
A Prospective Study on Deep Inspiration Breath Hold Thoracic Radiation Therapy Guided by Bronchoscopically Implanted Electromagnetic Transponders
 , , , , ,
, , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility
2.2. Procedures and Treatment
2.3. Follow-Up and Toxicity Assessment
2.4. Statistical Analysis
3. Results
3.1. Patients
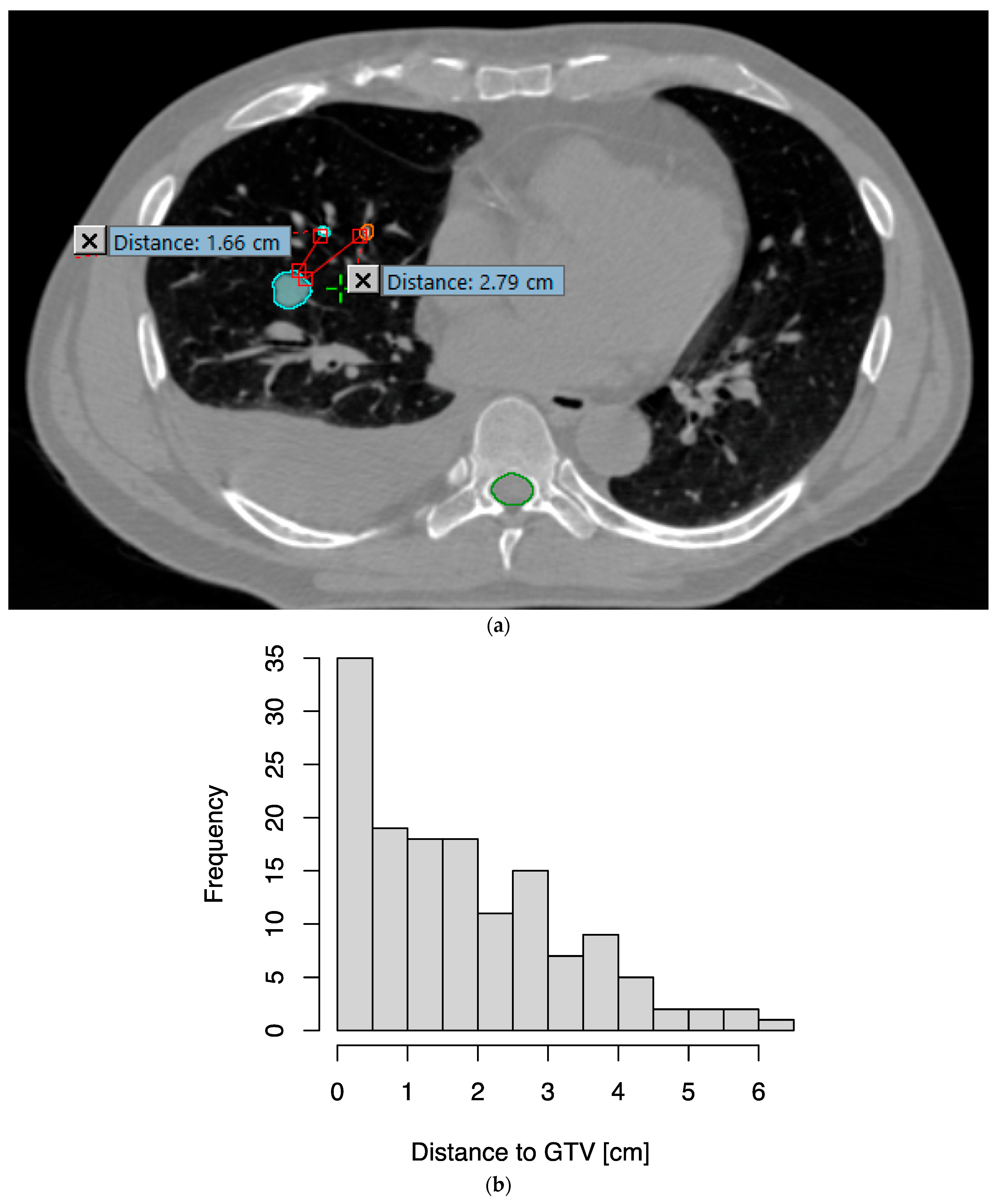
3.2. EMTs Were Implanted Close to the Tumor with Low Toxicity
3.3. Radiotherapy with EMT-Guided DIBH Was Feasible and Safe
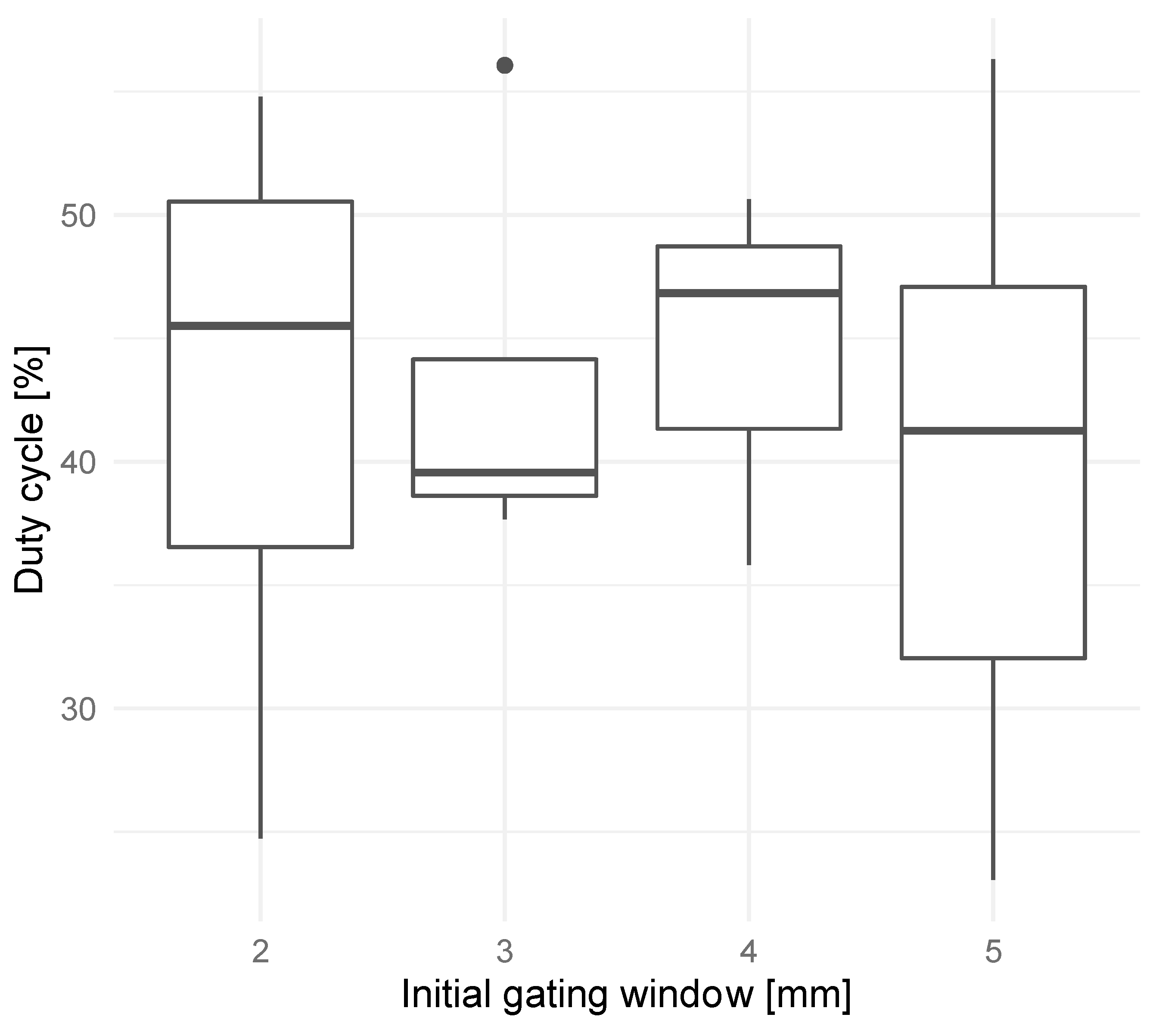
3.4. Gating Window Reduction
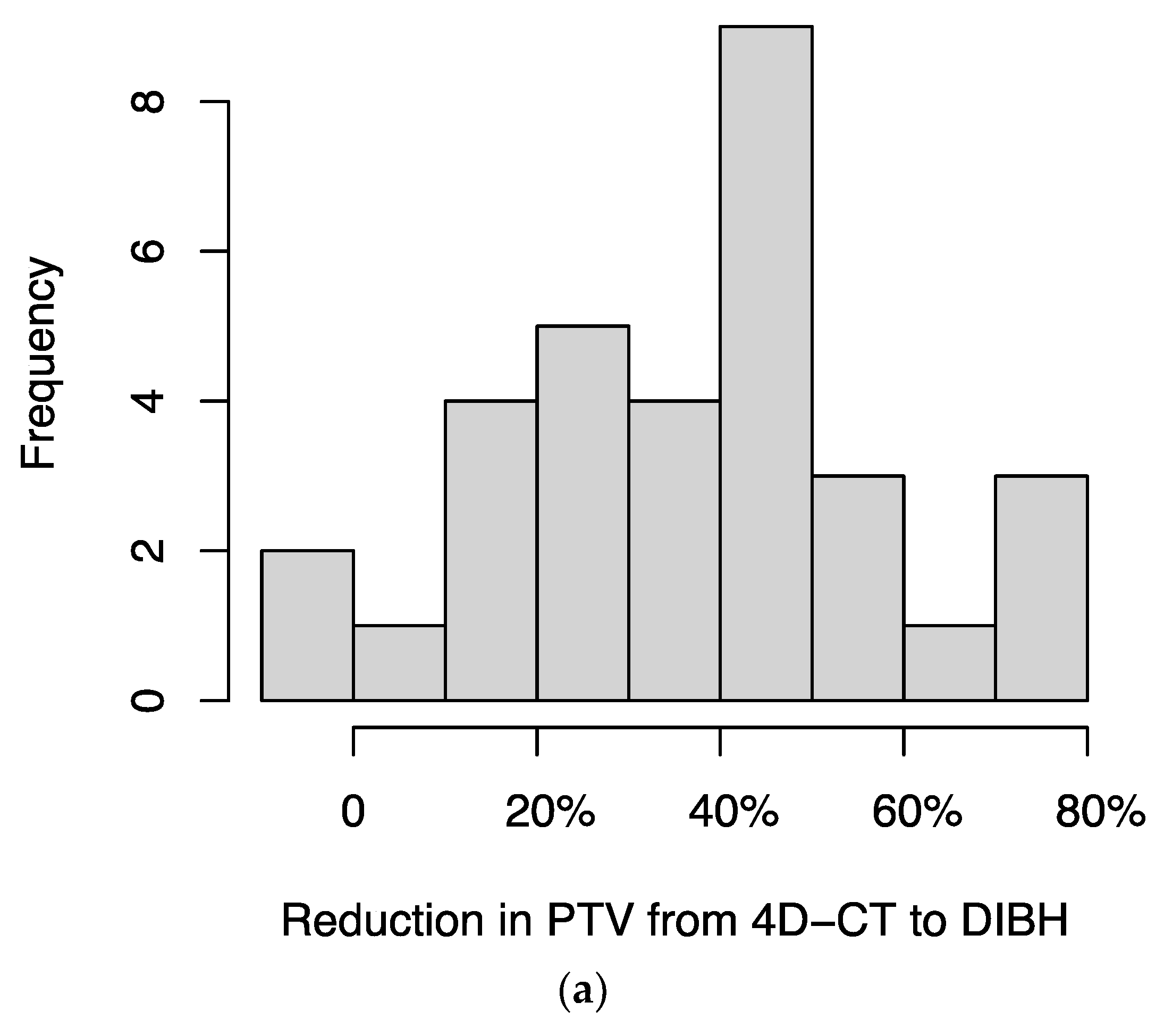
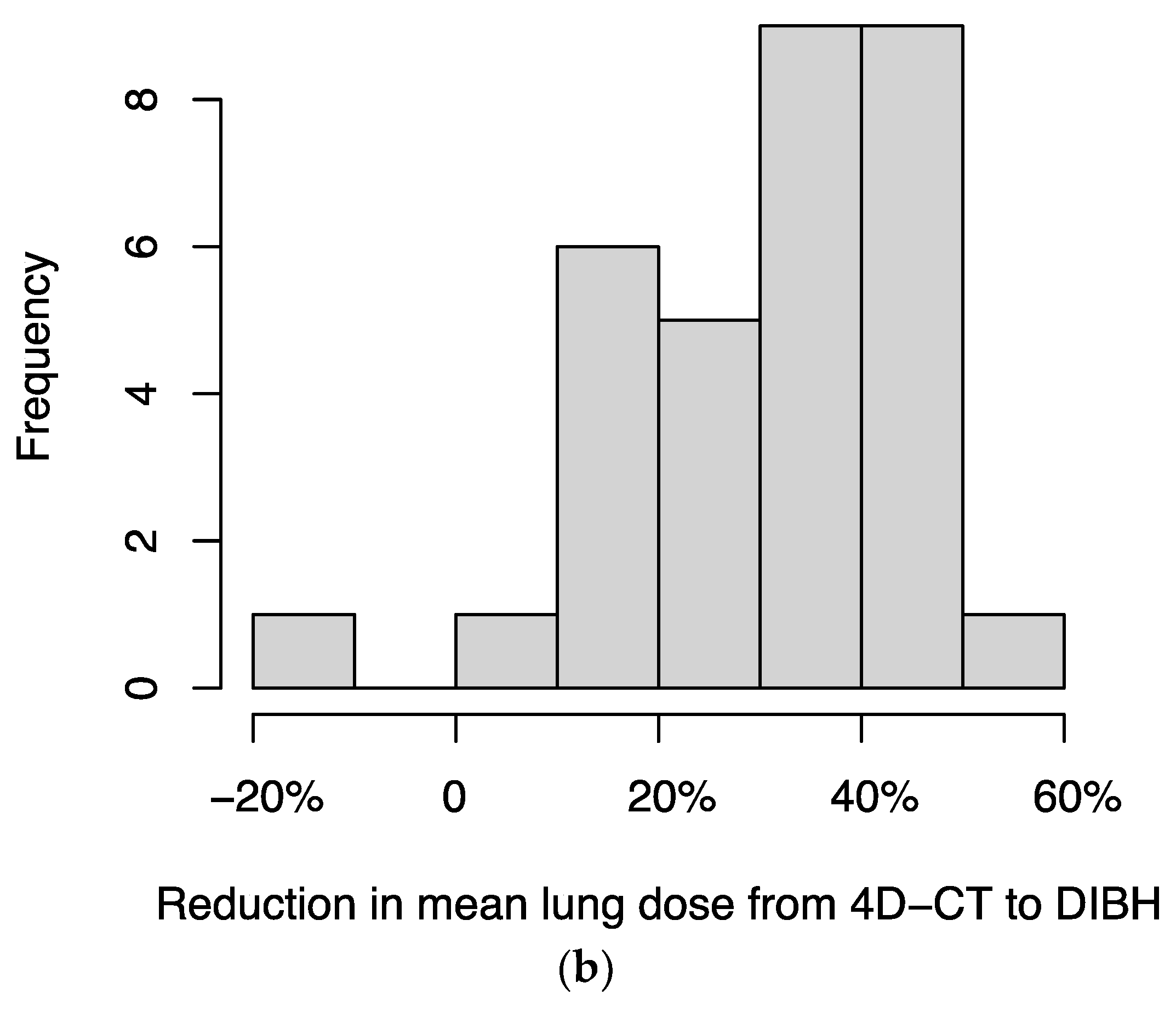
3.5. DIBH Reduced PTV and Lung Dose Compared to 4D-CT
3.6. Local Control
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Timmerman, R.; Paulus, R.; Galvin, J.; Michalski, J.; Straube, W.; Bradley, J.; Fakiris, A.; Bezjak, A.; Videtic, G.; Johnstone, D.; et al. Stereotactic Body Radiation Therapy for Inoperable Early Stage Lung Cancer. JAMA 2010, 303, 1070–1076. [Google Scholar] [CrossRef] [PubMed]
- Baumann, P.; Nyman, J.; Hoyer, M.; Wennberg, B.; Gagliardi, G.; Lax, I.; Drugge, N.; Ekberg, L.; Friesland, S.; Johansson, K.A.; et al. Outcome in a Prospective Phase II Trial of Medically Inoperable Stage I Non-Small-Cell Lung Cancer Patients Treated with Stereotactic Body Radiotherapy. J. Clin. Oncol. 2009, 27, 3290–3296. [Google Scholar] [CrossRef] [PubMed]
- Fakiris, A.J.; McGarry, R.C.; Yiannoutsos, C.T.; Papiez, L.; Williams, M.; Henderson, M.A.; Timmerman, R. Stereotactic Body Radiation Therapy for Early-Stage Non-Small-Cell Lung Carcinoma: Four-Year Results of a Prospective Phase II Study. Int. J. Radiat. Oncol. Biol. Phys. 2009, 75, 677–682. [Google Scholar] [CrossRef] [PubMed]
- Videtic, G.M.M.; Donington, J.; Giuliani, M.; Heinzerling, J.; Karas, T.Z.; Kelsey, C.R.; Lally, B.E.; Latzka, K.; Lo, S.S.; Moghanaki, D.; et al. Stereotactic Body Radiation Therapy for Early-Stage Non-Small Cell Lung Cancer: Executive Summary of an ASTRO Evidence-Based Guideline. Pract. Radiat. Oncol. 2017, 7, 295–301. [Google Scholar] [CrossRef] [PubMed]
- von Reibnitz, D.; Shaikh, F.; Wu, A.J.; Treharne, G.C.; Dick-Godfrey, R.; Foster, A.; Woo, K.M.; Shi, W.; Zhang, Z.; Din, S.U.; et al. Stereotactic Body Radiation Therapy (SBRT) Improves Local Control and Overall Survival Compared to Conventionally Fractionated Radiation for Stage I Non-Small Cell Lung Cancer (NSCLC). Acta Oncol. 2018, 57, 1567–1573. [Google Scholar] [CrossRef] [PubMed]
- Rusthoven, K.E.; Kavanagh, B.D.; Burri, S.H.; Chen, C.; Cardenes, H.; Chidel, M.A.; Pugh, T.J.; Kane, M.; Gaspar, L.E.; Schefter, T.E. Multi-Institutional Phase I/II Trial of Stereotactic Body Radiation Therapy for Lung Metastases. J. Clin. Oncol. 2009, 27, 1579–1584. [Google Scholar] [CrossRef]
