
Evaluation of Helium Ion Radiotherapy in Combination with Gemcitabine in Pancreatic Cancer In Vitro
 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Cell Culture and Reagents
2.2. Photon Radiotherapy
2.3. Helium Ion Radiotherapy
2.4. Gemcitabine Therapy
2.5. Clonogenic Assay
2.6. Combined Chemo- and Radiotherapy
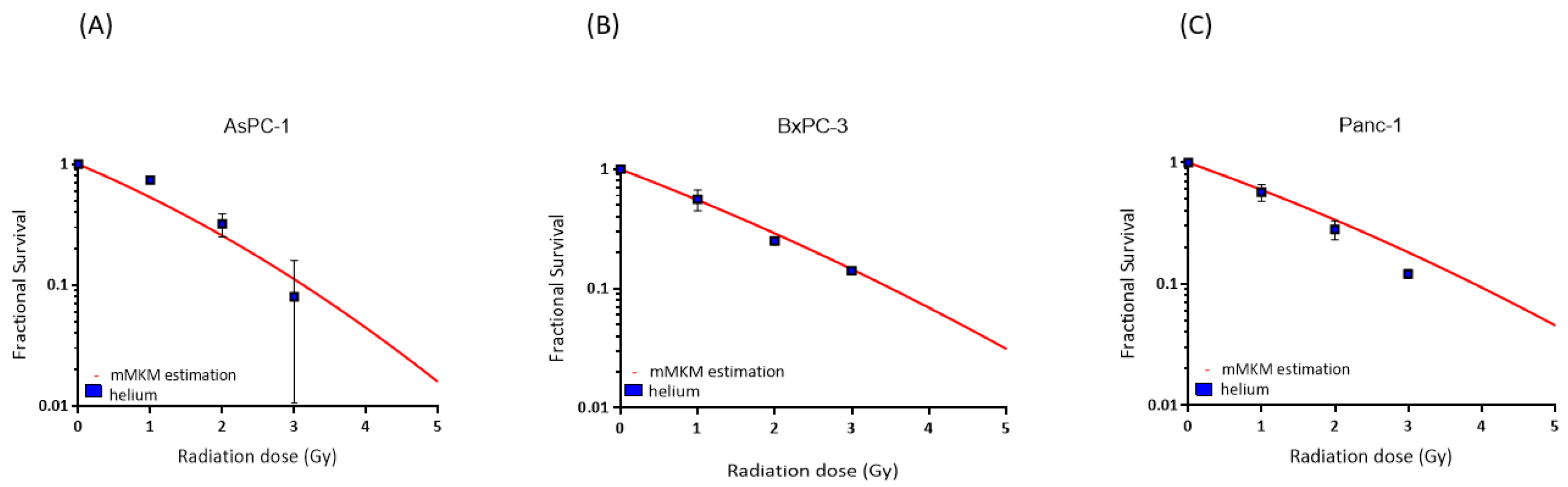
2.7. RBE-Weighted Dose Calculation with mMKM
3. Results
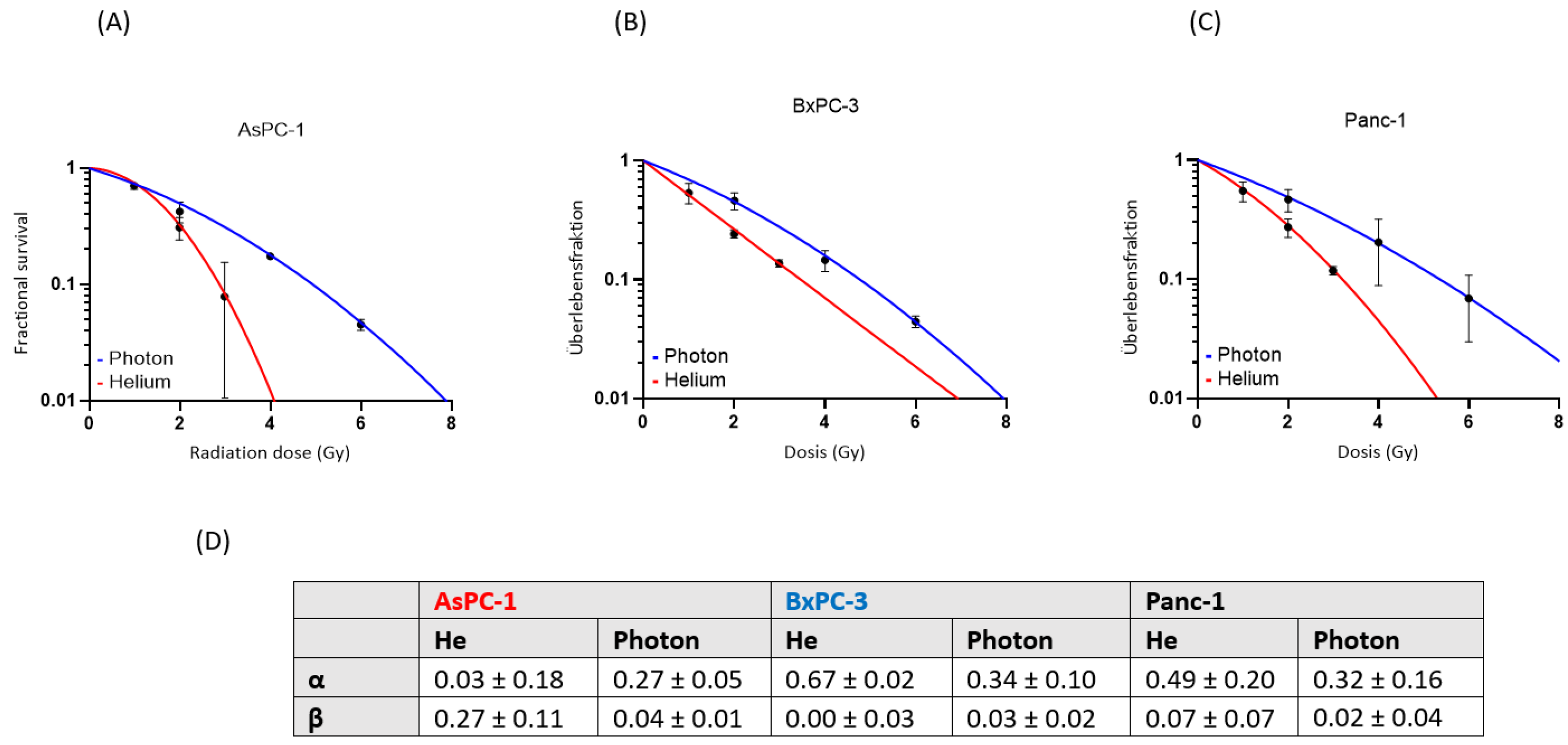
3.1. Clonogenic Survival and RBE after Photon versus Helium Irradiation and Gemcitabine Treatment
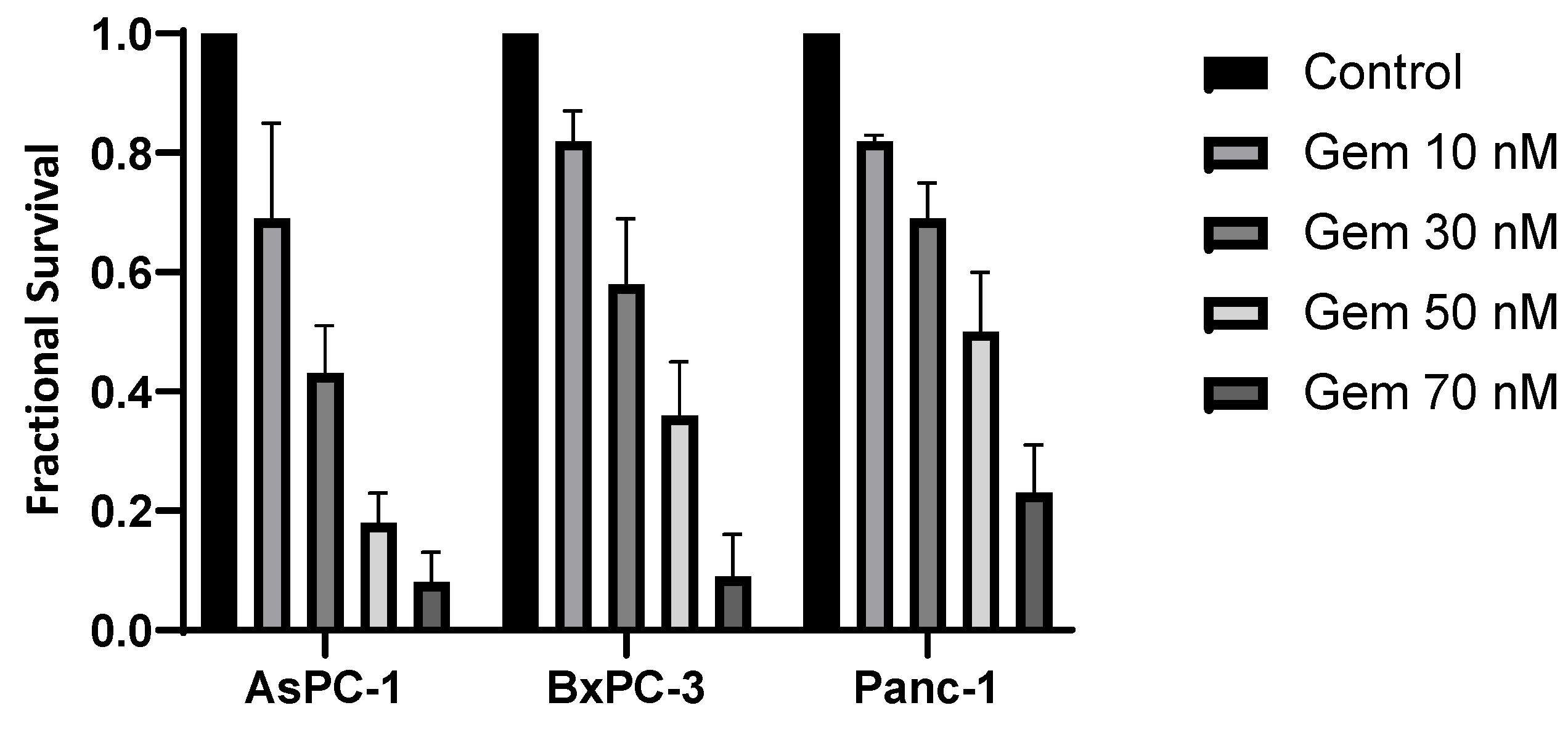
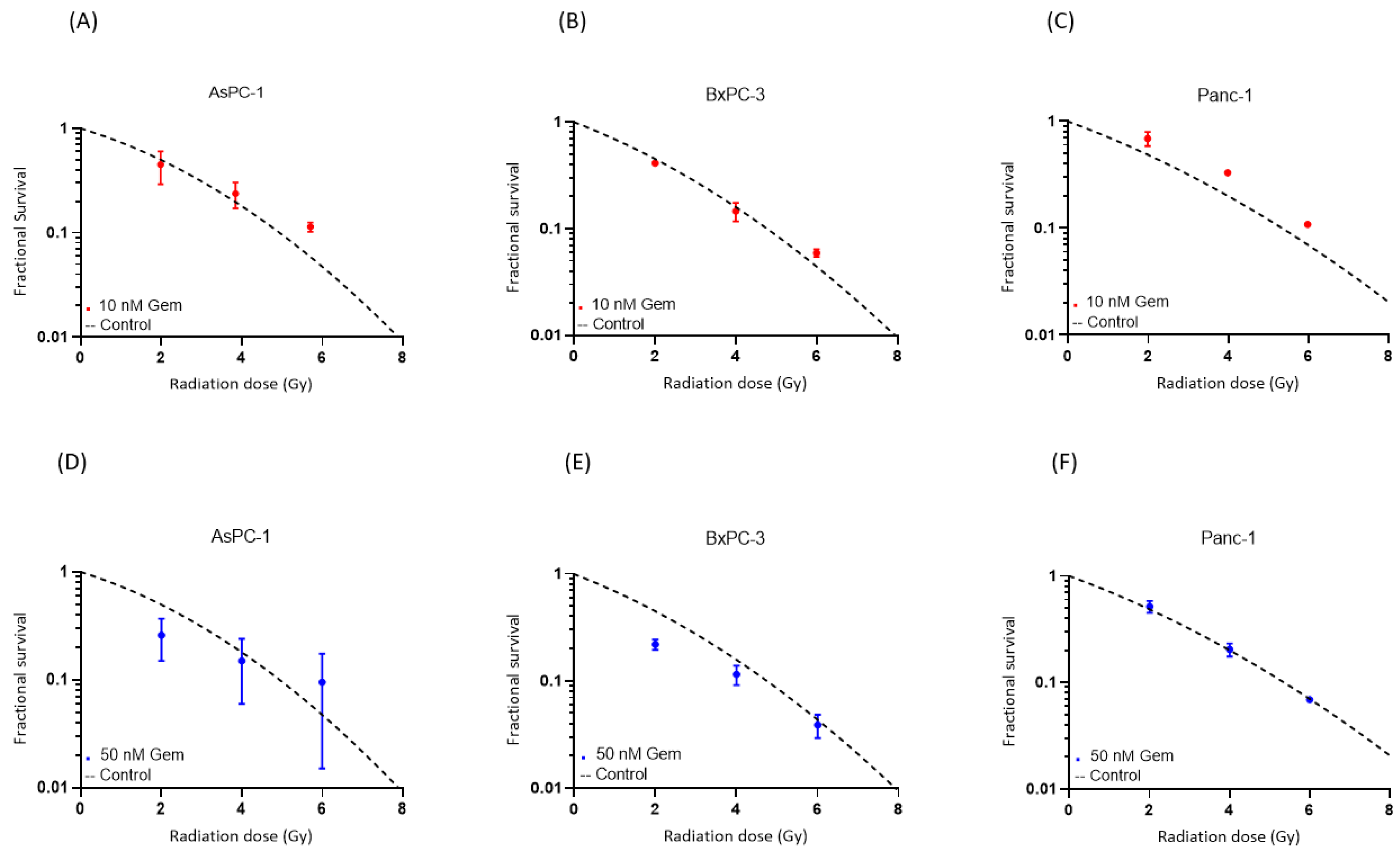
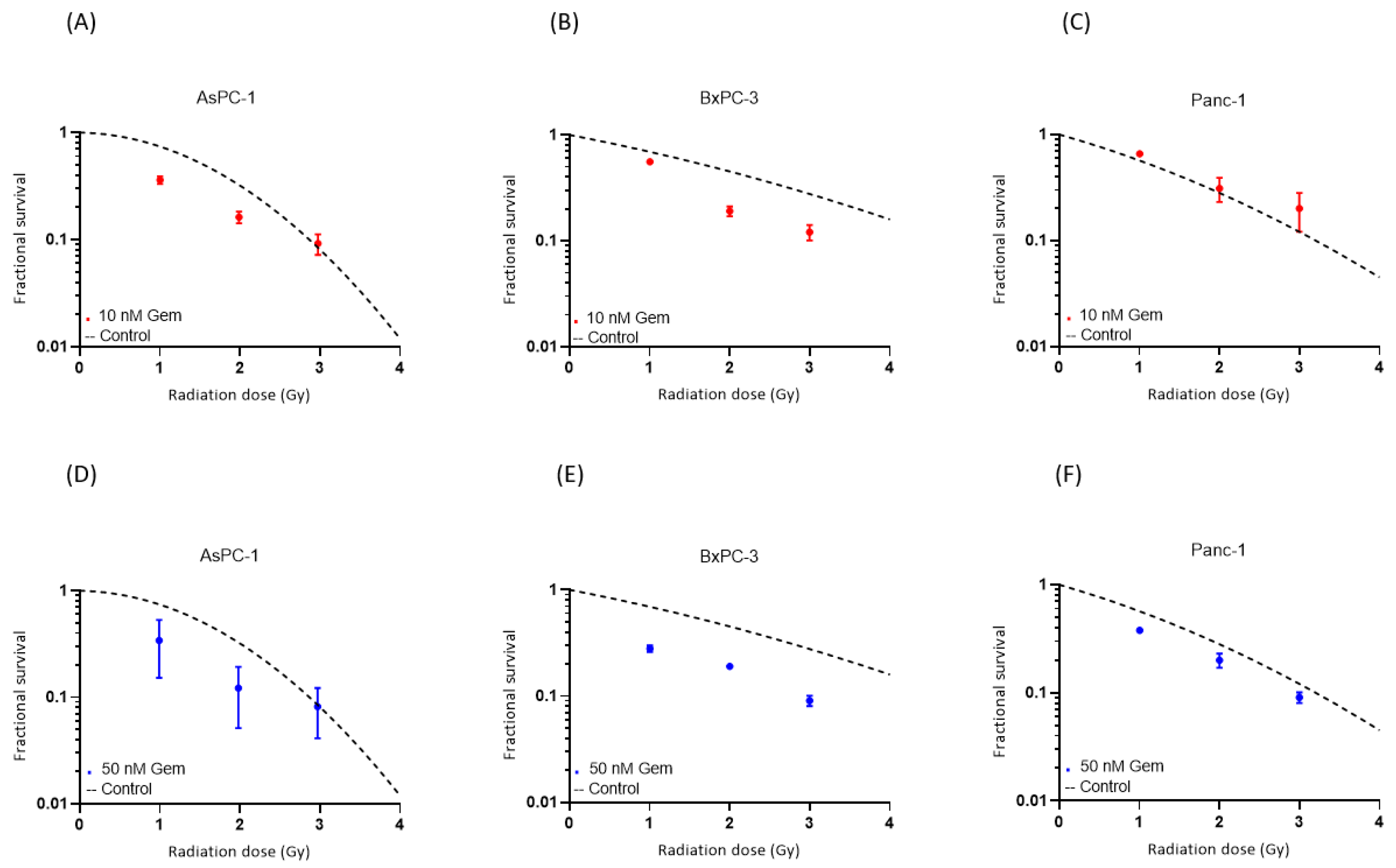
3.2. Cytotoxic Effect of Combined Chemo- and Radiotherapy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Khalaf, N.; El-Serag, H.B.; Abrams, H.R.; Thrift, A.P. Burden of Pancreatic Cancer: From Epidemiology to Practice. Clin. Gastroenterol. Hepatol. 2021, 19, 876–884. [Google Scholar] [CrossRef] [PubMed]
- Luo, W.; Tao, J.; Zheng, L.; Zhang, T. Current epidemiology of pancreatic cancer: Challenges and opportunities. Chin. J. Cancer Res. 2020, 32, 705–719. [Google Scholar] [CrossRef]
- Hermann, S.; Kraywinkel, K. Epidemiologie des Pankreaskarzinoms in Deutschland. Der Onkologe 2019, 25, 647–652. [Google Scholar] [CrossRef]
- Zhang, L.; Sanagapalli, S.; Stoita, A. Challenges in diagnosis of pancreatic cancer. World J. Gastroenterol. 2018, 24, 2047–2060. [Google Scholar] [CrossRef] [PubMed]
