
PAX1/JAM3 Methylation and HPV Viral Load in Women with Persistent HPV Infection

 ,
, 
Abstract
Simple Summary
Abstract
1. Background
2. Materials and Methods
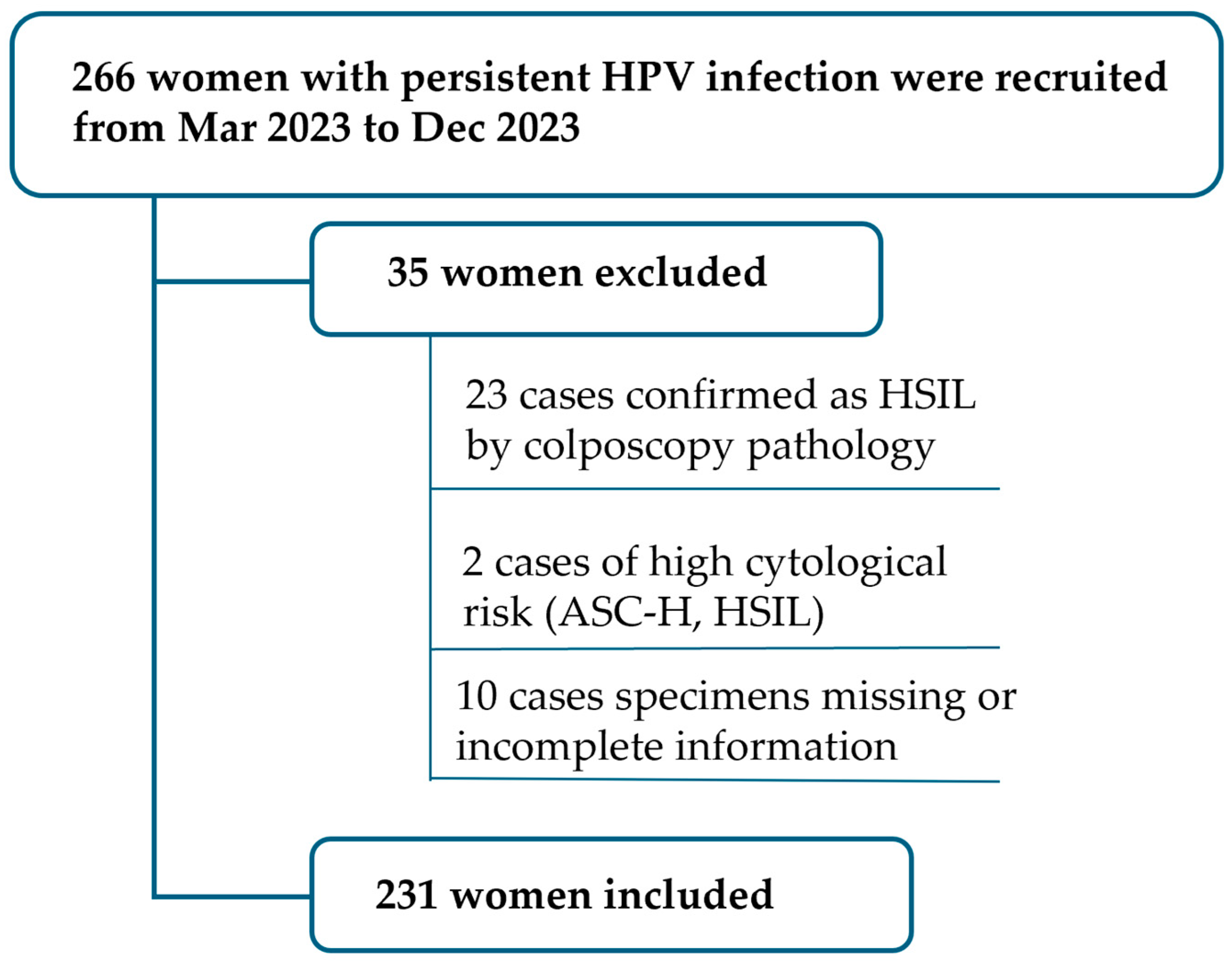
2.1. Study Population and Samples
2.2. Group and Previous History Collection
2.3. Methylation and HPV Viral Load
2.4. Colposcopy and Pathology
2.5. Statistical Methods
3. Result
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Van Doorslaer, K.; Chen, Z.; Bernard, H.U.; Chan, P.; Desalle, R.; Dillner, J.; Forslund, O.; Haga, T.; Mcbride, A.A.; Villa, L.L.; et al. Ictv virus taxonomy profile: Papillomaviridae. J. Gen. Virol. 2018, 99, 989–990. [Google Scholar] [CrossRef]
- Cosper, P.F.; Bradley, S.; Luo, L.; Kimple, R.J. Biology of hpv mediated carcinogenesis and tumor progression. Semin. Radiat. Oncol. 2021, 31, 265–273. [Google Scholar] [CrossRef]
- Munoz, N.; Bosch, F.X.; de Sanjose, S.; Herrero, R.; Castellsague, X.; Shah, K.V.; Snijders, P.J.; Meijer, C.J. Epidemiologic classification of human papillomavirus types associated with cervical cancer. N. Engl. J. Med. 2003, 348, 518–527. [Google Scholar] [CrossRef]
- World Health Organization. Who Guideline for Screening and Treatment of Cervical PRE-cancer Lesions for Cervical Cancer Prevention, Edition Second.2021[r/ol]. (2021-07-06)[2022-08-08]. Available online: https://www.who.int/publications/i/item/9789240030824. (accessed on 6 February 2023).
- Della, F.A.; Warburton, A.; Coursey, T.L.; Khurana, S.; Mcbride, A.A. Persistent human papillomavirus infection. Viruses 2021, 13, 321. [Google Scholar] [CrossRef]
- Shanmugasundaram, S.; You, J. Targeting persistent human papillomavirus infection. Viruses 2017, 9, 229. [Google Scholar] [CrossRef]
- Denis, F.; Hanz, S.; Alain, S. Clearance, persistence and recurrence of hpv infection. Gynecol. Obstet. Fertil. 2008, 36, 430–440. [Google Scholar] [CrossRef]
- Kaderli, R.; Schnuriger, B.; Brugger, L.E. The impact of smoking on hpv infection and the development of anogenital warts. Int. J. Colorectal Dis. 2014, 29, 899–908. [Google Scholar] [CrossRef]
- Kim, M.; Park, N.J.; Jeong, J.Y.; Park, J.Y. Multiple human papilloma virus (hpv) infections are associated with hsil and persistent hpv infection status in korean patients. Viruses 2021, 13, 1342. [Google Scholar] [CrossRef]
- Nguyen, H.; Le, T.M.; Lee, E.; Lee, D.; Choi, Y.; Cho, J.; Park, N.J.; Chong, G.O.; Seo, I.; Han, H.S. Relationship between human papillomavirus status and the cervicovaginal microbiome in cervical cancer. Microorganisms 2023, 11, 1417. [Google Scholar] [CrossRef]
