


Reactivation of Varicella-Zoster Virus in Patients with Lung Cancer Receiving Immune Checkpoint Inhibitors: Retrospective Nationwide Population-Based Cohort Study from South Korea
 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
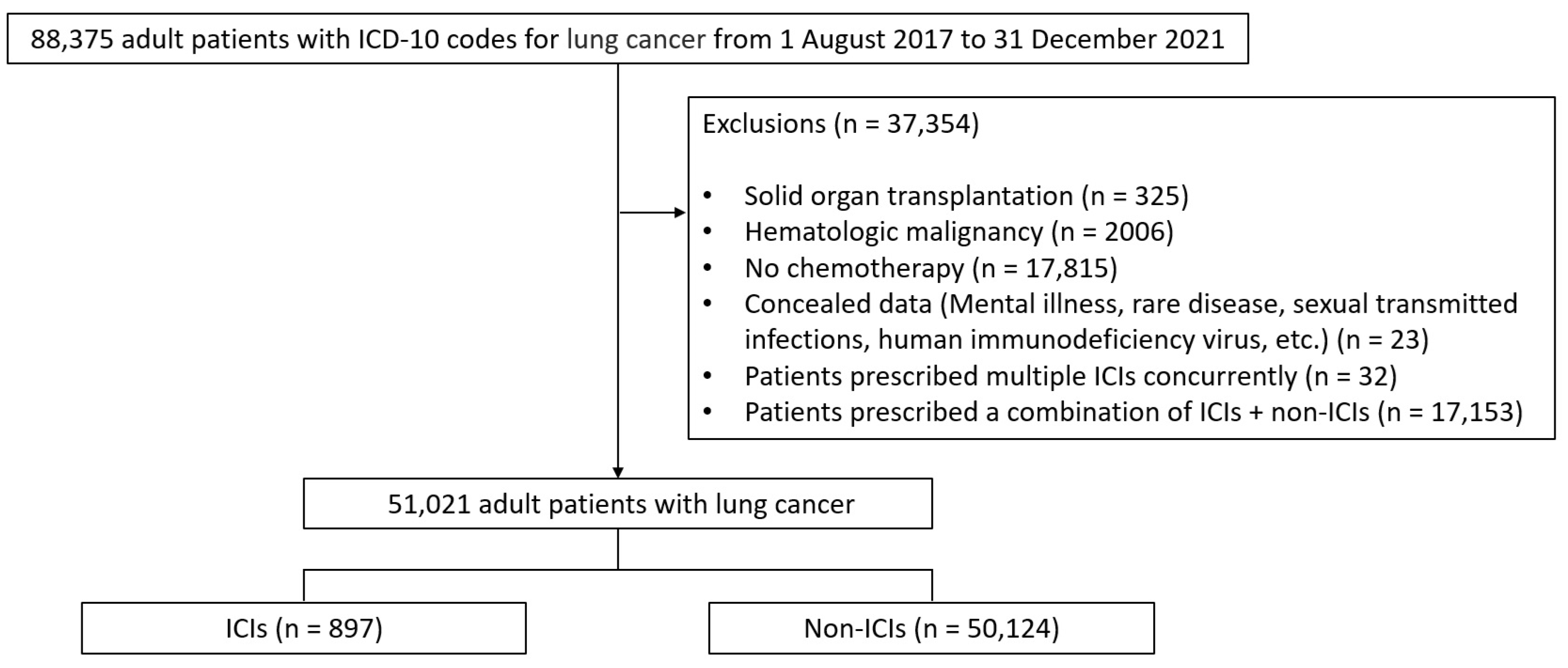
2.1. Study Design, Database, and Population
2.2. Definitions and Outcomes
2.3. Statistical Analyses
3. Results
3.1. Patient Disposition and Baseline Characteristics
3.2. Incidence Rate and Standardized Incidence Ratio of HZ in the ICI and Non-ICI Groups
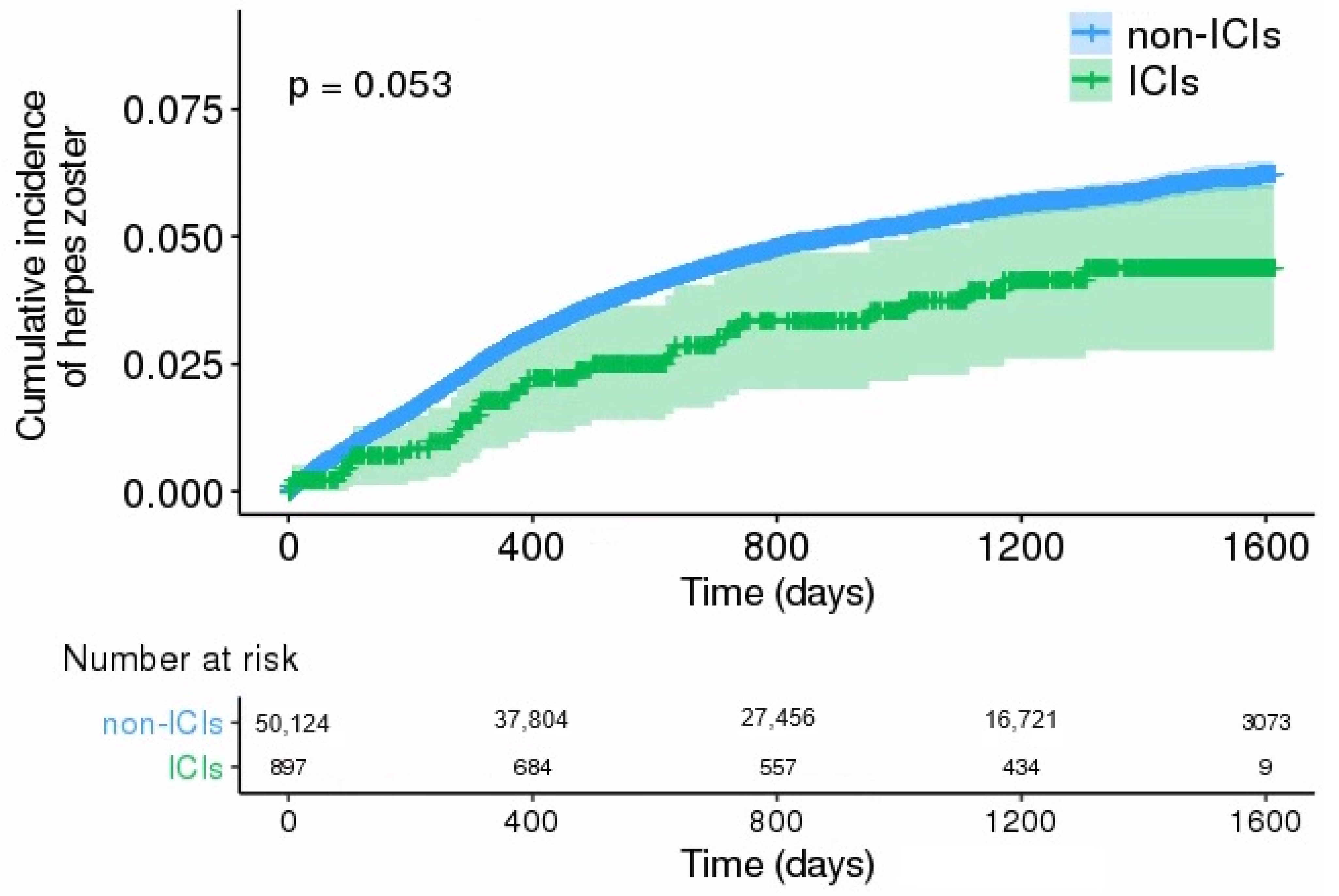
3.3. Comparison of HZ Incidence between ICI and Non-ICI Groups
3.4. Risk Factors for Development of HZ in Patients with Lung Cancer
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cohen, J.I. Herpes zoster. N. Engl. J. Med. 2013, 369, 1766–1767. [Google Scholar] [CrossRef]
- Gershon, A.A.; Gershon, M.D.; Breuer, J.; Levin, M.J.; Oaklander, A.L.; Griffiths, P.D. Advances in the understanding of the pathogenesis and epidemiology of herpes zoster. J. Clin. Virol. 2010, 48 (Suppl. 1), S2–S7. [Google Scholar] [CrossRef] [PubMed]
- Oxman, M.N. Immunization to reduce the frequency and severity of herpes zoster and its complications. Neurology 1995, 45, S41–S46. [Google Scholar] [CrossRef] [PubMed]
- Arvin, A.M.; Moffat, J.F.; Redman, R. Varicella-zoster virus: Aspects of pathogenesis and host response to natural infection and varicella vaccine. Adv. Virus Res. 1996, 46, 263–309. [Google Scholar] [CrossRef] [PubMed]
- Donahue, J.G.; Choo, P.W.; Manson, J.E.; Platt, R. The incidence of herpes zoster. Arch. Intern. Med. 1995, 155, 1605–1609. [Google Scholar] [CrossRef] [PubMed]
- McKay, S.L.; Guo, A.; Pergam, S.A.; Dooling, K. Herpes Zoster Risk in Immunocompromised Adults in the United States: A Systematic Review. Clin. Infect. Dis. 2020, 71, e125–e134. [Google Scholar] [CrossRef]
- Lin, Y.H.; Huang, L.M.; Chang, I.S.; Tsai, F.Y.; Lu, C.Y.; Shao, P.L.; Chang, L.Y.; Varicella-Zoster Working, G.; Advisory Committee on Immunization Practices, T. Disease burden and epidemiology of herpes zoster in pre-vaccine Taiwan. Vaccine 2010, 28, 1217–1220. [Google Scholar] [CrossRef] [PubMed]