- Müller, P.C.; Frey, M.C.; Ruzza, C.M.; Nickel, F.; Jost, C.; Gwerder, C.; Hackert, T.; Z’Graggen, K.; Kessler, U. Neoadjuvant Chemotherapy in Pancreatic Cancer: An Appraisal of the Current High-Level Evidence. Pharmacology 2021, 106, 143–153. [Google Scholar] [CrossRef] [PubMed]
- Kunzmann, V.; Algül, H.; Goekkurt, E.; Siegler, G.M.; Martens, U.M.; Waldschmidt, D.; Pelzer, U.; Hennes, E.; Fuchs, M.; Siveke, J.; et al. Conversion rate in locally advanced pancreatic cancer (LAPC) after nab-paclitaxel/gemcitabine- or FOLFIRINOX-based induction chemotherapy (NEOLAP): Final results of a multicenter randomised phase II AIO trial. Ann. Oncol. 2019, 30, v253–v324. [Google Scholar] [CrossRef]
- Versteijne, E.; Suker, M.; Groothuis, K.; Akkermans-Vogelaar, J.M.; Besselink, M.G.; Bonsing, B.A.; Buijsen, J.; Busch, O.R.; Creemers, G.M.; van Dam, R.M.; et al. Preoperative Chemoradiotherapy Versus Immediate Surgery for Resectable and Borderline Resectable Pancreatic Cancer: Results of the Dutch Randomized Phase III PREOPANC Trial. J. Clin. Oncol. 2020, 38, 1763–1773. [Google Scholar] [CrossRef] [PubMed]
- Ghaneh, P.; Palmer, D.H.; Cicconi, S.; Halloran, C.; Psarelli, E.E.; Rawcliffe, C.L.; Sripadam, R.; Mukherjee, S.; Wadsley, J.; Al-Mukhtar, A.; et al. ESPAC-5F: Four-arm, prospective, multicenter, international randomized phase II trial of immediate surgery compared with neoadjuvant gemcitabine plus capecitabine (GEMCAP) or FOLFIRINOX or chemoradiotherapy (CRT) in patients with borderline resectable pancreatic cancer. J. Clin. Oncol. 