Abstract
Total knee arthroplasty (TKA) is widely used in clinical practice as an effective treatment for end-stage knee joint lesions. It can effectively correct joint deformities, relieve painful symptoms, and improve joint function. The reconstruction of lower extremity joint lines and soft tissue balance are important factors related to the durability of the implant; therefore, it is especially important to measure the joint lines and associated angles before TKA. In this article, we review the technological progress in the preoperative measurement of TKA.
1. Introduction
Total knee arthroplasty (TKA) is the most conclusive treatment for severe knee osteoarthritis, and its efficacy relies on the reconstruction of joint lines and soft tissue balance in the lower extremity. The reconstruction of the knee joint, among various structures in the human skeletal and soft tissue systems, is the most complex, for it requires the integration of anatomy, kinesiology, biomechanics, and even tissue engineering. In the reconstructed knee, it is important to take into account the reconstruction of joint lines, the soft tissue balance, and patellar tracking so as to achieve the “forgotten knee” status. The ultimate goal of accurate reconstruction is pursued by orthopaedic surgeons of all ages.
In order to achieve more accurate alignment, more perfect soft tissue balance, and better prosthesis matching so as to obtain longer prosthesis life, better postoperative function, and higher patient satisfaction, AI-assisted TKA preoperative design can accurately carry out preoperative planning, artificial intelligence segmentation, and key point recognition of joint CT data and establish standardized measurement model by adjusting the joint orientation. After introducing the open/closed wedge parameters or prosthesis parameters, one must accurately judge the shape parameters, such as the height and inclination of the osteotomy surface, and finally form a highly reliable surgical prediction model and simulate the postoperative image.
Therefore, thorough preoperative planning, that is, the measurement of joint lines and angles, helps guide the surgeon during the procedure. Preoperative measurements taken for TKA include traditional plain film radiographic measurements, digital templating, computer navigation, and artificial intelligence (AI) measurements. AI has multiple definitions and is largely agreed upon as the intelligence demonstrated by machines. In the field of computer science, AI research is defined as the study of “intelligent agents”, which are “devices that perceive the environment and act to maximize the achievement of a goal”. In a broad sense, process digitization, computer navigation, and robotics all fall into the category of AI. Existing AI-assisted technologies have enabled modern medicine to make great strides toward precision, intelligence, and individualization.
This article reviews the advances in AI-based preoperative measurement for TKA and the problems associated with various measurement techniques.
2. Traditional Plain Film Radiographic Measurements
In the past, preoperative measurements for TKA relied on traditional plain film radiographic measurements. Preoperatively, a full-length film of the patient’s bilateral lower extremities was taken in the standing position along with the anteroposterior (AP) and lateral views of the affected knee joint and an axial film of the patella. Further, the surgeons needed to manually trace the femoral anatomical axis, tibial axis, and lower limb joint lines on the full-length film of bilateral lower limbs to determine the valgus angle. The disadvantage of this type of film template measurement based on X-ray films is that the magnification of X-ray images varies among different hospitals, thus affecting the accuracy of measurements made using the same film template. The basis for testing the practical value of preoperative template measurements is that the results of different surveyors are consistent under different conditions [1,2]. Studies have shown that the inter- and intra-rater variability at different times are as high as 46.8% and 43.6%, respectively; thus, for the initial TKA, the accuracy and reproducibility of preoperative template measurements are not high [3]. Moreover, the quality of the preoperative imaging film also affects the accuracy of the measurements. Traditional film templates have a fixed magnification of 115–120%, which often does not match the actual radiographic magnification. In addition, due to differences in the body type and posture of the patients, it is difficult to ensure that the radiographs are obtained at a constant magnification and match the film template, especially in patients with severe knee osteoarthritis and flexion contracture. Moreover, if the patient has an extra-articular deformity on the femoral or tibial side, the only position for AP projection of both lower extremities is with the patella facing forward, which can result in human errors in determining the anatomical axes of the femur and tibia.
3. Digital Templating Measurements
The initial digital measurement is based on the measurement function that comes with each hospital’s medical imaging information system. These measurements require full-length films of both lower extremities, AP, and lateral knee films. Instead of traditional film measurements, computed tomography (CT) images of lower limbs need to be taken. The joint line and valgus angle of the lower extremity are measured in the same way as in conventional film measurements. The difference is that the medical imaging information system allows accurate labelling of the trans-epicondylar axis (TEA) and the Whiteside’s line based on CT images of the lower extremity at the selected knee level, and the external rotation angle in osteotomy can be determined by the posterior condylar line (PCL) of the knee. However, in the past, based on the preoperative CT markings of the TEA and the Whiteside’s line or the default 3° of external rotation for osteotomy, the intraoperative accuracy was 90%, 83%, and 70%, respectively.