- Yenikomshian, M.A.; Guignard, A.P.; Haguinet, F.; LaCasce, A.S.; Skarin, A.T.; Trahey, A.; Karner, P.; Duh, M.S. The epidemiology of herpes zoster and its complications in Medicare cancer patients. BMC Infect. Dis. 2015, 15, 106. [Google Scholar] [CrossRef] [PubMed]
- Ribas, A.; Wolchok, J.D. Cancer immunotherapy using checkpoint blockade. Science 2018, 359, 1350–1355. [Google Scholar] [CrossRef] [PubMed]
- Dine, J.; Gordon, R.; Shames, Y.; Kasler, M.K.; Barton-Burke, M. Immune Checkpoint Inhibitors: An Innovation in Immunotherapy for the Treatment and Management of Patients with Cancer. Asia Pac. J. Oncol. Nurs. 2017, 4, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, Y.; Kikuchi, R.; Iwai, Y.; Ito, M.; Tsukamoto, H.; Yamazaki, K.; Nakamura, H.; Aoshiba, K. Varicella zoster virus encephalitis mimicking nivolumab-induced autoimmune neuropathy in a patient with lung cancer. J. Thorac. Oncol. 2019, 14, e163–e165. [Google Scholar] [CrossRef] [PubMed]
- Sakoh, T.; Kanzaki, M.; Miyamoto, A.; Mochizuki, S.; Kakumoto, T.; Sato, K.; Uesaka, Y.; Kishi, K. Ramsay-Hunt syndrome and subsequent sensory neuropathy as potential immune-related adverse events of nivolumab: A case report. BMC Cancer 2019, 19, 1220. [Google Scholar] [CrossRef] [PubMed]
- Gozzi, E.; Rossi, L.; Angelini, F.; Leoni, V.; Trenta, P.; Cimino, G.; Tomao, S. Herpes zoster granulomatous dermatitis in metastatic lung cancer treated with nivolumab: A case report. Thorac. Cancer 2020, 11, 1330–1333. [Google Scholar] [CrossRef] [PubMed]
- Taoka, M.; Ochi, N.; Yamane, H.; Yamamoto, T.; Kawahara, T.; Uji, E.; Kosaka, Y.; Takeda, K.; Nagasaki, Y.; Nakanishi, H.; et al. Herpes zoster in lung cancer patients treated with PD-1/PD-L1 inhibitors. Transl. Cancer Res. 2022, 11, 456–462. [Google Scholar] [CrossRef] [PubMed]
- Del Castillo, M.; Romero, F.A.; Argüello, E.; Kyi, C.; Postow, M.A.; Redelman-Sidi, G. The spectrum of serious infections among patients receiving immune checkpoint blockade for the treatment of melanoma. Clin. Infect. Dis. 2016, 63, 1490–1493. [Google Scholar] [CrossRef] [PubMed]
- Fujita, K.; Terashima, T.; Mio, T. Anti-PD1 Antibody Treatment and the Development of Acute Pulmonary Tuberculosis. J. Thorac. Oncol. 2016, 11, 2238–2240. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.R.; Keam, B.; Park, Y.S.; Kim, M.; Kim, T.M.; Kim, D.-W.; Heo, D.S. Pneumocystis Pneumonia Developing during Treatment of Recurrent Renal Cell Cancer with Nivolumab. Korean J. Med. 2018, 93, 571–574. [Google Scholar] [CrossRef]
