
The Vanishing Clinical Value of PD-L1 Status as a Predictive Biomarker in the First-Line Treatment of Urothelial Carcinoma of the Bladder

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
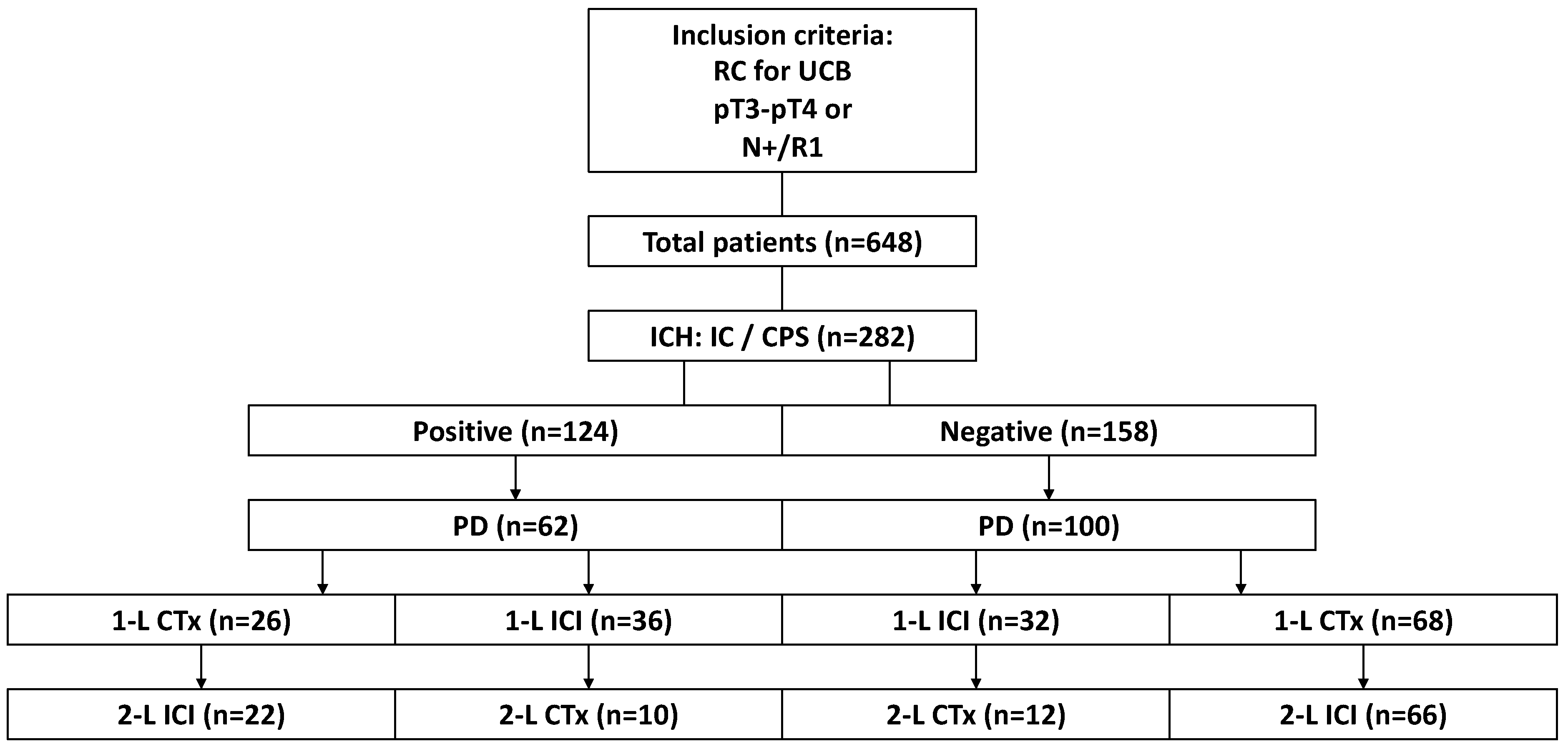
2.1. Clinical Cohort
2.2. Immunohistochemistry and Scoring of Protein Expression