- Dhakal, S.; Corbin, K.S.; Milano, M.T.; Philip, A.; Sahasrabudhe, D.; Jones, C.; Constine, L.S. Stereotactic Body Radiotherapy for Pulmonary Metastases from Soft-Tissue Sarcomas: Excellent Local Lesion Control and Improved Patient Survival. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, 940–945. [Google Scholar] [CrossRef]
- Milano, M.T.; Katz, A.W.; Zhang, H.; Okunieff, P. Oligometastases Treated with Stereotactic Body Radiotherapy: Long-Term Follow-up of Prospective Study. Int. J. Radiat. Oncol. Biol. Phys. 2012, 83, 878–886. [Google Scholar] [CrossRef]
- Ricardi, U.; Filippi, A.R.; Guarneri, A.; Ragona, R.; Mantovani, C.; Giglioli, F.; Botticella, A.; Ciammella, P.; Iftode, C.; Buffoni, L.; et al. Stereotactic Body Radiation Therapy for Lung Metastases. Lung Cancer 2012, 75, 77–81. [Google Scholar] [CrossRef]
- Lebow, E.S.; Lobaugh, S.M.; Zhang, Z.; Dickson, M.A.; Rosenbaum, E.; D’Angelo, S.P.; Nacev, B.A.; Shepherd, A.F.; Shaverdian, N.; Wolden, S.; et al. Stereotactic Body Radiation Therapy for Sarcoma Pulmonary Metastases. Radiother. Oncol. 2023, 187, 109824. [Google Scholar] [CrossRef]
- Curran, W.J.; Paulus, R.; Langer, C.J.; Komaki, R.; Lee, J.S.; Hauser, S.; Movsas, B.; Wasserman, T.; Rosenthal, S.A.; Gore, E.; et al. Sequential vs. Concurrent Chemoradiation for Stage III Non-Small Cell Lung Cancer: Randomized Phase III Trial RTOG 9410. J. Natl. Cancer Inst. 2011, 103, 1452–1460. [Google Scholar] [CrossRef] [PubMed]
- Aupérin, A.; Le Péchoux, C.; Rolland, E.; Curran, W.J.; Furuse, K.; Fournel, P.; Belderbos, J.; Clamon, G.; Ulutin, H.C.; Paulus, R.; et al. Meta-Analysis of Concomitant versus Sequential Radiochemotherapy in Locally Advanced Non-Small-Cell Lung Cancer. J. Clin. Oncol. 2010, 28, 2181–2190. [Google Scholar] [CrossRef] [PubMed]
- Daly, M.E.; Singh, N.; Ismaila, N.; Antonoff, M.B.; Arenberg, D.A.; Bradley, J.; David, E.; Detterbeck, F.; Früh, M.; Gubens, M.A.; et al. Management of Stage III Non-Small-Cell Lung Cancer: ASCO Guideline. J. Clin. Oncol. 2022, 40, 1356–1384. [Google Scholar] [CrossRef] [PubMed]
- McGarry, R.C.; Papiez, L.; Williams, M.; Whitford, T.; Timmerman, R.D. Stereotactic Body Radiation Therapy of Early-Stage Non-Small-Cell Lung Carcinoma: Phase I Study. Int. J. Radiat. Oncol. Biol. Phys. 2005, 63, 1010–1015. [Google Scholar] [CrossRef] [PubMed]
- Timmerman, R.; McGarry, R.; Yiannoutsos, C.; Papiez, L.; Tudor, K.; DeLuca, J.; Ewing, M.; Abdulrahman, R.; DesRosiers, C.; Williams, M.; et al. Excessive Toxicity When Treating Central Tumors in a Phase II Study of Stereotactic Body Radiation Therapy for Medically Inoperable Early-Stage Lung Cancer. J. Clin. Oncol. 2006, 24, 4833–4839. [Google Scholar] [CrossRef]