- Topalian, S.L.; Hodi, F.S.; Brahmer, J.R.; Gettinger, S.N.; Smith, D.C.; McDermott, D.F.; Powderly, J.D.; Carvajal, R.D.; Sosman, J.A.; Atkins, M.B.; et al. Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N. Engl. J. Med. 2012, 366, 2443–2454. [Google Scholar] [CrossRef] [PubMed]
- Brahmer, J.R.; Tykodi, S.S.; Chow, L.Q.; Hwu, W.J.; Topalian, S.L.; Hwu, P.; Drake, C.G.; Camacho, L.H.; Kauh, J.; Odunsi, K.; et al. Safety and activity of anti-PD-L1 antibody in patients with advanced cancer. N. Engl. J. Med. 2012, 366, 2455–2465. [Google Scholar] [CrossRef] [PubMed]
- Eigentler, T.K.; Hassel, J.C.; Berking, C.; Aberle, J.; Bachmann, O.; Grunwald, V.; Kahler, K.C.; Loquai, C.; Reinmuth, N.; Steins, M.; et al. Diagnosis, monitoring and management of immune-related adverse drug reactions of anti-PD-1 antibody therapy. Cancer Treat. Rev. 2016, 45, 7–18. [Google Scholar] [CrossRef] [PubMed]
- Fehrenbacher, L.; Spira, A.; Ballinger, M.; Kowanetz, M.; Vansteenkiste, J.; Mazieres, J.; Park, K.; Smith, D.; Artal-Cortes, A.; Lewanski, C.; et al. Atezolizumab versus docetaxel for patients with previously treated non-small-cell lung cancer (POPLAR): A multicentre, open-label, phase 2 randomised controlled trial. Lancet 2016, 387, 1837–1846. [Google Scholar] [CrossRef] [PubMed]
- Petrelli, F.; Morelli, A.M.; Luciani, A.; Ghidini, A.; Solinas, C. Risk of Infection with Immune Checkpoint Inhibitors: A Systematic Review and Meta-analysis. Target Oncol. 2021, 16, 553–568. [Google Scholar] [CrossRef] [PubMed]
- Shah, N.J.; Al-Shbool, G.; Blackburn, M.; Cook, M.; Belouali, A.; Liu, S.V.; Madhavan, S.; He, A.R.; Atkins, M.B.; Gibney, G.T.; et al. Safety and efficacy of immune checkpoint inhibitors (ICIs) in cancer patients with HIV, hepatitis B, or hepatitis C viral infection. J. Immunother. Cancer 2019, 7, 353. [Google Scholar] [CrossRef] [PubMed]
- Weinberg, A.; Levin, M.J. VZV T cell-mediated immunity. Curr. Top Microbiol. Immunol. 2010, 342, 341–357. [Google Scholar] [CrossRef] [PubMed]