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. TEAE
3.3. PFS
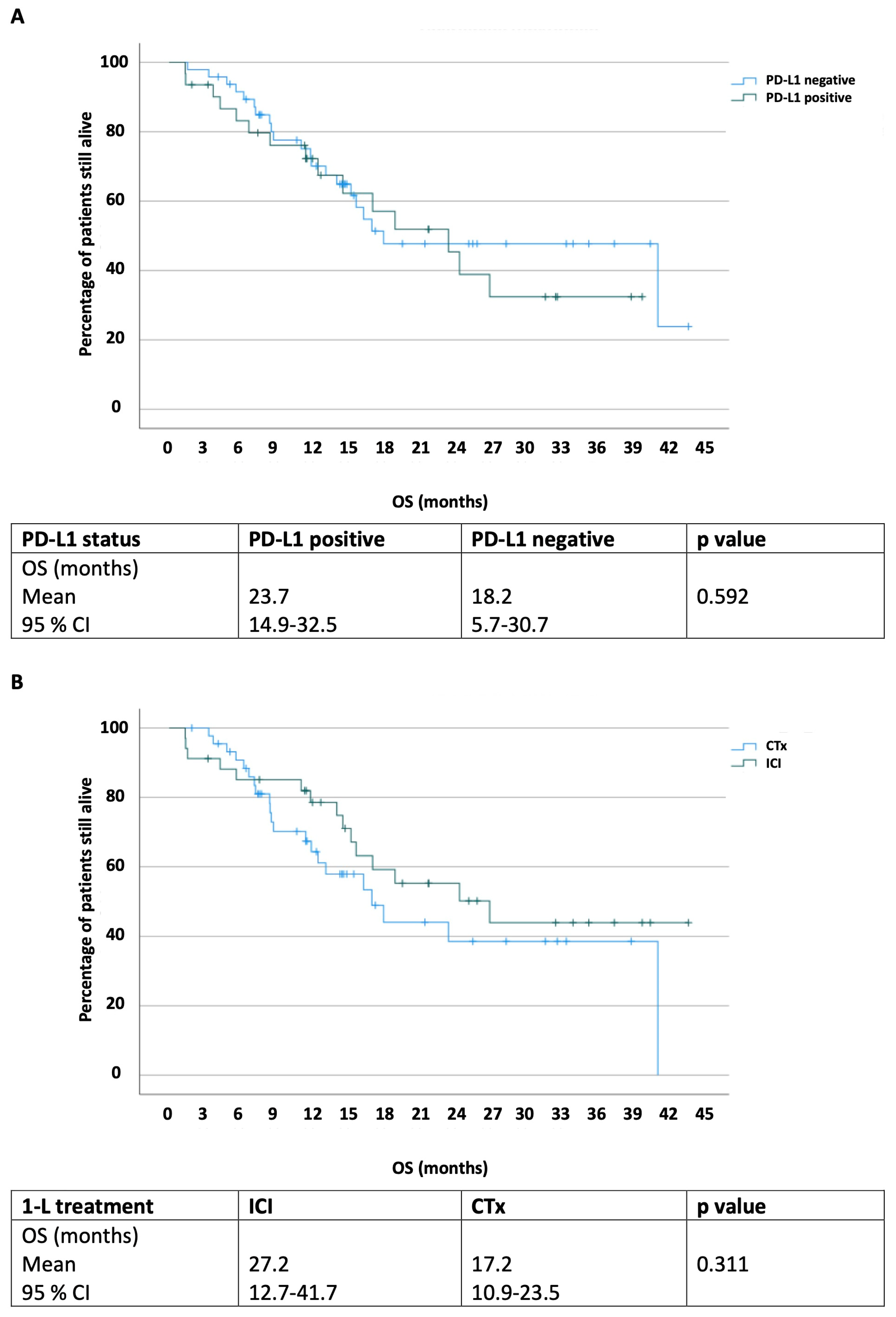
3.4. OS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Cancer Society. Key Statistics for Bladder Cancer. 2020. Available online: https://cancerstatisticscenter.cancer.org (accessed on 14 May 2022).
