

Drug Cost Avoidance Resulting from Participation in Clinical Trials: A 10-Year Retrospective Analysis of Cancer Patients with Solid Tumors
 , , , ,
, , , ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Design and Patients
2.2. Study Variables
2.3. Pharmaceutical Expenditure, Sponsor Contribution, and Drug Cost Avoidance
2.4. Statistical Analysis
3. Results
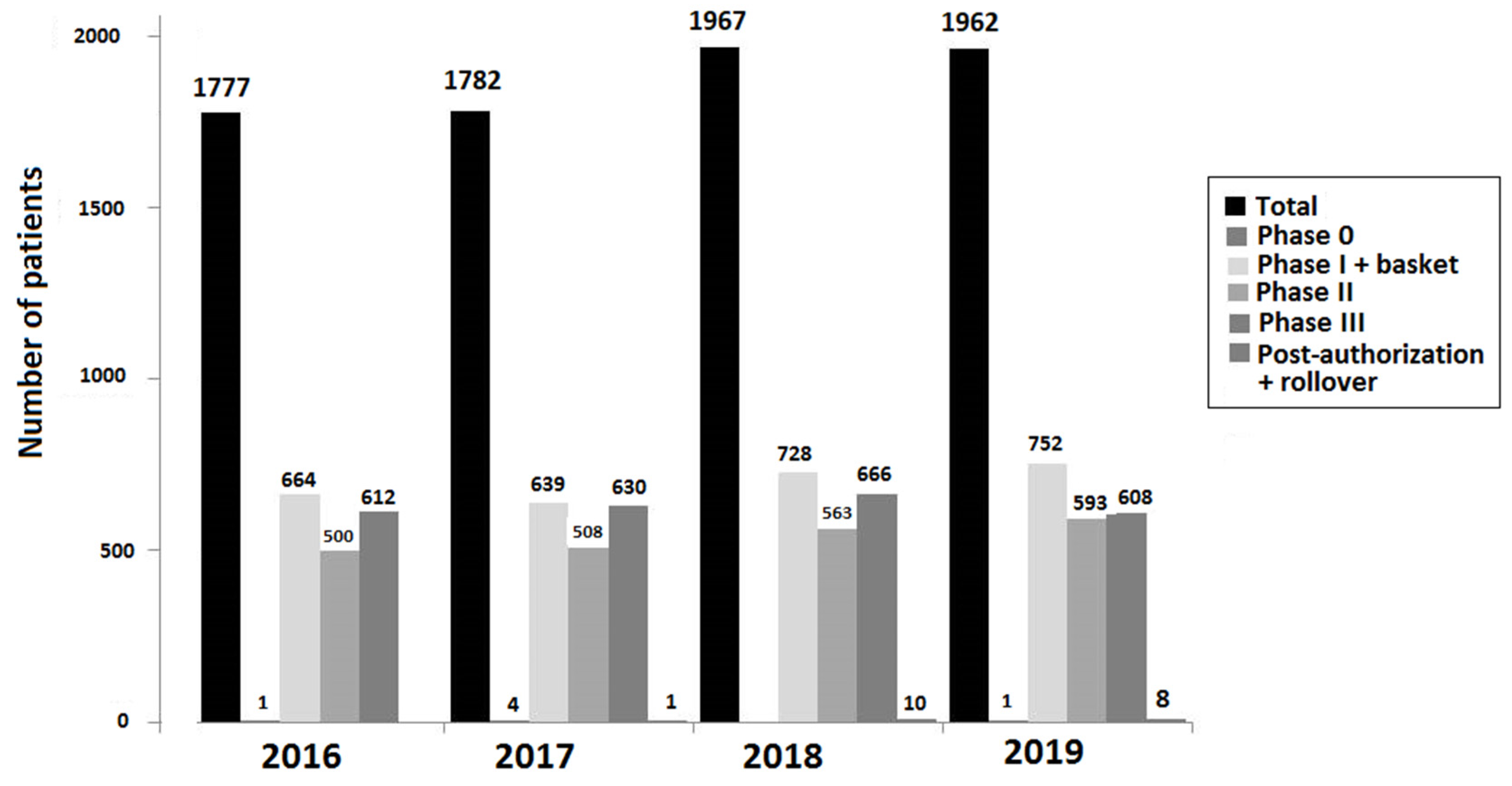
3.1. Clinical Trials and Patient Population
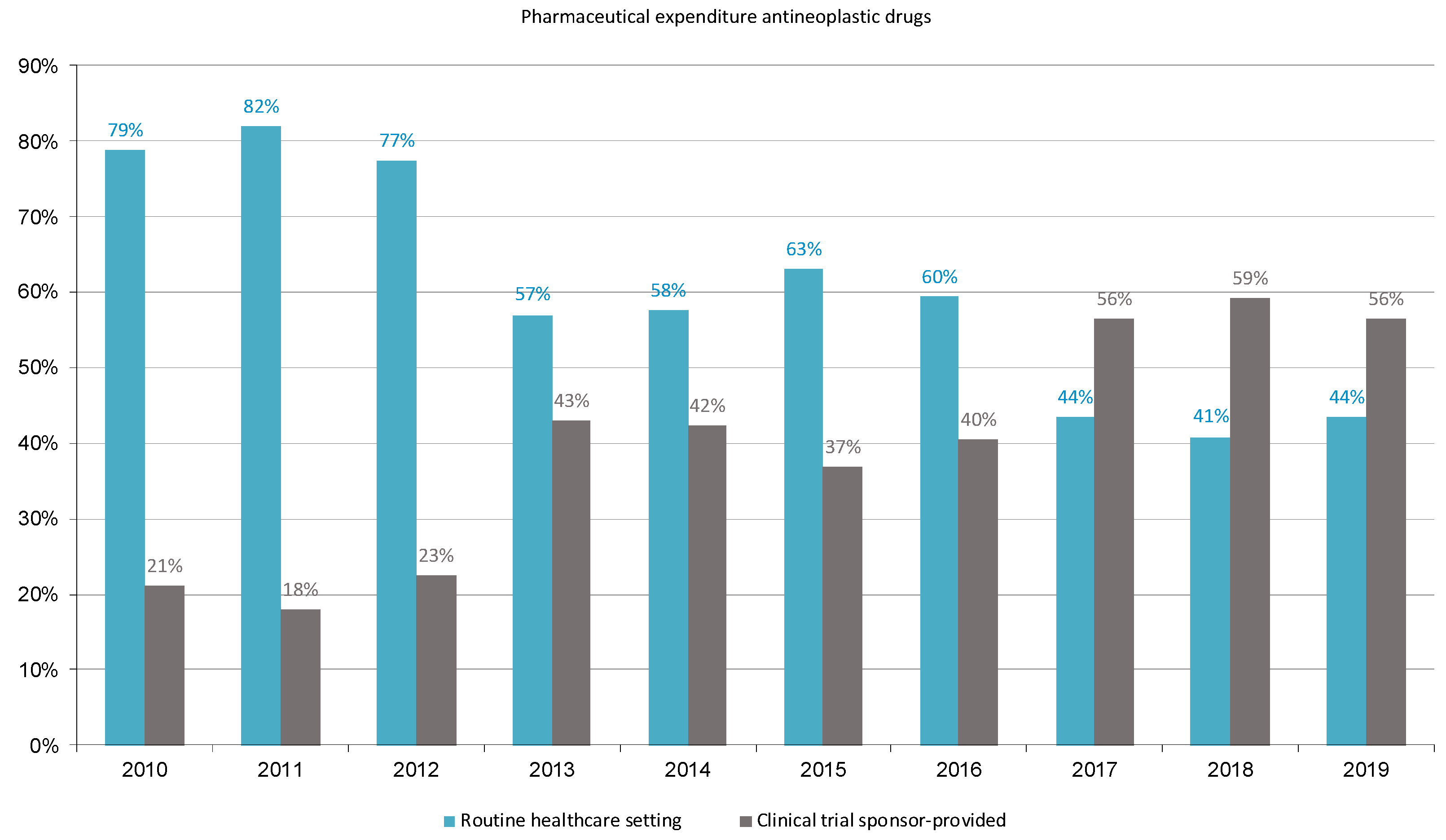
3.2. Pharmaceutical Expenditure on Cancer Treatment in Clinical Trials (Financial Contribution from the Sponsor)
3.3. Expenditure by Pharmacological Classes
3.4. Expenditure by Antineoplastic Agent
3.5. Expenditure by Tumor Location
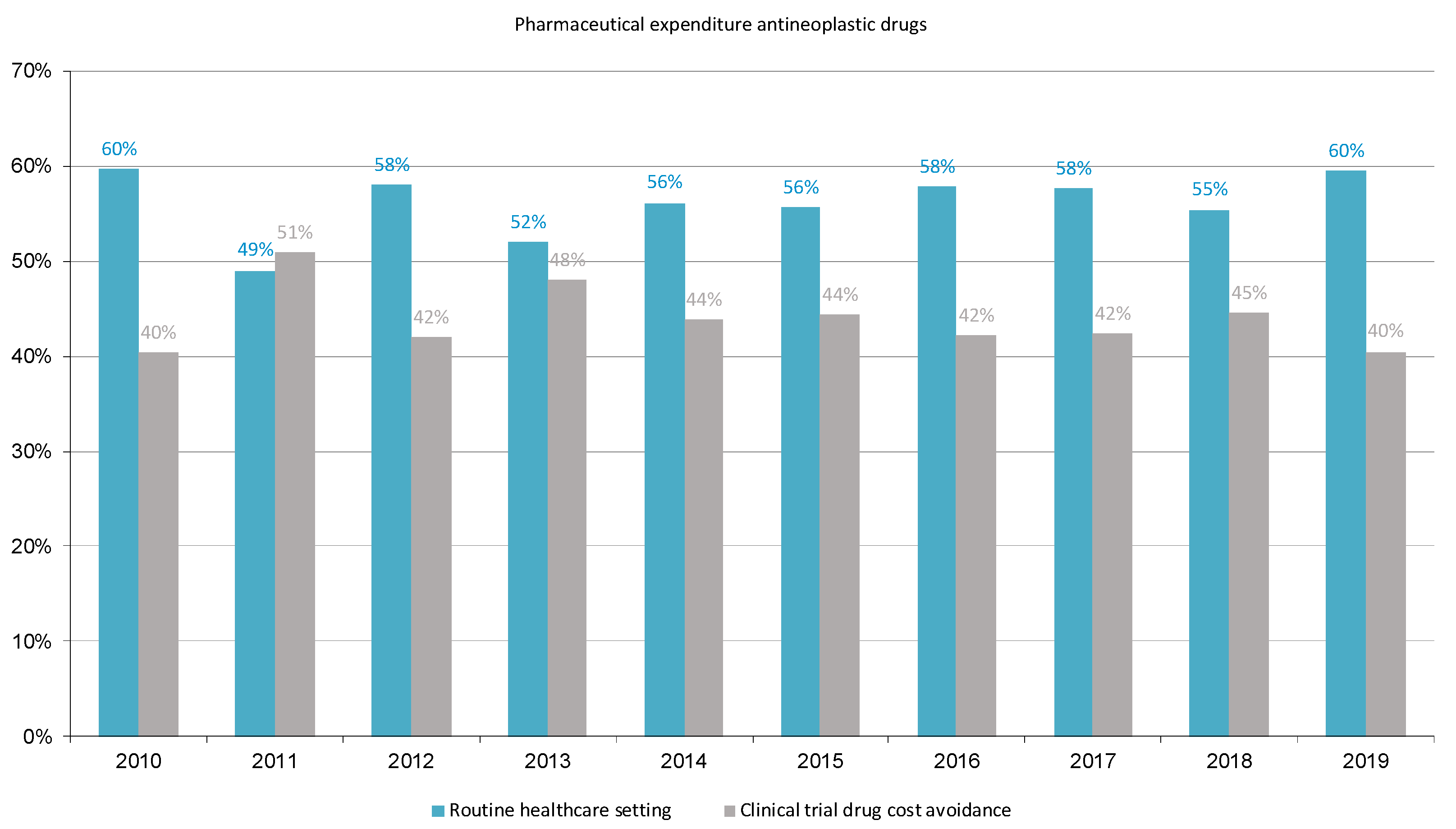
3.6. Estimation of Potential Drug Cost Avoidance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Workman, P.; Draetta, G.F.; Schellens, J.H.M.; Bernards, R. How much longer will we put up with $100,000 cancer drugs? Cell 2017, 168, 579–583. [Google Scholar] [CrossRef] [PubMed]
- Negrouk, A.; Lacombe, D.; Cardoso, F.; Morin, F.; Carrasco, E.; Maurel, J.; Maibach, R.; Aranda, E.; Marais, R.; Stahel, R.A. Safeguarding the future of independent, academic clinical cancer research in Europe for the benefit of patients. ESMO Open 2017, 2, e000187. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency, 1 September 2022, EudraCT Public Web Report for August 2022. Available online: https://eudract.ema.europa.eu/docs/statistics/EudraCT_Statistics_2022/EudraCT_Public_Web_Report_for_August_2022.pdf (accessed on 13 November 2023).
