
Perioperative Evaluation of the Physical Quality of Life of Patients with Non-Small Cell Lung Cancer: A Prospective Study

 , , ,
, , ,  and
and
Abstract
Simple Summary
Abstract
1. Introduction
2. Patients and Study Methods
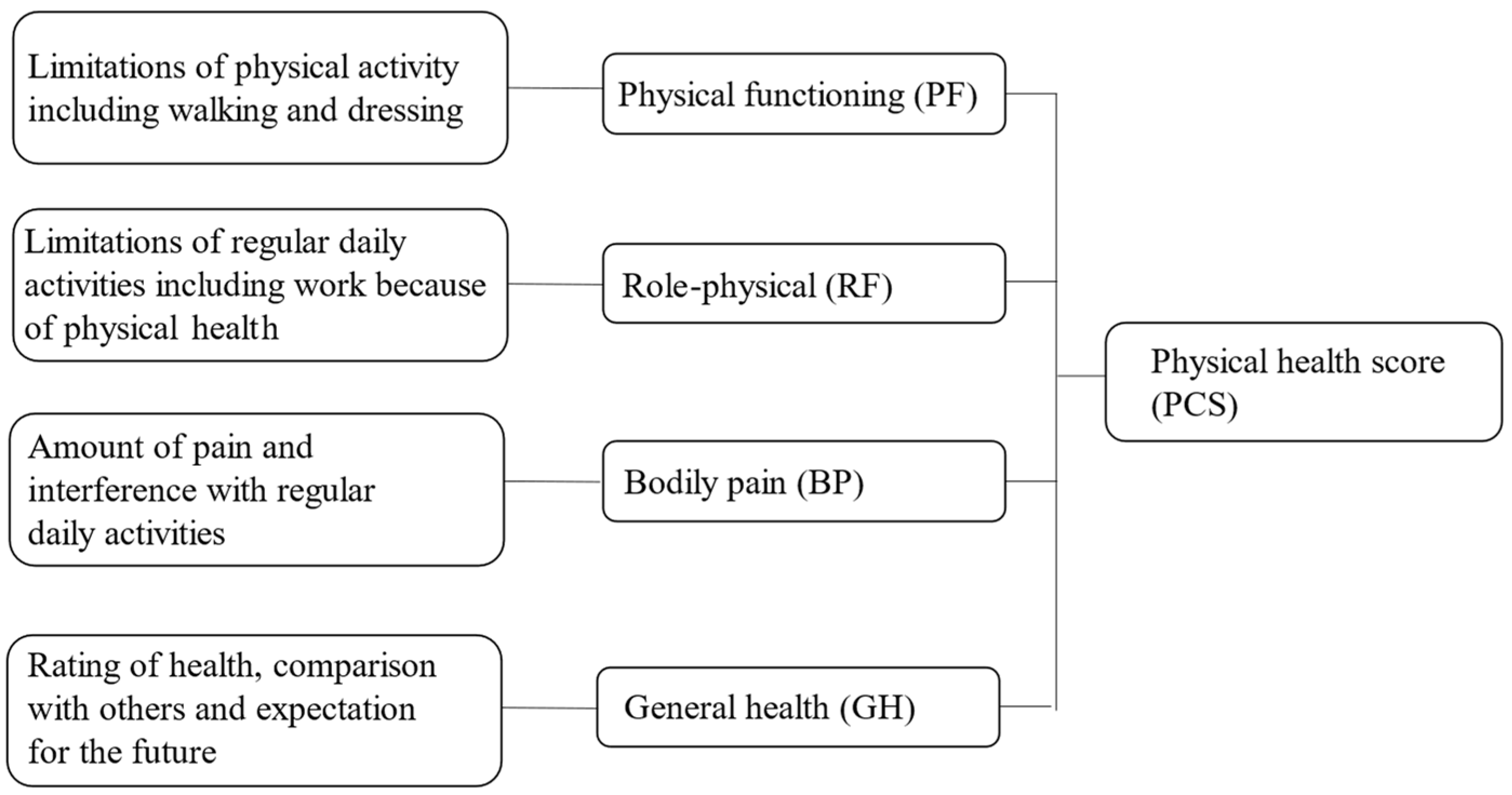
2.1. Quality of Life Assessment
2.2. Smoking Status
2.3. Performance Status
2.4. Living Conditions
2.5. Charlson Comorbidity Index
2.6. Statistical Analysis
3. Results
3.1. Baseline P-QOL Subscales
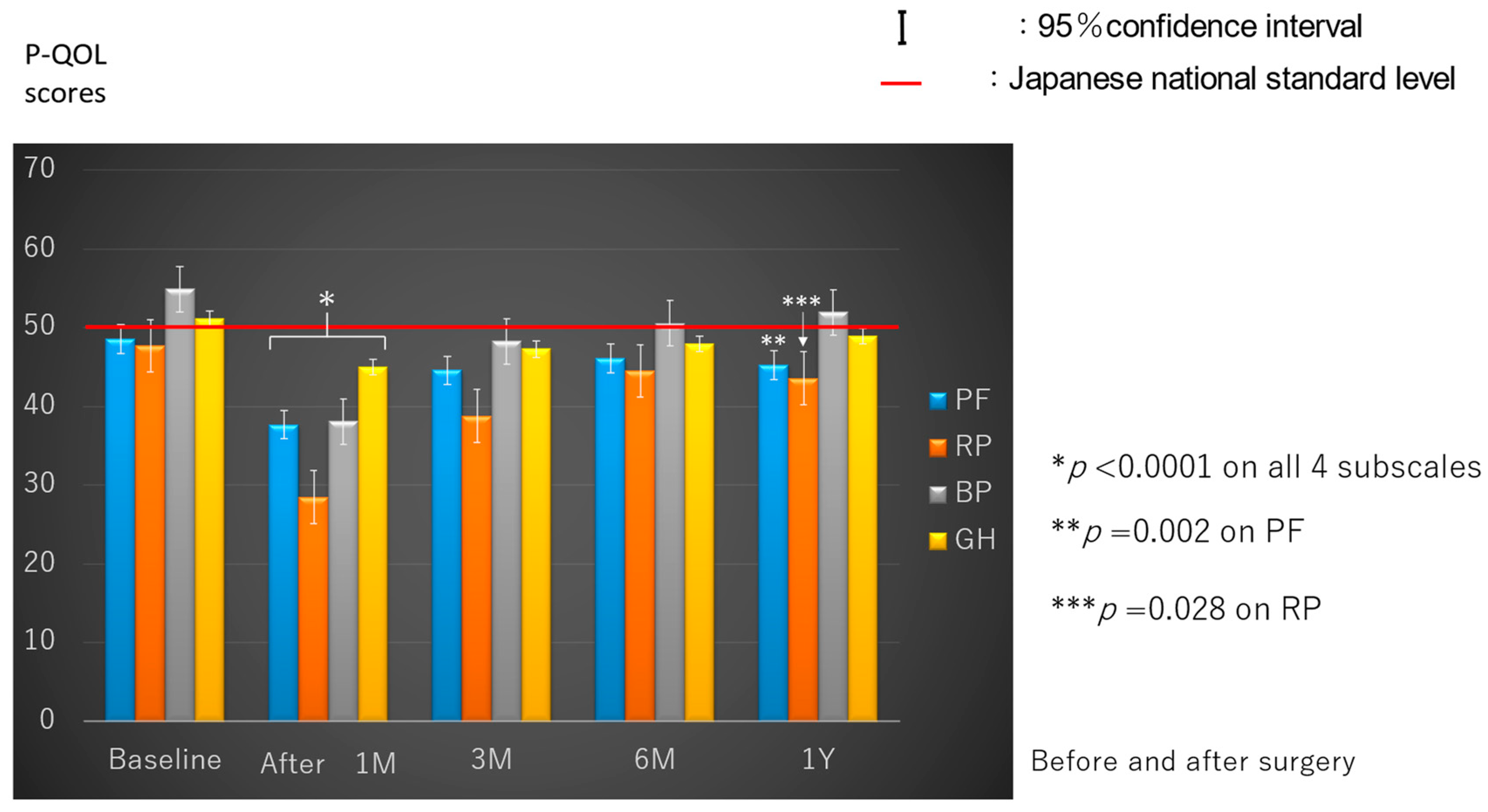
3.2. Postoperative P-QOL Evaluation
3.3. Predictors of Postoperative P-QOL
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

References
- Gajra, A.; Jatoi, A. Non-small-cell lung cancer in elderly patients: A discussion of treatment options. J. Clin. Oncol. 2014, 32, 2562–2569. [Google Scholar] [CrossRef] [PubMed]
- Bade, B.C.; Dela Cruz, C.S.D. Lung cancer 2020: Epidemiology, etiology, and prevention. Clin. Chest Med. 2020, 41, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Committee for Scientific Affairs, The Japanese Association for Thoracic Surgery; Minatoya, K.; Sato, Y.; Toh, Y.; Abe, T.; Endo, S.; Hirata, Y.; Ishida, M.; Iwata, H.; Kamei, T.; et al. Thoracic and cardiovascular surgeries in Japan during 2019: Annual report by the Japanese Association for Thoracic Surgery. Gen. Thorac. Cardiovasc. Surg. 2023, 71, 595–628. [Google Scholar] [PubMed]
- Booton, R.; Jones, M.; Thatcher, N. Lung cancer 7: Management of lung cancer in elderly patients. Thorax 2003, 58, 711–720. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Liu, N.; Andrew, N.E.; Cadilhac, D.A.; Yu, X.; Li, Z.; Wang, J.; Liang, Y. Health-related quality of life among elderly individuals living alone in an urban area of Shaanxi Province, China: A cross-sectional study. J. Int. Med. Res. 2020, 48, 300060520913146. [Google Scholar] [CrossRef] [PubMed]
- Allendorf, K. Going nuclear? Family structure and young women’s health in India, 1992–2006. Demography 2013, 50, 853–880. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.J.; Park, E.C.; Kim, S.J.; Lee, S.G. Quality of life of family members living with cancer patients. Asian Pac. J. Cancer Prev. 2015, 16, 6913–6917. [Google Scholar] [CrossRef] [PubMed]