- Ong, C.L.; Palma, D.; Verbakel, W.F.A.R.; Slotman, B.J.; Senan, S. Treatment of Large Stage I-II Lung Tumors Using Stereotactic Body Radiotherapy (SBRT): Planning Considerations and Early Toxicity. Radiother. Oncol. 2010, 97, 431–436. [Google Scholar] [CrossRef] [PubMed]
- Yorke, E.D.; Thor, M.; Gelblum, D.Y.; Gomez, D.R.; Rimner, A.; Shaverdian, N.; Shepherd, A.F.; Simone, C.B.; Wu, A.; McKnight, D.; et al. Treatment Planning and Outcomes Effects of Reducing the Preferred Mean Esophagus Dose for Conventionally Fractionated Non-small Cell Lung Cancer Radiotherapy. J. Appl. Clin. Med. Phys. 2021, 22, 42. [Google Scholar] [CrossRef] [PubMed]
- Marks, L.B.; Bentzen, S.M.; Deasy, J.O.; Kong, F.M.; Bradley, J.D.; Vogelius, I.S.; El Naqa, I.; Hubbs, J.L.; Lebesque, J.V.; Timmerman, R.D.; et al. Radiation Dose Volume Effects in the Lung. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, S70. [Google Scholar] [CrossRef]
- Kong, F.M.; Moiseenko, V.; Zhao, J.; Milano, M.T.; Li, L.; Rimner, A.; Das, S.; Li, X.A.; Miften, M.; Liao, Z.X.; et al. Organs at Risk Considerations for Thoracic Stereotactic Body Radiation Therapy: What Is Safe for Lung Parenchyma? Int. J. Radiat. Oncol. Biol. Phys. 2021, 110, 172–187. [Google Scholar] [CrossRef] [PubMed]
- Giraud, P.; Morvan, E.; Claude, L.; Mornex, F.; Le Pechoux, C.; Bachaud, J.M.; Boisselier, P.; Beckendorf, V.; Morelle, M.; Carrère, M.O. Respiratory Gating Techniques for Optimization of Lung Cancer Radiotherapy. J. Thorac. Oncol. 2011, 6, 2058–2068. [Google Scholar] [CrossRef]
- Papachristofilou, A.; Petermann, H.; Gross, M.; Schratzenstaller, U.; Parikh, P.J.; Paris, G.; Bolliger, C.T.; Weihann, K.; Macgregor, H.; Zimmerman, F. Real-Time Electromagnetic Localization and Tracking of Human Lung Cancer Using Internal Fiducials During Radiation Therapy: Implications for Target Planning and Treatment Delivery. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, S762–S763. [Google Scholar] [CrossRef]
- Bouilhol, G.; Ayadi, M.; Rit, S.; Thengumpallil, S.; Schaerer, J.; Vandemeulebroucke, J.; Claude, L.; Sarrut, D. Is Abdominal Compression Useful in Lung Stereotactic Body Radiation Therapy? A 4DCT and Dosimetric Lobe-Dependent Study. Phys. Med. 2013, 29, 333–340. [Google Scholar] [CrossRef] [PubMed]
- Hunjan, S.; Starkschall, G.; Prado, K.; Dong, L.; Balter, P. Lack of Correlation between External Fiducial Positions and Internal Tumor Positions during Breath-Hold CT. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, 1586–1591. [Google Scholar] [CrossRef]
- Li, R.; Mok, E.; Han, B.; Koong, A.; Xing, L. Evaluation of the Geometric Accuracy of Surrogate-Based Gated VMAT Using Intrafraction Kilovoltage X-ray Images. Med. Phys. 2012, 39, 2686–2693. [Google Scholar] [CrossRef] [PubMed]
