
Transfer Learning-Based Integration of Dual Imaging Modalities for Enhanced Classification Accuracy in Confocal Laser Endomicroscopy of Lung Cancer

 , , and
, , and 
Simple Summary
Abstract
1. Introduction
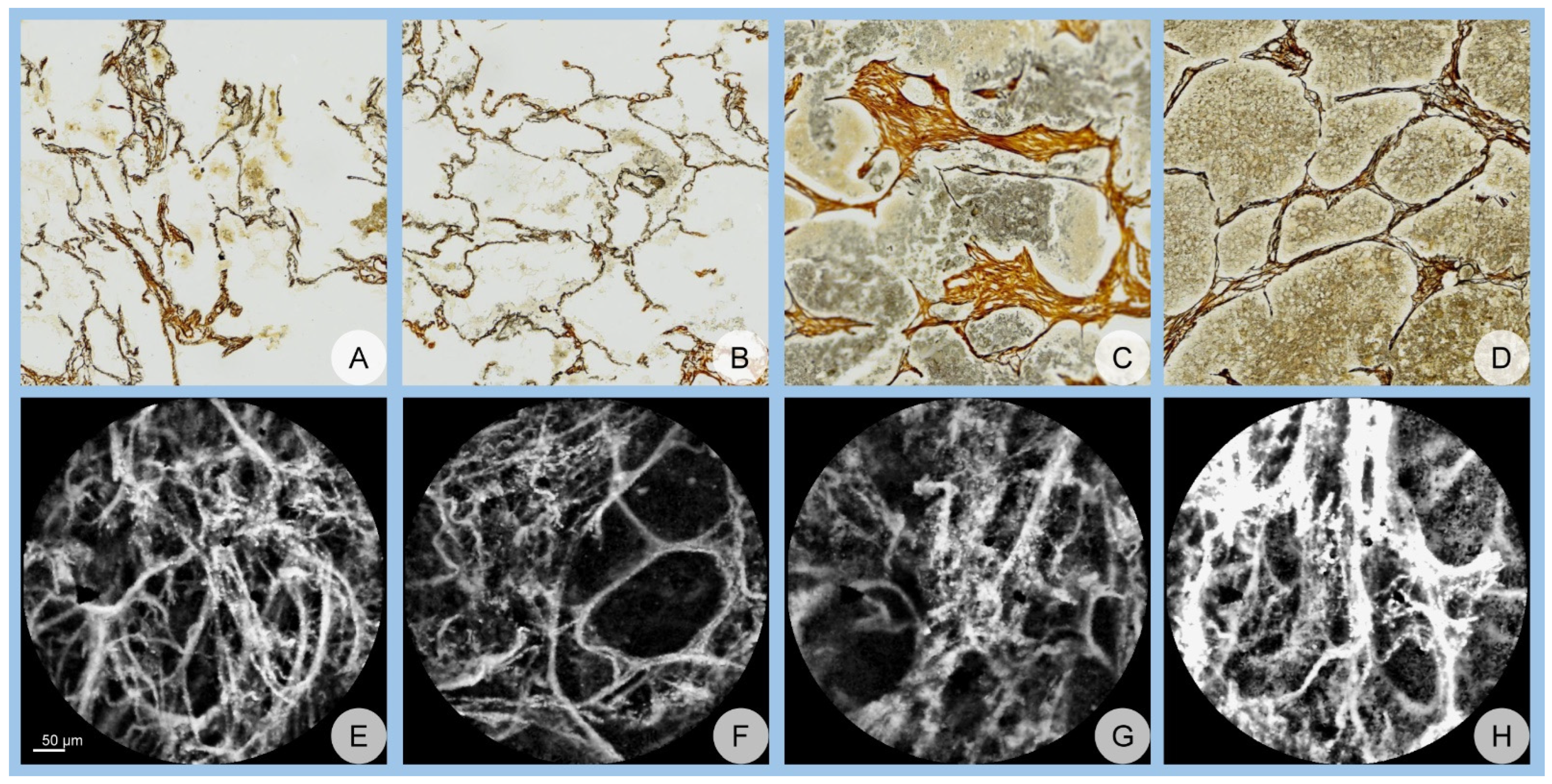
2. Materials and Methods
3. Results
3.1. Network Performance
3.1.1. Accuracy Assessment
3.1.2. AUC Assessment

{kind=link}
{kind=link}
{kind=link}
| Accuracy, Mean ± Standard Deviation (SD) | AlexNet | GoogLeNet | ResNet | ANOVA, p |
|---|---|---|---|---|
| Dual TL scenario | 94.97 ± 1.76 | 91.43 ± 2.17 | 89.87 ± 2.15 | <0.001 |
| Confocal TL scenario | 90.14 ± 2.13 | 85.71 ± 2.55 | 84.65 ± 1.84 | <0.001 |
| Student’s t-test, p | <0.001 | <0.001 | <0.001 |
| AUC, Mean ± Standard Deviation (SD) | AlexNet | GoogLeNet | ResNet | ANOVA, p |
|---|---|---|---|---|
| Dual TL scenario | 0.98 ± 0.01 | 0.97 ± 0.01 | 0.96 ± 0.01 | <0.001 |
| Confocal TL scenario | 0.97 ± 0.01 | 0.93 ± 0.02 | 0.94 ± 0.01 | <0.001 |
| Student’s t-test, p | <0.001 | <0.001 | <0.001 |
3.2. Confusion Matrix Analysis
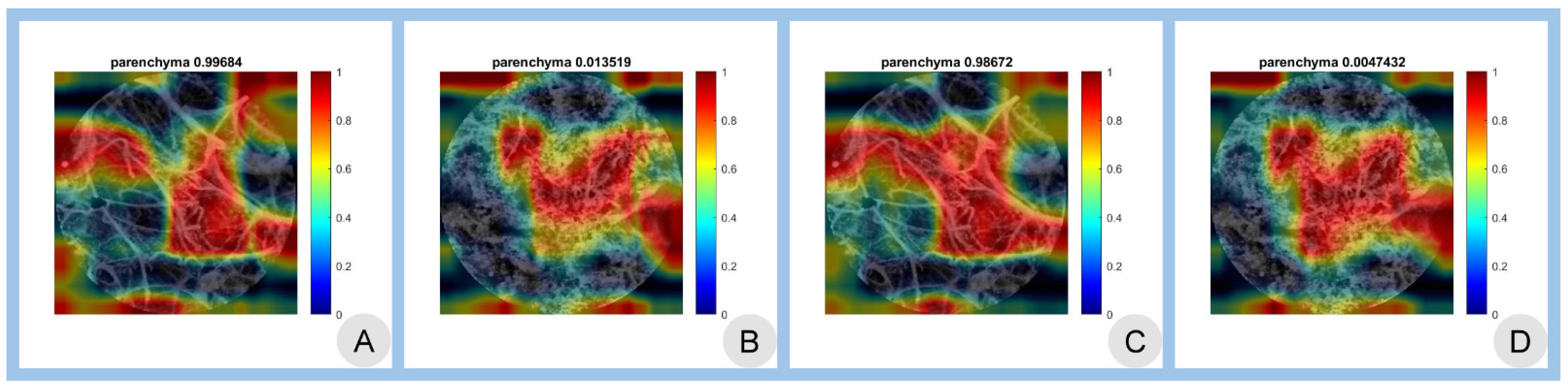
3.3. Class Activation Mapping
3.4. Summary of Performance Metrics
3.5. Statistical Significance
3.6. Overall Performance
4. Discussion
4.1. Limitations
4.2. Wrap-Up and Future Work
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AI | artificial intelligence |
| AUC | area under the curve |
| CAM | class activation mapping |
| CNN | convolutional neural network |
| DL | deep learning |
| LDCT | low-dose computed tomography |
| pCLE | confocal laser endomicroscopy |
| TL | transfer learning |
References
- Cai, W.; Zhu, X.; Li, Y.; Xu, Y. Interpretation of global lung cancer statistics. J. Thorac. Oncol. 2024, 19, 562–569. [Google Scholar]
- Barta, J.A.; Powell, C.A.; Wisnivesky, J.P. Global Epidemiology of Lung Cancer. Ann. Glob. Health 2019, 85, 8. [Google Scholar] [CrossRef]
- Collins, L.G.; Haines, C.; Perkel, R.; Enck, R.E. Lung cancer: Diagnosis and management. Am. Fam. Physician 2007, 75, 56–63. [Google Scholar]
- Malhotra, J.; Malvezzi, M.; Negri, E.; La Vecchia, C.; Boffetta, P. Risk factors for lung cancer worldwide. Eur. Respir. J. 2016, 48, 889–902. [Google Scholar] [CrossRef] [PubMed]