- Wagner, J.L.; Alberts, S.R.; Sloan, J.A.; Cha, S.; Killian, J.; O‘Connell, M.J.; Van Grevenhof, P.; Lindman, J.; Chute, C.G. Incremental costs of enrolling cancer patients in clinical trials: A population-based study. J. Natl. Cancer Inst. 1999, 91, 847–853. [Google Scholar] [CrossRef] [PubMed]
- Fireman, B.H.; Fehrenbacher, L.; Gruskin, E.P.; Ray, G.T. Cost of care for patients in cancer clinical trials. J. Natl. Cancer Inst. 2000, 92, 136–142. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Bennett, C.L.; Stinson, T.J.; Vogel, V.; Robertson, L.; Leedy, D.; O‘Brien, P.; Hobbs, J.; Sutton, T.; Ruckdeschel, J.C.; Chirikos, T.N.; et al. Evaluating the financial impact of clinical trials in oncology: Results from a pilot study from the Association of American Cancer Institutes/Northwestern University clinical trials costs and charges project. J. Clin. Oncol. 2000, 18, 2805–2810. [Google Scholar] [CrossRef] [PubMed]
- Goldman, D.P.; Berry, S.H.; McCabe, M.S.; Kilgore, M.L.; Potosky, A.L.; Schoenbaum, M.L.; Schonlau, M.; Weeks, J.C.; Kaplan, R.; Escarce, J.J. Incremental treatment costs in national cancer institute-sponsored clinical trials. JAMA 2003, 289, 2970–2977. [Google Scholar] [CrossRef] [PubMed]
- Jones, B.; Syme, R.; Eliasziw, M.; Eigl, B.J. Incremental costs of prostate cancer trials: Are clinical trials really a burden on a public payer system? Can. Urol. Assoc. J. 2013, 7, E231–E236. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Jones, B.; Eliasziw, M.; Eigl, B.J.; Syme, R. A comparison of incremental costs of breast cancer clinical trials to standard of care. J. Clin. Trials 2015, 5, 216. [Google Scholar] [CrossRef]
- McDonagh, M.S.; Miller, S.A.; Naden, E. Costs and savings of investigational drug services. Am. J. Health Syst. Pharm. 2000, 57, 40–43. [Google Scholar] [CrossRef]