- Wong, J.W.; Sharpe, M.B.; Jaffray, D.A.; Kini, V.R.; Robertson, J.M.; Stromberg, J.S.; Martinez, A.A. The Use of Active Breathing Control (ABC) to Reduce Margin for Breathing Motion. Int. J. Radiat. Oncol. Biol. Phys. 1999, 44, 911–919. [Google Scholar] [CrossRef] [PubMed]
- Dawson, L.A.; Brock, K.K.; Kazanjian, S.; Fitch, D.; McGinn, C.J.; Lawrence, T.S.; Ten Haken, R.K.; Balter, J. The Reproducibility of Organ Position Using Active Breathing Control (ABC) during Liver Radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2001, 51, 1410–1421. [Google Scholar] [CrossRef] [PubMed]
- Hanley, J.; Debois, M.M.; Mah, D.; Mageras, G.S.; Raben, A.; Rosenzweig, K.; Mychalczak, B.; Schwartz, L.H.; Gloeggler, P.J.; Lutz, W.; et al. Deep Inspiration Breath-Hold Technique for Lung Tumors: The Potential Value of Target Immobilization and Reduced Lung Density in Dose Escalation. Int. J. Radiat. Oncol. Biol. Phys. 1999, 45, 603–611. [Google Scholar] [CrossRef] [PubMed]
- Rosenzweig, K.E.; Hanley, J.; Mah, D.; Mageras, G.; Hunt, M.; Toner, S.; Burman, C.; Ling, C.C.; Mychalczak, B.; Fuks, Z.; et al. The Deep Inspiration Breath-Hold Technique in the Treatment of Inoperable Non-Small-Cell Lung Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2000, 48, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Barnes, E.A.; Murray, B.R.; Robinson, D.M.; Underwood, L.J.; Hanson, J.; Roa, W.H.Y. Dosimetric Evaluation of Lung Tumor Immobilization Using Breath Hold at Deep Inspiration. Int. J. Radiat. Oncol. Biol. Phys. 2001, 50, 1091–1098. [Google Scholar] [CrossRef]
- Mah, D.; Hanley, J.; Rosenzweig, K.E.; Yorke, E.; Braban, L.; Ling, C.C.; Leibel, S.A.; Mageras, G. Technical Aspects of the Deep Inspiration Breath-Hold Technique in the Treatment of Thoracic Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2000, 48, 1175–1185. [Google Scholar] [CrossRef]
- Muralidhar, K.R.; Komanduri, K.; Rout, B.K.; Ramesh, K.K.D. Commissioning and Quality Assurance of Calypso Four-Dimensional Target Localization System in Linear Accelerator Facility. J. Med. Phys. Assoc. Med. Phys. India 2013, 38, 143. [Google Scholar] [CrossRef] [PubMed]
- Tanyi, J.A.; He, T.; Summers, P.A.; Mburu, R.G.; Kato, C.M.; Rhodes, S.M.; Hung, A.Y.; Fuss, M. Assessment of Planning Target Volume Margins for Intensity-Modulated Radiotherapy of the Prostate Gland: Role of Daily Inter- and Intrafraction Motion. Int. J. Radiat. Oncol. Biol. Phys. 2010, 78, 1579–1585. [Google Scholar] [CrossRef] [PubMed]
- Shinohara, E.T.; Kassaee, A.; Mitra, N.; Vapiwala, N.; Plastaras, J.P.; Drebin, J.; Wan, F.; Metz, J.M. Feasibility of Electromagnetic Transponder Use to Monitor Inter- and Intrafractional Motion in Locally Advanced Pancreatic Cancer Patients. Int. J. Radiat. Oncol. Biol. Phys. 2012, 83, 566–573. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.P.; Kupelian, P.A.; Waghorn, B.J.; Willoughby, T.R.; Rineer, J.M.; Mañon, R.R.; Vollenweider, M.A.; Meeks, S.L. Real-Time Tumor Tracking in the Lung Using an Electromagnetic Tracking System. Int. J. Radiat. Oncol. Biol. Phys. 2013, 86, 477–483. [Google Scholar] [CrossRef] [PubMed]