- Lipfert, F.W.; Wyzga, R.E. Longitudinal relationships between lung cancer mortality and air pollution. Risk Anal. 2019, 39, 1646–1664. [Google Scholar]
- Maisonneuve, P.; Rampinelli, C.; Bertolotti, R.; Melloni, G.; Pelosi, G.; de Braud, F.; Spaggiari, L.; Pastorino, U. Low-dose computed tomography screening for lung cancer in smokers. JAMA 2019, 322, 584–594. [Google Scholar]
- Gouvinhas, C.; De Mello, R.A.; Oliveira, D.; Castro-Lopes, J.M.; Castelo-Branco, P.; Dos Santos, R.S.; Hespanhol, V.; Pozza, D.H. Lung cancer: A brief review of epidemiology and screening strategies. Future Oncol. 2018, 14, 567–575. [Google Scholar] [CrossRef] [PubMed]
- Shankar, A.; Dubey, A.; Saini, D.; Singh, M.; Prasad, C.P.; Roy, S.; Mandal, C.; Bhandari, S.; Kumar, S.; Lathwal, A.; et al. Environ-mental and occupational determinants of lung cancer. Transl. Lung Cancer Res. 2019, 8 (Suppl. S1), S31–S49. [Google Scholar] [CrossRef]
- Hocking, W.G. Integrating prevention and screening for lung cancer into clinical practice. Chest 2013, 143, 1216–1224. [Google Scholar]
- D’Urso, D.; Doneddu, G.; Lojacono, M.; Tanda, F.; Serra, M.; Marras, V.; Cossu, A.; Corda, S.; Piredda, S.; Deidda, M.; et al. Sputum analysis for non-invasive early lung cancer detection. Respir. Med. 2013, 107, 853–858. [Google Scholar] [CrossRef]
- Lebrett, M.B.; Crosbie, P.A. Targeting lung cancer screening to individuals at highest risk. Lancet Respir. Med. 2020, 8, 226–228. [Google Scholar]
- Takemura, S.; Kurimoto, N.; Miyazawa, T.; Ohta, K.; Hino, H.; Murata, Y.; Takai, Y.; Kaneko, Y.; Maekura, R. Probe-based confocal laser endomicroscopy for rapid diagnosis of pulmonary nodules. Respir. Res. 2019, 20, 162. [Google Scholar]
- Chaudoir, B.R.; Brandi, C.; McGill, S.; Smith, R.A.; Wilson, J.; Park, G.; Klein, C. Frontier in pathology: Comparison of pCLE and biopsy. J. Thorac. Dis. 2014, 6, 523–530. [Google Scholar]
- Wellikoff, A.S.; Holladay, R.C.; Downie, G.H. Comparison of in vivo probe-based confocal laser endomicroscopy with biopsy. Respiration 2015, 90, 205–212. [Google Scholar]
