
Effect of Neoadjuvant Chemotherapy on Tumor-Infiltrating Lymphocytes in Resectable Gastric Cancer: Analysis from a Western Academic Center

 , , ,
, , ,
Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Patient Cohort
2.2. Definitions and Immunologic Profile Characterization
2.3. Multiplex Immunohistochemistry
2.4. Statistical Analysis
3. Results
3.1. Patient Cohort
3.2. Demographic and Clinicopathologic Characteristics of Upfront Surgery and NAC Cohorts
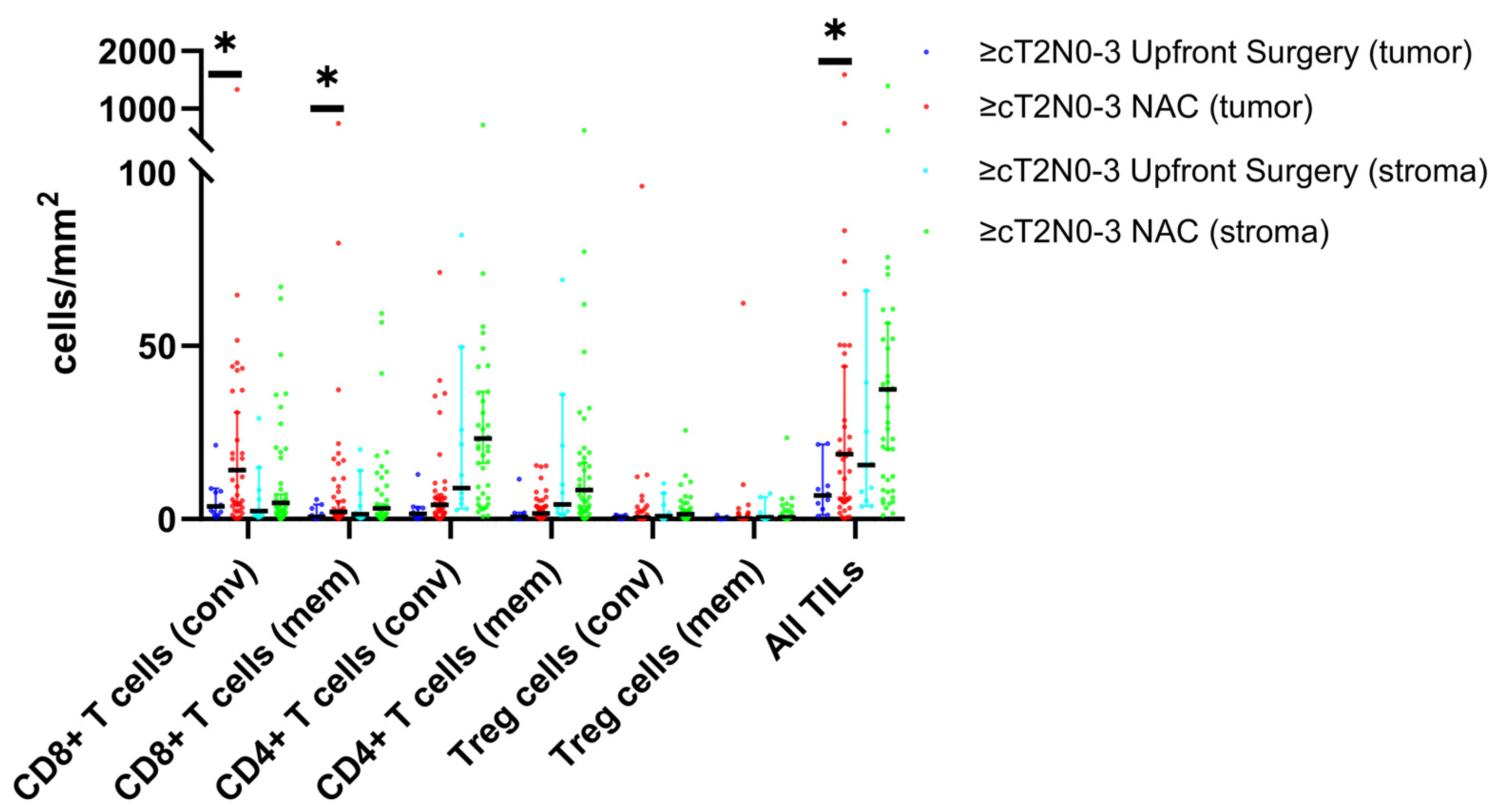
3.3. TIL and Molecular Profiles of Upfront Surgery and NAC Cohorts
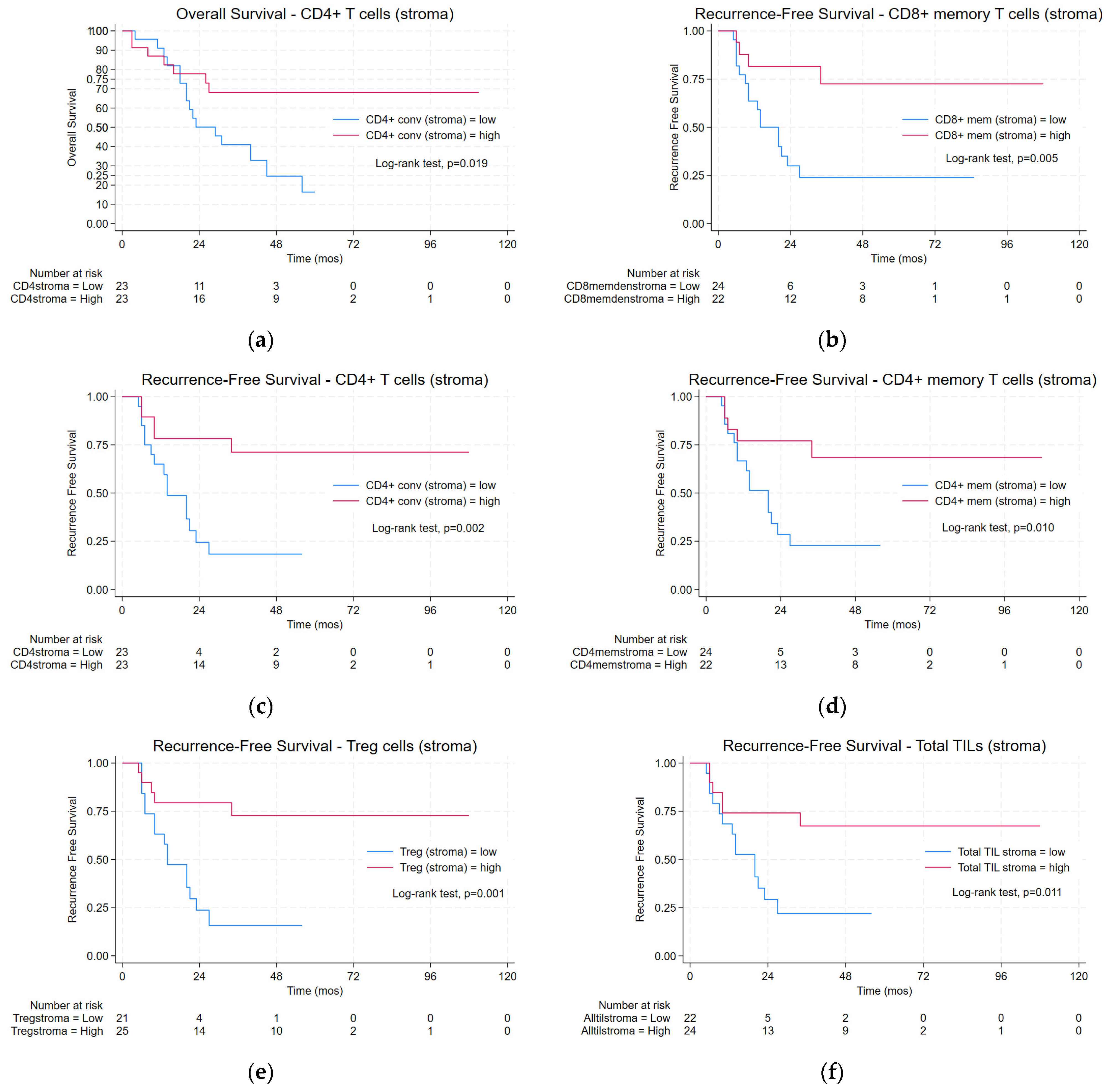
3.4. TIL Density and Oncologic Outcomes
3.5. TIL Density and Pathologic Response
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- de Martel, C.; Forman, D.; Plummer, M. Gastric cancer: Epidemiology and risk factors. Gastroenterol. Clin. N. Am. 2013, 42, 219–240. [Google Scholar] [CrossRef] [PubMed]
- Rawla, P.; Barsouk, A. Epidemiology of gastric cancer: Global trends, risk factors and prevention. Gastroenterol. Rev. 2019, 14, 26–38. [Google Scholar] [CrossRef] [PubMed]
- Morgan, E.; Arnold, M.; Camargo, M.C.; Gini, A.; Kunzmann, A.T.; Matsuda, T.; Meheus, F.; Verhoeven, R.H.A.; Vignat, J.; Laversanne, M.; et al. The current and future incidence and mortality of gastric cancer in 185 countries, 2020–2040: A population-based modelling study. EClinicalMedicine 2022, 47, 101404. [Google Scholar] [CrossRef] [PubMed]
- American Cancer Society. Cancer Facts & Figures 2024. Stomach Cancer Survival Rates: American Cancer Society. 2024. Available online: https://www.cancer.org/cancer/types/stomach-cancer/detection-diagnosis-staging/survival-rates.html (accessed on 31 January 2024).
