Barriers and Enabling Factors for Central and Household Level Water Treatment in a Refugee Setting: A Mixed-Method Study among Rohingyas in Cox’s Bazar, Bangladesh

 ,
,  , ,
, ,
Abstract
:1. Background
2. Methods
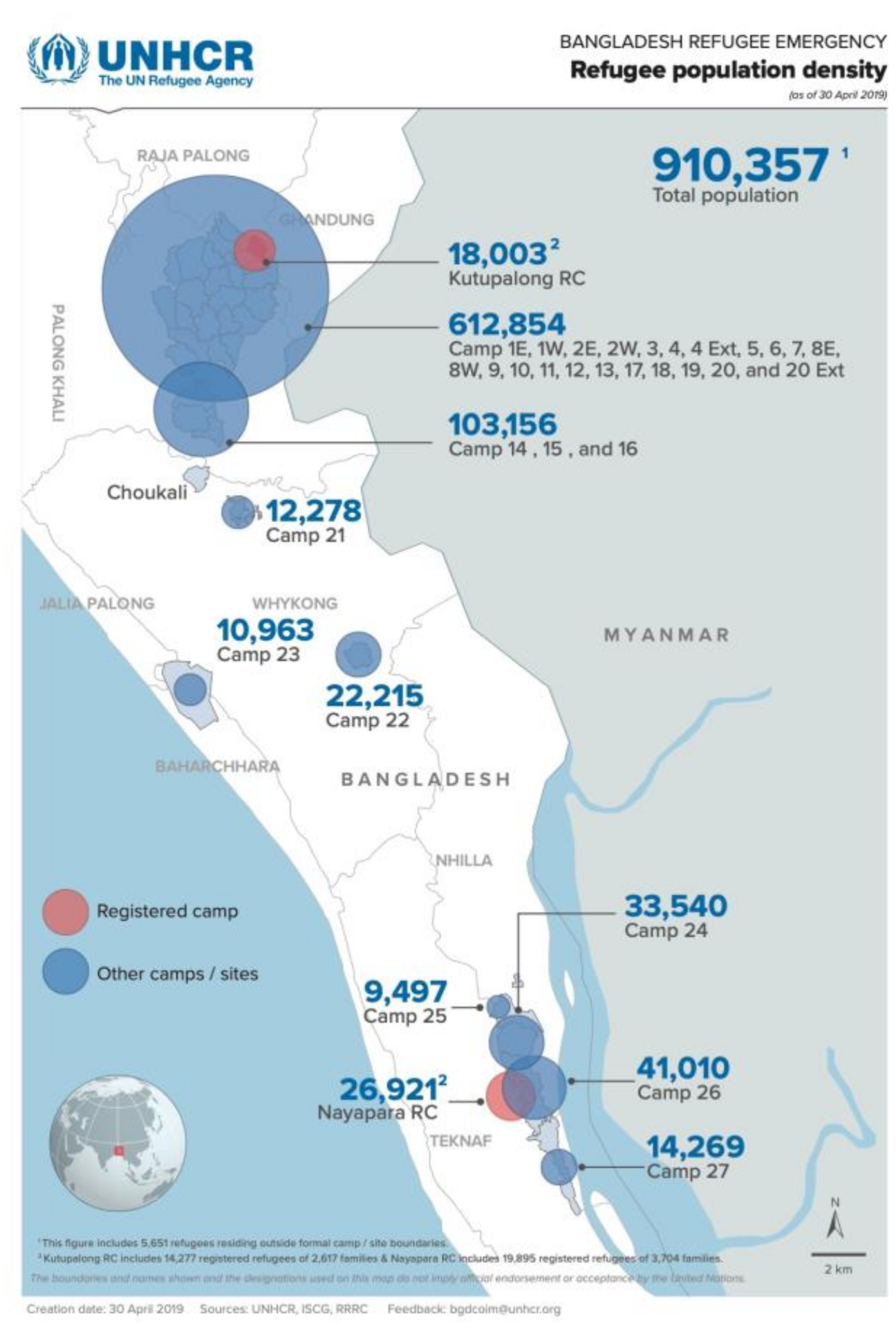
2.1. Study Area
2.2. Water Treatment Program Delivery and Communication with Community Members
2.3. Data Collection
2.4. Water Sample Collection and Analysis
2.5. Data Analysis
- -
- ‘Doers’—those that had access to chlorine (Aquatabs) and used/chose piped water chlorination sources daily or most of the time
- -
- ‘Non-Doers’—those that had access to chlorine and used/chose piped water chlorination sources on an intermittent basis or chose not to use at all
2.6. Ethical Approval
3. Results
3.1. Respondents’ Characteristics
3.2. Water Source, Perceptions Related to Water Source, and Water Quality
3.3. Barriers to Water Treatment
3.3.1. Water Collection and Household Storage
3.3.2. Water Treatment Program Delivery and Communication with Community Members
3.3.3. Smell and Taste of Treated Water
3.3.4. Fear of Religious Conversion
3.3.5. Inadequate Supply of Water Treatment Products
3.4. Motivators for Water Treatment
3.4.1. Perceived Health Benefits
3.4.2. Ease of Use
3.5. Residual Chlorine in the Water
4. Discussion
4.1. Limitations
4.2. Recommendations
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mahmud, Z.H.; Islam, S.; Imran, K.M.; Hakim, S.A.I.; Worth, M.; Ahmed, A.; Hossan, S.; Haider, M.; Islam, M.R.; Hossain, F.; et al. Occurrence of Escherichia coli and faecal coliforms in drinking water at source and household point-of-use in Rohingya camps, Bangladesh. Gut Pathog. 2019, 11, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mokomane, M.; Kasvosve, I.; De Melo, E.; Pernica, J.M.; Goldfarb, D.M. The global problem of childhood diarrhoeal diseases: Emerging strategies in prevention and management. Ther. Adv. Infect. Dis. 2017, 5, 29–43. [Google Scholar] [CrossRef] [PubMed]
- Watson, J.T.; Gayer, M.; Connolly, M.A. Epidemics after Natural Disasters. Emerg. Infect. Dis. 2007, 13, 1–5. [Google Scholar] [CrossRef] [PubMed]
- WHO. Preventing Diarrhoea through Better Water, Sanitation and Hygiene: Exposures and Impacts in Low-and Middle-Income Countries; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Connolly, M.A.; Gayer, M.; Ryan, M.J.; Salama, P.; Spiegel, P.B.; Heymann, D.L. Communicable diseases in complex emergencies: Impact and challenges. Lancet 2004, 364, 1974–1983. [Google Scholar] [CrossRef]