- Yserbyt, J.; Dooms, C.; Ninane, V. Perspectives using probe-based confocal laser endomicroscopy. Respiration 2013, 85, 304–310. [Google Scholar]
- Danilevskaya, O.V.; Sazonov, D.V.; Zabozlaev, F.G.; Averyanov, A.V.; Sorokina, A.; Sotnikova, A.G.; Urazovsky, N.; Kuzovlev, O.P.; Shablovsky, O.R. Confocal laser endomicroscopy in diagnosis of solitary and multiple pulmonary nodular infiltrates. Eur. Respir. J. 2012, 40, 660. [Google Scholar]
- Shafiek, H.; Fiorentino, F.; Larici, A.; Ravaglia, C.; Poletti, V.; Tognini, G.; Roviaro, G.; Fanti, S.; Neri, E.; Fiume, D. Usefulness of bron-choscopic probe-based confocal laser endomicroscopy in pneumonia. Respir. Res. 2016, 17, 51. [Google Scholar]
- Yserbyt, J.; Dooms, C.; Verleden, G.M.; Vanaudenaerde, B.M.; Vos, R.; Weynand, B.; Decramer, M.; Verleden, S.E. Probe-based confocal laser endomicroscopy in acute lung rejection. Am. J. Transplant. 2011, 11, 2466–2472. [Google Scholar]
- Salaün, M.; Guisier, F.; Lena, H.; Thiberville, L. In vivo probe-based confocal laser endomicroscopy in pulmonary pathology. Respir. Res. 2019, 20, 225. [Google Scholar]
- Buchner, A.M.; Gómez, V.; Heckman, M.G.; Shah, R.J.; Schueler, B.A.; Ghabril, M.S.; Raimondo, M.; Krishna, M.; Wallace, M.B. The learning curve of in vivo probe-based confocal laser endomicroscopy. Endoscopy 2009, 41, 902–908. [Google Scholar]
- Nóbrega, R.V.M.; Peixoto, S.A.; Silva, S.P.; Filho, P.P. Lung nodule classification via deep transfer learning in CT Lung Images. In Proceedings of the 2018 IEEE 31st International Symposium on Computer-Based Medical Systems (CBMS), Karlstad, Sweden, 18–21 June 2018; pp. 244–249. [Google Scholar]
- Lakhani, P.; Sundaram, B. Deep learning at chest radiography: Automated classification of tuberculosis. Radiology 2017, 284, 574–582. [Google Scholar] [CrossRef] [PubMed]
- Lin, Z. Interpretability study of pretrained models via transfer learning for lung cancer prediction. Proc. SPIE Med. Imaging 2022, 12451, 124514X. [Google Scholar]
- Zhang, Z. The transferability of transfer learning model based on ImageNet for medical image classification tasks. Appl. Comput. Eng. 2023, 18, 143–151. [Google Scholar] [CrossRef]