- Motzer, R.J.; Tannir, N.M.; McDermott, D.F.; Aren Frontera, O.; Melichar, B.; Choueiri, T.K.; Plimack, E.R.; Barthelemy, P.; Porta, C.; George, S.; et al. Nivolumab plus Ipilimumab versus Sunitinib in Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2018, 378, 1277–1290. [Google Scholar] [CrossRef] [PubMed]
- Herbst, R.S.; Baas, P.; Kim, D.W.; Felip, E.; Perez-Gracia, J.L.; Han, J.Y.; Molina, J.; Kim, J.H.; Arvis, C.D.; Ahn, M.J.; et al. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): A randomised controlled trial. Lancet 2016, 387, 1540–1550. [Google Scholar] [CrossRef] [PubMed]
- Bang, Y.J.; Kang, Y.K.; Catenacci, D.V.; Muro, K.; Fuchs, C.S.; Geva, R.; Hara, H.; Golan, T.; Garrido, M.; Jalal, S.I.; et al. Pembrolizumab alone or in combination with chemotherapy as first-line therapy for patients with advanced gastric or gastroesophageal junction adenocarcinoma: Results from the phase II nonrandomized KEYNOTE-059 study. Gastric Cancer 2019, 22, 828–837. [Google Scholar] [CrossRef]
- Borghaei, H.; Paz-Ares, L.; Horn, L.; Spigel, D.R.; Steins, M.; Ready, N.E.; Chow, L.Q.; Vokes, E.E.; Felip, E.; Holgado, E.; et al. Nivolumab versus Docetaxel in Advanced Nonsquamous Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2015, 373, 1627–1639. [Google Scholar] [CrossRef]
- Kelly, R.J.; Ajani, J.A.; Kuzdzal, J.; Zander, T.; Van Cutsem, E.; Piessen, G.; Mendez, G.; Feliciano, J.; Motoyama, S.; Lievre, A.; et al. Adjuvant Nivolumab in Resected Esophageal or Gastroesophageal Junction Cancer. N. Engl. J. Med. 2021, 384, 1191–1203. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network. Clinical Practice guidelines in Oncology: Gastric Cancer. NCCN Guidelines 2023 (Version 1). Available online: https://www.nccn.org/guidelines/category_1 (accessed on 15 February 2024).