The medical imaging information system allows only preoperative measurements of all angles but does not simulate the intraoperative knee osteotomy and the post-osteotomy prosthesis placement. In TKA, according to the isometric osteotomy method, the specific thickness of the osteotomy also affects the choice of the size of the prosthesis. The accuracy of the digital planning software in predicting the size of tibial prosthesis has been reported to be as low as 63%, and that in predicting the size of femoral prosthesis is 69% [4]. Schotanus et al. [5] similarly concluded that the outcome of digital preoperative planning was yet to be determined.
In the field of orthopaedic surgery, digital technology has made it possible to digitally simulate surgery. The CT scan of the patient’s knee joint, with a slice thickness of 1 mm, is obtained in the DICOM format, and the obtained data are input into the corresponding digital software to reconstruct a three-dimensional (3D) bony model of the knee joint. Further, calibrated weight-bearing full-length AP and lateral radiographs of the lower limb are taken, and the statistical shape model (SSM) technique is used to derive the 3D model of the knee joint. The 3D model is then automatically aligned with the CT-reconstructed bony 3D model of the knee joint to obtain a 3D spatial model of the knee joint and the full-length of bilateral lower limbs. After scanning all models of the selected prosthesis, the installation and alignment of the prosthesis are simulated on the 3D model using the measured joint lines and angles. The application of such digital simulation technology in the preoperative measurement of TKA has enabled the lower extremity joint line measurement and osteotomy and prosthesis installation to be more accurate, which is a great leap forward in joint surgery measurement technology. It has been confirmed [6,7] that the deviation of the SSM technique in fitting the knee joint is less than 0.2–0.4 mm, which can meet the rigorous standards required for clinical application.
5. Patient-Specific Instrumentation Measurement Technology
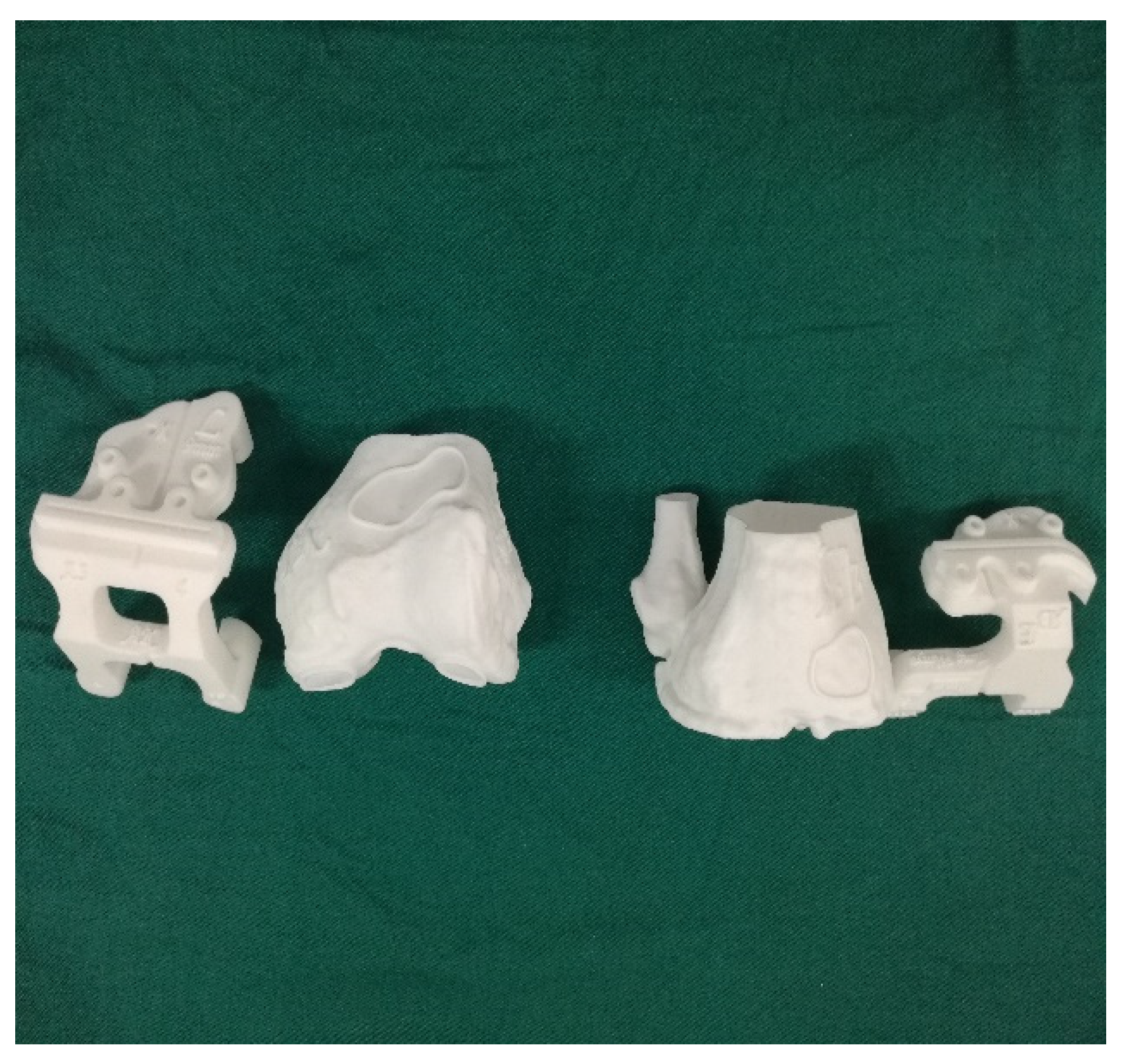
Some scholars do not support the inclusion of patient-specific instrumentation (PSI) under the category of artificial intelligence, though the authors do not agree with this view. PSI also requires data on the hip joint, knee joint, and ankle joint of the patient to be obtained through CT imaging, which are then digitally processed. The two-dimensional data are reconstructed into a 3D model, and then the corresponding osteotomy volume, angle, and prosthesis type are determined. After planning, the PSI is automatically generated, and the personalized osteotomy surgical guide is obtained via 3D printing technology (Figure 1 and Figure 2).
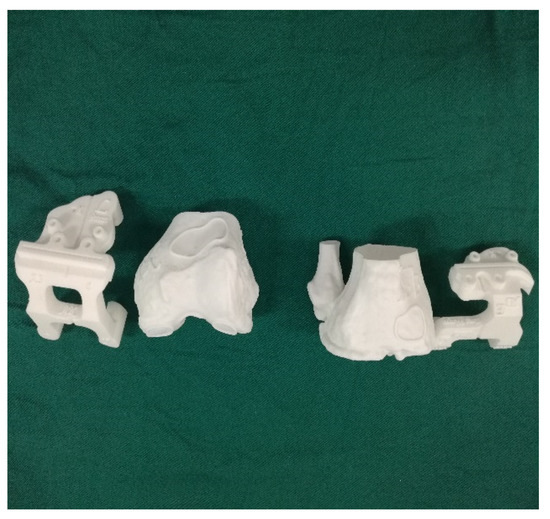
Figure 1.
3D printing pre-operative template.
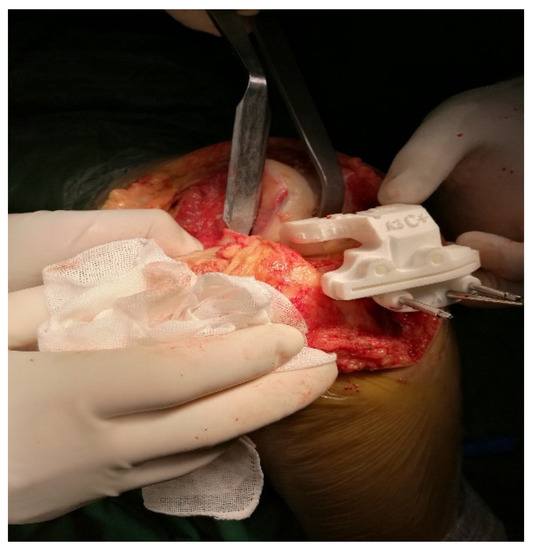
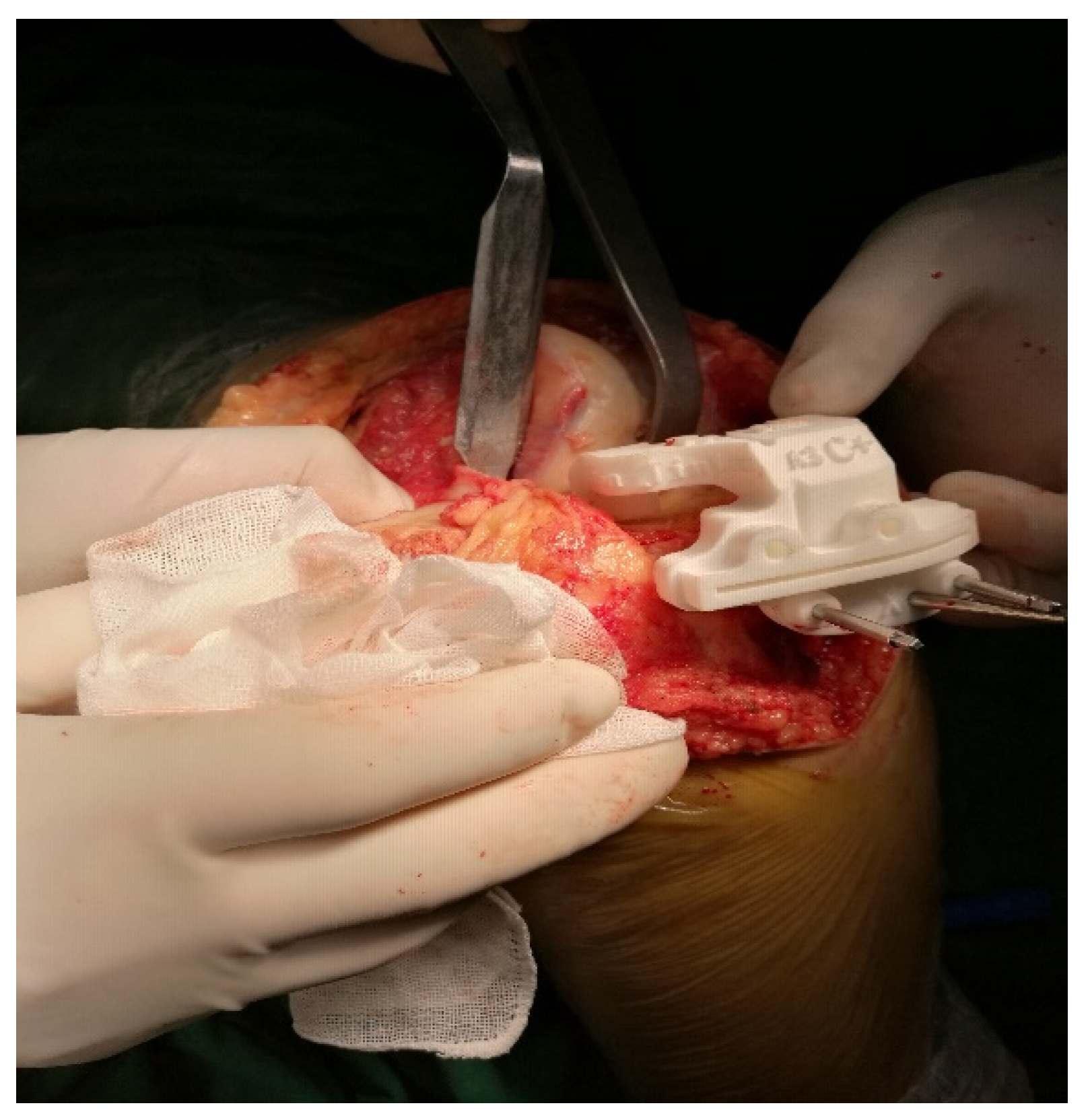
Figure 2.
Intraoperative application of 3D printing template.