- Osmani, N.; Rezayi, S.; Esmaeeli, E.; Karimi, A. Transfer learning from non-medical images to medical images. Front. Health Inform. 2024, 13, 177. [Google Scholar] [CrossRef]
- Romero, M.; Interian, Y.; Solberg, T.; Valdes, G. Targeted transfer learning for small medical datasets. Med. Phys. 2019, 46, 2328–2337. [Google Scholar]
- Bungărdean, R.M.; Şerbănescu, M.-S.; Streba, C.T.; Crişan, M. Deep learning with transfer learning in pathology. Case study: Classification of basal cell carcinoma. Rom. J. Morphol. Embryol. 2022, 62, 1017–1028. [Google Scholar] [CrossRef]
- Celik, Y.; Talo, M.; Yıldırım, Ö.; Karabatak, M.; Acharya, U.R. Automated invasive ductal carcinoma detection using deep transfer learning. Pattern Recognit. Lett. 2020, 133, 232–239. [Google Scholar] [CrossRef]
- Anusha, M.; Reddy, D.S. Enhancing lung and colon cancer diagnosis using ImageNet-trained transfer learning. In Proceedings of the 2024 Tenth International Conference on Bio Signals, Images, and Instrumentation (ICBSII), Chennai, India, 20–22 March 2024; pp. 1–4. [Google Scholar]
- Said, M.M.; Islam, M.S.; Sumon, M.S.I.; Vranić, S.; Al Saady, R.M.; Alqahtani, A.; Chowdhury, M.; Pedersen, S. Innovative deep learning for lung and colon cancer classification. Appl. Comput. Intell. Soft. Comput. 2024, 2024, 5562890. [Google Scholar]
- Gao, R.; Tang, Y.; Xu, K.; Kammer, M.; Antic, S.; Deppen, S.; Sandler, K.; Massion, P.; Huo, Y.; Landman, B.A. Deep multi-path network integrating incomplete biomarker and chest CT data. Proc. SPIE Med. Imaging 2020, 11596, 115961E. [Google Scholar]
- MathWorks. AlexNet. Available online: https://www.mathworks.com/help/deeplearning/ref/alexnet.html (accessed on 28 January 2025).
- MathWorks. GoogLeNet. Available online: https://www.mathworks.com/help/deeplearning/ref/googlenet.html (accessed on 28 January 2025).
- MathWorks. ResNet-18. Available online: https://www.mathworks.com/help/deeplearning/ref/resnet18.html (accessed on 28 January 2025).
- ImageNet. Available online: http://www.image-net.org/ (accessed on 28 January 2025).