- Charlton, M.E.; Adamo, M.; Sun, L.; Deorah, S. Bladder cancer collaborative stage variables and their data quality, usage, and clinical implications: A review of SEER data, 2004–2010. Cancer 2014, 120 (Suppl. 23), 3815–3825. [Google Scholar] [CrossRef] [PubMed]
- Burger, M.; Catto, J.W.; Dalbagni, G.; Grossman, H.B.; Herr, H.; Karakiewicz, P.; Lotan, Y. Epidemiology and risk factors of urothelial bladder cancer. Eur. Urol. 2013, 63, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.B.; Deal, A.M.; Woods, M.E.; Wallen, E.M.; Pruthi, R.S.; Chen, R.C.; Nielsen, M.E. Muscle-invasive bladder cancer: Evaluating treatment and survival in the National Cancer Data Base. BJU Int. 2014, 114, 719–726. [Google Scholar] [CrossRef] [PubMed]
- Witjes, J.A.; Bruins, H.M.; Cathomas, R.; Comperat, E.M.; Cowan, N.C.; Gakis, G.; Hernandez, V.; Linares Espinos, E.; Lorch, A.; Neuzillet, Y.; et al. European Association of Urology Guidelines on Muscle-invasive and Metastatic Bladder Cancer: Summary of the 2020 Guidelines. Eur. Urol. 2021, 79, 82–104. [Google Scholar] [CrossRef] [PubMed]
- Tamalunas, A.; Volz, Y.; Schlenker, B.A.; Buchner, A.; Kretschmer, A.; Jokisch, F.; Rodler, S.; Schulz, G.; Eismann, L.; Pfitzinger, P.; et al. Is It Safe to Offer Radical Cystectomy to Patients above 85 Years of Age? A Long-Term Follow-Up in a Single-Center Institution. Urol. Int. 2020, 104, 975–981. [Google Scholar] [CrossRef] [PubMed]
- Stein, J.P.; Lieskovsky, G.; Cote, R.; Groshen, S.; Feng, A.C.; Boyd, S.; Skinner, E.; Bochner, B.; Thangathurai, D.; Mikhail, M.; et al. Radical cystectomy in the treatment of invasive bladder cancer: Long-term results in 1054 patients. J. Clin. Oncol. 2001, 19, 666–675. [Google Scholar] [CrossRef] [PubMed]
- Necchi, A.; Sonpavde, G.; Lo Vullo, S.; Giardiello, D.; Bamias, A.; Crabb, S.J.; Harshman, L.C.; Bellmunt, J.; De Giorgi, U.; Sternberg, C.N.; et al. Nomogram-based Prediction of Overall Survival in Patients with Metastatic Urothelial Carcinoma Receiving First-line Platinum-based Chemotherapy: Retrospective International Study of Invasive/Advanced Cancer of the Urothelium (RISC). Eur. Urol. 2017, 71, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Tamalunas, A.; Schulz, G.B.; Rodler, S.; Apfelbeck, M.; Stief, C.G.; Casuscelli, J. Systemic treatment of bladder cancer. Urol. A 2021, 60, 247–258. [Google Scholar] [CrossRef] [PubMed]
- Galsky, M.D.; Hahn, N.M.; Rosenberg, J.; Sonpavde, G.; Hutson, T.; Oh, W.K.; Dreicer, R.; Vogelzang, N.; Sternberg, C.N.; Bajorin, D.F.; et al. Treatment of Patients with Metastatic Urothelial Cancer “Unfit” for Cisplatin-Based Chemotherapy. J. Clin. Oncol. 2011, 29, 2432–2438. [Google Scholar] [CrossRef]
- Antoni, S.; Ferlay, J.; Soerjomataram, I.; Znaor, A.; Jemal, A.; Bray, F. Bladder Cancer Incidence and Mortality: A Global Overview and Recent Trends. Eur. Urol. 2017, 71, 96–108. [Google Scholar] [CrossRef]