- LaFleur, J.; Tyler, L.S.; Sharma, R.R. Economic benefits of investigational drug services at an academic institution. Am. J. Health Syst. Pharm. 2004, 61, 27–32. [Google Scholar] [CrossRef]
- Shen, L.J.; Chou, H.; Huang, C.F.; Chou, G.M.; Chan, W.K.; Wu, F.L. Economic benefits of sponsored clinical trials on pharmaceutical expenditures at a medical center in Taiwan. Contemp. Clin. Trials 2011, 32, 485–491. [Google Scholar] [CrossRef]
- Uecke, O.; Reszka, R.; Linke, J.; Steul, M.; Posselt, T. Clinical trials: Considerations for researchers and hospital administrators. Health Care Manag. Rev. 2008, 33, 103–112. [Google Scholar] [CrossRef]
- Grossi, F.; Genova, C.; Gaitan, N.D.; Dal Bello, M.G.; Rijavec, E.; Barletta, G.; Sini, C.; Donato, C.; Beltramini, S.; Pronzato, P.; et al. Free drugs in clinical trials and their potential cost saving impact on the National Health Service: A retrospective cost analysis in Italy. Lung Cancer 2013, 81, 236–240. [Google Scholar] [CrossRef] [PubMed]
- Tang, P.A.; Hay, A.E.; O‘Callaghan, C.J.; Mittmann, N.; Chambers, C.R.; Pater, J.L.; Leighl, N.B. Estimation of drug cost avoidance and pathology cost avoidance through participation in NCIC Clinical Trials Group phase III clinical trials in Canada. Curr. Oncol. 2016, 23 (Suppl. S1), S7–S13. [Google Scholar] [CrossRef]
- Liniker, E.; Harrison, M.; Weaver, J.M.; Agrawal, N.; Chhabra, A.; Kingshott, V.; Bailey, S.; Eisen, T.G.; Corrie, P.G. Treatment costs associated with interventional cancer clinical trials conducted at a single UK institution over 2 years (2009–2010). Br. J. Cancer 2013, 109, 2051–2057. [Google Scholar] [CrossRef]