- Li, F.; Li, C.; Cai, X.; Xie, Z.; Zhou, L.; Cheng, B.; Zhong, R.; Xiong, S.; Li, J.; Chen, Z.; et al. The association between CD8+ tumor-infiltrating lymphocytes and the clinical outcome of cancer immunotherapy: A systematic review and meta-analysis. EClinicalMedicine 2021, 41, 101134. [Google Scholar] [CrossRef]
- Loupakis, F.; Depetris, I.; Biason, P.; Intini, R.; Prete, A.A.; Leone, F.; Lombardi, P.; Filippi, R.; Spallanzani, A.; Cascinu, S.; et al. Prediction of Benefit from Checkpoint Inhibitors in Mismatch Repair Deficient Metastatic Colorectal Cancer: Role of Tumor Infiltrating Lymphocytes. Oncologist 2020, 25, 481–487. [Google Scholar] [CrossRef]
- Paijens, S.T.; Vledder, A.; de Bruyn, M.; Nijman, H.W. Tumor-infiltrating lymphocytes in the immunotherapy era. Cell. Mol. Immunol. 2021, 18, 842–859. [Google Scholar] [CrossRef] [PubMed]
- Uryvaev, A.; Passhak, M.; Hershkovits, D.; Sabo, E.; Bar-Sela, G. The role of tumor-infiltrating lymphocytes (TILs) as a predictive biomarker of response to anti-PD1 therapy in patients with metastatic non-small cell lung cancer or metastatic melanoma. Med. Oncol. 2018, 35, 25. [Google Scholar] [CrossRef] [PubMed]
- Emens, L.A.; Cruz, C.; Eder, J.P.; Braiteh, F.; Chung, C.; Tolaney, S.M.; Kuter, I.; Nanda, R.; Cassier, P.A.; Delord, J.P.; et al. Long-term Clinical Outcomes and Biomarker Analyses of Atezolizumab Therapy for Patients With Metastatic Triple-Negative Breast Cancer: A Phase 1 Study. JAMA Oncol. 2019, 5, 74–82. [Google Scholar] [CrossRef] [PubMed]
- Hurkmans, D.P.; Kuipers, M.E.; Smit, J.; van Marion, R.; Mathijssen, R.H.J.; Postmus, P.E.; Hiemstra, P.S.; Aerts, J.; von der Thusen, J.H.; van der Burg, S.H. Tumor mutational load, CD8(+) T cells, expression of PD-L1 and HLA class I to guide immunotherapy decisions in NSCLC patients. Cancer Immunol. Immunother. 2020, 69, 771–777. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Gao, P.; Hao, Z.; Chen, L.; Li, X.; Jiao, Y.; Liu, J.; Li, J.; Zhang, Y.; Peng, X.; et al. The effect of neoadjuvant chemotherapy on the tumor immune microenvironment in gastrointestinal tumors. Front. Oncol. 2022, 12, 1054598. [Google Scholar] [CrossRef] [PubMed]
- Merlano, M.C.; Denaro, N.; Galizia, D.; Ruatta, F.; Occelli, M.; Minei, S.; Abbona, A.; Paccagnella, M.; Ghidini, M.; Garrone, O. How Chemotherapy Affects the Tumor Immune Microenvironment: A Narrative Review. Biomedicines 2022, 10, 1822. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Zhang, Z.; Wang, Z.; Wu, P.; Qiu, F.; Huang, J. Prognostic and predictive value of tumor-infiltrating lymphocytes in breast cancer: A systematic review and meta-analysis. Clin. Transl. Oncol. 2016, 18, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Xing, X.; Shi, J.; Jia, Y.; Dou, Y.; Li, Z.; Dong, B.; Guo, T.; Cheng, X.; Li, X.; Du, H.; et al. Effect of neoadjuvant chemotherapy on the immune microenvironment in gastric cancer as determined by multiplex immunofluorescence and T cell receptor repertoire analysis. J. Immunother. Cancer 2022, 10, e003984. [Google Scholar] [CrossRef]
- Joshi, S.S.; Badgwell, B.D. Current treatment and recent progress in gastric cancer. CA Cancer J. Clin. 2021, 71, 264–279. [Google Scholar] [CrossRef]
- Park, Y.S.; Kook, M.C.; Kim, B.H.; Lee, H.S.; Kang, D.W.; Gu, M.J.; Shin, O.R.; Choi, Y.; Lee, W.; Kim, H.; et al. A standardized pathology report for gastric cancer: 2nd edition. J. Pathol. Transl. Med. 2023, 57, 1–27. [Google Scholar] [CrossRef]
- Burgart, L.J.; Chopp, W.V.; Jain, D. Protocol for the Examination of Specimens from Patients with Carcinoma of the Stomach; College of American Pathologists: Northfield, IL, USA, 2020. [Google Scholar]