- Smola, S. Immunopathogenesis of hpv-associated cancers and prospects for immunotherapy. Viruses 2017, 9, 254. [Google Scholar] [CrossRef]
- Bonde, J.; Bottari, F.; Iacobone, A.D.; Cocuzza, C.E.; Sandri, M.T.; Bogliatto, F.; Khan, K.S.; Ejegod, D.M.; Gary, D.S.; Andrews, J.C. Human papillomavirus same genotype persistence and risk: A systematic review. J. Low. Genit. Tract Dis. 2021, 25, 27–37. [Google Scholar] [CrossRef]
- Elfgren, K.; Elfstrom, K.M.; Naucler, P.; Arnheim-Dahlstrom, L.; Dillner, J. Management of women with human papillomavirus persistence: Long-term follow-up of a randomized clinical trial. Am. J. Obstet. Gynecol. 2017, 216, 261–264. [Google Scholar] [CrossRef]
- Szymonowicz, K.A.; Chen, J. Biological and clinical aspects of hpv-related cancers. Cancer Biol. Med. 2020, 17, 864–878. [Google Scholar] [CrossRef]
- Ramirez, A.T.; Sanchez, G.I.; Nedjai, B.; Agudelo, M.C.; Brentnall, A.R.; Cuschieri, K.; Castaneda, K.M.; Cuzick, J.; Lorincz, A.T. Effective methylation triage of hpv positive women with abnormal cytology in a middle-income country. Int. J. Cancer. 2021, 148, 1383–1393. [Google Scholar] [CrossRef]
- Song, F.; Yan, P.; Huang, X.; Wang, C.; Qu, X.; Du, H.; Wu, R. Triaging hpv-positive, cytology-negative cervical cancer screening results with extended hpv genotyping and p16(ink4a) immunostaining in china. BMC Infect. Dis. 2021, 21, 400. [Google Scholar] [CrossRef]
- Berggrund, M.; Gustavsson, I.; Aarnio, R.; Hedlund-Lindberg, J.; Sanner, K.; Wikstrom, I.; Enroth, S.; Olovsson, M.; Gyllensten, U. Hpv viral load in self-collected vaginal fluid samples as predictor for presence of cervical intraepithelial neoplasia. Virol. J. 2019, 16, 146. [Google Scholar] [CrossRef]
- Verhelst, S.; Poppe, W.A.; Bogers, J.J.; Depuydt, C.E. Serial measurement of type-specific human papillomavirus load enables classification of cervical intraepithelial neoplasia lesions according to occurring human papillomavirus-induced pathway. Eur. J. Cancer. Prev. 2017, 26, 156–164. [Google Scholar] [CrossRef]
- Schmitt, M.; Depuydt, C.; Benoy, I.; Bogers, J.; Antoine, J.; Pawlita, M.; Arbyn, M. Viral load of high-risk human papillomaviruses as reliable clinical predictor for the presence of cervical lesions. Cancer Epidemiol. Biomarkers Prev. 2013, 22, 406–414. [Google Scholar] [CrossRef]
- Carcopino, X.; Henry, M.; Mancini, J.; Giusiano, S.; Boubli, L.; Olive, D.; Tamalet, C. Significance of hpv 16 and 18 viral load quantitation in women referred for colposcopy. J. Med. Virol. 2012, 84, 306–313. [Google Scholar] [CrossRef]