- McDonald, A.M.; Colvin, T.; Boggs, D.H.; Spencer, S.A.; Popple, R.A.; Clayton, R.; Minnich, D.; Dobelbower, M.C. Longitudinal Assessment of Anchored Transponder Migration Following Lung Stereotactic Body Radiation Therapy. J. Appl. Clin. Med. Phys. 2019, 20, 17. [Google Scholar] [CrossRef] [PubMed]
- Mayse, M.L.; Smith, R.L.; Park, M.; Monteon, G.H.; Silver, E.H.; Parikh, P.J.; Misselhorn, D.L.; Talcott, M.R.; Dimmer, S.; Bradley, J.D. Development of a Non-Migrating Electromagnetic Transponder System for Lung Tumor Tracking. Int. J. Radiat. Oncol. Biol. Phys. 2008, 72, S430. [Google Scholar] [CrossRef]
- Jaccard, M.; Champion, A.; Dubouloz, A.; Picardi, C.; Plojoux, J.; Soccal, P.; Miralbell, R.; Dipasquale, G.; Caparrotti, F. Clinical Experience with Lung-Specific Electromagnetic Transponders for Real-Time Tumor Tracking in Lung Stereotactic Body Radiotherapy. Phys. Imaging Radiat. Oncol. 2019, 12, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Boggs, D.H.; Popple, R.; McDonald, A.; Minnich, D.; Willey, C.D.; Spencer, S.; Shen, S.; Dobelbower, M.C. Electromagnetic Transponder Based Tracking and Gating in the Radiotherapeutic Treatment of Thoracic Malignancies. Pract. Radiat. Oncol. 2019, 9, 456–464. [Google Scholar] [CrossRef] [PubMed]
- Dobelbower, M.C.; Popple, R.A.; Minnich, D.J.; Nader, D.A.; Zimmerman, F.; Paris, G.E.; Herth, F.J.F.; Gompelmann, D.; Roeder, F.F.; Parikh, P.J.; et al. Anchored Transponder Guided Lung Radiation Therapy. Pract. Radiat. Oncol. 2020, 10, e37–e44. [Google Scholar] [CrossRef]
- Harris, W.; Yorke, E.; Li, H.; Czmielewski, C.; Chawla, M.; Lee, R.P.; Hotca-Cho, A.; McKnight, D.; Rimner, A.; Lovelock, D.M. Can Bronchoscopically Implanted Anchored Electromagnetic Transponders Be Used to Monitor Tumor Position and Lung Inflation during Deep Inspiration Breath-Hold Lung Radiotherapy? Med. Phys. 2022, 49, 2621–2630. [Google Scholar] [CrossRef]
- Balter, J.M.; Wright, J.N.; Newell, L.J.; Friemel, B.; Dimmer, S.; Cheng, Y.; Wong, J.; Vertatschitsch, E.; Mate, T.P. Accuracy of a Wireless Localization System for Radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2005, 61, 933–937. [Google Scholar] [CrossRef] [PubMed]
- Willoughby, T.R.; Kupelian, P.A.; Pouliot, J.; Shinohara, K.; Aubin, M.; Roach, M.; Skrumeda, L.L.; Balter, J.M.; Litzenberg, D.W.; Hadley, S.W.; et al. Target Localization and Real-Time Tracking Using the Calypso 4D Localization System in Patients with Localized Prostate Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2006, 65, 528–534. [Google Scholar] [CrossRef]