- Calvin-Lamas, M.; Portela-Pereira, P.; Rabuñal-Alvarez, M.T.; Martinez-Breijo, S.; Martín-Herranz, M.I.; Gómez-Veiga, F. Drug cost avoidance in prostate cancer clinical trials. Actas Urol. Esp. 2015, 39, 553–557. [Google Scholar] [CrossRef] [PubMed]
- Mañes-Sevilla, M.; Romero-Jiménez, R.; Herranz-Alonso, A.; Sánchez-Fresneda, M.; Gonzalez-Haba, E.; Collado-Borrel, R.; Benedi-González, J.; Sanjurjo-Sáez, M. Drug cost avoidance in clinical trials of breast cancer. J. Oncol. Pharm. Pract. 2019, 25, 1099–1104. [Google Scholar] [CrossRef]
- Capdevila, F.; Vera, R.; Ochoa, P.; Galbete, A.; Sanchez-Iriso, E. Cancer clinical trials: Treatment costs associated with a Spanish National Health System Institution. Ther. Innov. Regul. Sci. 2019, 53, 641–647. [Google Scholar] [CrossRef] [PubMed]
- Carreras, M.J.; Tomás-Guillén, E.; Farriols, A.; Renedo-Miró, B.; Valdivia, C.; Vidal, J.; Saura, C.; Carles, J.; Felip, E.; Gorgas, M.Q.; et al. Use of drugs in clinical practice and the associated cost of cancer treatment in adult patients with solid tumors: A 10-year retrospective cohort study. Curr. Oncol. 2023, 30, 7984–8004. [Google Scholar] [CrossRef]
- Hospital Universitari Vall d’Hebron, 2018 Hospital Memory. Available online: https://www.vallhebron.com/sites/default/filesmemoria-hospital-vall-hebron-2018.pdf (accessed on 4 May 2023).
- Cancer Types, National Cancer Institute at the National Institutes of Health. Available online: https://www.cancer.gov/types (accessed on 8 May 2023).
- CIMA, Centro de Información Online de Medicamentos de la AEMPS, Online Drug Information Center of the AEMPS. Available online: https://cima.aemps.es/cima/publico/home.html (accessed on 8 May 2023).
- Registro Español de Estudios Clínicos (REEC). AEMPS. Available online: https://reec.aemps.es/reec/public/list.html (accessed on 8 May 2023).