- Laing, K.J.; Ouwendijk, W.J.D.; Koelle, D.M.; Verjans, G. Immunobiology of Varicella-Zoster Virus Infection. J. Infect. Dis. 2018, 218, S68–S74. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.Y.; Kim, M.; Keam, B.; Kim, T.M.; Kim, D.-W.; Heo, D.S.; Jo, S.J. The risk of herpes zoster in patients with non-small cell lung cancer according to chemotherapy regimens: Tyrosine kinase inhibitors versus cytotoxic chemotherapy. Cancer Res. Treat. 2019, 51, 169–177. [Google Scholar] [CrossRef] [PubMed]
- Abendroth, A.; Lin, I.; Slobedman, B.; Ploegh, H.; Arvin, A.M. Varicella-zoster virus retains major histocompatibility complex class I proteins in the Golgi compartment of infected cells. J. Virol. 2001, 75, 4878–4888. [Google Scholar] [CrossRef] [PubMed]
- Zangeneh, Z.; Golmoghaddam, H.; Emad, M.; Erfani, N.; Doroudchi, M. Elevated PD-1 expression and decreased telomerase activity in memory T cells of patients with symptomatic Herpes Zoster infection. Cell. Mol. Biol. 2014, 60, 13–21. [Google Scholar] [PubMed]
- Jones, D.; Como, C.N.; Jing, L.; Blackmon, A.; Neff, C.P.; Krueger, O.; Bubak, A.N.; Palmer, B.E.; Koelle, D.M.; Nagel, M.A. Varicella zoster virus productively infects human peripheral blood mononuclear cells to modulate expression of immunoinhibitory proteins and blocking PD-L1 enhances virus-specific CD8+ T cell effector function. PLoS Pathog. 2019, 15, e1007650. [Google Scholar] [CrossRef] [PubMed]
- Channappanavar, R.; Twardy, B.S.; Suvas, S. Blocking of PDL-1 interaction enhances primary and secondary CD8 T cell response to herpes simplex virus-1 infection. PLoS ONE 2012, 7, e39757. [Google Scholar] [CrossRef] [PubMed]
- Hamashima, R.; Uchino, J.; Morimoto, Y.; Iwasaku, M.; Kaneko, Y.; Yamada, T.; Takayama, K. Association of immune checkpoint inhibitors with respiratory infections: A review. Cancer Treat. Rev. 2020, 90, 102109. [Google Scholar] [CrossRef] [PubMed]
- Delanoy, N.; Michot, J.M.; Comont, T.; Kramkimel, N.; Lazarovici, J.; Dupont, R.; Champiat, S.; Chahine, C.; Robert, C.; Herbaux, C.; et al. Haematological immune-related adverse events induced by anti-PD-1 or anti-PD-L1 immunotherapy: A descriptive observational study. Lancet Haematol. 2019, 6, e48–e57. [Google Scholar] [CrossRef] [PubMed]