- Poghosyan, H.; Sheldon, L.K.; Leveille, S.G.; Cooley, M.E. Health-related quality of life after surgical treatment in patients with non-small cell lung cancer: A systematic review. Lung Cancer 2013, 81, 11–26. [Google Scholar] [CrossRef]
- Movsas, B.; Moughan, J.; Sarna, L.; Langer, C.; Werner-Wasik, M.; Nicolaou, N.; Komaki, R.; Machtay, M.; Wasserman, T.; Bruner, D.W. Quality of life supersedes the classic prognosticators for long-term survival in locally advanced non-small-cell lung cancer: An analysis of RTOG 9801. J. Clin. Oncol. 2009, 27, 5816–5822. [Google Scholar] [CrossRef] [PubMed]
- Fukai, R.; Nishida, T.; Igarashi, Y.; Murata, T.; Sunoh, Y.; Miyake, K.; Isogai, N.; Shimoyama, R.; Kawachi, J.; Kashiwagi, H. Perioperative progress and predictor of the postoperative mental quality of life for lung cancer patients. Br. J. Cancer Res. 2021, 4, 485–490. [Google Scholar]
- Fukuhara, S.; Bito, S.; Green, J.; Hsiao, A.; Kurokawa, K. Translation, adaptation, and validation of the SF-36 health survey for use in Japan. J. Clin. Epidemiol. 1998, 51, 1037–1044. [Google Scholar] [CrossRef] [PubMed]
- McHorney, C.A.; Ware, J.E., Jr.; Lu, J.F.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36): III. Tests of data quality, scaling assumptions, and reliability across diverse patient groups. Med. Care 1994, 32, 40–66. [Google Scholar] [CrossRef] [PubMed]
- Möller, A.; Sartipy, U. Predictors of postoperative quality of life after surgery for lung cancer. J. Thorac. Oncol. 2012, 7, 406–411. [Google Scholar] [CrossRef] [PubMed]
- Myrdal, G.; Valtysdottir, S.; Lambe, M.; Ståhle, E. Quality of life following lung cancer surgery. Thorax 2003, 58, 194–197. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Sarna, L.; Cooley, M.E.; Brown, J.K.; Chernecky, C.; Padilla, G.; Danao, L.; Chakravarty, D.; Elashoff, D. Women with lung cancer: Quality of life after thoracotomy: A 6-month prospective study. Cancer Nurs. 2010, 33, 85–92. [Google Scholar] [CrossRef]
- Ostroff, J.S.; Krebs, P.; Coups, E.J.; Burkhalter, J.E.; Feinstein, M.B.; Steingart, R.M.; Logue, A.E.; Park, B.J. Health-related quality of life among early-stage, non-small cell, lung cancer survivors. Lung Cancer 2011, 71, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Oken, M.M.; Creech, R.H.; Tormey, D.C.; Horton, J.; Davis, T.E.; McFadden, E.T.; Carbone, P.P. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am. J. Clin. Oncol. 