- Llisterri Caro, J.L.; Martín, J.V. Research as a source of sustainability of the health system in primary care. Semergen 2013, 39, 1–2. [Google Scholar] [CrossRef]
- Gasperoni, L.; Cafaro, A.; Ferretti, E.; Di Iorio, V.; Nanni, O.; Masini, C. The role of clinical trials in the sustainability of the Italian national health service cancer drug expenditure. Eur. J. Hosp. Pharm. 2023, 30, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Walter, E.; Eichhober, G.; Voit, M.; Baumgartner, C.; Celedin, A.; Holzhauser, C.; Mraz, B.; Ornauer, C.; Pleiner-Duxneuner, J.; Ponner, B.; et al. Economic impact of industry-sponsored clinical trials of pharmaceutical products in Austria. J. Med. Econ. 2020, 23, 566–574. [Google Scholar] [CrossRef]
- D‘Ambrosio, F.; De Feo, G.; Botti, G.; Capasso, A.; Pignata, S.; Maiolino, P.; Triassi, M.; Nardone, A.; Perrone, F.; Piezzo, M.; et al. Clinical trials and drug cost savings for Italian health service. BMC Health Serv. Res. 2020, 20, 1089. [Google Scholar] [CrossRef]
- Bentley, C.; Cressman, S.; van der Hoek, K.; Arts, K.; Dancey, J.; Peacock, S. Conducting clinical trials-costs, impacts, and the value of clinical trials networks: A scoping review. Clin. Trials 2019, 16, 183–193. [Google Scholar] [CrossRef] [PubMed]
- Bredin, C.; Eliasziw, M.; Syme, R. Drug cost avoidance resulting from cancer clinical trials. Contemp. Clin. Trials 2010, 31, 524–529. [Google Scholar] [CrossRef]
- Seow, H.Y.; Whelan, P.; Levine, M.N.; Cowan, K.; Lysakowski, B.; Kowaleski, B.; Snider, A.; Xu, R.Y.; Arnold, A. Funding oncology clinical trials: Are cooperative group trials sustainable? J. Clin. Oncol. 2012, 30, 1456–1461. [Google Scholar] [CrossRef]
- Carreras, M.J. Analysis of Pharmaceutical Expenditure in the Treatment of Solid Tumors at the Vall d‘Hebron University Hospital and Its Contribution to the Sustainability of the Healthcare System. Ph.D. Thesis, Universitat Autònoma de Barcelona, Barcelona, Spain, 2020. Available online: http://hdl.handle.net/10803/670441 (accessed on 3 January 2024).




{kind=link}
{kind=link}
{kind=link}
| Study Year | Clinical Trials | |||||
|---|---|---|---|---|---|---|
| Total | Phase 0 n (%) | Phase I and Basket n (%) | Phase II n (%) | Phase III n (%) | Post-Authorization and Rollovers n (%) | |
| 2010 | 140 | 0 | 37 (26.4) | 54 (38,6) | 49 (35.0) | 0 |
| 2011 | 161 | 0 | 48 (29.8) | 57 (35.4) | 56 (34.8) | 0 |
| 2012 | 219 | 0 | 66 (30.1) | 85 (38.8) | 68 (31.0) | 0 |
| 2013 | 232 | 0 | 75 (32.3) | 96 (41.4) | 61 (26.3) | 0 |
| 2014 | 251 | 0 | 83 (33.1) | 99 (39,4) | 64 (25.5) | 5 (2.0) |
| 2015 | 303 | 0 | 106 (35.0) | 94 (31.0) | 89 (29.4) | 14 (4.6) |
| 2016 | 370 | 0 | 129 (34.9) | 117 (31.6) | 108 (29.2) | 16 (4.3) |
| 2017 | 374 | 0 | 137 (36.6) | 107 (28.6) | 111 (29.7) | 19 (5.1) |
| 2018 | 421 | 0 | 161 (38.2) | 131 (31.1) | 107 (25.4) | 22 (5.2) |
| 2019 | 459 | 1 (0.2) | 162 (35.3) | 141 (30.7) | 121 (26.4) | 34 (7.4) |
| 2010–2019 | 2930 | 1 (0.03) | 1004 (34.3) | 981 (33.5) | 834 (28.5) | 110 (3.7) |
| Study Years | Expenditures of Antineoplastic Drugs | |
|---|---|---|
| Intravenous | Oral | |
| 2010 | EUR 2,457,850 | NR |
| 2011 | EUR 1,700,250 | NR |
| 2012 | EUR 2,203,633 | NR |
| 2013 | EUR 3,331,912 | EUR 1,845,309 |