- Fuchs, C.S.; Ozguroglu, M.; Bang, Y.J.; Di Bartolomeo, M.; Mandala, M.; Ryu, M.H.; Fornaro, L.; Olesinski, T.; Caglevic, C.; Chung, H.C.; et al. Pembrolizumab versus paclitaxel for previously treated PD-L1-positive advanced gastric or gastroesophageal junction cancer: 2-year update of the randomized phase 3 KEYNOTE-061 trial. Gastric Cancer 2022, 25, 197–206. [Google Scholar] [CrossRef] [PubMed]
- Marabelle, A.; Le, D.T.; Ascierto, P.A.; Di Giacomo, A.M.; De Jesus-Acosta, A.; Delord, J.P.; Geva, R.; Gottfried, M.; Penel, N.; Hansen, A.R.; et al. Efficacy of Pembrolizumab in Patients With Noncolorectal High Microsatellite Instability/Mismatch Repair-Deficient Cancer: Results from the Phase II KEYNOTE-158 Study. J. Clin. Oncol. 2020, 38, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Shitara, K.; Rha, S.Y.; Wyrwicz, L.S.; Oshima, T.; Karaseva, N.; Osipov, M.; Yasui, H.; Yabusaki, H.; Afanasyev, S.; Park, Y.K.; et al. Neoadjuvant and adjuvant pembrolizumab plus chemotherapy in locally advanced gastric or gastro-oesophageal cancer (KEYNOTE-585): An interim analysis of the multicentre, double-blind, randomised phase 3 study. Lancet Oncol. 2024, 25, 212–224. [Google Scholar] [CrossRef] [PubMed]
- Presti, D.; Dall’Olio, F.G.; Besse, B.; Ribeiro, J.M.; Di Meglio, A.; Soldato, D. Tumor infiltrating lymphocytes (TILs) as a predictive biomarker of response to checkpoint blockers in solid tumors: A systematic review. Crit. Rev. Oncol. Hematol. 2022, 177, 103773. [Google Scholar] [CrossRef] [PubMed]
- Iwahori, K.; Uenami, T.; Yano, Y.; Ueda, T.; Tone, M.; Naito, Y.; Suga, Y.; Fukushima, K.; Shiroyama, T.; Miyake, K.; et al. Peripheral T cell cytotoxicity predicts the efficacy of anti-PD-1 therapy for advanced non-small cell lung cancer patients. Sci. Rep. 2022, 12, 17461. [Google Scholar] [CrossRef] [PubMed]
- Al-Batran, S.E.; Hofheinz, R.D.; Pauligk, C.; Kopp, H.G.; Haag, G.M.; Luley, K.B.; Meiler, J.; Homann, N.; Lorenzen, S.; Schmalenberg, H.; et al. Histopathological regression after neoadjuvant docetaxel, oxaliplatin, fluorouracil, and leucovorin versus epirubicin, cisplatin, and fluorouracil or capecitabine in patients with resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4-AIO): Results from the phase 2 part of a multicentre, open-label, randomised phase 2/3 trial. Lancet Oncol. 2016, 17, 1697–1708. [Google Scholar] [CrossRef] [PubMed]
- Ychou, M.; Boige, V.; Pignon, J.P.; Conroy, T.; Bouche, O.; Lebreton, G.; Ducourtieux, M.; Bedenne, L.; Fabre, J.M.; Saint-Aubert, B.; et al. Perioperative chemotherapy compared with surgery alone for resectable gastroesophageal adenocarcinoma: An FNCLCC and FFCD multicenter phase III trial. J. Clin. Oncol. 2011, 29, 1715–1721. [Google Scholar] [CrossRef] [PubMed]
- Wei, Q.; Xu, Q.; Yuan, X.; Li, J.J.; Chen, L.; Luo, C.; Zhu, X.; Ying, J.E. Immunological impact of chemotherapy on the tumor microenvironment in gastric cancer. J. Surg. Oncol. 2021, 123, 1708–1715. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Martinez, E.; Gil, G.L.; Benito, A.C.; Gonzalez-Billalabeitia, E.; Conesa, M.A.; Garcia Garcia, T.; Garcia-Garre, E.; Vicente, V.; Ayala de la Pena, F. Tumor-infiltrating immune cell profiles and their change after neoadjuvant chemotherapy predict response and prognosis of breast cancer. Breast Cancer Res. 2014, 16, 488. [Google Scholar] [CrossRef]
- James, F.R.; Jiminez-Linan, M.; Alsop, J.; Mack, M.; Song, H.; Brenton, J.D.; Pharoah, P.D.P.; Ali, H.R. Association between tumour infiltrating lymphocytes, histotype and clinical outcome in epithelial ovarian cancer. BMC Cancer 2017, 17, 657. [Google Scholar] [CrossRef]
