González Fernández, A.; Simpson, P.; D’Santos, C.S.; Arends, M.J.; et al. Uncoupling of GTP hydrolysis from eIF6 release on the ribosome causes Shwachman-Diamond syndrome. Genes. Dev. 2011, 25, 917–929. [Google Scholar] [CrossRef] [PubMed]
- Jaako, P.; Faille, A.; Tan, S.; Wong, C.C.; Escudero-Urquijo, N.; Castro-Hartmann, P.; Wright, P.; Hilcenko, C.; Adams, D.J.; Warren, A.J. eIF6 rebinding dynamically couples ribosome maturation and translation. Nat. Commun. 2022, 13, 1562. [Google Scholar] [CrossRef]
- Kargas, V.; Castro-Hartmann, P.; Escudero-Urquijo, N.; Dent, K.; Hilcenko, C.; Sailer, C.; Zisser, G.; Marques-Carvalho, M.J.; Pellegrino, S.; Wawiórka, L.; et al. Mechanism of completion of peptidyltransferase centre assembly in eukaryotes. eLife 2019, 8, e44904. [Google Scholar] [CrossRef] [PubMed]
- Armistead, J.; Triggs-Raine, B. Diverse diseases from a ubiquitous process: The ribosomopathy paradox. FEBS Lett. 2014, 588, 1491–1500. [Google Scholar] [CrossRef]
- Aspesi, A.; Ellis, S.R. Rare ribosomopathies: Insights into mechanisms of cancer. Nat. Rev. Cancer 2019, 19, 228–238. [Google Scholar] [CrossRef]
- Mäkitie, O.; Ellis, L.; Durie, P.R.; Morrison, J.A.; Sochett, E.B.; Rommens, J.M.; Cole, W.G. Skeletal phenotype in patients with Shwachman-Diamond syndrome and mutations in SBDS. Clin. Genet. 2004, 65, 101–112. [Google Scholar] [CrossRef] [PubMed]
- Aggett, P.J.; Harries, J.T.; Harvey, B.A.; Soothill, J.F. An inherited defect of neutrophil mobility in Shwachman syndrome. J. Pediatr. 1979, 94, 391–394. [Google Scholar] [CrossRef]
- Fewtrell, M.S.; Kinsey, S.E.; Williams, D.M.; Bishop, N.J. Bone mineralization and turnover in children with congenital neutropenia, and its relationship to treatment with recombinant human granulocyte-colony stimulating factor. Br. J. Haematol. 1997, 97, 734–736. [Google Scholar] [CrossRef] [PubMed]
- Donadieu, J.; Fenneteau, O.; Beaupain, B.; Beaufils, S.; Bellanger, F.; Mahlaoui, N.; Lambilliotte, A.; Aladjidi, N.; Bertrand, Y.; Mialou, V.; et al. Classification of and risk factors for hematologic complications in a French national cohort of 102 patients with Shwachman-Diamond syndrome. Haematologica 2012, 97, 1312–1319. [Google Scholar] [CrossRef]
- Alter, B.P.; Giri, N.; Savage, S.A.; Rosenberg, P.S. Cancer in the National Cancer Institute inherited bone marrow failure syndrome cohort after fifteen years of follow-up. Haematologica 2018, 103, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Kawashima, N.; Oyarbide, U.; Cipolli, M.; Bezzerri, V.; Corey, S.J. Shwachman-Diamond syndromes: Clinical, genetic, and biochemical insights from the rare variants. Haematologica 2023, 108, 2594–2605. [Google Scholar] [CrossRef] [PubMed]
- Oyarbide, U.; Shah, A.N.; Amaya-Mejia, W.; Snyderman, M.; Kell, M.J.; Allende, D.S.; Calo, E.; Topczewski, J.; Corey, S.J. Loss of Sbds in zebrafish leads to neutropenia and pancreas and liver atrophy. JCI Insight 2020, 5, e134309. [Google Scholar] [CrossRef] [PubMed]
- Levin, T.L.; Mäkitie, O.; Berdon, W.E.; Lachman, R.S. Shwachman-Bodian-Diamond syndrome: Metaphyseal chondrodysplasia in children with pancreatic insufficiency and neutropenia. Pediatr. Radiol. 2015, 45, 1066–1071. [Google Scholar] [CrossRef] [PubMed]