- Yin, A.; Zhang, Q.; Kong, X.; Jia, L.; Yang, Z.; Meng, L.; Li, L.; Wang, X.; Qiao, Y.; Lu, N.; et al. Jam3 methylation status as a biomarker for diagnosis of preneoplastic and neoplastic lesions of the cervix. Oncotarget 2015, 6, 44373–44387. [Google Scholar] [CrossRef]
- Boers, A.; Bosgraaf, R.P.; van Leeuwen, R.W.; Schuuring, E.; Heideman, D.A.; Massuger, L.F.; Verhoef, V.M.; Bulten, J.; Melchers, W.J.; van der Zee, A.G.; et al. Dna methylation analysis in self-sampled brush material as a triage test in hrhpv-positive women. Br. J. Cancer 2014, 111, 1095–1101. [Google Scholar] [CrossRef]
- Thompson, B.; Davidson, E.A.; Liu, W.; Nebert, D.W.; Bruford, E.A.; Zhao, H.; Dermitzakis, E.T.; Thompson, D.C.; Vasiliou, V. Overview of pax gene family: Analysis of human tissue-specific variant expression and involvement in human disease. Hum. Genet. 2021, 140, 381–400. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.C.; Huang, R.L.; Wang, H.C.; Liao, Y.P.; Yu, M.H.; Lai, H.C. High methylation rate of lmx1a, nkx6-1, pax1, ptprr, sox1, and znf582 genes in cervical adenocarcinoma. Int. J. Gynecol. Cancer 2014, 24, 201–209. [Google Scholar] [CrossRef]
- Fang, C.; Wang, S.Y.; Liou, Y.L.; Chen, M.H.; Ouyang, W.; Duan, K.M. The promising role of pax1 (aliases: hup48, ofc2) gene methylation in cancer screening. Mol. Genet. Genom. Med. 2019, 7, e506. [Google Scholar] [CrossRef] [PubMed]
- Kan, Y.Y.; Liou, Y.L.; Wang, H.J.; Chen, C.Y.; Sung, L.C.; Chang, C.F.; Liao, C.I. Pax1 methylation as a potential biomarker for cervical cancer screening. Int. J. Gynecol. Cancer 2014, 24, 928–934. [Google Scholar] [CrossRef]
- Lai, H.C.; Lin, Y.W.; Huang, T.H.; Yan, P.; Huang, R.L.; Wang, H.C.; Liu, J.; Chan, M.W.; Chu, T.Y.; Sun, C.A.; et al. Identification of novel dna methylation markers in cervical cancer. Int. J. Cancer 2008, 123, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Guo, R.; Lai, T.; Qiao, L.; Fu, H. The application of pax1 methylation detection and hpv e6/e7 mrna detection in cervical cancer screening. J. Obstet. Gynaecol. Res. 2021, 47, 2720–2728. [Google Scholar] [CrossRef]
- Liang, H.; Li, G.L.; Liu, J.; Fu, M.; Huang, H.; Zhao, K.; Wei, Y.; Xiao, J. The application value of pax1 and znf582 gene methylation in high grade intraepithelial lesion and cervical cancer. Clin. Transl. Oncol. 2021, 23, 283–288. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Zhao, C.; Zhao, Y.; Li, J.; Zhang, X.; Zhang, W.; Gao, Q.; Wei, L. Association and effectiveness of pax1 methylation and hpv viral load for the detection of cervical high-grade squamous intraepithelial lesion. Pathogens 2022, 12, 63. [Google Scholar] [CrossRef]