- Jary, M.; Liu, W.W.; Yan, D.; Bai, I.; Muranyi, A.; Colle, E.; Brocheriou, I.; Turpin, A.; Radosevic-Robin, N.; Bourgoin, P.; et al. Immune microenvironment in patients with mismatch-repair-proficient oligometastatic colorectal cancer exposed to chemotherapy: The randomized MIROX GERCOR cohort study. Mol. Oncol. 2022, 16, 2260–2273. [Google Scholar] [CrossRef]
- Qi, J.; Liu, X.; Yan, P.; He, S.; Lin, Y.; Huang, Z.; Zhang, S.; Xie, S.; Li, Y.; Lu, X.; et al. Analysis of Immune Landscape Reveals Prognostic Significance of Cytotoxic CD4(+) T Cells in the Central Region of pMMR CRC. Front. Oncol. 2021, 11, 724232. [Google Scholar] [CrossRef]
- Gaudreau, P.O.; Negrao, M.V.; Mitchell, K.G.; Reuben, A.; Corsini, E.M.; Li, J.; Karpinets, T.V.; Wang, Q.; Diao, L.; Wang, J.; et al. Neoadjuvant Chemotherapy Increases Cytotoxic T Cell, Tissue Resident Memory T Cell, and B Cell Infiltration in Resectable NSCLC. J. Thorac. Oncol. 2021, 16, 127–139. [Google Scholar] [CrossRef] [PubMed]
- Hu, M.; Li, K.; Maskey, N.; Xu, Z.; Peng, C.; Wang, B.; Li, Y.; Yang, G. Decreased intratumoral Foxp3 Tregs and increased dendritic cell density by neoadjuvant chemotherapy associated with favorable prognosis in advanced gastric cancer. Int. J. Clin. Exp. Pathol. 2014, 7, 4685–4694. [Google Scholar]
- Pages, F.; Berger, A.; Camus, M.; Sanchez-Cabo, F.; Costes, A.; Molidor, R.; Mlecnik, B.; Kirilovsky, A.; Nilsson, M.; Damotte, D.; et al. Effector memory T cells, early metastasis, and survival in colorectal cancer. N. Engl. J. Med. 2005, 353, 2654–2666. [Google Scholar] [CrossRef] [PubMed]
- Brightman, S.E.; Becker, A.; Thota, R.R.; Naradikian, M.S.; Chihab, L.; Zavala, K.S.; Ramamoorthy Premlal, A.L.; Griswold, R.Q.; Dolina, J.S.; Cohen, E.E.W.; et al. Neoantigen-specific stem cell memory-like CD4(+) T cells mediate CD8(+) T cell-dependent immunotherapy of MHC class II-negative solid tumors. Nat. Immunol. 2023, 24, 1345–1357. [Google Scholar] [CrossRef]
- Huang, Q.; Wu, X.; Wang, Z.; Chen, X.; Wang, L.; Lu, Y.; Xiong, D.; Liu, Q.; Tian, Y.; Lin, H.; et al. The primordial differentiation of tumor-specific memory CD8(+) T cells as bona fide responders to PD-1/PD-L1 blockade in draining lymph nodes. Cell 2022, 185, 4049–4066. [Google Scholar] [CrossRef] [PubMed]
- Zuazo, M.; Arasanz, H.; Fernandez-Hinojal, G.; Garcia-Granda, M.J.; Gato, M.; Bocanegra, A.; Martinez, M.; Hernandez, B.; Teijeira, L.; Morilla, I.; et al. Functional systemic CD4 immunity is required for clinical responses to PD-L1/PD-1 blockade therapy. EMBO Mol. Med. 2019, 11, e10293. [Google Scholar] [CrossRef]
- Perez, E.A.; Ballman, K.V.; Tenner, K.S.; Thompson, E.A.; Badve, S.S.; Bailey, H.; Baehner, F.L. Association of Stromal Tumor-Infiltrating Lymphocytes With Recurrence-Free Survival in the N9831 Adjuvant Trial in Patients With Early-Stage HER2-Positive Breast Cancer. JAMA Oncol. 2016, 2, 56–64. [Google Scholar] [CrossRef]
- Chen, L.; Gibbons, D.L.; Goswami, S.; Cortez, M.A.; Ahn, Y.H.; Byers, L.A.; Zhang, X.; Yi, X.; Dwyer, D.; Lin, W.; et al. Metastasis is regulated via microRNA-200/ZEB1 axis control of tumour cell PD-L1 expression and intratumoral immunosuppression. Nat. Commun. 2014, 5, 5241. [Google Scholar] [CrossRef]
- Sun, X.F.; Zhang, H. Clinicopathological significance of stromal variables: Angiogenesis, lymphangiogenesis, inflammatory infiltration, MMP and PINCH in colorectal carcinomas. Mol. Cancer 2006, 5, 43. [Google Scholar] [CrossRef] [PubMed]
- Guo, S.; Deng, C.X. Effect of Stromal Cells in Tumor Microenvironment on Metastasis Initiation. Int. J. Biol. Sci. 2018, 14, 2083–2093. [Google Scholar] [CrossRef]