- Anastasopoulou, A.; Ziogas, D.C.; Samarkos, M.; Kirkwood, J.M.; Gogas, H. Reactivation of tuberculosis in cancer patients following administration of immune checkpoint inhibitors: Current evidence and clinical practice recommendations. J. Immunother. Cancer 2019, 7, 239. [Google Scholar] [CrossRef] [PubMed]
- Lasagna, A.; Arlunno, B.; Imarisio, I. A case report of pulmonary nocardiosis during pembrolizumab: The emerging challenge of the infections on immunotherapy. Immunotherapy 2022, 14, 1369–1375. [Google Scholar] [CrossRef] [PubMed]
- Lazar-Molnar, E.; Chen, B.; Sweeney, K.A.; Wang, E.J.; Liu, W.; Lin, J.; Porcelli, S.A.; Almo, S.C.; Nathenson, S.G.; Jacobs, W.R., Jr. Programmed death-1 (PD-1)-deficient mice are extraordinarily sensitive to tuberculosis. Proc. Natl. Acad. Sci. USA 2010, 107, 13402–13407. [Google Scholar] [CrossRef] [PubMed]
- Tousif, S.; Singh, Y.; Prasad, D.V.; Sharma, P.; Van Kaer, L.; Das, G. T cells from Programmed Death-1 deficient mice respond poorly to Mycobacterium tuberculosis infection. PLoS ONE 2011, 6, e19864. [Google Scholar] [CrossRef] [PubMed]
- Sakai, S.; Kauffman, K.D.; Sallin, M.A.; Sharpe, A.H.; Young, H.A.; Ganusov, V.V.; Barber, D.L. CD4 T Cell-Derived IFN-gamma Plays a Minimal Role in Control of Pulmonary Mycobacterium tuberculosis Infection and Must Be Actively Repressed by PD-1 to Prevent Lethal Disease. PLoS Pathog. 2016, 12, e1005667. [Google Scholar] [CrossRef] [PubMed]
- Price, P.; Murdoch, D.M.; Agarwal, U.; Lewin, S.R.; Elliott, J.H.; French, M.A. Immune restoration diseases reflect diverse immunopathological mechanisms. Clin. Microbiol. Rev. 2009, 22, 651–663. [Google Scholar] [CrossRef]
- Liu, Z.; Liu, T.; Zhang, X.; Si, X.; Wang, H.; Zhang, J.; Huang, H.; Sun, X.; Wang, J.; Wang, M.; et al. Opportunistic infections complicating immunotherapy for non-small cell lung cancer. Thorac. Cancer 2020, 11, 1689–1694. [Google Scholar] [CrossRef] [PubMed]
- Thompson, J.A.; Schneider, B.J.; Brahmer, J.; Andrews, S.; Armand, P.; Bhatia, S.; Budde, L.E.; Costa, L.; Davies, M.; Dunnington, D.; et al. Management of Immunotherapy-Related Toxicities, Version 1.2019. J. Natl. Compr. Cancer Netw. 2019, 17, 255–289. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| ICIs | Non-ICIs (n = 50,124) | p-Value | |||||