1982, 5, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Birim, O.; Maat, A.P.W.M.; Kappetein, A.P.; van Meerbeeck, J.P.; Damhuis, R.A.M.; Bogers, A.J.J.C. Validation of the Charlson comorbidity index in patients with operated primary non-small cell lung cancer. Eur. J. Cardiothorac. Surg. 2003, 23, 30–34. [Google Scholar] [CrossRef] [PubMed]
- Win, T.; Sharples, L.; Wells, F.C.; Ritchie, A.J.; Munday, H.; Laroche, C.M. Effect of lung cancer surgery on quality of life. Thorax 2005, 60, 234–238. [Google Scholar] [CrossRef] [PubMed]
- Balduyck, B.; Hendriks, J.; Lauwers, P.; Sardari Nia, P.; Van Schil, P. Quality of life evolution after lung cancer surgery in septuagenarians: A prospective study. Eur. J. Cardiothorac. Surg. 2009, 35, 1070–1075, discussion 1075. [Google Scholar] [CrossRef] [PubMed]
- Brunelli, A.; Socci, L.; Refai, M.; Salati, M.; Xiumé, F.; Sabbatini, A. Quality of life before and after major lung resection for lung cancer: A prospective follow-up analysis. Ann. Thorac. Surg. 2007, 84, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transpl. 2013, 48, 452–458. [Google Scholar] [CrossRef]
- Sok, M.; Zavrl, M.; Greif, B.; Srpčič, M. Objective assessment of WHO/ECOG performance status. Support. Care Cancer 2019, 27, 3793–3798. [Google Scholar] [CrossRef] [PubMed]
- Kawaguchi, Y.; Hanaoka, J.; Oshio, Y.; Hashimoto, M.; Igarashi, T.; Kataoka, Y.; Kaku, R.; Namura, Y.; Akazawa, A. Decrease in performance status after lobectomy mean poor prognosis in elderly lung cancer patients. J. Thorac. Dis. 2017, 9, 1525–1530. [Google Scholar] [CrossRef]
- Friedlaender, A.; Liu, S.V.; Passaro, A.; Metro, G.; Banna, G.; Addeo, A. The role of performance status in small-cell lung cancer in the era of immune checkpoint inhibitors. Clin. Lung Cancer 2020, 21, e539–e543. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Qiu, T.; Pei, L.; Zhang, Y.; Xu, L.; Cui, Y.; Liang, N.; Li, S.; Chen, W.; Huang, Y. Two-Week multimodal prehabilitation program improves perioperative functional capability in patients undergoing thoracoscopic lobectomy for lung cancer: A randomized controlled trial. Anesth. Analg. 2020, 131, 840–849. [Google Scholar] [CrossRef]