| 2014 | EUR 4,636,490 | EUR 2,022,064 |
| 2015 | EUR 4,120,596 | EUR 2,876,494 |
| 2016 | EUR 6,220,320 | EUR 3,545,183 |
| 2017 | EUR 12,675,915 | EUR 6,086,139 |
| 2018 | EUR 17,844,749 | EUR 8,166,853 |
| 2019 | EUR 17,074,664 | EUR 10,497,663 |
| Total | EUR 72,266,379 | EUR 35,039,705 |
| Overall | EUR 107,306,084 | |
| Cytotoxic Drugs | Immunotherapy | Targeted Therapy | Other Drugs | Total | |
|---|---|---|---|---|---|
| Antineoplastic drugs | |||||
| Intravenous | EUR 6,322,282 | EUR 35,623,961 | EUR 23,958,403 | EUR 65,904,646 | |
| Oral | EUR 424,306 | EUR 34,609,333 | EUR 6066 | EUR 35,039,705 | |
| Total | EUR 6,746,588 | EUR 35,623,961 | EUR 58,567,736 | EUR 100,944,351 | |
| Study year | |||||
| 2013 | EUR 957,915 | EUR 590,250 | EUR 3,629,056 | EUR 5,177,221 | |
| 2014 | EUR 613,360 | EUR 1,517,637 | EUR 4,527,558 | EUR 6,658,554 | |
| 2015 | EUR 796,317 | EUR 222,342 | EUR 5,978,431 | EUR 6,997,090 | |
| 2016 | EUR 891,738 | EUR 2,536,316 | EUR 6,337,449 | EUR 9,765,502 | |
| 2017 | EUR 1,175,345 | EUR 6,900,964 | EUR 10,685,745 | EUR 18,762,054 | |
| 2018 | EUR 1,001,328 | EUR 12,169,256 | EUR 12,841,019 | EUR 26,011,603 | |
| 2019 | EUR 1,310,587 | EUR 11,687,195 | EUR 14,568,479 | EUR 6066 | EUR 27,572,327 |
| Study Year | Cytotoxic Drugs | Immunotherapy | Targeted Therapy | Total Expenditure | Change vs. Previous Year, % |
|---|---|---|---|---|---|
| 2010 | EUR 506,138 | -EUR | EUR 1,951,712 | EUR 2,457,850 | |
| 2011 | EUR 599,725 | -EUR | EUR 1,100,526 | EUR 1,700,250 | −30.8% |
| 2012 | EUR 860,070 | -EUR | EUR 1,343,563 | EUR 2,203,633 | 29.6 |
| 2013 | EUR 863,237 | EUR 590,250 | EUR 1,848,425 | EUR 3,331,912 | 51.2 |
| 2014 | EUR 568,777 | EUR 1,517,637 | EUR 2,550,076 | EUR 4,636,490 | 39.1 |
| 2015 | EUR 787,984 | EUR 222,342 | EUR 3,110,270 | EUR 4,120,596 | −11.1 |
| 2016 | EUR 866,817 | EUR 2,536,316 | EUR 2,817,187 | EUR 6,220,320 | 51.0 |
| 2017 | EUR 1,047,329 | EUR 6,900,964 | EUR 4,727,621 | EUR 12,675,915 | 103.8 |
| 2018 | EUR 940,547 | EUR 12,169,256 | EUR 4,734,946 | EUR 17,844,749 | 40.8 |
| 2019 | EUR 1,217,591 | EUR 11,687,195 | EUR 4,169,878 | EUR 17,074,664 | −4.3 |
| 2010 | 2019 | ||||
|---|---|---|---|---|---|
| Antineoplastic Agent | Expenditure | % of Total Expenditure | Antineoplastic Agent | Expenditure | % of Total Expenditure |
| Trastuzumab | EUR 919,484 | 37.4 | Pembrolizumab | EUR 3,590,128.10 | 13.0 |
| Bevacizumab | EUR 449,063 | 18.3 | Nivolumab | EUR 2,489,205.42 | 9.0 |
| Aflibercept/placebo | EUR 301,600 | 12.3 | Cabozantinib | EUR 2,392,934.10 | 8.7 |
| Docetaxel | EUR 191,287 | 7.8 | Atezolizumab | EUR 1,983,242.04 | 7.2 |
| Pemetrexed | EUR 145,919 | 5.9 | Bevacizumab | EUR 1,696,849.55 | 6.1 |
| Cetuximab | EUR 145,079 | 5.9 | Palbociclib | EUR 1,449,416.28 | 5.3 |
| Panitumumab | EUR 129,287 | 5.3 | Olaparib | EUR 1,338,767.04 | 4.9 |
| Total | 92.8 | Lorlatinib | EUR 1,094,262.59 | 4.0 | |
| Ipilumumab | EUR 786,563.46 | 2.8 | |||
| Pembrolizumab | EUR 670,891,67 | 2.4 | |||
| Pemetrexed | EUR 615,425.91 | 2.2 | |||
| Pertuzumab | EUR 581,406.00 | 2.1 | |||
| Avelumab | EUR 568,416.00 | 2.1 | |||
| Abiraterone | EUR 500,524.62 | 1.8 | |||
| Pembrolizumab/placebo | EUR 405,841.74 | 1.5 | |||