- Balar, A.V.; Galsky, M.D.; Rosenberg, J.E.; Powles, T.; Petrylak, D.P.; Bellmunt, J.; Loriot, Y.; Necchi, A.; Hoffman-Censits, J.; Perez-Gracia, J.L.; et al. Atezolizumab as first-line treatment in cisplatin-ineligible patients with locally advanced and metastatic urothelial carcinoma: A single-arm, multicentre, phase 2 trial. Lancet 2017, 389, 67–76. [Google Scholar] [CrossRef] [PubMed]
- Balar, A.V.; Castellano, D.; O’Donnell, P.H.; Grivas, P.; Vuky, J.; Powles, T.; Plimack, E.R.; Hahn, N.M.; de Wit, R.; Pang, L.; et al. First-line pembrolizumab in cisplatin-ineligible patients with locally advanced and unresectable or metastatic urothelial cancer (KEYNOTE-052): A multicentre, single-arm, phase 2 study. Lancet Oncol. 2017, 18, 1483–1492. [Google Scholar] [CrossRef] [PubMed]
- Mellman, I.; Coukos, G.; Dranoff, G. Cancer immunotherapy comes of age. Nature 2011, 480, 480–489. [Google Scholar] [CrossRef] [PubMed]
- Keir, M.E.; Butte, M.J.; Freeman, G.J.; Sharpe, A.H. PD-1 and its ligands in tolerance and immunity. Annu. Rev. Immunol. 2008, 26, 677–704. [Google Scholar] [CrossRef]
- Callea, M.; Albiges, L.; Gupta, M.; Cheng, S.-C.; Genega, E.M.; Fay, A.P.; Song, J.; Carvo, I.; Bhatt, R.S.; Atkins, M.B.; et al. Differential expression of PD-L1 between primary and metastatic sites in clear cell Renal Cell Carcinoma. Cancer Immunol. Res. 2015, 3, 1158–1164. [Google Scholar] [CrossRef] [PubMed]
- Alves, A.M.; Paredes, J.; Schmitt, F. Expression of PD-L1 in primary breast carcinoma and lymph node metastases. Surg. Exp. Pathol. 2019, 2, 7. [Google Scholar] [CrossRef]
- Schulz, G.B.; Todorova, R.; Braunschweig, T.; Rodler, S.; Volz, Y.; Eismann, L.; Pfitzinger, P.; Jokisch, F.; Buchner, A.; Stief, C.; et al. PD-L1 expression in bladder cancer: Which scoring algorithm in what tissue? Urol. Oncol. 2021, 39, 734.e1–734.e10. [Google Scholar] [CrossRef] [PubMed]
- Bellmunt, J.; Mullane, S.A.; Werner, L.; Fay, A.P.; Callea, M.; Leow, J.J.; Taplin, M.E.; Choueiri, T.K.; Hodi, F.S.; Freeman, G.J.; et al. Association of PD-L1 expression on tumor-infiltrating mononuclear cells and overall survival in patients with urothelial carcinoma. Ann. Oncol. 2015, 26, 812–817. [Google Scholar] [CrossRef] [PubMed]
- McDermott, D.F.; Atkins, M.B. PD-1 as a potential target in cancer therapy. Cancer Med. 2013, 2, 662–673. [Google Scholar] [CrossRef]
- Powles, T.; Kockx, M.; Rodriguez-Vida, A.; Duran, I.; Crabb, S.J.; Van Der Heijden, M.S.; Szabados, B.; Pous, A.F.; Gravis, G.; Herranz, U.A.; et al. Clinical efficacy and biomarker analysis of neoadjuvant atezolizumab in operable urothelial carcinoma in the ABACUS trial. Nat. Med. 2019, 25, 1706–1714. [Google Scholar] [CrossRef]
- Necchi, A.; Raggi, D.; Gallina, A.; Madison, R.; Colecchia, M.; Luciano, R.; Montironi, R.; Giannatempo, P.; Fare, E.; Pederzoli, F.; et al. Updated Results of PURE-01 with Preliminary Activity of Neoadjuvant Pembrolizumab in Patients with Muscle-invasive Bladder Carcinoma with Variant Histologies. Eur. Urol. 2019, 77, 439–446. [Google Scholar] [CrossRef] [PubMed]