Several studies have shown that the use of 3D-printed osteotomy guides can achieve favourable lower limb force lines during TKA [26,27], shorten the operation time, and achieve good results in controlling the femoral component rotation and tibial slope [28,29,30] and pre-operative planning of the required prosthesis type. However, TKA with PSI takes into account only the osteotomy aspect, while the soft tissue release and balance need to be controlled by the surgeons on the basis of their surgical experience. The PSI is based on CT and on bony landmarks. Intraoperatively, however, the guide may be inaccurately attached due to soft tissue coverage or obscuration. The future of this technique involves the inclusion of nuclear magnetic imaging.
6. Preoperative Planning of Robot-Assisted TKA
Before robot-assisted total knee arthroplasty, the AIHIP/KNEE software system was used in the preoperative planning of hip arthroplasty or knee arthroplasty. The system applies computer 3D data analysis based on CT or MRI, applies computer depth learning algorithm to segment joint CT data and identify key points, establishes a standardized measurement model, and then introduces prosthesis parameters to accurately judge parameters, such as osteotomy plane height and posterior inclination angle.
Institutions performing robotic research in China and abroad have explored the introduction of robotic surgery in arthroplasty, and the use of robot-assisted TKA systems is an historic moment. Robot-assisted TKA is currently the highest-level embodiment of artificial intelligence (AI) in knee surgery.