| Cetuximab | EUR 393,887.10 | 1.4 | |||
| Lenvatinib | EUR 386,416.81 | 1.4 | |||
| Dinutuximab | EUR 348,727.07 | 1.3 | |||
| Atezolizumab/placebo | EUR 326,070.63 | 1.2 | |||
| Osimertinib | EUR 300,501.60 | 1.1 | |||
| Sunitinib | EUR 299,647.57 | 1.1 | |||
| BMS-986213/Nivolumab | EUR 289,906.56 | 1.0 | |||
| Axitinib | EUR 280,783.80 | 1.0 | |||
| Enzalutamide | EUR 274,394.96 | 1.0 | |||
| Trastuzumab s.c. | EUR 271,830.00 | 1.0 | |||
| Apalutamide | EUR 259,110.00 | 0.9 | |||
| Ipilimumab/placebo | EUR 222,314.53 | 0.8 | |||
| Trastuzumab | EUR 217,028.66 | 0.8 | |||
| Alectinib | EUR 204,001.91 | 0.7 | |||
| Panitumumab | EUR 183,674.66 | 0.7 | |||
| Nivolumab/placebo | EUR 183,520.80 | 0.7 | |||
| Niraparib | EUR 181,838.25 | 0.7 | |||
| Olaratumab/placebo | EUR 181,812.21 | 0.7 | |||
| Total | 90.6 | ||||
| 2010 | 2019 | ||||
|---|---|---|---|---|---|
| Tumor Location | % of Total Expenditure | % of Total Patients | Tumor Location | % of Total Expenditure | % of Total Patients |
| Breast | 46.4 | 34.8 | Lung, non-small cell | 27.0 | 17.5 |
| Colon | 18.0 | 19.1 | Advanced solid tumor | 10.1 | 20.2 |
| Ovary | 14.3 | 8.7 | Breast | 9.5 | 9.9 |
| Lung, non-small cell | 9.6 | 13.5 | Colon | 8.0 | 7.6 |
| Prostate | 5.8 | 3.0 | Ovary | 7.0 | 5.2 |
| Pancreas endocrine | 1.9 | 0.8 | Melanoma | 6.2 | 5.4 |
| Rectum | 1.5 | 3.2 | Kidney | 5.2 | 3.7 |
| Advanced solid tumors | 1.3 | 8.4 | Pancreas exocrine | 2.9 | 4.3 |
| Oral cavity and oropharynx | 0.4 | 1.6 | Uterine cervix | 2.7 | 3.4 |
| Stomach | 0.3 | 1.6 | Lung, small cell | 2.6 | 2.7 |
| Pancreas exocrine | 0.2 | 2.4 | Endometrium | 2.3 | 3.2 |
| Lung, small cell | 0.2 | 0.5 | Urinary bladder | 2.2 | 2.7 |
| Urinary bladder | 0.04 | 2.2 | Stomach | 2.2 | 3.1 |
| Kidney | 0.02 | 0.5 | Oral cavity and oropharynx | 2.1 | 2.2 |
| Soft tissue sarcoma | 0.01 | 0.3 | Mesothelioma | 1.7 | 1.5 |
| Endometrium | 0.01 | 0.8 | Esophagus | 1.5 | 1.1 |
| Extrahepatic bile duct | 0.0 | 0.3 | Soft tissue sarcoma | 1.4 | 1.0 |
| Rhinopharynx/cavum | 1.2 | 0.4 | |||
| Neuroendocrine | 0.7 | 1.4 | |||
| Hepatic carcinoma | 0.7 | 0.5 | |||
| Thymoma | 0.7 | 0.5 | |||
| Brain | 0.5 | 0.7 | |||
| Prostate | 0.5 | 1.0 | |||
| Squamous cell skin cancer | 0.4 | 0.3 | |||
| Larynx/hypopharynx | 0.3 | 0.09 | |||
| Rectum | 0.2 | 0.6 | |||
| Basal cell carcinoma | 0.2 | 0.2 | |||
| Merkel carcinoma | 0.07 | 0.2 | |||
| Extrahepatic bile duct | 0.02 | 1.1 | |||
| Urothelial cancer | 0.0 | 0.09 | |||
| Adrenal | 0.09 | ||||
| Anus | 0.4 | ||||
| Pancreas endocrine | 0.5 | ||||
| Thyroid | 0.3 | ||||
| Gallbladder | 0.09 | ||||
| Study Years | Expenditures on Antineoplastic Drugs | ||
|---|---|---|---|
| Intravenous | Oral | Total | |
| 2010 | EUR 1,650,750 | EUR 4,541,111 | EUR 6,191,865 |
| 2011 | EUR 1,205,680 | EUR 6,829,844 | EUR 8,035,524 |
| 2012 | EUR 1,322,395 | EUR 4,141,530 | EUR 5,463,925 |
| 2013 | EUR 2,349,744 | EUR 3,994,676 | EUR 6,344,420 |
| 2014 | EUR 2,157,533 | EUR 4,933,760 | EUR 7,091,293 |
| 2015 | EUR 3,034,919 | EUR 6,474,355 | EUR 9,509,274 |
| 2016 | EUR 4,087,619 | EUR 6,370,112 | EUR 10,457,731 |
| 2017 | EUR 4,722,001 | EUR 5,911,956 | EUR 10,633,957 |
| 2018 | EUR 7,266,822 | EUR 7,196,238 | EUR 14,463,060 |
