
Assessment of PSMA Expression of Healthy Organs in Different Stages of Prostate Cancer Using [68Ga]Ga-PSMA-11-PET Examinations

 , , , and
, , , and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Patients
2.2. PET-MRI Examination
2.3. PET-CT Examination
2.4. Image Analysis
2.5. Protocol of PSMA-RLT
2.6. Statistical Analysis
3. Results
3.1. PSMA Uptake in Different Cohorts
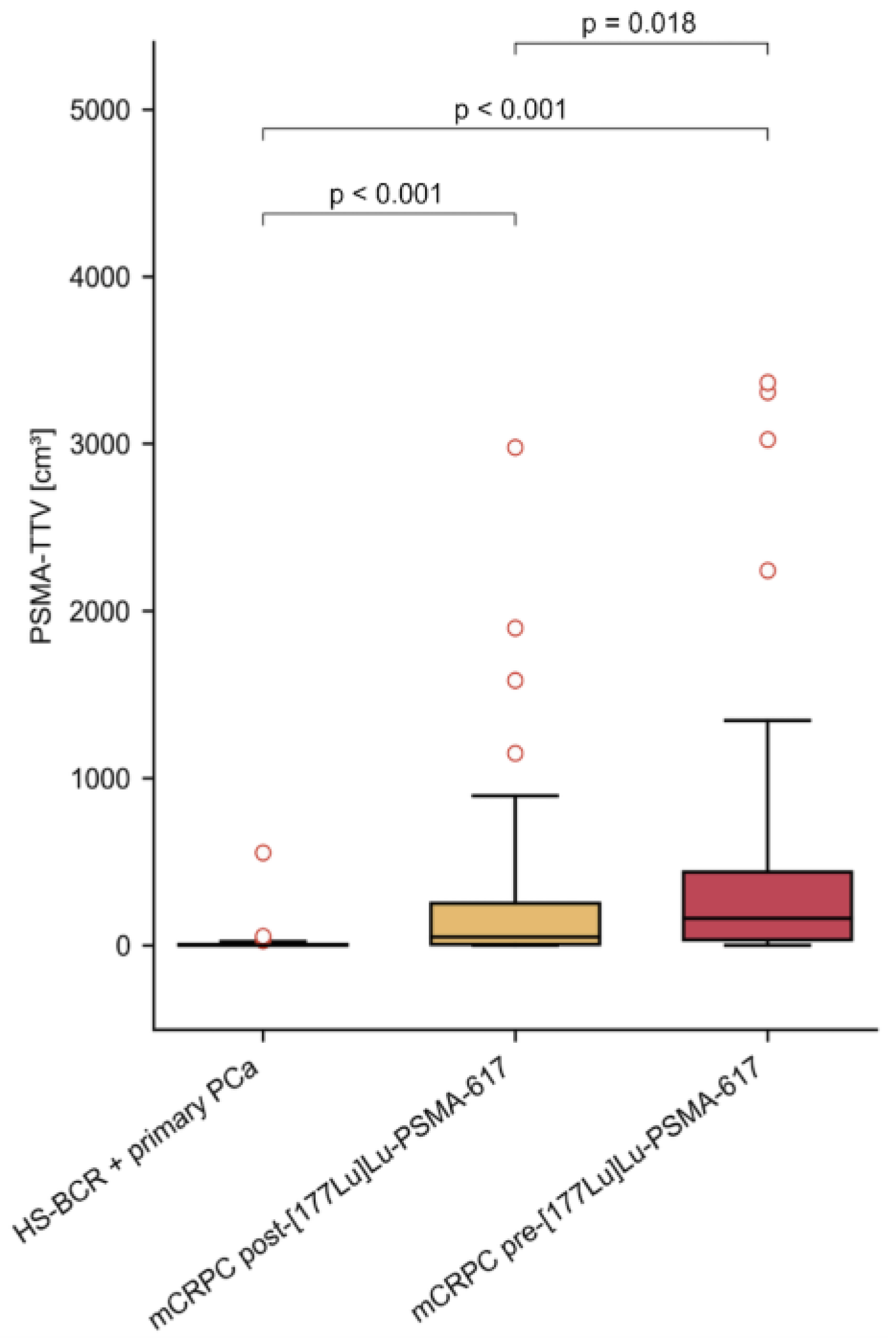
3.2. PSMA-TTV in Different Cohorts
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rawla, P. Epidemiology of Prostate Cancer. World J. Oncol. 2019, 10, 63–89. [Google Scholar] [CrossRef] [PubMed]
- Wasim, S.; Park, J.; Nam, S.; Kim, J. Review of Current Treatment Intensification Strategies for Prostate Cancer Patients. Cancers 2023, 15, 5615. [Google Scholar] [CrossRef]
- Chang, S.S. Overview of Prostate-Specific Membrane Antigen. Rev. Urol. 2004, 6 (Suppl. S10), S13–S18. [Google Scholar] [PubMed]
- Freedland, S.J.; Humphreys, E.B.; Mangold, L.A.; Eisenberger, M.; Dorey, F.J.; Walsh, P.C.; Partin, A.W. Risk of prostate cancer-specific mortality following biochemical recurrence after radical prostatectomy. JAMA 2005, 294, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Kupelian, P.A.; Buchsbaum, J.C.; Elshaikh, M.; Reddy, C.A.; Zippe, C.; Klein, E.A. Factors affecting recurrence rates after prostatectomy or radiotherapy in localized prostate carcinoma patients with biopsy Gleason score 8 or above. Cancer 2002, 95, 2302–2307. [Google Scholar] [CrossRef] [PubMed]
- Shore, N.D.; Moul, J.W.; Pienta, K.J.; Czernin, J.; King, M.T.; Freedland, S.J. Biochemical recurrence in patients with prostate cancer after primary definitive therapy: Treatment based on risk stratification. Prostate Cancer Prostatic Dis. 2023, 1–10. [Google Scholar] [CrossRef]
- Chandrasekar, T.; Yang, J.C.; Gao, A.C.; Evans, C.P. Mechanisms of resistance in castration-resistant prostate cancer (CRPC). Transl. Androl. Urol. 2015, 4, 365–380. [Google Scholar] [CrossRef] [PubMed]
- Kirby, M.; Hirst, C.; Crawford, E.D. Characterising the castration-resistant prostate cancer population: A systematic review. Int. J. Clin. Pract. 2011, 65, 1180–1192. [Google Scholar] [CrossRef]
- Silver, D.A.; Pellicer, I.; Fair, W.R.; Heston, W.D.; Cordon-Cardo, C. Prostate-specific membrane antigen expression in normal and malignant human tissues. Clin. Cancer Res. 1997, 3, 81–85. [Google Scholar]