- Santanam, L.; Noel, C.; Willoughby, T.R.; Esthappan, J.; Mutic, S.; Klein, E.E.; Low, D.A.; Parikh, P.J. Quality Assurance for Clinical Implementation of an Electromagnetic Tracking System. Med. Phys. 2009, 36, 3477–3486. [Google Scholar] [CrossRef] [PubMed]
- Santanam, L.; Malinowski, K.; Hubenshmidt, J.; Dimmer, S.; Mayse, M.L.; Bradley, J.; Chaudhari, A.; Lechleiter, K.; Goddu, S.K.M.; Esthappan, J.; et al. Fiducial-Based Translational Localization Accuracy of Electromagnetic Tracking System and on-Board Kilovoltage Imaging System. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 892–899. [Google Scholar] [CrossRef]
- Su, Z.; Zhang, L.; Murphy, M.; Williamson, J. An Analysis of Prostate Patient Setup and Tracking Data: Potential Intervention Strategies. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, 880. [Google Scholar] [CrossRef]
- Chaurasia, A.R.; Sun, K.J.; Premo, C.; Brand, T.; Tinnel, B.; Barczak, S.; Halligan, J.; Brown, M.; Macdonald, D. Evaluating the Potential Benefit of Reduced Planning Target Volume Margins for Low and Intermediate Risk Patients with Prostate Cancer Using Real-Time Electromagnetic Tracking. Adv. Radiat. Oncol. 2018, 3, 630. [Google Scholar] [CrossRef] [PubMed]
- Mu, Z.; Wang, Q.; Guo, C.; Feng, Y.; Gu, H.; Zhai, Z.; Wu, J.; He, X. The First Internal Electromagnetic Motion Monitoring Implementation for Stereotactic Liver Radiotherapy in China: Procedures and Preliminary Results. J. Cancer Res. Clin. Oncol. 2022, 148, 1429–1436. [Google Scholar] [CrossRef]
- Worm, E.S.; Høyer, M.; Hansen, R.; Larsen, L.P.; Weber, B.; Grau, C.; Poulsen, P.R. A Prospective Cohort Study of Gated Stereotactic Liver Radiation Therapy Using Continuous Internal Electromagnetic Motion Monitoring. Int. J. Radiat. Oncol. Biol. Phys. 2018, 101, 366–375. [Google Scholar] [CrossRef]
- Kaučić, H.; Kosmina, D.; Schwarz, D.; Mack, A.; Šobat, H.; Čehobašić, A.; Leipold, V.; Andrašek, I.; Avdičević, A.; Mlinarić, M. Stereotactic Ablative Radiotherapy Using CALYPSO® Extracranial Tracking for Intrafractional Tumor Motion Management—A New Potential Local Treatment for Unresectable Locally Advanced Pancreatic Cancer? Results from a Retrospective Study. Cancers 2022, 14, 2688. [Google Scholar] [CrossRef]
- Willmann, J.; Sidiqi, B.; Wang, C.; Czmielewski, C.; Li, H.J.; Dick-Godfrey, R.; Chawla, M.; Lee, R.P.; Gelb, E.; Wu, A.J.; et al. Four-Dimensional Computed Tomography-Based Correlation of Respiratory Motion of Lung Tumors with Implanted Fiducials and an External Surrogate. Adv. Radiat. Oncol. 2021, 7, 100885. [Google Scholar] [CrossRef]
- Shirato, H.; Suzuki, K.; Sharp, G.C.; Fujita, K.; Onimaru, R.; Fujino, M.; Kato, N.; Osaka, Y.; Kinoshita, R.; Taguchi, H.; et al. Speed and Amplitude of Lung Tumor Motion Precisely Detected in Four-Dimensional Setup and in Real-Time Tumor-Tracking Radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2006, 64, 1229–1236. [Google Scholar] [CrossRef] [PubMed]