- Nica, R.-E.; Șerbănescu, M.-S.; Florescu, L.-M.; Camen, G.-C.; Streba, C.T.; Gheonea, I.-A. Deep Learning: A Promising Method for Histological Class Prediction of Breast Tumors in Mammography. J. Digit. Imaging 2021, 34, 1190–1198. [Google Scholar] [CrossRef]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. Imagenet classification with deep convolutional neural networks. Adv. Neural Inf. Process Syst. 2012, 25, 1097–1105. [Google Scholar] [CrossRef]
- Szegedy, C.; Liu, W.; Jia, Y.; Sermanet, P.; Reed, S.; Anguelov, D.; Erhan, D.; Vanhoucke, V.; Rabinovich, A. Going deeper with convo-lutions. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Boston, MA, USA, 8–12 June 2015; pp. 1–9. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep Residual Learning for Image Recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 26 June–1 July 2016; pp. 770–778. [Google Scholar]
- Tortora, M.; Cordelli, E.; Sicilia, R.; Nibid, L.; Ippolito, E.; Perrone, G.; Ramella, S.; Soda, P. RadioPathomics: Multimodal Learning in Non-Small Cell Lung Cancer. arXiv 2022, arXiv:2204.12423. [Google Scholar]
- Mercuţ, R.; Ciurea, M.E.; Traşcă, E.T.; Ionescu, M.; Mercuţ, M.F.; Rădulescu, P.M.; Călăraşu, C.; Streba, L.; Ionescu, A.G.; Rădulescu, D. Applying Neural Networks to Analyse Inflammatory, Sociodemographic, and Psychological Factors in Non-Melanoma Skin Cancer and Colon Cancer: A Statistical and Artificial Intelligence Approach. Diagnostics 2024, 14, 2759. [Google Scholar] [CrossRef]
- Radulescu, D.; Calafeteanu, D.M.; Radulescu, P.-M.; Boldea, G.-J.; Mercut, R.; Ciupeanu-Calugaru, E.D.; Georgescu, E.-F.; Boldea, A.M.; Georgescu, I.; Caluianu, E.-I.; et al. Enhancing the Understanding of Abdominal Trauma During the COVID-19 Pandemic Through Co-Occurrence Analysis and Machine Learning. Diagnostics 2024, 14, 2444. [Google Scholar] [CrossRef] [PubMed]
- Şerbănescu, M.-S.; Manea, N.C.; Streba, L.; Belciug, S.; Pleşea, I.E.; Pirici, I.; Bungărdean, R.M.; Pleşea, R.M. Automated Gleason grading of prostate cancer using transfer learning from general-purpose deep-learning networks. Rom. J. Morphol. Embryol. 2020, 61, 149–155. [Google Scholar] [CrossRef]
- Şerbănescu, M.-S.; Oancea, C.-N.; Streba, C.T.; Pleşea, I.E.; Pirici, D.; Streba, L.; Pleşea, R.M. Agreement of two pre-trained deep-learning neural networks built with transfer learning with six pathologists on 6000 patches of prostate cancer from Gleason2019 Challenge. Rom. J. Morphol. Embryol. 2020, 61, 513–519. [Google Scholar] [CrossRef]
- Șerbănescu, M.-S.; Bungărdean, R.M.; Georgiu, C.; Crișan, M. Nodular and Micronodular Basal Cell Carcinoma Subtypes Are Different Tumors Based on Their Morphological Architecture and Their Interaction with the Surrounding Stroma. Diagnostics 2022, 12, 1636. [Google Scholar] [CrossRef] [PubMed]
- Bungărdean, R.-M.; Şerbănescu, M.-S.; Colosi, H.A.; Crişan, M. High-frequency ultrasound: An essential non-invasive tool for the pre-therapeutic assessment of basal cell carcinoma. Rom. J. Morphol. Embryol. 2022, 62, 545–551. [Google Scholar] [CrossRef] [PubMed]
- Mitroi, G.; Pleşea, R.M.; Pop, O.T.; Ciovică, D.V.; Şerbănescu, M.S.; Alexandru, D.O.; Stoiculescu, A.; Pleşea, I.E. Correlations between intratumoral interstitial fibrillary network and vascular network in Srigley patterns of prostate adenocarcinoma. Rom. J. Morphol. Embryol. 2015, 56, 1319–1328. [Google Scholar] [PubMed]