- Ahn, Y.E.; Koh, C.K. Effects of living alone and sedentary behavior on quality of life in patients with multimorbidities: A secondary analysis of cross-sectional survey data obtained from the national community database. J. Nurs. Res. 2021, 29, e173. [Google Scholar] [CrossRef]
- Lee, S.; Ma, C.; Zhang, S.; Ou, F.S.; Bainter, T.M.; Niedzwiecki, D.; Saltz, L.B.; Mayer, R.J.; Whittom, R.; Hantel, A.; et al. Marital status, living arrangement, and cancer recurrence and survival in patients with stage Ⅲ colon cancer: Findings from CALBG 89803 (alliance). Oncologist 2022, 27, e494–e505. [Google Scholar] [CrossRef]
- Cavalli-Björkman, N.; Qvortrup, C.; Sebjørnsen, S.; Pfeiffer, P.; Wentzel-Larsen, T.; Glimelius, B.; Sorbye, H. Lower treatment intensity and poorer survival in metastatic colorectal cancer patients who live alone. Br. J. Cancer 2012, 107, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Dalton, S.O.; Schüz, J.; Engholm, G.; Johansen, C.; Kjaer, S.K.; Steding-Jessen, M.; Storm, H.H.; Olsen, J.H. Social inequality in incidence of and survival from cancer in a population-based study in Denmark, 1994–2003: Summary of findings. Eur. J. Cancer 2008, 44, 2074–2085. [Google Scholar] [CrossRef]
- Cheng, L.; Sit, J.W.H.; Chan, H.Y.L.; Choi, K.C.; Cheung, R.K.Y.; Wong, M.M.H.; Li, F.Y.K.; Lee, T.Y.; Fung, E.S.M.; Tai, K.M.; et al. Sarcopenia risk and associated factors among Chinese community-dwelling older adults living alone. Sci. Rep. 2021, 11, 22219. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg, M.; Danovitch, I.; IsHak, W.W. Quality of life and smoking. Am. J. Addict. 2014, 23, 540–562. [Google Scholar] [CrossRef] [PubMed]
- Efendi, V.; Özalevli, S.; Naz, İ.; Kilinç, O. The effects of smoking on body composition, pulmonary function, physical activity and health-related quality of life among healthy women. Tuberk. Toraks 2018, 66, 101–108. [Google Scholar] [CrossRef] [PubMed]
- de Groot, P.; Munden, R.F. Lung cancer epidemiology, risk factors, and prevention. Radiol. Clin. N. Am. 2012, 50, 863–876. [Google Scholar] [CrossRef] [PubMed]
- Loeb, L.A.; Ernster, V.L.; Warner, K.E.; Abbotts, J.; Laszlo, J. Smoking and lung cancer: An overview. Cancer Res. 1984, 44, 5940–5958. [Google Scholar] [PubMed]
- Hays, J.T.; Croghan, I.T.; Baker, C.L.; Cappelleri, J.C.; Bushmakin, A.G. Changes in health-related quality of life with smoking cessation treatment. Eur. J. Public Health 2012, 22, 224–229. [Google Scholar] [CrossRef] [PubMed]