2020, 38, 4505. [Google Scholar] [CrossRef]
- Feig, C.; Gopinathan, A.; Neesse, A.; Chan, D.S.; Cook, N.; Tuveson, D.A. The pancreas cancer microenvironment. Clin. Cancer Res. 2012, 18, 4266–4276. [Google Scholar] [CrossRef]
- Byun, H.K.; Han, M.C.; Yang, K.; Kim, J.S.; Yoo, G.S.; Koom, W.S.; Kim, Y.B. Physical and Biological Characteristics of Particle Therapy for Oncologists. Cancer Res. Treat. 2021, 53, 611–620. [Google Scholar] [CrossRef]
- Mohamad, O.; Sishc, B.J.; Saha, J.; Pompos, A.; Rahimi, A.; Story, M.D.; Davis, A.J.; Kim, D.W.N. Carbon Ion Radiotherapy: A Review of Clinical Experiences and Preclinical Research, with an Emphasis on DNA Damage/Repair. Cancers 2017, 9, 66. [Google Scholar] [CrossRef] [PubMed]
- Lopez Perez, R.; Nicolay, N.H.; Wolf, J.C.; Frister, M.; Schmezer, P.; Weber, K.J.; Huber, P.E. DNA damage response of clinical carbon ion versus photon radiation in human glioblastoma cells. Radiother. Oncol. 2019, 133, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Knäusl, B.; Fuchs, H.; Dieckmann, K.; Georg, D. Can particle beam therapy be improved using helium ions?—A planning study focusing on pediatric patients. Acta Oncol. 2016, 55, 751–759. [Google Scholar] [CrossRef] [PubMed]