- Tamalunas, A.; Buchner, A.; Kretschmer, A.; Jokisch, F.; Schulz, G.; Eismann, L.; Stief, C.G.; Grimm, T. Impact of Routine Laboratory Parameters in Patients Undergoing Radical Cystectomy for Urothelial Carcinoma of the Bladder: A Long-Term Follow-Up. Urol. Int. 2020, 104, 551–558. [Google Scholar] [CrossRef] [PubMed]
- Food and Drug Administration. Keytruda (Pembrolizumab) or Tecentriq (Atezolizumab): FDA Alerts Health Care Professionals and Investigators. FDA Statement- Decreased Survival in Some Patients in Clinial Trials Associated with Monotherapy; Food and Drug Administration: Silver Spring, MD, USA, 2018. [Google Scholar]
- European Medicines Agency. EMA Restricts Use of Keytruda and Tecentriq in Bladder Cancer: Data Show Lower Survival in Some Patients with Low Levels of Cancer Protein PD-L1; European Medicines Agency: Amsterdam, The Netherlands, 2018. [Google Scholar]
- Galsky, M.D.; Arija, J.A.A.; Bamias, A.; Davis, I.D.; De Santis, M.; Kikuchi, E.; Garcia-Del-Muro, X.; De Giorgi, U.; Mencinger, M.; Izumi, K.; et al. Atezolizumab with or without chemotherapy in metastatic urothelial cancer (IMvigor130): A multicentre, randomised, placebo-controlled phase 3 trial. Lancet 2020, 395, 1547–1557. [Google Scholar] [CrossRef] [PubMed]
- Powles, T.; Csoszi, T.; Ozguroglu, M.; Matsubara, N.; Geczi, L.; Cheng, S.Y.; Fradet, Y.; Oudard, S.; Vulsteke, C.; Morales Barrera, R.; et al. Pembrolizumab alone or combined with chemotherapy versus chemotherapy as first-line therapy for advanced urothelial carcinoma (KEYNOTE-361): A randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 931–945. [Google Scholar] [CrossRef]
- Powles, T.; van der Heijden, M.S.; Castellano, D.; Galsky, M.D.; Loriot, Y.; Petrylak, D.P.; Ogawa, O.; Park, S.H.; Lee, J.L.; De Giorgi, U.; et al. Durvalumab alone and durvalumab plus tremelimumab versus chemotherapy in previously untreated patients with unresectable, locally advanced or metastatic urothelial carcinoma (DANUBE): A randomised, open-label, multicentre, phase 3 trial. Lancet Oncol. 2020, 21, 1574–1588. [Google Scholar] [CrossRef]
- Humphrey, P.A.; Moch, H.; Cubilla, A.L.; Ulbright, T.M.; Reuter, V.E. The 2016 WHO Classification of Tumours of the Urinary System and Male Genital Organs-Part B: Prostate and Bladder Tumours. Eur. Urol. 2016, 70, 106–119. [Google Scholar] [CrossRef] [PubMed]
- Schildhaus, H.U. Predictive value of PD-L1 diagnostics. Pathologe 2018, 39, 498–519. [Google Scholar] [CrossRef] [PubMed]
- Haanen, J.; Carbonnel, F.; Robert, C.; Kerr, K.M.; Peters, S.; Larkin, J.; Jordan, K.; Committee, E.G. Management of toxicities from immunotherapy: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29, iv264–iv266. [Google Scholar] [CrossRef] [PubMed]
- Schalper, K.A.; Velcheti, V.; Carvajal, D.; Wimberly, H.; Brown, J.; Pusztai, L.; Rimm, D.L. In situ tumor PD-L1 mRNA expression is associated with increased TILs and better outcome in breast carcinomas. Clin. Cancer Res. 2014, 20, 2773–2782. [Google Scholar] [CrossRef]
- Gadiot, J.; Hooijkaas, A.I.; Kaiser, A.D.; van Tinteren, H.; van Boven, H.; Blank, C. Overall survival and PD-L1 expression in metastasized malignant melanoma. Cancer 2011, 117, 2192–2201. [Google Scholar] [CrossRef]