- Pichler, J.; Meyer, R.; Köglmeier, J.; Ancliff, P.; Shah, N. Nutritional status in children with Shwachman-diamond syndrome. Pancreas 2015, 44, 590–595. [Google Scholar] [CrossRef] [PubMed]
- Group, W.M.G.R.S. WHO Child Growth Standards based on length/height, weight and age. Acta Paediatr. Suppl. 2006, 450, 76–85. [Google Scholar] [CrossRef]
- de Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef]
- Cipolli, M.; Tridello, G.; Micheletto, A.; Perobelli, S.; Pintani, E.; Cesaro, S.; Maserati, E.; Nicolis, E.; Danesino, C. Normative growth charts for Shwachman-Diamond syndrome from Italian cohort of 0–8 years old. BMJ Open 2019, 9, e022617. [Google Scholar] [CrossRef]
- Cole, T.J. Sample size and sample composition for constructing growth reference centiles. Stat. Methods Med. Res. 2021, 30, 488–507. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Green, P.J. Smoothing reference centile curves: The LMS method and penalized likelihood. Stat. Med. 1992, 11, 1305–1319. [Google Scholar] [CrossRef]
- Cacciari, E.; Milani, S.; Balsamo, A.; Dammacco, F.; De Luca, F.; Chiarelli, F.; Pasquino, A.; Tonini, G.; Vanelli, M. Italian cross-sectional growth charts for height, weight and BMI (6–20 y). Eur. J. Clin. Nutr. 2002, 56, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Natale, V.; Rajagopalan, A. Worldwide variation in human growth and the World Health Organization growth standards: A systematic review. BMJ Open 2014, 4, e003735. [Google Scholar] [CrossRef] [PubMed]
- Piras, G.N.; Bozzola, M.; Bianchin, L.; Bernasconi, S.; Bona, G.; Lorenzoni, G.; Buzi, F.; Rigon, F.; Tonini, G.; De Sanctis, V.; et al. The levelling-off of the secular trend of age at menarche among Italian girls. Heliyon 2020, 6, e04222. [Google Scholar] [CrossRef]
- Goobie, S.; Popovic, M.; Morrison, J.; Ellis, L.; Ginzberg, H.; Boocock, G.R.; Ehtesham, N.; Bétard, C.; Brewer, C.G.; Roslin, N.M.; et al. Shwachman-Diamond syndrome with exocrine pancreatic dysfunction and bone marrow failure maps to the centromeric region of chromosome 7. Am. J. Hum. Genet. 2001, 68, 1048–1054. [Google Scholar] [CrossRef]
- Kent, A.; Murphy, G.H.; Milla, P. Psychological characteristics of children with Shwachman syndrome. Arch. Dis. Child. 1990, 65, 1349–1352. [Google Scholar] [CrossRef]
- Cole, T.J. The development of growth references and growth charts. Ann. Hum Biol. 2012, 39, 382–394. [Google Scholar] [CrossRef]
- Cipolli, M.; Boni, C.; Penzo, M.; Villa, I.; Bolamperti, S.; Baldisseri, E.; Frattini, A.; Porta, G.; Api, M.; Selicato, N.; et al. Ataluren improves myelopoiesis and neutrophil chemotaxis by restoring ribosome biogenesis and reducing p53 levels in Shwachman-Diamond syndrome cells. Br. J. Haematol. 2023, 204, 292–305. [Google Scholar] [CrossRef]
- Malouf, C.; Loughran, S.J.; Wilkinson, A.C.; Shimamura, A.; Río, P. Translational research for bone marrow failure patients. Exp. Hematol. 2022, 105, 18–21. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | N |
|---|---|
| Total | 121 |
| Sex | |
| Males (%) | 70 (57.9) |
| Females (%) | 51 (42.1) |
| Age at diagnosis (months) | |
| Median (min–max) | 1.3 (0–35.6) |
| Gestational age (weeks) | |
| Median (min–max) | 39 (29–42) |