- Hofman, M.S.; Lawrentschuk, N.; Francis, R.J.; Tang, C.; Vela, I.; Thomas, P.; Rutherford, N.; Martin, J.M.; Frydenberg, M.; Shakher, R.; et al. Prostate-specific membrane antigen PET-CT in patients with high-risk prostate cancer before curative-intent surgery or radiotherapy (proPSMA): A prospective, randomised, multicentre study. Lancet 2020, 395, 1208–1216. [Google Scholar] [CrossRef]
- Afshar-Oromieh, A.; Holland-Letz, T.; Giesel, F.L.; Kratochwil, C.; Mier, W.; Haufe, S.; Debus, N.; Eder, M.; Eisenhut, M.; Schäfer, M.; et al. Diagnostic performance of 68Ga-PSMA-11 (HBED-CC) PET/CT in patients with recurrent prostate cancer: Evaluation in 1007 patients. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 1258–1268. [Google Scholar] [CrossRef]
- Sartor, O.; de Bono, J.; Chi, K.N.; Fizazi, K.; Herrmann, K.; Rahbar, K.; Tagawa, S.T.; Nordquist, L.T.; Vaishampayan, N.; El-Haddad, G.; et al. Lutetium-177–PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2021, 385, 1091–1103. [Google Scholar] [CrossRef]
- Rasul, S.; Hacker, M.; Kretschmer-Chott, E.; Leisser, A.; Grubmüller, B.; Kramer, G.; Shariat, S.; Wadsak, W.; Mitterhauser, M.; Hartenbach, M.; et al. Clinical outcome of standardized 177Lu-PSMA-617 therapy in metastatic prostate cancer patients receiving 7400 MBq every 4 weeks. Eur. J. Nucl. Med. 2020, 47, 713–720. [Google Scholar] [CrossRef]
- Hofman, M.S.; Emmett, L.; Sandhu, S.; Iravani, A.; Joshua, A.M.; Goh, J.C.; Pattison, D.A.; Tan, T.H.; Kirkwood, I.D.; Ng, S.; et al. [177Lu]Lu-PSMA-617 versus cabazitaxel in patients with metastatic castration-resistant prostate cancer (TheraP): A randomised, open-label, phase 2 trial. Lancet 2021, 397, 797–804. [Google Scholar] [CrossRef] [PubMed]
- Ferdinandus, J.; Fendler, W.P.; Farolfi, A.; Washington, S.; Mohammad, O.; Pampaloni, M.H.; Scott, P.J.; Rodnick, M.; Viglianti, B.L.; Eiber, M.; et al. PSMA PET Validates Higher Rates of Metastatic Disease for European Association of Urology Biochemical Recurrence Risk Groups: An International Multicenter Study. J. Nucl. Med. 2022, 63, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Grubmüller, B.; Senn, D.; Kramer, G.; Baltzer, P.; D’Andrea, D.; Grubmüller, K.H.; Mitterhauser, M.; Eidherr, H.; Haug, A.R.; Wadsak, W.; et al. Response assessment using 68Ga-PSMA ligand PET in patients undergoing 177Lu-PSMA radioligand therapy for metastatic castration-resistant prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 1063–1072. [Google Scholar] [CrossRef]