- Koshiol, J.; Lindsay, L.; Pimenta, J.M.; Poole, C.; Jenkins, D.; Smith, J.S. Persistent human papillomavirus infection and cervical neoplasia: A systematic review and meta-analysis. Am. J. Epidemiol. 2008, 168, 123–137. [Google Scholar] [CrossRef]
- Rositch, A.F.; Koshiol, J.; Hudgens, M.G.; Razzaghi, H.; Backes, D.M.; Pimenta, J.M.; Franco, E.L.; Poole, C.; Smith, J.S. Patterns of persistent genital human papillomavirus infection among women worldwide: A literature review and meta-analysis. Int. J. Cancer 2013, 133, 1271–1285. [Google Scholar] [CrossRef] [PubMed]
- Duan, L.; Du, H.; Wang, C.; Huang, X.; Qu, X.; Shi, B.; Liu, Y.; Zhang, W.; Duan, X.; Wei, L.; et al. The application of bmrt-hpv viral load to secondary screening strategies for cervical cancer. PLoS ONE 2020, 15, e232117. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Zhao, C.; Zhao, Y.; Li, J.; Wei, L. Age-stratified analysis of vaginal microbiota dysbiosis and the relationship with hpv viral load in hpv-positive women. J. Immunol. Res. 2022, 2022, 1372926. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, A.C.; Schiffman, M.; Herrero, R.; Hildesheim, A.; Bratti, C.; Sherman, M.E.; Solomon, D.; Guillen, D.; Alfaro, M.; Morales, J.; et al. Longitudinal study of human papillomavirus persistence and cervical intraepithelial neoplasia grade 2/3: Critical role of duration of infection. J. Natl. Cancer Inst. 2010, 102, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Kjaer, S.K.; Frederiksen, K.; Munk, C.; Iftner, T. Long-term absolute risk of cervical intraepithelial neoplasia grade 3 or worse following human papillomavirus infection: Role of persistence. J. Natl. Cancer Inst. 2010, 102, 1478–1488. [Google Scholar] [CrossRef] [PubMed]
- Fontaine, J.; Hankins, C.; Money, D.; Rachlis, A.; Pourreaux, K.; Ferenczy, A.; Coutlee, F. Human papillomavirus type 16 (hpv-16) viral load and persistence of hpv-16 infection in women infected or at risk for hiv. J. Clin. Virol. 2008, 43, 307–312. [Google Scholar] [CrossRef]
- Dong, L.; Wang, M.Z.; Zhao, X.L.; Feng, R.M.; Hu, S.Y.; Zhang, Q.; Smith, J.S.; Qiao, Y.L.; Zhao, F.H. Human papillomavirus viral load as a useful triage tool for non-16/18 high-risk human papillomavirus positive women: A prospective screening cohort study. Gynecol. Oncol. 2018, 148, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Carcopino, X.; Bolger, N.; Henry, M.; Mancini, J.; Boubli, L.; Olive, D.; Cleary, S.; Prendiville, W.; Tamalet, C. Evaluation of type-specific hpv persistence and high-risk hpv viral load quantitation in hpv positive women under 30 with normal cervical cytology. J. Med. Virol. 2011, 83, 637–643. [Google Scholar] [CrossRef][Green Version]