AI technology was once limited by basic hardware, barren databases, deficits of algorithms, and so on.
Alan Turing first invented artificial intelligence in 1950. He established the Turing test, which is the earliest prototype of AI. Turing proposed that the concept of AI technology is a computer algorithm similar to human brain intelligence, but at the same time, its complexity and efficiency are no less than or even higher than human brain intelligence. At that time, due to the backwardness of basic hardware equipment, poor databases, lack of algorithms, and other limitations, the development of AI technology was basically at a standstill. However, in recent years, the rapid development of computer technology and Internet technology has brought about the improvement of computer hardware, computing power, and large databases; thus, intelligent algorithms, such as machine learning, reinforcement learning and deep learning have gradually emerged, which have ushered in the great-leap-forward development of AI technology and produced several macro technical directions, such as computer vision, speech recognition, natural language recognition, decision planning, and big data analysis. Great breakthroughs have been made in the intelligent identification, understanding, and decision-making of data. During this period, many scholars published important works on AI (Table 1), and the important scientific discoveries in the development process of AI embodied important historical significance (Table 2).

Table 1.
Important AI publications.
Table 2.
AI scientific findings.
In recent years, the rapid development of computer technology and the internet have granted AI intelligent algorithms for machine learning, reinforcement learning, and deep learning, in particular, convolution neural networks, cyclic neural networks, and recurrent neural networks. AI technology has ushered in development by great leaps and is, thus, being widely used in joint surgery.
Robot-assisted preoperative planning system includes mainly high-precision 3D reconstruction based on CT and MRI images, image-based determination of preoperative osteotomy area and osteotomy plane, joint prosthesis design and preparation, preoperative joint line measurement, biomechanical analysis of the knee joint after prosthesis implantation, and so on. Current robotic systems can be divided into three categories according to their working modes: active, semi-active, and passive. The commonly used robot systems are shown in Table 3.
Table 3.
Robot systems (commonly used).
The active robot does not require manual operation and operates according to the preoperative plan. However, the system has potential surgical risks, and its working process needs to be monitored by the doctor throughout to avoid accidents. The semi-active robot, also called the haptic robot, is used to perform surgical planning before the operation, and during the operation, the surgeon completes the operation with the help of the robotic arm. Moreover, if the intraoperative osteotomy exceeds the preoperative planning range, the system gives feedback to the surgeon by means of a sound and force feedback, and the robotic arm automatically stops the operation, thus ensuring that the surgical path and the range are consistent with those planned preoperatively [31,32].
At present, several robotic-assisted arthroplasty surgery systems have been developed in the United States, Japan, Israel, and the United Kingdom, including the MARS surgical system developed by the Research Office of Mechanical Engineering Department in Israel [33], the 7-degree-of-freedom MIS-UKA system for robot-assisted orthopaedic surgery developed in collaboration with the University of Tokyo and Chiba University in Japan [34], and the ROBODOC (Figure 3) robot system developed by Integrated Surgical Systems Company in the United States [35]. Similarly, MAKOplasty is a semi-autonomous robotic system based on CT scanning and visual navigation developed by MAKO(Figure 4) [36], and ACROBOT is a semi-automatic TKA system developed by Imperial College Mechatronics in Medicine Laboratory, UK [37].

Figure 3.
ROBODOC.

Figure 4.
MAKO.
ROBODOC robots were first introduced for TKA in 2000, received FDA approval in 2008, and were renamed THINK robots in 2014. In addition to the ROBODOC and MAKO systems, there are also the NAVIO and iBlock systems. NAVIO is a handheld robot that can be manipulated by a surgeon [32]. The system was first approved by the FDA in 2012 for unicondylar replacement and patellar replacement and is now available for TKA. It does not require preoperative CT images and serves as an open robotic assist system for different prostheses from different manufacturers [32,38].