|---|---|---|---|---|---|---|---|
| Atezolizumab (n = 126) | Durvalumab (n = 2) | Nivolumab (n = 309) | Pembrolizumab (n = 460) | Total (n = 897) | |||
| Age (year), n (%) | 0.008 | ||||||
| <40 (%) | 1 (0.8) | 0 (0) | 1 (0.3) | 4 (0.9) | 6 (0.7) | 475 (0.9) | |
| 40–50 (%) | 10 (7.9) | 0 (0) | 18 (5.8) | 16 (3.5) | 44 (4.9) | 2019 (4.0) | |
| 50–60 (%) | 22 (17.5) | 0 (0) | 55 (17.8) | 79 (17.2) | 156 (17.4) | 8040 (16.0) | |
| 60–70 (%) | 42 (33.3) | 2 (100) | 116 (37.5) | 143 (31.1) | 303 (33.8) | 18,395 (36.7) | |
| 70–80 (%) | 43 (34.1) | 0 (0) | 96 (31.1) | 159 (34.6) | 298 (33.2) | 17,555 (35.0) | |
| ≥80 (%) | 8 (6.3) | 0 (0) | 23 (7.4) | 59 (12.8) | 90 (10.0) | 3640 (7.3) | |
| Sex, n (%) | 0.3112 | ||||||
| Male | 89 (70.6) | 2 (100) | 253 (81.9) | 334 (72.6) | 678 (75.6) | 37,109 (74.0) | |
| Female | 37 (29.4) | 0 (0) | 56 (18.1) | 126 (27.4) | 219 (24.4) | 13,015 (26.0) | |
| Comorbidity, n (%) | |||||||
| Diabetes | 51 (40.5) | 0 (0) | 106 (34.3) | 193 (42.0) | 350 (39.0) | 21,708 (43.3) | 0.011 |
| Cardiovascular disease * | 51 (40.5) | 0 (0) | 81 (26.2) | 169 (36.7) | 301 (33.6) | 20,791 (41.5) | <0.001 |
| Chronic lung diseases | 94 (74.6) | 1 (50) | 199 (64.4) | 307 (66.7) | 601 (67.0) | 36,234 (72.3) | 0.001 |
| Chronic kidney diseases | 12 (9.5) | 0 (0) | 18 (5.8) | 29 (6.3) | 59 (6.6) | 2751 (5.5) | 0.179 |
| Chronic liver diseases | 6 (4.8) | 0 (0) | 10 (3.2) | 9 (2.0) | 25 (2.8) | 1404 (2.8) | 1.000 |
| Rheumatic diseases | 9 (7.1) | 0 (0) | 7 (2.3) | 32 (7.0) | 48 (5.4) | 3221(6.4) | 0.217 |
| Concomitant use of immunosuppressive drugs, n (%) | |||||||
| Immunosuppressant | 10 (7.9) | 0 (0) | 6 (1.9) | 15 (3.3) | 31 (3.5) | 2428 (4.8) | 0.065 |
| Steroid ** | 4 (3.2) | 0 (0) | 12 (3.9) | 18 (3.9) | 34 (3.8) | 3386 (6.8) | 0.001 |
| ICIs | Non-ICIs | |||||
|---|---|---|---|---|---|---|
| Event (n) | Person-Years | Incidence * (95% CI) | Event (n) | Person-Years | Incidence * (95% CI) | |
| Total | 29 | 2395.45 | 1210.63 (844.97–1689.36) | 2233 | 119,537.78 | 1868.03 (1791.34–1945.44) |
| Age, n (%) | ||||||
| <40 | 0 | 13.92 | 0 (0–0) | 19 | 1166.73 | 1628.48 (1047.07–2438.24) |
| 40–49 | 0 | 131.22 | 0 (0–0) | 74 | 5042.06 | 1467.65 (1170.00–1820.42) |