| 2019 | EUR 6,666,428 | EUR 7,805,132 | EUR 14,471,560 |
| Total | EUR 34,463,891 | EUR 58,198,718 | EUR 92,662,609 |
| Study Years | Pharmaceutical Expenditure of Antineoplastic Agents | |||||
|---|---|---|---|---|---|---|
| Healthcare Setting | Clinical Trial Setting | Potential Drug Cost Avoidance | ||||
| Intravenous | Oral | Intravenous | Oral | Intravenous | Oral | |
| 2010 | EUR 6,565,263 | EUR 2,579,163 | EUR 2,457,850 | NR | EUR 1,650,750 | EUR 4,541,115 |
| 2011 | EUR 4,464,740 | EUR 3,271,684 | EUR 1,700,250 | NR | EUR 1,205,680 | EUR 6,829,844 |
| 2012 | EUR 4,695,722 | EUR 2,853,205 | EUR 2,203,633 | NR | EUR 1,322,395 | EUR 4,141,530 |
| 2013 | EUR 4,436,132 | EUR 2,437,685 | EUR 3,331,912 | EUR 1,845,309 | EUR 2,349,744 | EUR 3,994,676 |
| 2014 | EUR 5,770,959 | EUR 3,302,873 | EUR 4,636,490 | EUR 2,022,064 | EUR 2,157,533 | EUR 4,933,760 |
| 2015 | EUR 7,596,964 | EUR 4,346,928 | EUR 4,120,596 | EUR 2,876,494 | EUR 3,034,919 | EUR 6,474.355 |
| 2016 | EUR 9,769,375 | EUR 4,581,945 | EUR 6,220,320 | EUR 3,545,183 | EUR 4,087,619 | EUR 6,370,112 |
| 2017 | EUR 9,475,022 | EUR 4,990,955 | EUR 12,675,915 | EUR 6,086,139 | EUR 4,722,001 | EUR 5,911,956 |
| 2018 | EUR 11,252,776 | EUR 6,723,301 | EUR 17,844,749 | EUR 8,166,853 | EUR 7,266,822 | EUR 7,196,238 |
| 2019 | EUR 12,666,317 | EUR 8,615,087 | EUR 17,074,664 | EUR 10,497,663 | EUR 6,666,428 | EUR 7,805,132 |
| Total | EUR 76,693,270 | EUR 43,702,826 | EUR 72,266,379 | EUR 35,039,705 | EUR 34,463,891 | EUR 58,198,718 |
| Overall | EUR 120,396,096 | EUR 107,306,084 | EUR 92,662,609 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carreras, M.-J.; Renedo-Miró, B.; Valdivia, C.; Tomás-Guillén, E.; Farriols, A.; Mañós, L.; Vidal, J.; Alcalde, M.; De la Paz, I.; Jiménez-Lozano, I.; et al. Drug Cost Avoidance Resulting from Participation in Clinical Trials: A 10-Year Retrospective Analysis of Cancer Patients with Solid Tumors. Cancers 2024, 16, 1529. https://doi.org/10.3390/cancers16081529
Carreras M-J, Renedo-Miró B, Valdivia C, Tomás-Guillén E, Farriols A, Mañós L, Vidal J, Alcalde M, De la Paz I, Jiménez-Lozano I, et al. Drug Cost Avoidance Resulting from Participation in Clinical Trials: A 10-Year Retrospective Analysis of Cancer Patients with Solid Tumors. Cancers. 2024; 16(8):1529. https://doi.org/10.3390/cancers16081529
Chicago/Turabian StyleCarreras, Maria-Josep, Berta Renedo-Miró, Carolina Valdivia, Elena Tomás-Guillén, Anna Farriols, Laura Mañós, Jana Vidal, María Alcalde, Isabel De la Paz, Inés Jiménez-Lozano, and et al. 2024. "Drug Cost Avoidance Resulting from Participation in Clinical Trials: A 10-Year Retrospective Analysis of Cancer Patients with Solid Tumors" Cancers 16, no. 8: 1529. https://doi.org/10.3390/cancers16081529
APA StyleCarreras, M.-J., Renedo-Miró, B., Valdivia, C., Tomás-Guillén, E., Farriols, A., Mañós, L., Vidal, J., Alcalde, M., De la Paz, I., Jiménez-Lozano, I., Palacio-Lacambra, M.-E., Sabaté, N., Felip, E., Garralda, E., Garau, M., Gorgas, M.-Q., Monterde, J., & Tabernero, J. (2024). Drug Cost Avoidance Resulting from Participation in Clinical Trials: A 10-Year Retrospective Analysis of Cancer Patients with Solid Tumors. Cancers, 16(8), 1529. https://doi.org/10.3390/cancers16081529