- Woodruff, K.H.; Castro, J.R.; Quivey, J.M.; Saunders, W.M.; Chen, G.T.; Lyman, J.T.; Pitluck, S.; Tobias, C.A.; Walton, R.E.; Peters, T.C. Postmortem examination of 22 pancreatic carcinoma patients treated with helium ion irradiation. Cancer 1984, 53, 420–425. [Google Scholar] [CrossRef] [PubMed]
- Saunders, W.; Castro, J.R.; Chen, G.T.; Collier, J.M.; Zink, S.R.; Pitluck, S.; Phillips, T.L.; Char, D.; Gutin, P.; Gauger, G.; et al. Helium-ion radiation therapy at the Lawrence Berkeley Laboratory: Recent results of a Northern California Oncology Group Clinical Trial. Radiat. Res. Suppl. 1985, 8, S227–S234. [Google Scholar] [CrossRef] [PubMed]
- Castro, J.R.; Char, D.H.; Petti, P.L.; Daftari, I.K.; Quivey, J.M.; Singh, R.P.; Blakely, E.A.; Phillips, T.L. 15 years experience with helium ion radiotherapy for uveal melanoma. Int. J. Radiat. Oncol. Biol. Phys. 1997, 39, 989–996. [Google Scholar] [CrossRef] [PubMed]
- Bonaccorsi, S.G.; Tessonnier, T.; Hoeltgen, L.; Meixner, E.; Harrabi, S.; Hörner-Rieber, J.; Haberer, T.; Abdollahi, A.; Debus, J.; Mairani, A. Exploring Helium Ions’ Potential for Post-Mastectomy Left-Sided Breast Cancer Radiotherapy. Cancers 2024, 16, 410. [Google Scholar] [CrossRef] [PubMed]
- Kopp, B.; Mein, S.; Tessonnier, T.; Besuglow, J.; Harrabi, S.; Heim, E.; Abdollahi, A.; Haberer, T.; Debus, J.; Mairani, A. Rapid effective dose calculation for raster-scanning (4)He ion therapy with the modified microdosimetric kinetic model (mMKM). Phys. Med. 2021, 81, 273–284. [Google Scholar] [CrossRef] [PubMed]