- WASH Sector-Cox’s Bazar: ReliefWeb. WASH Sector Strategy For Rohingyas Influx March to December 2018. Available online: https://reliefweb.int/sites/reliefweb.int/files/resources/wash_sector_cbx_mar_-_dec_2018_strategy.pdf (accessed on 30 July 2020).
- UNHCR. Rohingya Emergency. 2019. Available online: https://www.unhcr.org/rohingya-emergency.html (accessed on 30 July 2020).
- Sikder, M.K.; Mirindi, P.; String, G.; Lantagne, D.S. Delivering Drinking Water by Truck in Humanitarian Contexts: Results from Mixed-Methods Evaluations in the Democratic Republic of the Congo and Bangladesh. Environ. Sci. Technol. 2020, 54, 5041–5050. [Google Scholar] [CrossRef]
- REACH. Bangladesh Water, Sanitation and Hygiene Baseline Assessment—Cox’s Bazar, Rohingya Refugee Response, April 2018. 2018, REACH Initiative, UNICEF, WASH Cluster: ReliefWeb. Available online: https://reliefweb.int/sites/reliefweb.int/files/resources/reach_bgd_report_wash_hh_survey_april_2018_0.pdf (accessed on 30 July 2020).
- Branz, A.; Levine, M.; Lehmann, L.; Bastable, A.; Ali, S.I.; Kadir, K.; Yates, T.; Bloom, D.E.; Lantagne, D.S. Chlorination of drinking water in emergencies: A review of knowledge to develop recommendations for implementation and research needed. Waterlines 2017, 36, 4–39. [Google Scholar] [CrossRef]
- Lantagne, D.S.; Blount, B.C.; Cardinali, F.; Quick, R. Disinfection by-product formation and mitigation strategies in point-of-use chlorination of turbid and non-turbid waters in western Kenya. J. Water Health 2007, 6, 67–82. [Google Scholar] [CrossRef]
- Crider, Y.; Sultana, S.; Unicomb, L.; Davis, J.; Luby, S.P.; Pickering, A.J. Can you taste it? Taste detection and acceptability thresholds for chlorine residual in drinking water in Dhaka, Bangladesh. Sci. Total. Environ. 2018, 613, 840–846. [Google Scholar] [CrossRef]
- Cotruvo, J.A. 2017 WHO Guidelines for Drinking Water Quality: First Addendum to the Fourth Edition. J. Am. Water Work. Assoc. 2017, 109, 44–51. [Google Scholar] [CrossRef] [Green Version]
- Yates, T.; Vujcic, J.A.; Joseph, M.L.; Gallandat, K.; Lantagne, D. Efficacy and effectiveness of water, sanitation, and hygiene interventions in emergencies in low- and middle-income countries: A systematic review. Waterlines 2018, 37, 31–65. [Google Scholar] [CrossRef]
- Niederberger, E.; Glanville-Wallis, T. Community Engagement in WASH Emergencies: Understanding Barriers and Enablers Based on Action Research from Bangladesh and the Democratic Republic of Congo (DRC). Water 2019, 11, 862. [Google Scholar] [CrossRef] [Green Version]
- Oxfam. Bangladesh Rohingya Refugee Crisis. 2018. Available online: https://www.oxfam.org/en/what-we-do/emergencies/bangladesh-rohingya-refugee-crisis (accessed on 17 July 2020).