- Grubmüller, B.; Huebner, N.A.; Rasul, S.; Clauser, P.; Pötsch, N.; Grubmüller, K.H.; Hacker, M.; Hartenbach, S.; Shariat, S.F.; Hartenbach, M.; et al. Dual-Tracer PET-MRI-Derived Imaging Biomarkers for Prediction of Clinically Significant Prostate Cancer. Curr. Oncol. 2023, 30, 1683–1691. [Google Scholar] [CrossRef]
- Privé, B.M.; Janssen, M.J.R.; van Oort, I.M.; Muselaers, C.H.J.; Jonker, M.A.; van Gemert, W.A.; de Groot, M.; Westdorp, H.; Mehra, N.; Verzijlbergen, J.F.; et al. Update to a randomized controlled trial of lutetium-177-PSMA in Oligo-metastatic hormone-sensitive prostate cancer: The BULLSEYE trial. Trials 2021, 22, 768. [Google Scholar] [CrossRef] [PubMed]
- Dhiantravan, N.; Emmett, L.; Joshua, A.M.; Pattison, D.A.; Francis, R.J.; Williams, S.; Sandhu, S.; Davis, I.D.; Vela, I.; Neha, N.; et al. UpFrontPSMA: A randomized phase 2 study of sequential 177 Lu-PSMA-617 and docetaxel vs docetaxel in metastatic hormone-naïve prostate cancer (clinical trial protocol). BJU Int. 2021, 128, 331–342. [Google Scholar] [CrossRef]
- Kostos, L.K.; Buteau, J.P.; Kong, G.; Yeung, T.; Di Iulio, J.; Fahey, M.T.; Fettke, H.; Furic, L.; Hofman, M.S.; Azad, A. LuCAB: A phase I/II trial evaluating cabazitaxel in combination with [177Lu]Lu-PSMA-617 in patients (pts) with metastatic castration-resistant prostate cancer (mCRPC). J. Clin. Oncol. 2023, 41, TPS278. [Google Scholar] [CrossRef]
- Sandhu, S.; Joshua, A.M.; Emmett, L.; Crumbaker, M.; Bressel, M.; Huynh, R.; Banks, P.D.; Wallace, R.; Hamid, A.; Inderjeeth, A.J.; et al. LuPARP: Phase 1 trial of 177Lu-PSMA-617 and olaparib in patients with metastatic castration resistant prostate cancer (mCRPC). J. Clin. Oncol. 2023, 41, 5005. [Google Scholar] [CrossRef]