- Pleşea, I.E.; Stoiculescu, A.; Serbănescu, M.; Alexandru, D.O.; Man, M.; Pop, O.T.; Pleşea, R.M. Correlations between intratumoral vascular network and tumoral architecture in prostatic adenocarcinoma. Rom. J. Morphol. Embryol. 2013, 54, 299–308. [Google Scholar]
- Stoiculescu, A.; Plesea, I.E.; Pop, O.T.; Alexandru, D.O.; Man, M.; Serbanescu, M.; Plesea, R.M. Correlations between intratumoral in-terstitial fibrillary network and tumoral architecture in prostatic adenocarcinoma. Rom. J. Morphol. Embryol. 2012, 53, 941–950. [Google Scholar] [PubMed]
- Plesea, R.M.; Serbanescu, M.-S.; Ciovica, D.V.; Rosu, G.-C.; Moldovan, V.T.; Bungardean, R.M.; Popescu, N.A.; Plesea, I.E. The study of tumor architecture components in prostate adenocarcinoma using fractal dimension analysis. Rom. J. Morphol. Embryol. 2019, 60, 501–519. [Google Scholar] [PubMed]
- Hassan, S.A.A.; Sayed, M.S.; Abdalla, M.I.; Rashwan, M.A. Breast cancer masses classification using deep convolutional neural networks and transfer learning. Multimed. Tools Appl. 2020, 79, 30735–30768. [Google Scholar] [CrossRef]
- Jiang, Y.; Chen, L.; Zhang, H.; Xiao, X. Breast cancer histopathological image classification using convolutional neural networks with small SE-ResNet modules. Int. J. Comput. Assist. Radiol. Surg. 2017, 12, 1479–1486. [Google Scholar] [CrossRef]
- Mazo, C.; Bernal, J.; Trujillo, M.; Alegre, E. Transfer learning for classification of cardiovascular tissues in histological images. Comput. Methods Programs Biomed. 2018, 165, 69–76. [Google Scholar] [CrossRef]
- Neamah, K.; Mohamed, F.; Waheed, S.R.; Kurdi, W.H.M.; Taha, A.Y.; Kadhim, K.A. Utilizing Deep Improved ResNet-50 for Brain Tumor Classification Based on MRI. IEEE Open J. Comput. Soc. 2024, 5, 446–456. [Google Scholar] [CrossRef]
- Saleh, L.; Zhang, L. Medical Image Classification Using Transfer Learning and Network Pruning Algorithms. In Proceedings of the 2023 IEEE International Conference on Systems, Man, and Cybernetics (SMC), Honolulu, HI, USA, 1–4 October 2023; pp. 1932–1938. [Google Scholar]
- Anusha, M.; Reddy, D.S. Enhancing Lung and Colon Cancer Diagnosis: An ImageNet-Trained Transfer Learning Approach for Histopathological Image Analysis. In Proceedings of the 2024 Tenth International Conference on Bio Signals, Images, and Instrumentation (ICBSII), Chennai, India, 20–22 March 2024; pp. 1–4. [Google Scholar]
- Boumaraf, S.; Liu, X.; Zheng, Z.; Ma, X.; Ferkous, C. A new transfer learning-based approach to magnification dependent and independent classification of breast cancer in histopathological images. Biomed. Signal Process. Control 2021, 63, 102192. [Google Scholar] [CrossRef]
- Leung, K.H.; Rowe, S.P.; Sadaghiani, M.S.; Leal, J.P.; Mena, E.; Choyke, P.L.; Du, Y.; Pomper, M.G. Deep Semisupervised Transfer Learning for Fully Automated Whole-Body Tumor Quantification and Prognosis of Cancer on PET/CT. J. Nucl. Med. 2024, 65, 643–650. [Google Scholar] [CrossRef] [PubMed]
- Hu, Q.; Whitney, H.M.; Giger, M.L. A deep learning methodology for improved breast cancer diagnosis using multiparametric MRI. Sci. Rep. 2020, 10, 10536. [Google Scholar] [CrossRef]
- Xu, Y.; Jia, Z.; Wang, L.-B.; Ai, Y.; Zhang, F.; Lai, M.; Chang, E.I.-C. Large scale tissue histopathology image classification, segmentation, and visualization via deep convolutional activation features. BMC Bioinform. 2019, 19, 281. [Google Scholar] [CrossRef]