- Tan, M.H.; Nowak, N.J.; Loor, R.; Ochi, H.; Sandberg, A.A.; Lopez, C.; Pickren, J.W.; Berjian, R.; Douglass, H.O., Jr.; Chu, T.M. Characterization of a new primary human pancreatic tumor line. Cancer Investig. 1986, 4, 15–23. [Google Scholar] [CrossRef]
- Chen, W.H.; Horoszewicz, J.S.; Leong, S.S.; Shimano, T.; Penetrante, R.; Sanders, W.H.; Berjian, R.; Douglass, H.O.; Martin, E.W.; Chu, T.M. Human pancreatic adenocarcinoma: In vitro and in vivo morphology of a new tumor line established from ascites. In Vitro Cell. Dev. Biol.-Plant 1982, 18, 24–34. [Google Scholar] [CrossRef]
- Loukopoulos, P.; Kanetaka, K.; Takamura, M.; Shibata, T.; Sakamoto, M.; Hirohashi, S. Orthotopic transplantation models of pancreatic adenocarcinoma derived from cell lines and primary tumors and displaying varying metastatic activity. Pancreas 2004, 29, 193–203. [Google Scholar] [CrossRef] [PubMed]
- Franken, N.A.; Rodermond, H.M.; Stap, J.; Haveman, J.; van Bree, C. Clonogenic assay of cells in vitro. Nat. Protoc. 2006, 1, 2315–2319. [Google Scholar] [CrossRef] [PubMed]
- Steel, G.G.; Peckham, M.J. Exploitable mechanisms in combined radiotherapy-chemotherapy: The concept of additivity. Int. J. Radiat. Oncol. Biol. Phys. 1979, 5, 85–91. [Google Scholar] [CrossRef]