- Wen, Y.; Chen, Y.; Duan, X.; Zhu, W.; Cai, C.; Deng, T.; Zeng, G. The clinicopathological and prognostic value of PD-L1 in urothelial carcinoma: A meta-analysis. Clin. Exp. Med. 2019, 19, 407–416. [Google Scholar] [CrossRef] [PubMed]
- Powles, T.; Eder, J.P.; Fine, G.D.; Braiteh, F.S.; Loriot, Y.; Cruz, C.; Bellmunt, J.; Burris, H.A.; Petrylak, D.P.; Teng, S.L.; et al. MPDL3280A (anti-PD-L1) treatment leads to clinical activity in metastatic bladder cancer. Nature 2014, 515, 558–562. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, P.H.; Balar, A.V.; Vuky, J.; Castellano, D.E.; Bellmunt, J.; Powles, T.; Bajorin, D.F.; Grivas, P.; Hahn, N.M.; Plimack, E.R.; et al. KEYNOTE-052: Phase 2 study evaluating first-line pembrolizumab (pembro) in cisplatin-ineligible advanced urothelial cancer (UC)—Updated response and survival results. J. Clin. Oncol. 2019, 37, 4546. [Google Scholar] [CrossRef]
- Bellmunt, J.; de Wit, R.; Vaughn, D.J.; Fradet, Y.; Lee, J.L.; Fong, L.; Vogelzang, N.J.; Climent, M.A.; Petrylak, D.P.; Choueiri, T.K.; et al. Pembrolizumab as Second-Line Therapy for Advanced Urothelial Carcinoma. N. Engl. J. Med. 2017, 376, 1015–1026. [Google Scholar] [CrossRef] [PubMed]
- Yearley, J.H.; Gibson, C.; Yu, N.; Moon, C.; Murphy, E.; Juco, J.; Lunceford, J.; Cheng, J.; Chow, L.Q.M.; Seiwert, T.Y.; et al. PD-L2 Expression in Human Tumors: Relevance to Anti-PD-1 Therapy in Cancer. Clin. Cancer Res. 2017, 23, 3158–3167. [Google Scholar] [CrossRef] [PubMed]
- Dowell, A.C.; Munford, H.; Goel, A.; Gordon, N.S.; James, N.D.; Cheng, K.K.; Zeegers, M.P.; Ward, D.G.; Bryan, R.T. PD-L2 Is Constitutively Expressed in Normal and Malignant Urothelium. Front. Oncol. 2021, 11, 626748. [Google Scholar] [CrossRef] [PubMed]
- George, S.; Papanicolau-Sengos, A.; Lenzo, F.L.; Conroy, J.M.; Nesline, M.; Pabla, S.; Glenn, S.T.; Burgher, B.; Andreas, J.; Giamo, V.; et al. PD-L2 amplification and durable disease stabilization in patient with urothelial carcinoma receiving pembrolizumab. Oncoimmunology 2018, 7, e1460298. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Du, J.; Gao, Z.; Sun, H.; Mei, M.; Wang, Y.; Ren, Y.; Zhou, X. Evolving landscape of PD-L2: Bring new light to checkpoint immunotherapy. Br. J. Cancer 2023, 128, 1196–1207. [Google Scholar] [CrossRef] [PubMed]
- Faraj, S.F.; Munari, E.; Guner, G.; Taube, J.; Anders, R.; Hicks, J.; Meeker, A.; Schoenberg, M.; Bivalacqua, T.; Drake, C.; et al. Assessment of tumoral PD-L1 expression and intratumoral CD8+ T cells in urothelial carcinoma. Urology 2015, 85, 703.e1–703.e6. [Google Scholar] [CrossRef]
- Robertson, A.G.; Kim, J.; Al-Ahmadie, H.; Bellmunt, J.; Guo, G.; Cherniack, A.D.; Hinoue, T.; Laird, P.W.; Hoadley, K.A.; Akbani, R.; et al. Comprehensive Molecular Characterization of Muscle-Invasive Bladder Cancer. Cell 2017, 171, 540–556.e25. [Google Scholar] [CrossRef]