| 50–59 | 4 | 446.80 | 895.25 (363.36–1962.22) | 410 | 20,084.68 | 2041.36 (1853.26–2243.62) |
| 60–69 | 11 | 849.69 | 1294.60 (729.75–2164.36) | 921 | 43,870.17 | 2099.38 (1968.17–2237.11) |
| 70–79 | 12 | 784.60 | 1529.44 (882.22–2508.54) | 716 | 41,251.46 | 1735.70 (1610.87–1862.60) |
| ≥80 | 2 | 169.22 | 1181.90 (365.61–3292.58) | 93 | 8122.67 | 1144.94 (935.18–1389.07) |
| Sex, n (%) | ||||||
| Male | 23 | 1810.25 | 1270.54 (849.45–1839.98) | 1471 | 89,520.82 | 1643.19 (1561.37–1728.22) |
| Female | 6 | 585.20 | 1025.29 (480.92–1993.90) | 762 | 30,016.96 | 2538.56 (2364.71–2721.94) |
| ICIs | Non-ICIs | |||||||
|---|---|---|---|---|---|---|---|---|
| Observed Event (n) | Expected Event (n) | SIR (95% CI) | p-Value | Observed Event (n) | Expected Event (n) | SIR (95% CI) | p-Value | |
| Male | ||||||||
| <40 | 0 | 0.01 | 0 (0–0) | 1.00 | 11 | 0.36 | 30.22 (16.74–54.57) | <0.01 |
| 40–49 | 0 | 0.10 | 0 (0–0) | 1.00 | 37 | 3.16 | 11.69 (8.47–16.13) | <0.01 |
| 50–59 | 2 | 0.47 | 4.26 (1.07–17.05) | 0.04 | 224 | 21.01 | 10.66 (9.35–12.15) | <0.01 |
| 60–69 | 18 | 1.49 | 5.37 (2.69–10.75) | <0.01 | 609 | 78.64 | 7.74 (7.15–8.38) | <0.01 |
| 70–79 | 11 | 1.91 | 5.75 (3.19–10.39) | <0.01 | 521 | 98.19 | 5.32 (4.88–5.79) | <0.01 |
| ≥80 | 2 | 1.98 | 1.01 (0.25–4.04) | 0.99 | 68 | 88.02 | 0.77 (0.61–0.98) | 0.03 |
| Female | ||||||||
| <40 | 0 | 0 | 0 (0–0) | 1.00 | 8 | 0.41 | 19.45 (9.73–38.90) | <0.01 |
| 40–49 | 0 | 0.08 | 0 (0–0) | 1.00 | 37 | 4.12 | 8.99 (6.51–12.40) | <0.01 |
| 50–59 | 2 | 0.43 | 4.68 (1.17–18.72) | 0.03 | 186 | 19.34 | 9.62 (8.33–11.10) | <0.01 |
| 60–69 | 3 | 0.75 | 3.99 (1.29–12.37) | 0.02 | 312 | 36.09 | 8.65 (7.74–9.66) | <0.01 |
| 70–79 | 1 | 0.51 | 1.96 (0.28–13.9) | 0.50 | 194 | 29.60 | 6.55 (5.69–7.54) | <0.01 |
| ≥80 | 0 | 0.43 | 0 (0–0) | 1.00 | 25 | 27.43 | 0.91 (0.62–1.35) | 0.64 |
| Unadjusted | Adjusted | |||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Total | 0.70 (0.48–1.01) | 0.05 | 0.69 (0.48–1.00) | 0.05 |
| Sex | ||||
| Male | 0.84 (0.55–1.26) | 0.39 | 0.84 (0.55–1.26) | 0.40 |
| Female | 0.43 (0.19–0.96) | 0.04 | 0.42 (0.19–0.94) | 0.04 |
| Age | ||||
| <68 years | 0.59 (0.35–0.99) | 0.05 | 0.58 (0.34–0.99) | 0.05 |
| ≥68 years | 0.84 (0.51–1.40) | 0.51 | 0.84 (0.50–1.40) | 0.50 |