- Mairani, A.; Magro, G.; Dokic, I.; Valle, S.M.; Tessonnier, T.; Galm, R.; Ciocca, M.; Parodi, K.; Ferrari, A.; Jäkel, O.; et al. Data-driven RBE parameterization for helium ion beams. Phys. Med. Biol. 2016, 61, 888–905. [Google Scholar] [CrossRef] [PubMed]
- Paganetti, H.; Niemierko, A.; Ancukiewicz, M.; Gerweck, L.E.; Goitein, M.; Loeffler, J.S.; Suit, H.D. Relative biological effectiveness (RBE) values for proton beam therapy. Int. J. Radiat. Oncol. Biol. Phys. 2002, 53, 407–421. [Google Scholar] [CrossRef] [PubMed]
- Tinganelli, W.; Durante, M. Carbon Ion Radiobiology. Cancers 2020, 12, 3022. [Google Scholar] [CrossRef]
- Wang, T.; Zhuang, Z.; Zhang, P.; Wang, Y.; Mu, L.; Jin, H.; Zhou, L.; Ma, X.; Liang, R.; Yuan, Y. Effect of arenobufagin on human pancreatic carcinoma cells. Oncol. Lett. 2017, 14, 4971–4976. [Google Scholar] [CrossRef] [PubMed]
- El Shafie, R.A.; Habermehl, D.; Rieken, S.; Mairani, A.; Orschiedt, L.; Brons, S.; Haberer, T.; Weber, K.J.; Debus, J.; Combs, S.E. In vitro evaluation of photon and raster-scanned carbon ion radiotherapy in combination with gemcitabine in pancreatic cancer cell lines. J. Radiat. Res. 2013, 54 (Suppl S1), i113–i119. [Google Scholar] [CrossRef] [PubMed]
- Weber, K.-J.; Wenz, F. Strahlenbiologische Grundlagen. In Strahlentherapie; Wannenmacher, M., Debus, J., Wenz, F., Eds.; Springer: Berlin/Heidelberg, Germany, 2006. [Google Scholar]