- Amin, N.; Crider, Y.S.; Unicomb, L.; Das, K.K.; Gope, P.S.; Mahmud, Z.H.; Islam, M.S.; Davis, J.; Luby, S.P.; Pickering, A.J. Field trial of an automated batch chlorinator system at shared water points in an urban community of Dhaka, Bangladesh. J. Water Sanit. Hyg. Dev. 2016, 6, 32–41. [Google Scholar] [CrossRef]
- Mitro, B.; Wolfe, M.; Galeano, M.; Sikder, M.; Gallandat, K.; Lantagne, D. Barriers and Facilitators to Chlorine Tablet Distribution and Use in Emergencies: A Qualitative Assessment. Water 2019, 11, 1121. [Google Scholar] [CrossRef] [Green Version]
- Doocy, S.; Burnham, G. Point-of-use water treatment and diarrhoea reduction in the emergency context: An effectiveness trial in Liberia. Trop. Med. Int. Health 2006, 11, 1542–1552. [Google Scholar] [CrossRef] [PubMed]
- Luby, S.P.; Keswick, B.H.; Hoekstra, R.M.; Mendoza, C.; Chiller, T.M. Difficulties in bringing point-of-use water treatment to scale in rural Guatemala. Am. J. Trop. Med. Hyg. 2008, 78, 382–387. [Google Scholar] [CrossRef] [PubMed]
- Luoto, J.; Najnin, N.; Mahmud, M.; Albert, J.; Islam, M.S.; Luby, S.P.; Unicomb, L.; Levine, D.I. What Point-of-Use Water Treatment Products Do Consumers Use? Evidence from a Randomized Controlled Trial among the Urban Poor in Bangladesh. PLoS ONE 2011, 6, e26132. [Google Scholar] [CrossRef] [Green Version]
- Olembo, L.; Kaona, F.; Tuba, M.; Burnham, G. Safe Water Systems: An Evaluation of the Zambia Clorin Program; Johns Hopkins University Mimeograph: Baltimore, MD, USA, 2004. [Google Scholar]
- Wu, H.; Dorea, C.C. Towards a Predictive Model for Initial Chlorine Dose in Humanitarian Emergencies. Water 2020, 12, 1506. [Google Scholar] [CrossRef]
- Gallandat, K.; Stack, D.; String, G.; Lantagne, D. Residual Maintenance Using Sodium Hypochlorite, Sodium Dichloroisocyanurate, and Chlorine Dioxide in Laboratory Waters of Varying Turbidity. Water 2019, 11, 1309. [Google Scholar] [CrossRef] [Green Version]
- Haq, Z.; Shaikh, B.T.; Tran, N.T.; Hafeez, A.; Ghaffar, A. System within systems: Challenges and opportunities for the Expanded Programme on Immunisation in Pakistan. Health Res. Policy Syst. 2019, 17, 51. [Google Scholar] [CrossRef] [Green Version]
- Basharat, S.; Shaikh, B.T. Polio immunization in Pakistan: Ethical issues and challenges. Public Health Rev. 2017, 38, 6. [Google Scholar] [CrossRef] [Green Version]
- Shakeel, S.I.; Brown, M.; Sethi, S.; Mackey, T.K. Achieving the end game: Employing “vaccine diplomacy” to eradicate polio in Pakistan. BMC Public Health 2019, 19, 79. [Google Scholar] [CrossRef]
- Government of People’s Republic of Bangladesh. Bangladesh Water Act. 2013; Government of People’s Republic of Bangladesh: Dhaka, Bangladesh, 2013.