- Booth, J.; Caillet, V.; Briggs, A.; Hardcastle, N.; Angelis, G.; Jayamanne, D.; Shepherd, M.; Podreka, A.; Szymura, K.; Nguyen, D.T.; et al. MLC Tracking for Lung SABR Is Feasible, Efficient and Delivers High-Precision Target Dose and Lower Normal Tissue Dose. Radiother. Oncol. 2021, 155, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Sarkar, V.; Szegedi, M.; Paxton, A.; Nelson, G.; Rassiah-Szegedi, P.; Reddy, C.B.; Tao, R.; Hitchcock, Y.J.; Kokeny, K.E.; Salter, B.J. Erratum: Preliminary Clinical Experience with Calypso Anchored Beacons for Tumor Tracking in Lung SBRT (Medical Physics, (2020), 47, 9, (4407-4415), 10.1002/Mp.14300). Med. Phys. 2021, 48, 533. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.C.; Buduhan, G.; Venkataraman, S.; Tan, L.; Sasaki, D.; Bashir, B.; Ahmed, N.; Kidane, B.; Sivananthan, G.; Koul, R.; et al. Endobronchially Implanted Real-Time Electromagnetic Transponder Beacon–Guided, Respiratory-Gated SABR for Moving Lung Tumors: A Prospective Phase 1/2 Cohort Study. Adv. Radiat. Oncol. 2023, 8, 101243. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, D.; Nill, S.; Roeder, F.; Gompelmann, D.; Herth, F.; Oelfke, U. Motion Monitoring during a Course of Lung Radiotherapy with Anchored Electromagnetic Transponders: Quantification of Inter- and Intrafraction Motion and Variability of Relative Transponder Positions. Strahlenther. Onkol. 2017, 193, 840. [Google Scholar] [CrossRef] [PubMed]
- Berbeco, R.I.; Nishioka, S.; Shirato, H.; Chen, G.T.Y.; Jiang, S.B. Residual Motion of Lung Tumours in Gated Radiotherapy with External Respiratory Surrogates. Phys. Med. Biol. 2005, 50, 3655–3667. [Google Scholar] [CrossRef] [PubMed]
- Koch, N.; Liu, H.H.; Starkschall, G.; Jacobson, M.; Forster, K.; Liao, Z.; Komaki, R.; Stevens, C.W. Evaluation of Internal Lung Motion for Respiratory-Gated Radiotherapy Using MRI: Part I—Correlating Internal Lung Motion with Skin Fiducial Motion. Int. J. Radiat. Oncol. Biol. Phys. 2004, 60, 1459–1472. [Google Scholar] [CrossRef] [PubMed]
- Nabavizadeh, N.; Zhang, J.; Elliott, D.A.; Tanyi, J.A.; Thomas, C.R.; Fuss, M.; Deffebach, M. Electromagnetic Navigational Bronchoscopy-Guided Fiducial Markers for Lung Stereotactic Body Radiation Therapy: Analysis of Safety, Feasibility, and Interfraction Stability. J. Bronchol. Interv. Pulmonol. 2014, 21, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Godley, A.; Zheng, D.; Rong, Y. MR-linac Is the Best Modality for Lung SBRT. J. Appl. Clin. Med. Phys. 2019, 20, 7. [Google Scholar] [CrossRef]