- van der Weele, P.; van Logchem, E.; Wolffs, P.; van den Broek, I.; Feltkamp, M.; de Melker, H.; Meijer, C.J.; Boot, H.; King, A.J. Correlation between viral load, multiplicity of infection, and persistence of hpv16 and hpv18 infection in a dutch cohort of young women. J. Clin. Virol. 2016, 83, 6–11. [Google Scholar] [CrossRef]
- Manawapat, A.; Stubenrauch, F.; Russ, R.; Munk, C.; Kjaer, S.K.; Iftner, T. Physical state and viral load as predictive biomarkersfor persistence and progression of hpv16-positive cervical lesions: Results from a population based long-term prospective cohort study. Am. J. Cancer Res. 2012, 2, 192–203. [Google Scholar]
- Pett, M.; Coleman, N. Integration of high-risk human papillomavirus: A key event in cervical carcinogenesis? J. Pathol. 2007, 212, 356–367. [Google Scholar] [CrossRef] [PubMed]
- Wissing, M.D.; Louvanto, K.; Comete, E.; Burchell, A.N.; El-Zein, M.; Rodrigues, A.; Tellier, P.P.; Coutlee, F.; Franco, E.L. Human papillomavirus viral load and transmission in young, recently formed heterosexual couples. J. Infect. Dis. 2019, 220, 1152–1161. [Google Scholar] [CrossRef] [PubMed]
- van Eer, K.; Laabi, I.; van Benthem, B.; Steenbergen, R.; King, A.J. The association between viral load and concurrent human papillomavirus infection at the genital and anal sites of young women and the impact of vaccination. Tumour Virus Res. 2022, 13, 200233. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.L.; Ho, S.C.; Su, Y.F.; Juan, Y.C.; Huang, C.Y.; Chao, A.S.; Hsu, Z.S.; Chang, C.F.; Fwu, C.W.; Chang, T.C. Dna methylation marker for the triage of hrhpv positive women in cervical cancer screening: Real-world evidence in taiwan. Gynecol. Oncol. 2021, 161, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Chao, T.K.; Ke, F.Y.; Liao, Y.P.; Wang, H.C.; Yu, C.P.; Lai, H.C. Triage of cervical cytological diagnoses of atypical squamous cells by dna methylation of paired boxed gene 1 (pax1). Diagn. Cytopathol. 2013, 41, 41–46. [Google Scholar] [CrossRef]
- Li, M.; Zhao, C.; Zhao, Y.; Li, J.; Wang, J.; Luo, H.; Tang, Z.; Guo, Y.; Wei, L. The role of pax1 methylation in predicting the pathological upgrade of cervical intraepithelial neoplasia before cold knife conization. Front. Oncol. 2022, 12, 1064722. [Google Scholar] [CrossRef]
- Li, X.; Zhou, X.; Zeng, M.; Zhou, Y.; Zhang, Y.; Liou, Y.L.; Zhu, H. Methylation of pax1 gene promoter in the prediction of concurrent chemo-radiotherapy efficacy in cervical cancer. J. Cancer 2021, 12, 5136–5143. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Categories | Overall | HPV Duration | p | ||
|---|---|---|---|---|---|