- Zhu, Y.; Tzoras, E.; Matikas, A.; Bergh, J.; Valachis, A.; Zerdes, I.; Foukakis, T. Expression patterns and prognostic implications of tumor-infiltrating lymphocytes dynamics in early breast cancer patients receiving neoadjuvant therapy: A systematic review and meta-analysis. Front. Oncol. 2022, 12, 999843. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Zhang, T.; Ye, J.; Li, H.; Huang, J.; Li, X.; Wu, B.; Huang, X.; Hou, J. Tumor-infiltrating lymphocytes predict response to chemotherapy in patients with advance non-small cell lung cancer. Cancer Immunol. Immunother. 2012, 61, 1849–1856. [Google Scholar] [CrossRef] [PubMed]
- Kong, J.C.H.; Guerra, G.R.; Millen, R.M.; Roth, S.; Xu, H.; Neeson, P.J.; Darcy, P.K.; Kershaw, M.H.; Sampurno, S.; Malaterre, J.; et al. Tumor-Infiltrating Lymphocyte Function Predicts Response to Neoadjuvant Chemoradiotherapy in Locally Advanced Rectal Cancer. JCO Precis. Oncol. 2018, 2, 1–15. [Google Scholar] [CrossRef]
- Sirody, J.; Kaji, A.H.; Hari, D.M.; Chen, K.T. Patterns of gastric cancer metastasis in the United States. Am. J. Surg. 2022, 224, 445–448. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | Overall Cohort (n = 68) | Upfront Surgery (n = 18) | NAC (n = 50) | p-Value | ≥cT2N0-3 US (n = 11) | ≥cT2N0-3 NAC (n = 46) | p-Value |
|---|---|---|---|---|---|---|---|
| Demographic Characteristics | |||||||
| Sex, n (%) Male Female | 40 (58.8) 28 (41.2) | 8 (44.4) 10 (55.6) | 32 (64.0) 18 (36.0) | 0.148 | 7 (63.6) 4 (36.4) | 30 (65.2) 16 (34.8) | 0.921 |
| Age at diagnosis, mean (SD) | 62.8 (53.3, 73.3) | 64.6 (+/−18.0) | 65.5 (+/−13.5) | 0.531 | 69.8 (+/−16.6) | 63.0 (+/−13.4) | 0.156 |
| Race, n (%) White Black/African American Asian American Indian/Alaskan native Other | 46 (67.6) 6 (8.8) 8 (11.8) 1 (1.5) 7 (10.3) | 13 (72.2) 1 (5.6) 2 (11.1) - 2 (11.1) | 33 (66.0) 5 (10.0) 6 (12.0) 1 (2.0) 5 (10.0) | 0.944 | 7 (63.6) 1 (9.1) 1 (9.1) - 2 (18.2) | 31 (67.4) 4 (8.7) 6 (13.0) - 5 (10.9) | 0.944 |
| ECOG status 0 1 2 | 36 (52.9) 28 (41.2) 4 (5.9) | 7 (38.9) 9 (50.0) 2 (11.1) | 29 (58.0) 19 (38.0) 2 (4.0) | 0.285 | 4 (36.4) 5 (45.5) 2 (18.2) | 26 (56.5) 18 (39.1) 2 (4.3) | 0.202 |
| Clinicopathologic Characteristics | |||||||
| Clinical T stage, n (%) T1a T1b T2 T3 T4 T4a T4b Missing | 3 (4.4) 7 (10.3) 12 (17.6) 35 (51.5) 1 (1.5) 7 (10.3) 2 (2.9) 1 (1.5) | 2 (11.1) 5 (27.8) 7 (38.9) 3 (16.7) - - 1 (5.6) - | 1 (2.0) 2 (4.0) 5 (10.0) 32 (64.0) 1 (2.0) 7 (14.0) 1 (2.0) 1 (2.0) | <0.001 | - - 7 (63.6) 3 (75.0) - - 1 (9.1) - | - - 5 (10.9) 32 (69.6) 1 (2.2) 7 (15.2) 1 (2.2) - | <0.001 |
| Clinical N stage, n (%) N0 N1-2 Missing | 39 (57.4) 28 (41.2) 1 (1.5) | 16 (88.9) 2 (11.1) - | 23 (46.9) 26 (52.0) 1 (2.1) | 0.002 | 9 (81.8) 2 (18.2) - | 20 (43.5) 25 (54.3) 1 (2.2) | 0.026 |
| Overall clinical stage, n (%) Stage I Stage II Stage III Stage IVa Missing | 19 (27.9) 21 (30.9) 25 (36.8) 2 (2.9) 1 (1.5) | 14 (77.8) 2 (11.1) 1 (5.6) 1 (5.6) | 5 (10.2) 19 (38.0) 24 (48.0) 1 (2.0) 1 (2.0) | <0.001 | 7 (63.6) 2 (18.2) 1 (9.1) 1 (9.1) - | 3 (6.5) 18 (39.1) 24 (52.2) 1 (2.2) - | <0.001 |
| Tumor location, n (%) Distal Proximal Linitis plastica Undefined | 45 (66.2) 18 (26.5) 4 (5.9) 1 (1.5) | 15 (75.0) 2 (10.0) - 1 (5.0) | 30 (60.0) 16 (32.0) 4 (8.0) - | 0.091 | 10 (90.9) - - 1 (9.1) | 26 (56.5) 16 (34.8) 4 (8.7) - | 0.034 |
| Histologic subtype, n (%) Intestinal Diffuse/signet-ring Mixed Neuroendocrine | 24 (35.3) 39 (57.4) 3 (4.4) 2 (2.9) | 9 (50.0) 8 (44.4) - 1 (5.6) | 15 (30.0) 31 (62.0) 3 (6.0) 1 (2.0) | 0.277 | 7 (63.6) 4 (36.4) - - | 15 (32.6) 28 (60.9) 2 (4.3) 1 (2.2) | 0.275 |