| Diabetes | ||||
| No | 0.81 (0.53–1.23) | 0.32 | 0.84 (0.55–1.28) | 0.41 |
| Yes | 0.49 (0.23–1.03) | 0.06 | 0.48 (0.23–1.01) | 0.05 |
| Cardiovascular disease | ||||
| No | 0.65 (0.42–1.01) | 0.06 | 0.65 (0.41–1.01) | 0.05 |
| Yes | 0.80 (0.42–1.55) | 0.52 | 0.85 (0.44–1.64) | 0.63 |
| Chronic lung diseases | ||||
| No | 0.59 (0.32–1.11) | 0.10 | 0.58 (0.31–1.09) | 0.09 |
| Yes | 0.76 (0.48–1.19) | 0.23 | 0.76 (0.48–1.20) | 0.24 |
| Chronic kidney diseases | ||||
| No | 0.71 (0.49–1.03) | 0.07 | 0.70 (0.48–1.02) | 0.07 |
| Yes | 0.52 (0.07–3.74) | 0.52 | 0.52 (0.07–3.89) | 0.53 |
| Chronic liver diseases | ||||
| No | 0.68 (0.47–0.99) | 0.05 | 0.68 (0.47–0.99) | 0.05 |
| Yes | 1.57 (0.22–11.41) | 0.65 | 1.18 (0.13–10.91) | 0.88 |
| Rheumatic diseases | ||||
| No | 0.66 (0.45–0.97) | 0.03 | 0.65 (0.44–0.97) | 0.03 |
| Yes | 1.52 (0.48–4.78) | 0.47 | 1.76 (0.52–5.93) | 0.36 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, J.; Park, S.-Y.; Park, J.-Y.; Kim, D.; Lee, K.; Choi, S. Reactivation of Varicella-Zoster Virus in Patients with Lung Cancer Receiving Immune Checkpoint Inhibitors: Retrospective Nationwide Population-Based Cohort Study from South Korea. Cancers 2024, 16, 1499. https://doi.org/10.3390/cancers16081499
Jung J, Park S-Y, Park J-Y, Kim D, Lee K, Choi S. Reactivation of Varicella-Zoster Virus in Patients with Lung Cancer Receiving Immune Checkpoint Inhibitors: Retrospective Nationwide Population-Based Cohort Study from South Korea. Cancers. 2024; 16(8):1499. https://doi.org/10.3390/cancers16081499
Chicago/Turabian StyleJung, Jiyun, Seong-Yeon Park, Jae-Yoon Park, Dalyong Kim, Kyoungmin Lee, and Sungim Choi. 2024. "Reactivation of Varicella-Zoster Virus in Patients with Lung Cancer Receiving Immune Checkpoint Inhibitors: Retrospective Nationwide Population-Based Cohort Study from South Korea" Cancers 16, no. 8: 1499. https://doi.org/10.3390/cancers16081499
APA StyleJung, J., Park, S.-Y., Park, J.-Y., Kim, D., Lee, K., & Choi, S. (2024). Reactivation of Varicella-Zoster Virus in Patients with Lung Cancer Receiving Immune Checkpoint Inhibitors: Retrospective Nationwide Population-Based Cohort Study from South Korea. Cancers, 16(8), 1499. https://doi.org/10.3390/cancers16081499