Currently, several hospitals in China are collaborating on the development of surgical robots for joint surgery. The computer-assisted orthopaedic surgery system, WATO, developed by the Department of Orthopaedics of Shanghai Changzheng Hospital and Shanghai Jiao Tong University Institute of Image Processing and Pattern Recognition in 2009, provides the surgeon with a surgical plan based on CT images before surgery, albeit with the disadvantage that the surgical incision is larger than that of conventional surgery [39]. The Gusheng Yuanhua Orthopaedic Surgery Robot, jointly developed by six hospitals, including the Department of Orthopaedics of the First Medical Centre of Chinese PLA General Hospital and Yuanhua Intelligent Technology (Shenzhen) Co., Ltd. (Heping Industrial Park, Heping Road, Yucui Community, Longhua Street, Longhua District, Shenzhen City, Guangdong Province, China) in 2020, also carries out preoperative planning on the basis of CT images when performing TKA. Notably, its human–machine interaction strategy is optimized with the habits of Chinese surgeons, and is, thus, more in line with the requirements of Chinese surgeons. Compared with the Mako robot, it is smaller in size and has a 7-degree-of-freedom manipulator with a larger range of motion and better flexibility. In addition, in 2021, the orthopaedic team of the Ninth People’s Hospital Affiliated with Shanghai Jiaotong University School of Medicine developed the Honghu orthopaedic surgical robot for TKA and reported five cases of TKA using the robot.
The significance of robot-assisted joint replacement is to greatly improve the accuracy of intraoperative operation, which benefits from three guarantees: (1) accurate measurement and planning of preoperative CT data; (2) the stable assistance of the mechanical arm during the operation; and (3) timely registration and monitoring during operation. The shortcomings and complications of early robotic joint surgery, after years of continuous correction and improvement, have no longer become the limiting factor of surgery.
It is generally accepted that excellent long-term postoperative results can be obtained when the postoperative knee varus or valgus is controlled within 3° after TKA surgery, but most of the current coronal lower extremity joint lines are controlled by relying on femoral intramedullary positioning and tibial extramedullary positioning. Further, the operation depends on the surgeon’s experience, which makes it difficult to achieve standardization and reproducibility of surgical outcomes. As can be seen from the above, the gradual deepening of the study of artificial intelligence has brought revolutionary changes in medicine, and concurrently, the preoperative planning of total knee arthroplasty in joint surgery is also moving towards the paradigm of precision medicine.
7. Conclusions
TKA requires accurate force line and soft tissue balance after operation. In order to achieve this goal, the planning of preoperative imaging of patients is particularly important. The application of computer-aided technology and artificial intelligence preoperative measurement can enable surgeons to control the osteotomy plane and angle more accurately. Although these advances have certain risks and disadvantages, in the field of joint surgery, AI assistance will still be the direction of future development and will also bring more breakthroughs.
Author Contributions
W.L., writing of the manuscript and conceptualization and design of the study; S.-M.X., investigation; D.-B.Z., investigation; H.-Y.B., resources; G.-S.G., guidance and review of manuscripts. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bothra, V.; Lemon, G.; Lang, D. Reliability of templating in estimating the size of uni-condylar knee arthroplasty. J. Arthroplast. 2003, 18, 780–783. [Google Scholar] [CrossRef]
- Kasis, A.G.; Pacheco, R.J.; Hekal, W.; Farhan, M.J.; Smith, D.M.; Ali, A.M. The precision and accuracy of templating the size of unicondylar knee arthroplasty. Knee 2004, 11, 395–398. [Google Scholar] [CrossRef]
- Arora, J.; Sharma, S.; Blyth, M. The role of pre-operative templating in primary total knee replacement. Knee Surg. Sport. Traumatol. Arthrosc. 2005, 13, 187–189. [Google Scholar] [CrossRef]