| Weight at birth | |
| Median (min–max) | 2.7 (0.9–4.2) |
| Pancreatic insufficiency at follow-up | |
| Yes (%) | 80 (66.1) |
| No (%) | 31 (25.6) |
| Unknown (%) | 10 (8.3) |
| Pancreatic insufficiency (at least once) | |
| Yes (%) | 113 (93.4) |
| No (%) | 7 (5.8) |
| Unknown (%) | 1 (0.8) |
| Pancreatic enzyme | |
| No, never (%) | 10 (8.3) |
| Yes, ongoing (%) | 80 (66.1) |
| Yes, in the past, but stopped (%) | 22 (18.2) |
| Unknown (%) | 9 (7.4) |
| GH | |
| Yes (%) | 8 (6.6) |
| No (%) | 113 (93.4) |
| HSCT | |
| Yes (%) | 19 (15.7) |
| No (%) | 102 (84.3) |
| Mutations | N (%) |
| c.258+2T>C and c.183-184TA>CT | 68 (56.2) |
| c.258+2T>C and c.258+2T>C | 12 (9.9) |
| c.258+2T>C and c.183-184TA>CT+c.258+2T>C | 17 (14) |
| c.258+2T>C and c.258+533_459+403del | 5 (4.1) |
| c.258+2T>C and c.187G>T | 2 (1.7) |
| c.258+2T>C and c.101A>T | 1 (0.8) |
| c.258+2T>C and c.107delT | 1 (0.8) |
| c.258+2T>C and c.128+6T>C | 1 (0.8) |
| c.258+2T>C and c.212C>T | 1 (0.8) |
| c.258+2T>C and c.289-292del | 1 (0.8) |
| c.258+2T>C and c.300delAC | 1 (0.8) |
| c.258+2T>C and c.307-308delCA | 1 (0.8) |
| c.258+2T>C and c.352A>G | 1 (0.8) |
| c.258+2T>C and c.356G>A | 1 (0.8) |
| c.258+2T>C and c.624+1G>C | 1 (0.8) |
| c.258+2T>C and c.92-93GC>AG | 1 (0.8) |
| c.258+2T>C and c.184A>T | 1 (0.8) |
| c.258+2T>C and c.18dup | 1 (0.8) |
| c.258+2T>C and c.IVS1-71del83bp | 1 (0.8) |
| c.258+2T>C and c.652C>T | 1 (0.8) |
| c.258+2T>C and c.95A>G | 1 (0.8) |
| c.523C>T and c.523C>T | 1 (0.8) |
| Age | SDS M | SDS F | Gen. Pop. M * | Gen. Pop. F * |
|---|---|---|---|---|
| Height | ||||
| 2–6 | 33.3 | 34.8 | 31.5 | 33.1 |
| 6–10 | 18.5 | 19.9 | 19.0 | 19.7 |
| 10–14 | 14.8 | 17.6 | 18.4 | 14.9 |
| 14–18 | 7.5 | 6.8 | 6.9 | 1.8 |
| Weight | ||||
| 2–6 | 71.1 | 73.7 | 71.9 | 78.0 |
| 6–10 | 55.0 | 55.0 | 59.5 | 60.7 |
| 10–14 | 50.7 | 56.6 | 59.0 | 52.6 |
| 14–18 | 40.2 | 34.0 | 23.1 | 4.1 |
| BMI | ||||
| 2–6 | −3.6 | −4.9 | −3.0 | 0.0 |
| 6–10 | 12.4 | 8.5 | 12.5 | 12.4 |
| 10–14 | 10.1 | 16.7 | 16.1 | 14.9 |
| 14–18 | 18.5 | 10.7 | 5.3 | 1.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pegoraro, A.; Bezzerri, V.; Tridello, G.; Brignole, C.; Lucca, F.; Pintani, E.; Danesino, C.; Cesaro, S.; Fioredda, F.; Cipolli, M. Growth Charts for Shwachman–Diamond Syndrome at Ages 0 to 18 Years. Cancers 2024, 16, 1420. https://doi.org/10.3390/cancers16071420
Pegoraro A, Bezzerri V, Tridello G, Brignole C, Lucca F, Pintani E, Danesino C, Cesaro S, Fioredda F, Cipolli M. Growth Charts for Shwachman–Diamond Syndrome at Ages 0 to 18 Years. Cancers. 2024; 16(7):1420. https://doi.org/10.3390/cancers16071420
Chicago/Turabian StylePegoraro, Anna, Valentino Bezzerri, Gloria Tridello, Cecilia Brignole, Francesca Lucca, Emily Pintani, Cesare Danesino, Simone Cesaro, Francesca Fioredda, and Marco Cipolli. 2024. "Growth Charts for Shwachman–Diamond Syndrome at Ages 0 to 18 Years" Cancers 16, no. 7: 1420. https://doi.org/10.3390/cancers16071420
APA StylePegoraro, A., Bezzerri, V., Tridello, G., Brignole, C., Lucca, F., Pintani, E., Danesino, C., Cesaro, S., Fioredda, F., & Cipolli, M. (2024). Growth Charts for Shwachman–Diamond Syndrome at Ages 0 to 18 Years. Cancers, 16(7), 1420. https://doi.org/10.3390/cancers16071420