- Rosenberg, J.E.; Hoffman-Censits, J.; Powles, T.; van der Heijden, M.S.; Balar, A.V.; Necchi, A.; Dawson, N.; O’Donnell, P.H.; Balmanoukian, A.; Loriot, Y.; et al. Atezolizumab in patients with locally advanced and metastatic urothelial carcinoma who have progressed following treatment with platinum-based chemotherapy: A single-arm, multicentre, phase 2 trial. Lancet 2016, 387, 1909–1920. [Google Scholar] [CrossRef] [PubMed]
- Powles, T.; Valderrama, B.P.; Gupta, S.; Bedke, J.; Kikuchi, E.; Hoffman-Censits, J.; Iyer, G.; Vulsteke, C.; Park, S.H.; Shin, S.J.; et al. Enfortumab Vedotin and Pembrolizumab in Untreated Advanced Urothelial Cancer. N. Engl. J. Med. 2024, 390, 875–888. [Google Scholar] [CrossRef] [PubMed]
- Erlmeier, F.; Seitz, A.K.; Hatzichristodoulou, G.; Stecher, L.; Retz, M.; Gschwend, J.E.; Weichert, W.; Kubler, H.R.; Horn, T. The Role of PD-L1 Expression and Intratumoral Lymphocytes in Response to Perioperative Chemotherapy for Urothelial Carcinoma. Bladder Cancer 2016, 2, 425–432. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Total Tested (n = 282) | PD-L1+ (n = 124) | PD-L1− (n = 158) | p-Value |
|---|---|---|---|
| Age | |||
| Median | 74 | 74 | 0.755 |
| IQR | 64–79 | 58–80 | |
| Sex | |||
| Male | 76 (61.3%) | 114 (72.2%) | 0.436 |
| Female | 48 (38.7%) | 44 (27.8%) | 0.187 |
| PD-L1 status | |||
| IC 2/3 | 24 (19.3%) | N/A | |
| CPS ≥ 10 | 59 (47.6%) | N/A | |
| IC 2/3 + CPS ≥ 10 | 41 (33.1%) | N/A | |
| Comorbidities | |||
| None | 21 (16.9%) | 47 (29.7%) | 0.138 |
| 1 | 24 (19.4%) | 35 (22.2%) | 0.562 |
| 2 | 36 (29.0%) | 35 (22.2%) | 0.498 |
| >2 | 43 (34.7%) | 41 (26.0%) | 0.322 |
| ECOG | |||
| 0 | 40 (32.3%) | 60 (38.0%) | 0.417 |
| 1 | 52 (41.9%) | 76 (48.1%) | 0.502 |
| ≥2 | 32 (25.8%) | 22 (13.9%) | 0.177 |
| Progressive disease | 62 (50.0%) | 100 (63.3%) | 0.217 |
| Localization | |||
| Local | 36 (58.1%) | 96 (96.0%) | 0.359 |
| Nodal | 50 (80.6%) | 78 (78.0%) | 0.548 |
| Pulmonal | 12 (19.4%) | 20 (20.0%) | 0.555 |
| Hepatic | 4 (6.5%) | 24 (24.0%) | 0.031 |
| Bone | 10 (16.1%) | 16 (16.0%) | 0.603 |
| Peritoneal | 6 (9.7%) | 2 (2.0%) | 0.165 |
| Cerebral | 2 (3.2%) | 0 (0.0%) | 0.392 |
| Staging | |||
| None-invasive tumors | 0 (0.0%) | 14 (14.0%) | 0.029 |
| T2 | 12 (19.4%) | 24 (24.0%) | 0.420 |
| T3 | 28 (45.2%) | 28 (28.0%) | 0.091 |
| T4 | 22 (35.5%) | 34 (34.0%) | 0.539 |
| ≥T2 | 62 (100%) | 86 (86.0%) | 0.029 |
| Nodal status | |||
| NX | 14 (22.6%) | 4 (4.0%) | 0.112 |
| N0 | 20 (32.3%) | 28 (28.0%) | 0.673 |
| N1 | 16 (25.8%) | 42 (42.0%) | 0.107 |
| N2 | 12 (19.4%) | 18 (18.0%) | 0.765 |
| N3 | 0 (0.0%) | 8 (8.0%) | 0.138 |
| N+ | 28 (45.2%) | 68 (68.0%) | 0.212 |
| Resection status | |||
| R0 | 48 (77.4%) | 84 (84.0%) | 0.664 |
| R1 | 14 (22.6%) | 16 (16.0%) | 0.433 |
| TEAE; N (%) (n = 156) | Any Grade | Grade ≤ II | Grade III |
|---|---|---|---|
| Overall TEAEs; N (%) | 96 (61.5%) | 60 (37.0%) | 16 (9.9%) |
| Thyroiditis | 18 (11.5%) | 12 (7.7%) | 0 |
| Colitis | 16 (9.9%) | 8 (5.1%) | 2 (1.3%) |
| Hepatitis | 12 (7.7%) | 6 (3.8%) | 4 (2.6%) |
| Fatigue | 12 (7.7%) | 6 (3.8%) | 0 |
| Pruritus | 10 (6.4%) | 6 (3.8%) | 0 |
| Rash, maculopapular | 8 (5.1%) | 6 (3.8%) | 2 (1.3%) |