- Wenzl, T.; Wilkens, J.J. Modelling of the oxygen enhancement ratio for ion beam radiation therapy. Phys. Med. Biol. 2011, 56, 3251–3268. [Google Scholar] [CrossRef]
- Mose, S.; Class, R.; Weber, H.W.; Rahn, A.; Brady, L.W.; Böttcher, H.D. Radiation enhancement by gemcitabine-mediated cell cycle modulations. Am. J. Clin. Oncol. 2003, 26, 60–69. [Google Scholar] [CrossRef]
- Principe, D.R.; Underwood, P.W.; Korc, M.; Trevino, J.G.; Munshi, H.G.; Rana, A. The Current Treatment Paradigm for Pancreatic Ductal Adenocarcinoma and Barriers to Therapeutic Efficacy. Front. Oncol. 2021, 11, 688377. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Russell, C.C.; Scarlett, C.J.; McCluskey, A. Small molecule inhibitors in pancreatic cancer. RSC Med. Chem. 2020, 11, 164–183. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; Hegde, S.; Knolhoff, B.L.; Zhu, Y.; Herndon, J.M.; Meyer, M.A.; Nywening, T.M.; Hawkins, W.G.; Shapiro, I.M.; Weaver, D.T.; et al. Targeting focal adhesion kinase renders pancreatic cancers responsive to checkpoint immunotherapy. Nat. Med. 2016, 22, 851–860. [Google Scholar] [CrossRef]
- Carbone, D.; De Franco, M.; Pecoraro, C.; Bassani, D.; Pavan, M.; Cascioferro, S.; Parrino, B.; Cirrincione, G.; Dall’Acqua, S.; Moro, S.; et al. Discovery of the 3-Amino-1,2,4-triazine-Based Library as Selective PDK1 Inhibitors with Therapeutic Potential in Highly Aggressive Pancreatic Ductal Adenocarcinoma. Int. J. Mol. Sci. 2023, 24, 3679. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Experimental | RBE | ||