- Ercumen, A.; Naser, A.M.; Unicomb, L.; Arnold, B.F.; Colford, J.M., Jr.; Luby, S.P. Effects of Source- versus Household Contamination of Tubewell Water on Child Diarrhea in Rural Bangladesh: A Randomized Controlled Trial. PLoS ONE 2015, 10, e0121907. [Google Scholar] [CrossRef]
- Enger, K.S.; Nelson, K.L.; Rose, J.B.; Eisenberg, J.N. The joint effects of efficacy and compliance: A study of household water treatment effectiveness against childhood diarrhea. Water Res. 2013, 47, 1181–1190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, J.; Clasen, T. High Adherence Is Necessary to Realize Health Gains from Water Quality Interventions. PLoS ONE 2012, 7, e36735. [Google Scholar] [CrossRef] [Green Version]
- Ramesh, A.; Blanchet, K.; Ensink, J.H.J.; Roberts, B. Evidence on the Effectiveness of Water, Sanitation, and Hygiene (WASH) Interventions on Health Outcomes in Humanitarian Crises: A Systematic Review. PLoS ONE 2015, 10, e0124688. [Google Scholar] [CrossRef]
- Rosa, G.; Huaylinos, M.L.; Gil, A.; Lanata, C.; Clasen, T. Assessing the Consistency and Microbiological Effectiveness of Household Water Treatment Practices by Urban and Rural Populations Claiming to Treat Their Water at Home: A Case Study in Peru. PLoS ONE 2014, 9, e114997. [Google Scholar] [CrossRef] [Green Version]
- Ali, S.I.; Fesselet, J.-F.; Ali, S.S. Effectiveness of emergency water treatment practices in refugee camps in South Sudan. Bull. World Health Organ. 2015, 93, 550–558. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Socio-Demographic Characteristics | Camp 4 | Camp 18 | Camp 22 | Camp 26 | Overall |
|---|---|---|---|---|---|
| Number of participants | 53 | 57 | 58 | 62 | 230 |
| Median age—Adult (in years) | 35 | 34 | 34 | 35 | 35 |
| Median age—Adolescents (in years) | 14 | 15 | 16 | 14 | 15 |
| Education: | n (%) | n (%) | n (%) | n (%) | n (%) |
| No formal education | 26 (49) | 28 (49) | 30 (52) | 36 (58) | 120 (52) |
| Grade 1 to 5 | 12 (23) | 14 (25) | 16 (28) | 18 (29) | 60 (26) |
| Grade 6 to 9 | 10 (19) | 11 (19) | 6 (10) | 6 (10) | 33 (14) |
| Grade 10 and above | 4 (8) | 3 (5) | 5 (9) | 1 (2) | 13 (6) |
| Hafez * | 1 (2) | 1 (2) | 1 (2) | 1 (2) | 4 (2) |
| Water sources: | n (%) | n (%) | n (%) | n (%) | n (%) |
| Shallow tubewell | 33 (85) | 22 (55) | 0 (0) | 5 (14) | 60 (38) |
| Deep tubewell | 6 (15) | 1 (2.5) | 0 (0) | 0 (0) | 7 (4.4) |
| Piped water chlorination | 0 (0) | 1 (2.5) | 19 (45) | 23 (62) | 43 (27) |
| Rain water | 0 (0) | 0 (0) | 7 (17) | 0 (0) | 7 (4.4) |
| Cisterns/well | 0 (0) | 0 (0) | 8 (19) | 0 (0) | 8 (5.1) |
| Small streams | 0 (0) | 3 (7.5) | 3 (7.1) | 9 (24) | 15 (9.5) |
| Puddles | 0 (0) | 3 (7.5) | 2 (4.8) | 0 (0) | 5 (3.2) |
| Canal | 0 (0) | 0 (0) | 3 (7.1) | 0 (0) | 3 (1.9) |
| Total water sources | 39 (100) | 40 (100) | 42 (100) | 37 (100) | 158 (100) |
| Indicators | Household Point of Use Water Treatment Using Chlorine Tablets | Piped Water Chlorination | Overall | ||
|---|---|---|---|---|---|
| Camp 4 | Camp 18 | Camp 22 | Camp 26 | ||