- Menten, M.J.; Fast, M.F.; Nill, S.; Kamerling, C.P.; McDonald, F.; Oelfke, U. Lung Stereotactic Body Radiotherapy with an MR-Linac—Quantifying the Impact of the Magnetic Field and Real-Time Tumor Tracking. Radiother. Oncol. 2016, 119, 461. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | n = 48 |
|---|---|
| Age—Median (IQR) | 69 (60, 73) |
| Sex—n (%) | |
| F | 27 (56%) |
| M | 21 (44%) |
| Disease type—n (%) | |
| Lung primary | 35 (73%) |
| Lung metastasis | 13 (27%) |
| Stage—n (%) | |
| I | 15 (31%) |
| II | 2 (4.2%) |
| III | 6 (13%) |
| IV | 22 (46%) |
| Local recurrence | 3 (6.3%) |
| RT type—n (%) | |
| Stereotactic body RT | 37 (77%) |
| Hypofractionated RT (8 or 15 fractions) | 4 (8.3%) |
| Conventionally fractionated RT | 7 (15%) |
| Treatment position—n (%) | |
| Supine | 40 (83%) |
| Prone | 6 (13%) |
| Not feasible | 2 (4.2%) |
| Toxicities Related to Transponder Implantation | |||
|---|---|---|---|
| Grade | 2 | 3 | 4 |
| Pneumothorax | 0 | 0 | 0 |
| Pneumonia | 0 | 0 | 1 |
| Supraventricular tachycardia | 0 | 1 | 0 |
| Total | 0 | 1 | 1 |
| Toxicities Related to Presence of Transponders | |||
| Grade | 2 | 3 | 4 |
| Cough | 5 | 1 | 0 |
| Dyspnea | 0 | 1 | 0 |
| Pneumonia | 0 | 2 | 0 |
| Pulmonary hemorrhage or hemoptysis | 1 | 0 | 0 |
| Total | 6 (6 pts) | 4 (2 pts) | 0 |
| Toxicities Related to RT | |||
| Grade | 2 | 3 | 4 |
| Cough | 11 | 1 | 0 |
| Dyspnea | 2 | 1 | 0 |
| Pneumonitis | 6 | 1 | 0 |
| Pneumonia | 0 | 2 | 0 |
| Chest wall pain | 1 | 0 | 0 |
| Dysphagia | 4 | 1 | 0 |
| Nausea | 1 | 0 | 0 |
| Vomiting | 1 | 0 | 0 |
| Anorexia | 2 | 0 | 0 |
| Dehydration | 1 | 1 | 0 |
| Fatigue | 9 | 0 | 0 |
| Dermatitis | 2 | 0 | 0 |
| Pulmonary hemorrhage or hemoptysis | 1 | 0 | 0 |
| Total | 41 (18 pts) | 7 (4 pts) | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meng, Y.J.; Mankuzhy, N.P.; Chawla, M.; Lee, R.P.; Yorke, E.D.; Zhang, Z.; Gelb, E.; Lim, S.B.; Cuaron, J.J.; Wu, A.J.; et al. A Prospective Study on Deep Inspiration Breath Hold Thoracic Radiation Therapy Guided by Bronchoscopically Implanted Electromagnetic Transponders. Cancers 2024, 16, 1534. https://doi.org/10.3390/cancers16081534
Meng YJ, Mankuzhy NP, Chawla M, Lee RP, Yorke ED, Zhang Z, Gelb E, Lim SB, Cuaron JJ, Wu AJ, et al. A Prospective Study on Deep Inspiration Breath Hold Thoracic Radiation Therapy Guided by Bronchoscopically Implanted Electromagnetic Transponders. Cancers. 2024; 16(8):1534. https://doi.org/10.3390/cancers16081534
Chicago/Turabian StyleMeng, Yuzhong Jeff, Nikhil P. Mankuzhy, Mohit Chawla, Robert P. Lee, Ellen D. Yorke, Zhigang Zhang, Emily Gelb, Seng Boh Lim, John J. Cuaron, Abraham J. Wu, and et al. 2024. "A Prospective Study on Deep Inspiration Breath Hold Thoracic Radiation Therapy Guided by Bronchoscopically Implanted Electromagnetic Transponders" Cancers 16, no. 8: 1534. https://doi.org/10.3390/cancers16081534