- Eapen, R.S.; Buteau, J.P.; Jackson, P.; Mitchell, C.; Oon, S.F.; Alghazo, O.; McIntosh, L.; Dhiantravan, N.; Scalzo, M.J.; O’Brien, J.; et al. Administering [177Lu]Lu-PSMA-617 Prior to Radical Prostatectomy in Men with High-risk Localised Prostate Cancer (LuTectomy): A Single-centre, Single-arm, Phase 1/2 Study. Eur. Urol. 2023, 85, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Seitzer, K.E.; Seifert, R.; Kessel, K.; Roll, W.; Schlack, K.; Boegemann, M.; Rahbar, K. Lutetium-177 Labelled PSMA Targeted Therapy in Advanced Prostate Cancer: Current Status and Future Perspectives. Cancers 2021, 13, 3715. [Google Scholar] [CrossRef] [PubMed]
- Peters, S.M.B.; Hofferber, R.; Privé, B.M.; de Bakker, M.; Gotthardt, M.; Janssen, M.; de Lange, F.; Muselaers, C.H.J.; Mehra, N.; Witjes, J.A.; et al. [68Ga]Ga-PSMA-11 PET imaging as a predictor for absorbed doses in organs at risk and small lesions in [177Lu]Lu-PSMA-617 treatment. Eur. J. Nucl. Med. 2022, 49, 1101–1112. [Google Scholar] [CrossRef] [PubMed]
- Kluge, K.; Haberl, D.; Einspieler, H.; Rasul, S.; Gutschmayer, S.; Kenner, L.; Kramer, G.; Grubmüller, B.; Shariat, S.; Haug, A.; et al. Antihormonal-Treatment Status Affects68Ga-PSMA-HBED-CC PET Biodistribution in Patients with Prostate Cancer. J. Nucl. Med. 2023, 64, 1730–1736. [Google Scholar] [CrossRef]
- Gafita, A.; Wang, H.; Robertson, A.; Armstrong, W.R.; Zaum, R.; Weber, M.; Yagubbayli, F.; Kratochwil, C.; Grogan, T.R.; Nguyen, K.; et al. Tumor Sink Effect in 68Ga-PSMA-11 PET: Myth or Reality? J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2022, 63, 226–232. [Google Scholar] [CrossRef]
- Tuncel, M.; Telli, T.; Tuncalı, M.; Karabulut, E. Predictive factors of tumor sink effect: Insights from 177Lu-Prostate-specific membrane antigen therapy. Ann. Nucl. Med. 2021, 35, 529–539. [Google Scholar] [CrossRef]
- Groener, D.; Wichert, J.; Adams, M.; Mader, N.; Klimek, K.; Ngoc, C.N.; Baumgarten, J.; Happel, C.; Mandel, P.; Chun, F.K.H.; et al. Impact of [177Lu]Lu-PSMA-617 Radioligand Therapy on Reference Organ Uptake Assessed by [68Ga]Ga-PSMA-11-PET/CT. Cancers 2023, 15, 3878. [Google Scholar] [CrossRef]
- Lyons, K.; Seghers, V.; Sorensen, J.I.L.; Zhang, W.; Paldino, M.J.; Krishnamurthy, R.; Rohren, E.M. Comparison of Standardized Uptake Values in Normal Structures Between PET/CT and PET/MRI in a Tertiary Pediatric Hospital: A Prospective Study. Am. J. Roentgenol. 2015, 205, 1094–1101. [Google Scholar] [CrossRef]
- Huber, R.; Sher, A.; Crisan, A.; Faulhaber, P. Comparisons of SUVs in normal structures between PET/CT and PET/MRI. J. Nucl. Med. 2014, 55 (Suppl. 1), 1506. [Google Scholar]