- Batchelor, T.J.P.; Rasburn, N.J.; Abdelnour-Berchtold, E.; Brunelli, A.; Cerfolio, R.J.; Gonzalez, M.; Ljungqvist, O.; Petersen, R.H.; Popescu, W.M.; Slinger, P.D.; et al. Guidelines for enhanced recovery after lung surgery: Recommendations of the enhanced recovery after surgery (ERAS®) society and the European society of thoracic surgeons (ESTS). Eur. J. Cardiothorac. Surg. 2019, 55, 91–115. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chron. Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Asmis, T.R.; Ding, K.; Seymour, L.; Shepherd, F.A.; Leighl, N.B.; Winton, T.L.; Whitehead, M.; Spaans, J.N.; Graham, B.C.; Goss, G.D. Age and comorbidity as independent prognostic factors in the treatment of non-small cell lung cancer: A review of National Cancer Institute of Canada Clinical Trials Group trials. J. Clin. Oncol. 2008, 26, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Wahlgren, T.; Levitt, S.; Kowalski, J.; Nilsson, S.; Brandberg, Y. Use of the Charlson combined comorbidity index to predict postradiotherapy quality of life for prostate cancer patients. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, 997–1004. [Google Scholar] [CrossRef] [PubMed]
- Jacot, W.; Colinet, B.; Bertrand, D.; Lacombe, S.; Bozonnat, M.C.; Daurès, J.P.; Pujol, J.L.; OncoLR Health Network. Quality of life and comorbidity score as prognostic determinants in non-small-cell lung cancer patients. Ann. Oncol. 2008, 19, 1458–1464. [Google Scholar] [CrossRef] [PubMed]
- Tsunoda, A.; Nakao, K.; Watanabe, M.; Matsui, N.; Tsunoda, Y. Health-related quality of life in patients with colorectal cancer who receive oral uracil and tegafur plus leucovorin. Jpn. J. Clin. Oncol. 2010, 40, 412–419. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Oun, R.; Moussa, Y.E.; Wheate, N.J. The side effects of platinum-based chemotherapy drugs: A review for chemists. Dalton Trans. 2018, 47, 6645–6653. [Google Scholar] [CrossRef] [PubMed]
- McHorney, C.A.; Ware, J.E., Jr.; Raczek, A.E. The MOS 36-item short-form health survey (SF-36): II. Psychometric and clinical tests of validity in measuring physical and mental health constructs. Med. Care 1993, 31, 247–263. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Characteristics | Number (%) |
|---|---|