|---|---|---|---|
| Radiation Dose | AsPC-1 | BxPC-3 | Panc-1 |
| 1 Gy | 0.96 | 1.71 | 1.65 |
| 2 Gy | 1.44 | 1.58 | 1.66 |
| 3 Gy | 1.69 | 1.40 | 1.67 |
| mMKM | RBE | ||
|---|---|---|---|
| Radiation Dose | AsPC-1 | BxPC-3 | Panc-1 |
| 1 Gy | 1.75 | 1.55 | 1.43 |
| 2 Gy | 1.60 | 1.48 | 1.38 |
| 3 Gy | 1.50 | 1.41 | 1.35 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cepni, B.; Tessonnier, T.; Dokic, I.; Brons, S.; Tawk, B.; Mairani, A.; Abdollahi, A.; Debus, J.; Herfarth, K.; Liermann, J. Evaluation of Helium Ion Radiotherapy in Combination with Gemcitabine in Pancreatic Cancer In Vitro. Cancers 2024, 16, 1497. https://doi.org/10.3390/cancers16081497
Cepni B, Tessonnier T, Dokic I, Brons S, Tawk B, Mairani A, Abdollahi A, Debus J, Herfarth K, Liermann J. Evaluation of Helium Ion Radiotherapy in Combination with Gemcitabine in Pancreatic Cancer In Vitro. Cancers. 2024; 16(8):1497. https://doi.org/10.3390/cancers16081497
Chicago/Turabian StyleCepni, Bahar, Thomas Tessonnier, Ivana Dokic, Stephan Brons, Bouchra Tawk, Andrea Mairani, Amir Abdollahi, Jürgen Debus, Klaus Herfarth, and Jakob Liermann. 2024. "Evaluation of Helium Ion Radiotherapy in Combination with Gemcitabine in Pancreatic Cancer In Vitro" Cancers 16, no. 8: 1497. https://doi.org/10.3390/cancers16081497