- Jentjens, S.; Mai, C.; Bidakhvidi, N.A.; De Coster, L.; Mertens, N.; Koole, M.; Everaerts, W.; Joniau, S.; Oyen, R.; Van Laere, K.; et al. Prospective comparison of simultaneous [68Ga]Ga-PSMA-11 PET/MR versus PET/CT in patients with biochemically recurrent prostate cancer. Eur. Radiol. 2022, 32, 901–911. [Google Scholar] [CrossRef] [PubMed]
- Freitag, M.T.; Radtke, J.P.; Afshar-Oromieh, A.; Roethke, M.C.; Hadaschik, B.; Gleave, M.; Bonekamp, D.; Kopka, K.; Eder, M.; Heusser, T.; et al. Local recurrence of prostate cancer after radical prostatectomy is at risk to be missed in 68Ga-PSMA-11-PET of PET/CT and PET/MRI: Comparison with mpMRI integrated in simultaneous PET/MRI. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 776–787. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Parameters | Primary PCa + HS-BCR (N: 102) | mCRPC before PSMA-RLT (N: 50) | mCRPC after PSMA-RLT (N: 50) |
|---|---|---|---|
| Median Age in years (range) | 71.5 (50; 87) | 71.5 (51; 84) | 72.0 (52; 84) |
| Previous therapies: Hormone therapy (N): | 1 | 37 | 37 |
| ADT (N) | 1 | 28 | 28 |
| Abiraterone/Enzalutamide (N) | 0 | 32 | 32 |
| Chemotherapy (N): | 0 | 33 | 33 |
| Docetaxel (N) | 0 | 30 | 30 |
| Docetaxel + Cabazitaxel (N) | 0 | 19 | 19 |
| Xofigo® (Ra-223) (N) | 0 | 15 | 15 |
| Patients with metastatic lesions (N): | 39 | 50 | 50 |
| Lymph node (N) | 33 | 38 | 37 |
| Bone (N) | 11 | 40 | 40 |
| Visceral (N) | 0 | 9 | 9 |
| PET-CT (N) | 31 | 10 | 3 |
| PET-MRI (N) | 71 | 40 | 47 |
| Organ | PSMA-PET Scans | |||||
|---|---|---|---|---|---|---|
| Primary PCa + HS-BCR (N: 102) | mCRPC before PSMA-RLT (N: 50) | mCRPC after PSMA-RLT (N: 50) | ||||
| SUVmean # | SUVmax # | SUVmean # | SUVmax # | SUVmean # | SUVmax # | |
| Submandibular gland | 17.53 * (1.94; 110.73) | 24.33 * (2.49; 160.40) | 12.07 * (3.88; 64.58) | 17.93 * (5.14; 115.97) | 10.25 (1.86; 31.15) | 14.00 (2.89; 45.24) |
| Thyroid | 1.70 * (0.18; 15.20) | 2.70 * (0.23; 20.63) | 1.15 * (0.43; 6.00) | 1.92 * (0.67; 12.61) | 1.18 (0.34; 3.06) | 1.84 (0.49; 6.08) |
| Heart | 1.10 * (0.36; 5.36) | 2.22 * (0.81; 13.12) | 0.81 * (0.27; 3.55) | 1.57 * (0.51; 13.17) | 0.84 (0.33; 2.81) | 1.42 (0.58; 6.06) |
| Lung | 0.47 (0.15; 2.53) | 1.06 (0.35; 8.00) | 0.38 (0.18; 3.42) | 0.94 (0.41; 7.81) | 0.38 (0.13; 4.83) | 0.77 (0.22; 11.00) |