| Pneumonitis | 6 (3.8%) | 2 (1.3%) | 4 (2.6%) |
| Nephritis | 6 (3.8%) | 4 (2.6%) | 2 (1.3%) |
| Arthralgia | 6 (3.8%) | 2 (1.3%) | 0 |
| Hypophysitis | 2 (1.3%) | 0 | 2 (1.3%) |
| irTEAE | PD-L1+ (n = 58) | PD-L1− (n = 98) | p-Value |
|---|---|---|---|
| Overall TEAEs; N (%) | 36 (62.6%) | 60 (61.2%) | 0.598 |
| Grade I | 8 (13.8%) | 20 (20.4%) | 0.338 |
| Grade II | 22 (37.9%) | 30 (30.6%) | 0.224 |
| Grade III | 6 (10.3%) | 10 (10.2%) | 0.767 |
| Grade IV | 0 | 0 |
| A | ||||||
|---|---|---|---|---|---|---|
| PD-L1 Status | PD-L1 Negative | PD-L1 Positive | p Value | |||
| PFS 1-L (months) | p = 0.162 | |||||
| (n) | 100 | 62 | ||||
| Median | 3.9 | 5.6 | ||||
| 95% CI | (3.2–4.6) | (0–17.0) | ||||
| PFS 2-L | p = 0.274 | |||||
| (n) | 78 | 32 | ||||
| Median | 4 | 6.5 | ||||
| 95% CI | (1.9–6.1) | (2.2–10.9) | ||||
| PD-L1 Status | PD-L1 Negative | IC 2/3 | CPS ≥ 10 | IC 2/3 and CPS ≥ 10 | p Value | |
| PFS 1-L | p = 0.251 * p = 0.047 | |||||
| (n) | 100 | 12 | 30 | 20 | ||
| Median | 3.9 | 6 | 3.4 | 14.3 * | ||
| 95% CI | (3.2–4.6) | (1.4–10.5) | (2.5–4.4) | (1.6–29.5) | ||
| PFS 2-L | p = 0.444 | |||||
| (n) | 78 | 8 | 14 | 10 | ||
| Median | 4 | 3.7 | NR | 6.5 | ||
| 95% CI | (1.9–6.1) | (2.9–4.5) | (1.3–13.0) | |||
| B | ||||||
| Treatment | CTx | ICI | p Value | |||
| PFS 1-L | p < 0.001 | |||||
| (n) | 94 | 68 | ||||
| Median | 3.5 | 17.5 | ||||
| 95% CI | (2.6–4.4) | (9.2–25.8) | ||||
| PFS 2-L | p = 0.671 | |||||
| (n) | 22 | 88 | ||||
| Median | 4.4 | 4 | ||||
| 95% CI | (3.7–5.1) | (1.3–6.7) | ||||
| C | ||||||
| 1-L Treatment | PFS 1-L | CTx | ICI | p Value | ||
| PD-L1 Status | ||||||
| PD-L1 positive | (n) | 26 | 32 | p < 0.001 | ||
| Median | 3.4 | 17.5 | ||||
| 95% CI | (2.9–3.9) | (11.0–24.1) | ||||
| PD-L1 negative | (n) | 68 | 32 | p = 0.03 | ||
| Median | 3.8 | 6.3 | ||||
| 95% CI | (2.3–5.2) | (2.0–10.6) | ||||
| p value | p < 0.001 | p = 0.648 | p = 0.327 | p = 0.079 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tamalunas, A.; Aydogdu, C.; Unterrainer, L.M.; Schott, M.; Rodler, S.; Ledderose, S.; Schulz, G.B.; Stief, C.G.; Casuscelli, J. The Vanishing Clinical Value of PD-L1 Status as a Predictive Biomarker in the First-Line Treatment of Urothelial Carcinoma of the Bladder. Cancers 2024, 16, 1536. https://doi.org/10.3390/cancers16081536
Tamalunas A, Aydogdu C, Unterrainer LM, Schott M, Rodler S, Ledderose S, Schulz GB, Stief CG, Casuscelli J. The Vanishing Clinical Value of PD-L1 Status as a Predictive Biomarker in the First-Line Treatment of Urothelial Carcinoma of the Bladder. Cancers. 2024; 16(8):1536. https://doi.org/10.3390/cancers16081536
Chicago/Turabian StyleTamalunas, Alexander, Can Aydogdu, Lena M. Unterrainer, Melanie Schott, Severin Rodler, Stephan Ledderose, Gerald B. Schulz, Christian G. Stief, and Jozefina Casuscelli. 2024. "The Vanishing Clinical Value of PD-L1 Status as a Predictive Biomarker in the First-Line Treatment of Urothelial Carcinoma of the Bladder" Cancers 16, no. 8: 1536. https://doi.org/10.3390/cancers16081536