- Syed, A.H.; Khan, T.; Khan, S.A. Deep Transfer Learning Techniques-Based Automated Classification and Detection of Pulmonary Fibrosis from Chest CT Images. Processes 2023, 11, 443. [Google Scholar] [CrossRef]
- Shi, Z.; Hao, H.; Zhao, M.; Feng, Y.; He, L.; Wang, Y.; Suzuki, K. A deep CNN-based transfer learning method for false positive reduction. Multimed. Tools Appl. 2019, 78, 1017–1033. [Google Scholar] [CrossRef]
- Jin, H.; Li, Z.; Tong, R.; Lin, L. A deep 3D residual CNN for false-positive reduction in pulmonary nodule detection. Med. Phys. 2018, 45, 2097–2107. [Google Scholar] [CrossRef]
- Noaman, N.F.; Kanber, B.M.; Al Smadi, A.; Jiao, L.; Alsmadi, M.K. Advancing Oncology Diagnostics: AI-Enabled Early Detection of Lung Cancer Through Hybrid Histological Image Analysis. IEEE Access 2024, 12, 64396–64415. [Google Scholar] [CrossRef]
- Setio, A.A.; Ciompi, F.; Litjens, G.J.; Gerke, P.K.; Jacobs, C.; Riel, S.J.; Wille, M.M.; Naqibullah, M.; Sánchez, C.I.; Ginneken, B.V. Pulmonary Nodule Detection in CT Images: False Positive Reduction Using Multi-View Convolutional Networks. IEEE Trans. Med. Imaging 2016, 35, 1160–1169. [Google Scholar] [CrossRef] [PubMed]
- Chaunzwa, T.L.; Hosny, A.; Xu, Y.; Shafer, A.; Diao, N.; Lanuti, M.; Christiani, D.C.; Mak, R.H.; Aerts, H.J.W.L. Deep learning classification of lung cancer histology using CT images. Eur. J. Radiol. 2021, 145, 110013. [Google Scholar] [CrossRef]
- Şerbănescu, M.S.; Pleşea, I.E. A hardware approach for histological and histopathological digital image stain normalization. Rom. J. Morphol. Embryol. 2015, 56 (Suppl. S2), 735–741. [Google Scholar]

| AlexNet | GoogLeNet | ResNet | ||||||
|---|---|---|---|---|---|---|---|---|
| Benign | Malignant | Benign | Malignant | Benign | Malignant | |||
| Actual class | Confocal TL scenario | Benign | 395 | 43 | 366 | 46 | 341 | 32 |
| Malignant | 5 | 357 | 34 | 354 | 59 | 368 | ||
| Dual TL scenario | Benign | 394 | 24 | 387 | 58 | 341 | 27 | |
| Malignant | 6 | 376 | 13 | 342 | 59 | 373 | ||
| Predicted class | ||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Șerbănescu, M.-S.; Streba, L.; Demetrian, A.D.; Gheorghe, A.-G.; Mămuleanu, M.; Pirici, D.-N.; Streba, C.-T. Transfer Learning-Based Integration of Dual Imaging Modalities for Enhanced Classification Accuracy in Confocal Laser Endomicroscopy of Lung Cancer. Cancers 2025, 17, 611. https://doi.org/10.3390/cancers17040611
Șerbănescu M-S, Streba L, Demetrian AD, Gheorghe A-G, Mămuleanu M, Pirici D-N, Streba C-T. Transfer Learning-Based Integration of Dual Imaging Modalities for Enhanced Classification Accuracy in Confocal Laser Endomicroscopy of Lung Cancer. Cancers. 2025; 17(4):611. https://doi.org/10.3390/cancers17040611
Chicago/Turabian StyleȘerbănescu, Mircea-Sebastian, Liliana Streba, Alin Dragoș Demetrian, Andreea-Georgiana Gheorghe, Mădălin Mămuleanu, Daniel-Nicolae Pirici, and Costin-Teodor Streba. 2025. "Transfer Learning-Based Integration of Dual Imaging Modalities for Enhanced Classification Accuracy in Confocal Laser Endomicroscopy of Lung Cancer" Cancers 17, no. 4: 611. https://doi.org/10.3390/cancers17040611
APA StyleȘerbănescu, M.-S., Streba, L., Demetrian, A. D., Gheorghe, A.-G., Mămuleanu, M., Pirici, D.-N., & Streba, C.-T. (2025). Transfer Learning-Based Integration of Dual Imaging Modalities for Enhanced Classification Accuracy in Confocal Laser Endomicroscopy of Lung Cancer. Cancers, 17(4), 611. https://doi.org/10.3390/cancers17040611