| 1–2 Years | ≥3 Years | ||||
| N | 231 | 156 | 75 | ||
| Age (mean (±SD)) | 46.4 (12.3) | 45.1 (12.4) | 48.9 (11.8) | 0.031 | |
| Previous Screening History (%) | No | 189 (81.8) | 130 (83.3) | 59 (78.7) | 0.261 |
| hrHPV (+) | 22 (9.5) | 15 (9.6) | 7 (9.3) | ||
| hrHPV (−) | 8 (3.5) | 6 (3.8) | 2 (2.7) | ||
| HSIL or CKC | 12 (5.2) | 5 (3.2) | 7 (9.3) | ||
| Cytology Results (%) | NILM | 172 (74.5) | 121 (77.6) | 51 (68.0) | 0.191 |
| ASC-US | 36 (15.6) | 23 (14.7) | 13 (17.3) | ||
| LSIL | 23 (10.0) | 12 (7.7) | 11 (14.7) | ||
| HPV Testing Results (%) | non-hrHPV | 44 (19.0) | 31 (19.9) | 13 (17.3) | 0.899 |
| 12 other hrHPV(+) | 127 (55.0) | 85 (54.5) | 42 (56.0) | ||
| HPV16/18 (+) | 60 (26.0) | 40 (25.6) | 20 (26.7) | ||
| Anti-HPV drug history (%) | No | 200 (86.6) | 134 (85.9) | 66 (88.0) | 0.816 |
| Yes | 31 (13.4) | 22 (14.1) | 9 (12.0) | ||
| Log hrHPV VL (median [IQR]) | 4.0 [2.4, 5.0] | 3.9 [2.2, 5.1] | 4.1 [2.9, 4.9] | 0.434 | |
| Log HPV16/18 VL (median [IQR]) | 0.0 [0.0, 1.1] | 0.0 [0.0, 1.1] | 0.0 [0.0, 1.0] | 0.872 | |
| Log non-HPV 16/18(+) VL (median [IQR]) | 2.8 [0.0, 4.5] | 2.5 [0.0, 4.5] | 3.6 [0.0, 4.5] | 0.556 | |
| PAX1m (ΔCp) (median [IQR]) | 12.8 [8.9, 17.5] | 16.3 [9.2, 17.6] | 10.6 [8.6, 16.9] | 0.025 | |
| JAM3m (ΔCp) (median [IQR]) | 14.1 [12.7, 16.1] | 14.4 [13.0, 16.7] | 13.7 [12.4, 14.9] | 0.007 | |
| Pathology (%) | Normal | 156 (67.5) | 104 (66.7) | 52 (69.3) | 0.799 |
| CIN1 | 75 (32.5) | 52 (33.3) | 23 (30.7) | ||
| Concurrent VaIN (%) | VaIN 1 | 23 (10.0) | 10 (6.4) | 13 (17.3) | 0.031 |
| VaIN 2/3 | 5 (2.2) | 4 (2.6) | 1 (1.3) | ||
| No VaIN | 203 (87.9) | 142 (91.0) | 61 (81.3) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, M.; Zhao, C.; Zhang, X.; Li, J.; Zhao, Y.; Zhang, W.; Ren, L.; Wei, L. PAX1/JAM3 Methylation and HPV Viral Load in Women with Persistent HPV Infection. Cancers 2024, 16, 1430. https://doi.org/10.3390/cancers16071430
Li M, Zhao C, Zhang X, Li J, Zhao Y, Zhang W, Ren L, Wei L. PAX1/JAM3 Methylation and HPV Viral Load in Women with Persistent HPV Infection. Cancers. 2024; 16(7):1430. https://doi.org/10.3390/cancers16071430
Chicago/Turabian StyleLi, Mingzhu, Chao Zhao, Xiaobo Zhang, Jingran Li, Yun Zhao, Wei Zhang, Lihua Ren, and Lihui Wei. 2024. "PAX1/JAM3 Methylation and HPV Viral Load in Women with Persistent HPV Infection" Cancers 16, no. 7: 1430. https://doi.org/10.3390/cancers16071430
APA StyleLi, M., Zhao, C., Zhang, X., Li, J., Zhao, Y., Zhang, W., Ren, L., & Wei, L. (2024). PAX1/JAM3 Methylation and HPV Viral Load in Women with Persistent HPV Infection. Cancers, 16(7), 1430. https://doi.org/10.3390/cancers16071430