- Levine, B.; Fabi, D.; Deirmengian, C. Digital templating in primary total hip and knee arthroplasty. Orthopedics 2010, 33, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Schotanus, M.G.; Schoenmakers, D.A.; Sollie, R.; Kort, N.P. Patient-specific instruments for total knee arthroplasty can accurately predict the component size as used peroperative. Knee Surg. Sport. Traumatol. Arthrosc. 2017, 25, 3844–3848. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.; Li, G. Construction of 3D human distal femoral surface models using a 3D statistical deformable mode. J. Biomech. 2011, 44, 2362–2368. [Google Scholar] [CrossRef]
- Zheng, G.; Gollmer, S.; Schumann, S.; Dong, X.; Feilkas, T.; Ballester, M.A.G. A 2D/3D correspondence building method for reconstruction of a patient-specific 3D bone surface model using point distribution models and calibrated X-ray images. Med. Image Anal. 2009, 13, 883–899. [Google Scholar] [CrossRef]
- Du, H.; Zhang, J.; Tang, H.; Lv, M.; Zhou, Y.X. Observation on the effect of computer-assisted navigation artificial knee arthroplasty. Shandong Med. 2014, 54, 74–77. [Google Scholar]
- Mason, J.B.; Fehring, T.K.; Estok, R.; Banel, D.; Fahrbach, K. Meta-analysis of alignment outcomes in computer-assisted total knee arthroplasty surgery. J. Arthroplast. 2007, 22, 1097–1106. [Google Scholar] [CrossRef] [PubMed]
- Cheng, T.; Zhang, G.; Zhang, X. Imageless navigation system does not improve component rotational alignment in total knee arthroplasty. J. Surg. Res. 2011, 171, 590–600. [Google Scholar] [CrossRef]
- Zhao, L.; Xu, F.; Lao, S.; Zhao, J.; Wei, Q. Comparison of the clinical effects of computer-assisted and traditional techniques in bilateral total knee arthroplasty: A meta-analysis of randomized controlled trials. PLoS ONE 2020, 15, e0239341. [Google Scholar] [CrossRef] [PubMed]
- Stiehl, J.B.; Konermann, W.H.; Haaker, R.G.; Saragaglia, D.; Picard, F. Computer-assisted implantation of total knee endoprosthesis with no preoperative imaging: The kinematic model. Navig. Robot. Total Jt. Spine Surg. 2004, 22, 226–233. [Google Scholar]
- Eric, J.H. Computer-assisted orthopaedic surgery: A new paradigm. Tech. Orthop. 2003, 18, 221–229. [Google Scholar]
- Fehring, T.K.; Mason, J.B.; Moskal, J.; Pollock, D.C.; Mann, J.; Williams, V.J. When computer-assisted knee replacement is the best alternative. Clin. Orthop. Relat. Res. 2006, 452, 132–136. [Google Scholar] [CrossRef] [PubMed]
- Selvanayagam, R.; Kumar, V.; Malhotra, R.; Srivastava, D.N.; Digge, V.K. A prospective randomized study comparing navigation versus conventional total knee arthroplasty. J. Orthop. Surg. 2019, 27, 2309499019848079. [Google Scholar] [CrossRef]
- Hanada, M.; Furuhashi, H.; Matsuyama, Y. Investigation of the control of rotational alignment in the tibial component during total knee arthroplasty. Eur. J. Orthop. Surg. Traumatol. 2019, 29, 1313–1317. [Google Scholar] [CrossRef] [PubMed]
- Thiengwittayaporn, S.; Fusakul, Y.; Kangkano, N.; Jarupongprapa, C.; Charoenphandhu, N. Hand-held navigation may improve accuracy in minimally invasive total knee arthroplasty: A prospective randomized controlled trial. Int. Orthop. 2016, 40, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Goh, G.S.H.; Liow, M.H.L.; Lim, W.S.R.; Tay, D.K.J.; Yeo, S.J.; Tan, M.H. Accelerometer-based navigation is as accurate as optical computer navigation in restoring the joint line and mechanical axis after total knee arthroplasty: A prospective matched study. J. Arthroplast. 2016, 31, 92–97. [Google Scholar] [CrossRef]
- Iorio, R.; Mazza, D.; Drogo, P.; Bolle, G.; Conteduca, F.; Redler, A.; Ferretti, A. Clinical and radiographic outcomes of an accelerometer-based system for the tibial resection in total knee arthroplasty. Int. Orthop. 2015, 39, 461–466. [Google Scholar] [CrossRef]
- Nam, D.; Nawabi, D.H.; Cross, M.B.; Heyse, T.J.; Mayman, D.J. Accelerometer-based computer navigation for performing the distal femoral resection in total knee arthroplasty. J. Arthroplast. 2012, 27, 1717–1722. [Google Scholar] [CrossRef]
- Novoa-Parra, C.D.; Sanjuan-Cerveró, R.; Franco-Ferrando, N.; Larrainzar-Garijo, R.; Egea-Castro, G.; Lizaur-Utrilla, A. Complications of computer-assisted navigation in total knee replacement: Retrospective cohort of eight hundred and seventy eight consecutive knees. Int. Orthop. 2020, 44, 2621–2626. [Google Scholar] [CrossRef] [PubMed]