| Liver | 5.74 * (1.77; 19.82) | 8.09 * (2.63; 75.85) | 3.59 * (1.19; 21.94) | 5.43 * (1.97; 40.11) | 3.00 (0.74; 9.14) | 4.39 (1.48; 12.25) |
| Spleen | 5.74 (1.25; 33.08) | 10.05 (2.62; 164.56) | 4.79 (1.11; 30.67) | 7.37 (1.96; 73.17) | 5.02 (1.06; 19.23) | 7.70 (1.61; 41.78) |
| Kidney | 38.09 * (2.03; 212.73) | 55.38 * (2.91; 268.14) | 18.99 * (3.75; 161.89) | 29.50 * (4.84; 283.31) | 19.38 (5.84; 69.07) | 32.08 (8.88; 128.87) |
| Pancreas | 2.44 * (0.66; 12.08) | 4.00 * (1.03; 22.50) | 1.71 * (0.54; 4.70) | 2.48 * (0.68; 9.59) | 1.56 (0.58; 3.78) | 2.36 (0.82; 7.40) |
| Small intestine (duodenum) | 2.63 * (0.10; 18.91) | 4.30 * (0.47; 30.59) | 1.84 * (0.27; 5.95) | 3.38 * (0.84; 10.18) | 1.50 (0.25; 10.14) | 2.60 (0.64; 15.76) |
| Testes | 1.58 * (0.39; 10.20) | 2.65 * (0.84; 19.75) | 0.80 * (0.16; 6.50) | 1.40 * (0.37; 14.11) | 0.70 (0.24; 14.89) | 1.23 (0.46; 23.89) |
| Bone marrow | 0.23 * (0.02; 1.29) | 1.08 * (0.18; 7.52) | 0.16 * (0.05; 0.99) | 0.66 * (0.18; 6.65) | 0.18 (0.05; 0.64) | 0.65 (0.15; 3.15) |
| Muscle (gluteus maximus) | 0.45 (0.16; 1.95) | 1.04 (0.36; 4.97) | 0.45 (0.18; 1.33) | 0,97 (0.34; 5.39) | 0.40 (0.16; 1.11) | 0.81 (0.29; 2.40) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Einspieler, H.; Kluge, K.; Haberl, D.; Schatz, K.; Nics, L.; Schmitl, S.; Geist, B.K.; Spielvogel, C.P.; Grubmüller, B.; Baltzer, P.A.T.; et al. Assessment of PSMA Expression of Healthy Organs in Different Stages of Prostate Cancer Using [68Ga]Ga-PSMA-11-PET Examinations. Cancers 2024, 16, 1514. https://doi.org/10.3390/cancers16081514
Einspieler H, Kluge K, Haberl D, Schatz K, Nics L, Schmitl S, Geist BK, Spielvogel CP, Grubmüller B, Baltzer PAT, et al. Assessment of PSMA Expression of Healthy Organs in Different Stages of Prostate Cancer Using [68Ga]Ga-PSMA-11-PET Examinations. Cancers. 2024; 16(8):1514. https://doi.org/10.3390/cancers16081514
Chicago/Turabian StyleEinspieler, Holger, Kilian Kluge, David Haberl, Katrin Schatz, Lukas Nics, Stefan Schmitl, Barbara Katharina Geist, Clemens P. Spielvogel, Bernhard Grubmüller, Pascal A. T. Baltzer, and et al. 2024. "Assessment of PSMA Expression of Healthy Organs in Different Stages of Prostate Cancer Using [68Ga]Ga-PSMA-11-PET Examinations" Cancers 16, no. 8: 1514. https://doi.org/10.3390/cancers16081514