| N = 53n (%) | N = 57n (%) | N = 58n (%) | N = 62n (%) | N = 230n (%) | |
| Desired water characteristics: perception about clean water (multiple responses allowed): | |||||
| Looked clear | 10 (19) | 20 (35) | 15 (26) | 23 (37) | 68 (30) |
| Absence of iron | 15 (28) | 16 (28) | 18 (31) | 19 (31) | 68 (30) |
| Absence of small insects | 18 (34) | 17 (30) | 13 (22) | 12 (19) | 60 (26) |
| No bad smell | 15 (28) | 19 (33) | 12 (21) | 14 (23) | 60 (26) |
| No bad taste | 9 (17) | 12 (21) | 11 (19) | 14 (23) | 46 (20) |
| Desired water characteristics: perception about safe water (multiple responses allowed): | |||||
| Looked clear | 12 (23) | 10 (18) | 10 (17) | 11 (18) | 43 (19) |
| Absence of iron | 21 (40) | 20 (35) | 19 (33) | 18 (29) | 78 (34) |
| Absence of small insects | 18 (34) | 19 (33) | 11 (19) | 10 (16) | 58 (25) |
| No bad smell | 10 (19) | 16 (28) | 13 (22) | 13 (21) | 52 (23) |
| No bad taste | 11 (21) | 9 (16) | 8 (14) | 9 (15) | 37 (16) |
| Deep tubewell (>182 m) | 25 (47) | 20 (35) | 19 (33) | 18 (29) | 82 (36) |
| Any underground source | 15 (28) | 16 (28) | 14 (24) | 9 (15) | 54 (23) |
| Indicators | Camp 4 | Camp 18 | Camp 22 | Camp 26 | Overall | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Doers | Non-Doers | Doers | Non-Doers | Doers | Non-Doers | Doers | Non-Doers | Doers | Non-Doers | |
| N = 43n (%) | N = 10n (%) | N = 45n (%) | N = 12n (%) | N = 38n (%) | N = 20n (%) | N = 38n (%) | N = 24n (%) | N = 164n (%) | N = 66n (%) | |
| Barriers (multiple responses allowed): | ||||||||||
| Smells bad | 16 (37 | 10 (100) | 15 (33) | 12 (100) | 16 (42) | 18 (90) | 19 (50) | 21 (88) | 66 (40) | 61 (92) |
| Different taste | 16 (37) | 8 (80) | 12 (27) | 10 (83) | 16 (42) | 20 (100) | 16 (42) | 20 (83) | 60 (37) | 58 (88) |
| Inadequate supply | 8 (19) | 7 (70) | 0 | 12 (100) | 3 (8) | 7 (35) | 16 (42) | 18 (75) | 27 (16) | 44 (67) |
| Not habituated | 9 (21) | 8 (80) | 9 (20) | 11 (92) | 8 (21) | 15 (75) | 8 (21) | 17 (71) | 34 (21) | 51 (77) |
| Hair became sticky | 18 (19) | 10 (100) | 18 (40) | 10 (83) | 9 (24) | 16 (80) | 9 (24) | 18 (75) | 54 (33) | 54 (82) |
| Tablet is alive | 7 (16) | 10 (100) | 6 (13) | 10 (83) | 0 | 0 | 0 | 0 | 13 (8) | 20 (30) |
| Tattoo will be visible | 8 (19) | 9 (90) | 5 (11) | 9 (75) | 0 | 0 | 0 | 0 | 13 (8) | 18 (27) |
| Will become Christian | 6 (14) | 7 (70) | 6 (13) | 11 (92) | 0 | 3 (15) | 0 | 5 (21) | 12 (7) | 26 (39) |
| May causes death | 2 (5) | 9 (90) | 1 (2) | 9 (75) | 0 | 1 (5) | 0 | 1 (4) | 3 (2) | 20 (30) |
| Motivators (multiple responses allowed): | ||||||||||
| Kills insect/germs | 36 (84) | 3 (30) | 39 (87) | 5 (42) | 31 (82) | 15 (75) | 32 (84) | 12 (50) | 138 (84) | 35 (53) |
| Good for health | 25 (58) | 5 (50) | 31 (69) | 7 (58) | 36 (95) | 12 (60) | 35 (92) | 9 (38) | 127 (77) | 33 (50) |
| Cleans water | 23 (53) | 3 (30) | 21 (47) | 4 (33) | 33 (87) | 9 (45) | 33 (87) | 7 (29) | 110 (67) | 23 (35) |
| Removes iron | 16 (37) | 2 (20) | 18 (40) | 7 (58) | 27 (71) | 8 (40) | 12 (32) | 9 (38) | 73 (45) | 26 (39) |