| Age (years) | |
| Mean ± SD (range) | 69.7 ± 8.5 (48–83) |
| Sex | |
| Male | 41 (47) |
| Female | 46 (53) |
| Performance status | |
| 0 | 72 (83) |
| 1–2 | 15 (17) |
| 3–5 | 0 (0) |
| Smoking status | |
| Stopped within 1 year preoperatively | 17 (20) |
| Remote or never smokers | 70 (80) |
| Living conditions | |
| Living alone | 10 (11) |
| Living with somebody | 77 (89) |
| Charlson comorbidity index | |
| <3 | 77 (89) |
| ≥3 | 10 (11) |
| Surgical approach | |
| Thoracoscopic | 74 (85) |
| Thoracotomy | 13 (15) |
| Procedure | |
| Segmentectomy | 5 (6) |
| Lobectomy | 79 (91) |
| Bilobectomy | 2 (2) |
| Pneumonectomy | 1 (1) |
| Histology | |
| Adenocarcinoma | 73 (84) |
| Squamous cell carcinoma | 12 (14) |
| Adenosquamous | 1 (1) |
| Carcinoid | 1(1) |
| Pathologic stage | |
| IA | 35 (40) |
| IB | 27 (31) |
| IIA | 7 (8) |
| IIB | 12 (14) |
| IIIA | 6 (7) |
| Variables | No. of | P-QOL Score | p-Value |
|---|---|---|---|
| Patients (%) | (Mean ± SD) | ||
| Age (years) | 0.022 | ||
| <70 | 35 (40) | 53.0 ± 6.1 | |
| ≥70 | 52 (60) | 46.5 ± 8.4 | |
| Sex | 0.25 | ||
| Male | 41 (47) | 49.5 ± 9.0 | |
| Female | 46 (53) | 51.5 ± 7.1 | |
| Smoking status | 0.025 | ||
| Stopped within | 17 (20) | 46.7 ± 10.6 | |
| 1 year preoperatively | |||
| Remote or never | 70 (80) | 51.5 ± 7.1 | |
| smokers | |||
| Performance status | <0.0001 | ||
| 0 | 72 (83) | 52.8 ± 6.0 | |
| 1–2 | 15 (17) | 41.8 ± 9.2 | |
| Living conditions | <0.001 | ||
| Living alone | 10 (11) | 42.0 ± 10.4 | |
| Living with | 77 (89) | 51.7 ± 7.1 | |
| somebody | |||
| Charlson comorbidity index | 0.47 | ||
| <3 | 77 (89) | 50.8 ± 7.3 | |
| ≥3 | 10 (11) | 48.8 ± 12.9 |
| Variables | Regression Coefficient (95% CI) | p-Value |
|---|---|---|
| Age | −0.88 (−3.80–2.05) | 0.553 |
| (≥70 years or not) | ||
| Smoking status | 2.47 (−0.96–5.90) | 0.156 |
| (Remote or never smokers or not) | ||
| Living conditions | −9.37 (−13.43–−5.32) | <0.0001 |
| (Living alone or not) | ||
| Performance status | −10.22 (−13.74–−7.40) | <0.0001 |
| (≥1 or not) | ||
| Variables | No. of | P-QOL Score | p-Value |
|---|---|---|---|
| Patients (%) | (Mean ± SD) | ||
| Age (years) | 0.336 | ||
| <70 | 35 (40) | 47.4 ± 8.4 | |
| ≥70 | 52 (60) | 46.5 ± 8.4 | |
| Sex | 0.43 | ||
| Male | 41 (47) | 46.4 ± 10.0 | |
| Female | 46 (53) | 47.9 ± 6.9 | |