| Preoperative and Intraoperative Characteristics | |||||||
| Neoadjuvant regimen, n (%) FOLFOX FLOT EOX DCF ECF ECX Other doublet combination (e.g., XELOX, CAPOX) | 25 (36.8) 6 (8.8) 6 (8.8) 5 (7.4) 2 (2.9) 1 (1.5) 4 (5.9) | - - - - - - - | 25 (36.8) 6 (8.8) 6 (8.8) 5 (7.4) 2 (2.9) 1 (1.5) 4 (5.9) | - | - - - - - - - | 23 (50.0) 6 (13.0) 6 (13.0) 5 (10.9) 1 (2.2) 1 (2.2) 4 (8.7) | - |
| Rounds of chemotherapy | 3.89 (+/−1.7) | - | - | - | 4.0 (3.0–4.0) | - | |
| Neoadjuvant radiation, n (%) No Yes | 65 (95.6) 3 (4.4) | - - | 45 (93.8) 3 (6.3) | 0.288 | 11 (100) | 43 (93.5) 3 (6.5) | 0.288 |
| Type of resection, n (%) Partial gastrectomy Total gastrectomy EMR/ESD | 40 (58.8) 23 (33.8) 5 (7.3) | 9 (50.0) 5 (27.8) 4 (20.0) | 31 (62.0) 18 (36.0) 1 (2.0) | 0.019 | 7 (63.6) 3 (27.3) 1 (9.1) | 28 (60.9) 17 (37.0) 1 (2.2) | 0.482 |
| Pathologic Tumor Characteristics | |||||||
| Pathologic overall stage, n (%) Stage I Stage II Stage III Stage IV | 21 (30.9) 20 (29.4) 20 (29.4) 7 (10.3) | 11 (61.1) 1 (5.6) 5 (27.8) 1 (5.6) | 10 (20.0) 19 (38.0) 15 (30.0) 6 (12.0) | 0.006 | 4 (36.4) 1 (9.1) 5 (45.5) 1 (9.1) | 9 (19.6) 18 (39.1) 15 (32.6) 4 (8.7) | 0.270 |
| Clinical to pathologic stage change, n (%) No change Downstage Upstage Missing | 35 (51.5) 17 (25.0) 15 (22.1) 1 (1.5) | 13 (72.2) 1 (5.6) 4 (22.2) - | 22 (44.0) 16 (32.0) 11 (22.0) 1 (2.0) | 0.058 | 6 (54.5) 1 (9.1) 4 (36.4) - | 21 (45.7) 16 (34.8) 9 (19.6) - | 0.201 |
| Histologic subtype, n (%) Intestinal Diffuse/signet-ring Mixed Neuroendocrine | 24 (35.3) 39 (57.4) 3 (4.4) 2 (2.9) | 9 (45.0) 10 (50.0) 1 (5.0) | 15 (31.3) 29 (60.4) 3 (6.3) 1 (2.1) | 0.443 | 7 (63.6) 4 (36.4) - - | 15 (32.6) 28 (60.9) 2 (4.3) 1 (2.2) | 0.275 |
| Histologic differentiation, n (%) Poor Poor–moderate Moderate Mod to well Well | 42 (61.8) 5 (7.4) 17 (25.0) 1 (1.5) 3 (4.4) | 7 (38.9) 2 (11.1) 6 (33.3) 1 (5.6) 2 (11.1) | 35 (70.0) 3 (6.0) 11 (22.0) - 1 (2.0) | 0.075 | 3 (27.3) 2 (18.2) 5 (45.5) 1 (9.1) - | 31 (67.4) 3 (6.5) 11 (23.9) - 1 (2.2) | 0.047 |
| Margin status, n (%) R0 R1 R2 | 58 (85.3) 10 (14.7) - | 18 (100) - - | 40 (80.0) 10 (20.0) - | 0.040 | 11 (100) - | 37 (80.4) 9 (19.6) - | 0.040 |
| Treatment effect, n (%) Minimal residual disease (CRS 3) Moderate response (CRS 2) Poor response (CRS 1) Unknown | 4 (8.0) 21 (42.0) 22 (44.0) 3 (6.0) | - | 4 (8.0) 21 (42.0) 22 (44.0) 3 (6.0) | - | - | 4 (8.7) 20 (43.5) 19 (41.3) 3 (6.5) | - |
| Molecular Phenotype and Tumor-Infiltrating Lymphocyte Profiles | |||||||
|---|---|---|---|---|---|---|---|
| Overall Cohort (n = 68) | Upfront Surgery (n = 18) | NAC (n = 50) | p-Value | ≥cT2N0-3 US (n = 11) | ≥cT2N0-3 NAC (n = 46) | p-Value | |
| EBV status, n (%) Negative Positive | 65 (95.6) 3 (4.4) | 18 (100) - | 47 (94.0) 3 (6.0) | 0.288 | 11 (100) - | 43 (93.5) 3 (6.5) | 0.384 |
| MMR, n (%) Proficient Deficient | 60 (88.2) 8 (11.8) | 17 (94.4) 1 (5.6) | 43 (86.0) 7 (14.0) | 0.340 | 10 (90.9) 1 (9.1) | 40 (87.0) 6 (13.0) | 0.720 |
| PD-L1 status, n (%) Negative Positive | 41 (60.3) 27 (39.7) | 11 (61.1) 7 (38.9) | 30 (60.0) 20 (40.0) | 0.934 | 7 (63.6) 4 (36.4) | 27 (58.7) 19 (41.3) | 0.764 |
| Tumor-Infiltrating Lymphocyte Densities—Intratumoral | |||||||
| CD8+ T cells, cells/mm2 Conventional (CD8+) Memory (CD8+/CD45RO+) | 8.6 (3.4, 37.1) 1.8 (0.8, 9.0) | 5.1 (2.1, 8.5) 1.0 (0.6, 4.8) | 14.25 (4.3, 43.7) 2.3 (1.1, 10.8) | 0.024 0.119 | 3.6 (2.0, 8.1) 0.7 (0.4, 3.1) | 14.2 (4.0, 43.7) 2.0 (1.0, 11.6) | 0.019 0.050 |
| CD4+ T cells, cells/mm2 Conventional (CD4+) Memory (CD4+/CD45RO+) | 3.4 (0.8, 8.0) 1.6 (0.4, 5.0) | 1.7 (0.6, 5.7) 0.8 (0.3, 3.3) | 4.5 (0.8, 9.2) 2.1 (0.6, 5.6) | 0.182 0.254 | 1.5 (0.3, 3.2) 0.6 (0.2, 1.7) | 4.2 (0.9, 8.3) 1.6 (0.5, 5.4) | 0.089 0.119 |