- Blue, M.; Douthit, C.; Dennison, J.; Caroom, C.; Jenkins, M. Periprosthetic fracture through a unicortical tracking pin site after computer navigated total knee replacement. Case Rep. Orthop. 2018, 2018, 2381406. [Google Scholar] [CrossRef]
- Kamara, E.; Berliner, Z.P.; Hepinstall, M.S.; Cooper, H.J. Pin site complications associated with computer-assisted navigation in hip and knee arthroplasty. J. Arthroplast. 2017, 32, 2842–2846. [Google Scholar] [CrossRef]
- Brown, M.J.; Matthews, J.R.; Bayers-Thering, M.T.; Phillips, M.J.; Krackow, K.A. Low incidence of postoperative complications with navigated total knee arthroplasty. J. Arthroplast. 2017, 32, 2120–2126. [Google Scholar] [CrossRef]
- Smith, T.J.; Siddiqi, A.; Forte, S.A.; Judice, A.; Sculco, P.K.; Vigdorchik, J.M.; Springer, B.D. Periprosthetic fractures through tracking pin sites following computer navigated and robotic total and unicompartmental knee arthroplasty: A systematic review. JBJ Rev. 2021, 9, e20.00091. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.Z.; Pei, G.X.; Lu, S.; Li, Z.J.; Zhao, J.M.; Wang, Y.W. Establishing lower-extremity mechanical axis by computer-aided design and its application in total knee arthroplasty. Chin. J. Orthop. 2013, 33, 1196–1203. [Google Scholar] [CrossRef]
- Levengood, G.A.; Dupee, J. Accuracy of coronal plane mechanical alignment in a customized, individually made total knee replacement with patient-specific instrumentation. J. Knee Surg. 2018, 31, 792–796. [Google Scholar] [CrossRef] [PubMed]
- Tian, S.C.; Yao, Q.Q.; Yin, X.D.; Liu, S.; Zhou, J.; Hu, J.; Wang, L.M. Effects of iASSIST navigation system and personal specific instrument assisted total knee arthroplasty in the treatment of osteoarthritis. Chin. J. Surg. 2017, 55, 423–429. [Google Scholar]
- Qiu, B.; Tang, B.S.; Deng, B.Y.; Liu, F.; Liu, F.; Zhen, D.; Zhu, W.M.; Zhang, M.J. Intelligentized surgery based on 3D printing technology for personalized total knee arthroplasty. Chin. J. Orthop. Trauma 2016, 18, 35–41. [Google Scholar] [CrossRef]
- Pauzenberger, L.; Munz, M.; Brandl, G.; Frank, J.K.; Heuberer, P.R.; Laky, B.; Anderl, W. Patient-specific instrumentation improved three-dimensional accuracy in total knee arthroplasty: A comparative radiographic analysis of 1257 to tall knee arthroplasties. J. Orthop. Surg. Res. 2019, 14, 437. [Google Scholar] [CrossRef] [PubMed]
- Netravali, N.A.; Shen, F.; Park, Y.; Bargar, W.L. A perspective on robotic assistance for knee arthroplasty. Adv. Orthop. 2013, 2013, 970703. [Google Scholar] [CrossRef] [PubMed]
- Jacofsky, D.J.; Allen, M. Robotics in Arthoplasty: A Comprehensive Review. J. Arthroplast. 2016, 31, 2353–2363. [Google Scholar] [CrossRef] [PubMed]
- Magnussen, R.A.; Trojani, C.; Granan, L.P.; Neyret, P.; Colombet, P.; Engebretsen, L.; SFA Revision ACL Group. Patient demographics and surgical characteristics in ACL revision: A comparison of French, Norwegian, and North American cohorts. Knee Surg. Sport. Traumatol. Arthrosc. 2015, 23, 2339–2348. [Google Scholar] [CrossRef]
- Seon, J.K.; Song, E.K.; Park, S.J. Comparison of minimally invasive unicompartmental knee arthroplasty with or without a navigation system. J. Arthroplast. 2009, 24, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Liow, M.H.L.; Chin, P.L.; Tay, K.J.D.; Chia, S.L.; Lo, N.N.; Yeo, S.J. Early experiences with robot-assisted total knee arthroplasty using the DigiMatch™ ROBODOC® surgical system. Singap. Med. J. 2014, 55, 529–534. [Google Scholar] [CrossRef]
- Dettmer, M.; Kreuzer, S.W. Bi-Unicompartmental, robot-assisted knee arthroplasty. Oper. Tech. Orthop. 2015, 25, 155–162. [Google Scholar] [CrossRef]
- Davies, B.; Jakopec, M.; Harris, S.J.; Baena, F.R.Y.; Barrett, A.; Evangelidis, A.; Cobb, J. Active-constraint robotics for surgery. Proc. IEEE 2006, 94, 1696–1704. [Google Scholar] [CrossRef]
- van der List, J.P.; Chawla, H.; Joskowicz, L.; Pearle, A.D. Current state of computer navigation and robotics in unicompartmental and total knee arthroplasty: A systematic review with meta-analysis. Knee Surg. Sport. Traumatol. Arthrosc. 2016, 24, 3482–3495. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.J.; Liu, Y.C. A new computer-assisted total knee arthroplasty system: WATO. Chin. Orthop. Jt. Surg. 2009, 2, 279283. [Google Scholar]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).