| Prevents diseases | 29 (67) | 2 (20) | 28 (62) | 8 (67) | 26 (68) | 7 (35) | 29 (76) | 8 (33) | 112 (68) | 25 (38) |
| Indicators | Camp 4 | Camp 18 | Camp 22 | Camp 26 | All Samples | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Source (N = 6) | Stored Water (N = 26 | Source (N = 8) | Stored Water (N = 23) | Source (N = 7) | Stored Water (N = 34) | Source (N = 5) | Stored Water (N = 20) | Source (N = 26) | Stored Water (N = 103) | |
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |
| Turbidity (NTU): | ||||||||||
| <5 | 5 (83) | 17 (65) | 1 (13) | 5 (22) | 2 (29) | 13 (38) | 4 (80) | 18 (90) | 11 (42) | 62 (51) |
| Mean NTU (SD) | 5 (7.9) | 6.3 (8.2) | 1 (3.4) | 3 (2.9) | 14 (12) | 11.7 (11) | 5.5 (11) | 0.4 (2.9) | 5.1 (10) | 7.1 (10) |
| Free chlorine (mg/L): | ||||||||||
| <0.2 | 5 (83) | 26 (100) | 8 (100) | 19 (83) | 6 (86) | 28 (82) | 4 (80) | 19 (95) | 23 (88) | 111 (91) |
| 0.2–2 | 0 | 0 | 0 | 1 (4.4) | 0 | 6 (18) | 0 | 1 (5.0) | 0 | 8 (6.6) |
| Mean mg/L (SD) | 0.04 (0.04) | 0.05 (0.03) | 0.04 (0.02) | 0.59 (0.55) | 0.02 (0.01) | 0.14 (0.21) | 0.02 (0.02) | 0.08 (0.10) | 0.03 (0.03) | 0.09 (0.07) |
| Total chlorine (mg/L): | ||||||||||
| <0.2 | 5 (83) | 26 (100) | 8 (100) | 19 (83) | 6 (86) | 23 (68) | 4 (80) | 12 (60) | 23 (88) | 99 (81) |
| 0.2–2 | 0 | 0 | 0 | 1 (4.4) | 0 | 2 (5.9) | 0 | 8 (40) | 0 | 11 (9.0) |
| >2 | 1 (17) | 0 | 0 | 3 (13) | 1 (14) | 9 (26) | 1 (20) | 0 | 3 (11) | 12 (9.8) |
| Mean mg/L (SD) | 0.03 (0.05) | 0.02 (0.02) | 0.03 (0.02) | 0.61 (0.68) | 0.02 (0.01) | 1.5 (1.3) | 0.03 (0.03) | 0.21 (0.24) | 0.03 (0.03) | 0.57 (0.53) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alam, M.-U.; Unicomb, L.; Ahasan, S.M.M.; Amin, N.; Biswas, D.; Ferdous, S.; Afrin, A.; Sarker, S.; Rahman, M. Barriers and Enabling Factors for Central and Household Level Water Treatment in a Refugee Setting: A Mixed-Method Study among Rohingyas in Cox’s Bazar, Bangladesh. Water 2020, 12, 3149. https://doi.org/10.3390/w12113149
Alam M-U, Unicomb L, Ahasan SMM, Amin N, Biswas D, Ferdous S, Afrin A, Sarker S, Rahman M. Barriers and Enabling Factors for Central and Household Level Water Treatment in a Refugee Setting: A Mixed-Method Study among Rohingyas in Cox’s Bazar, Bangladesh. Water. 2020; 12(11):3149. https://doi.org/10.3390/w12113149
Chicago/Turabian StyleAlam, Mahbub-Ul, Leanne Unicomb, S.M. Monirul Ahasan, Nuhu Amin, Debashish Biswas, Sharika Ferdous, Ayesha Afrin, Supta Sarker, and Mahbubur Rahman. 2020. "Barriers and Enabling Factors for Central and Household Level Water Treatment in a Refugee Setting: A Mixed-Method Study among Rohingyas in Cox’s Bazar, Bangladesh" Water 12, no. 11: 3149. https://doi.org/10.3390/w12113149
APA StyleAlam, M.-U., Unicomb, L., Ahasan, S. M. M., Amin, N., Biswas, D., Ferdous, S., Afrin, A., Sarker, S., & Rahman, M. (2020). Barriers and Enabling Factors for Central and Household Level Water Treatment in a Refugee Setting: A Mixed-Method Study among Rohingyas in Cox’s Bazar, Bangladesh. Water, 12(11), 3149. https://doi.org/10.3390/w12113149