| Smoking status | 0.002 | ||
| Stopped within | 17 (20) | 41.0 ± 10.5 | |
| 1 year preoperatively | |||
| Remote or never | 70 (80) | 48.6 ± 7.2 | |
| smokers | |||
| Performance status | <0.0001 | ||
| 0 | 72 (83) | 49.3 ± 6.6 | |
| 1–2 | 15 (17) | 38.6 ± 9.6 | |
| Living conditions | 0.021 | ||
| Living alone | 10 (11) | 41.6 ± 9.7 | |
| Living with | 77 (89) | 48.1 ± 7.9 | |
| somebody | |||
| Charlson comorbidity index | 0.003 | ||
| <3 | 77 (89) | 48.2 ± 6.9 | |
| ≥3 | 10 (11) | 39.1 ± 14.7 |
| Variables | Regression Coefficient (95% CI) | p-Value |
|---|---|---|
| Smoking status | −4.90 (−8.78–1.0) | 0.014 |
| (Stopped smoking within 1 years or not) | ||
| Performance status | 8.90 (5.10–12.70) | <0.0001 |
| (0 or not) | ||
| Living conditions | 5.76 (1.39–10.13) | 0.01 |
| (Living with somebody or not) | ||
| Charlson comorbidity index | −6.94 (−11.78–−2.10) | 0.006 |
| (≥3 or not) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fukai, R.; Nishida, T.; Sugimoto, H.; Hibino, M.; Horiuchi, S.; Kondo, T.; Teshima, S.; Hirata, M.; Asou, K.; Shimizu, E.; et al. Perioperative Evaluation of the Physical Quality of Life of Patients with Non-Small Cell Lung Cancer: A Prospective Study. Cancers 2024, 16, 1527. https://doi.org/10.3390/cancers16081527
Fukai R, Nishida T, Sugimoto H, Hibino M, Horiuchi S, Kondo T, Teshima S, Hirata M, Asou K, Shimizu E, et al. Perioperative Evaluation of the Physical Quality of Life of Patients with Non-Small Cell Lung Cancer: A Prospective Study. Cancers. 2024; 16(8):1527. https://doi.org/10.3390/cancers16081527
Chicago/Turabian StyleFukai, Ryuta, Tomoki Nishida, Hideyasu Sugimoto, Makoto Hibino, Shigeto Horiuchi, Tetsuri Kondo, Shinichi Teshima, Masahiro Hirata, Keiko Asou, Etsuko Shimizu, and et al. 2024. "Perioperative Evaluation of the Physical Quality of Life of Patients with Non-Small Cell Lung Cancer: A Prospective Study" Cancers 16, no. 8: 1527. https://doi.org/10.3390/cancers16081527
APA StyleFukai, R., Nishida, T., Sugimoto, H., Hibino, M., Horiuchi, S., Kondo, T., Teshima, S., Hirata, M., Asou, K., Shimizu, E., Saito, Y., & Sakao, Y. (2024). Perioperative Evaluation of the Physical Quality of Life of Patients with Non-Small Cell Lung Cancer: A Prospective Study. Cancers, 16(8), 1527. https://doi.org/10.3390/cancers16081527