| Treg cells, cells/mm2 Conventional (CD4+/FOXP3+) Memory (CD4+/CD45RO+) | 0.4 (0.1, 1.7) 0.2 (0.04, 1.7) | 0.5 (0.04, 1.5) 0.2 (0.02, 1.2) | 0.4 (0.1, 1.9) 0.2 (0.04, 0.9) | 0.671 0.950 | 0.3 (0.1, 1.1) 0.1 (0.04, 0.4) | 0.4 (0.1, 1.9) 0.2 (0.03, 0.8) | 0.442 0.754 |
| B cells, cells/mm2 Conventional (CD220+) Memory (CD220+/CD45RO+) | 0.02 (0.003, 0.15) 0 | 0.01 (0.01, 0.09) 0 | 0.04 (0.0, 0.16) 0 | 0.550 | 0.01 (0.0, 0.01) 0.0 | 0.03 (0.0, 0.16) 0.0 | 0.088 |
| All TILs (CD8+, CD4+, B cell) | 13.6 (5.5, 49.6) | 7.9 (4.1, 15.4) | 19.3 (5.6, 53.9) | 0.047 | 6.7 (2.8, 9.6) | 18.8 (5.4, 53.9) | 0.041 |
| ALL memory TILs | 0.3 (0.03, 2.3) | 0.11 (0.01, 0.49) | 0.28 (0.05, 3.48) | 0.098 | 0.05 (0.01, 0.3) | 0.2 (0.04, 3.1) | 0.048 |
| CD8:Treg ratio | 23.2 (6.6, 3.4) | 7.8 (3.7, 53.3) | 25.5 (12.4, 54.6) | 0.123 | 7.5 (3.1, 29.5) | 25.5 (7.0, 55.2) | 0.079 |
| Tumor-Infiltrating Lymphocyte Densities—Stromal | |||||||
| CD8+ T cells, cells/mm2 Conventional (CD8+) Memory (CD8+/CD45RO+) | 4.9 (1.6, 19.0) 3.3 (1.0, 11.6) | 6.4 (1.2, 21.4) 4.4 (0.9, 13.8) | 4.6 (1.8, 18.1) 3.1 (1.0, 8.8) | 0.597 0.396 | 2.3 (1.1, 8.4) 1.45 (0.6, 7.3) | 4.6 (1.9, 19.6) 3.1 (1.0, 10.2) | 0.203 0.385 |
| CD4+ T cells, cells/mm2 Conventional (CD4+) Memory (CD4+/CD45RO+) | 23.2 (6.3, 53.1) 9.7 (2.4, 29.0) | 23.6 (7.1, 73.7) 11.1 (3.0, 40.1) | 23.2 (6.0, 50.4) 8.4 (2.3, 21.0) | 0.906 0.359 | 8.9 (4.5, 21.2) 4.2 (1.8, 21.2) | 23.2 (7.0, 54.2) 8.4 (2.6, 22.7) | 0.143 0.454 |
| Treg cells, cells/mm2 Conventional (CD4+/FOXP3+) Memory (CD4+/CD45RO+) | 1.3 (0.2, 3.4) 0.5 (0.1, 1.8) | 1.0 (0.5, 4.9) 0.6 (0.2, 1.7) | 1.4 (0.2, 2.8) 0.5 (0.1, 1.3) | 0.592 0.254 | 0.8 (0.2, 4.1) 0.5 (0.1, 1.8) | 1.4 (0.2, 3.3) 0.5 (0.1, 1.7) | 0.716 0.952 |
| B cells, cells/mm2 Conventional (CD220+) Memory (CD220+/CD45RO+) | 1.2 (04, 6.7) 0.1 (0.02, 1.2) | 1.3 (0.6, 10.0) 0.2 (0.02, 1.7) | 0.9 (0.3, 5.6) 0.1 (0.2, 0.6) | 0.294 0.555 | 0.9 (0.2, 1.3) 0.3 (0.02, 0.3) | 1.1 (0.3, 6.6) 0.1 (0.02, 0.9) | 0.379 0.201 |
| All TILs (CD8+, CD4+, B cell) | 36.1 (8.6, 74.9) | 31.0 (8.7, 97.8) | 37.4 (8.3, 71.1) | 0.889 | 15.6 (5.3, 39.4) | 37.4 (10.6, 73.3) | 0.110 |
| CD8:Treg ratio | 3.6 (2.3, 10.3) | 3.4 (1.4, 16.2) | 3.6 (2.4, 9.6) | 0.479 | 2.3 (1.2, 4.8) | 3.6 (2.3, 9.6) | 0.152 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yee, E.J.; Gilbert, D.; Kaplan, J.; Wani, S.; Kim, S.S.; McCarter, M.D.; Stewart, C.L. Effect of Neoadjuvant Chemotherapy on Tumor-Infiltrating Lymphocytes in Resectable Gastric Cancer: Analysis from a Western Academic Center. Cancers 2024, 16, 1428. https://doi.org/10.3390/cancers16071428
Yee EJ, Gilbert D, Kaplan J, Wani S, Kim SS, McCarter MD, Stewart CL. Effect of Neoadjuvant Chemotherapy on Tumor-Infiltrating Lymphocytes in Resectable Gastric Cancer: Analysis from a Western Academic Center. Cancers. 2024; 16(7):1428. https://doi.org/10.3390/cancers16071428
Chicago/Turabian StyleYee, Elliott J., Danielle Gilbert, Jeffrey Kaplan, Sachin Wani, Sunnie S. Kim, Martin D. McCarter, and Camille L. Stewart. 2024. "Effect of Neoadjuvant Chemotherapy on Tumor-Infiltrating Lymphocytes in Resectable Gastric Cancer: Analysis from a Western Academic Center" Cancers 16, no. 7: 1428. https://doi.org/10.3390/cancers16071428
APA StyleYee, E. J., Gilbert, D., Kaplan, J., Wani, S., Kim, S. S., McCarter, M. D., & Stewart, C. L. (2024). Effect of Neoadjuvant Chemotherapy on Tumor-Infiltrating Lymphocytes in Resectable Gastric Cancer: Analysis from a Western Academic Center. Cancers, 16(7), 1428. https://doi.org/10.3390/cancers16071428