
Madelung’s Disease Evolving to Liposarcoma: An Uncommon Encounter
 , , , ,
, , , , 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
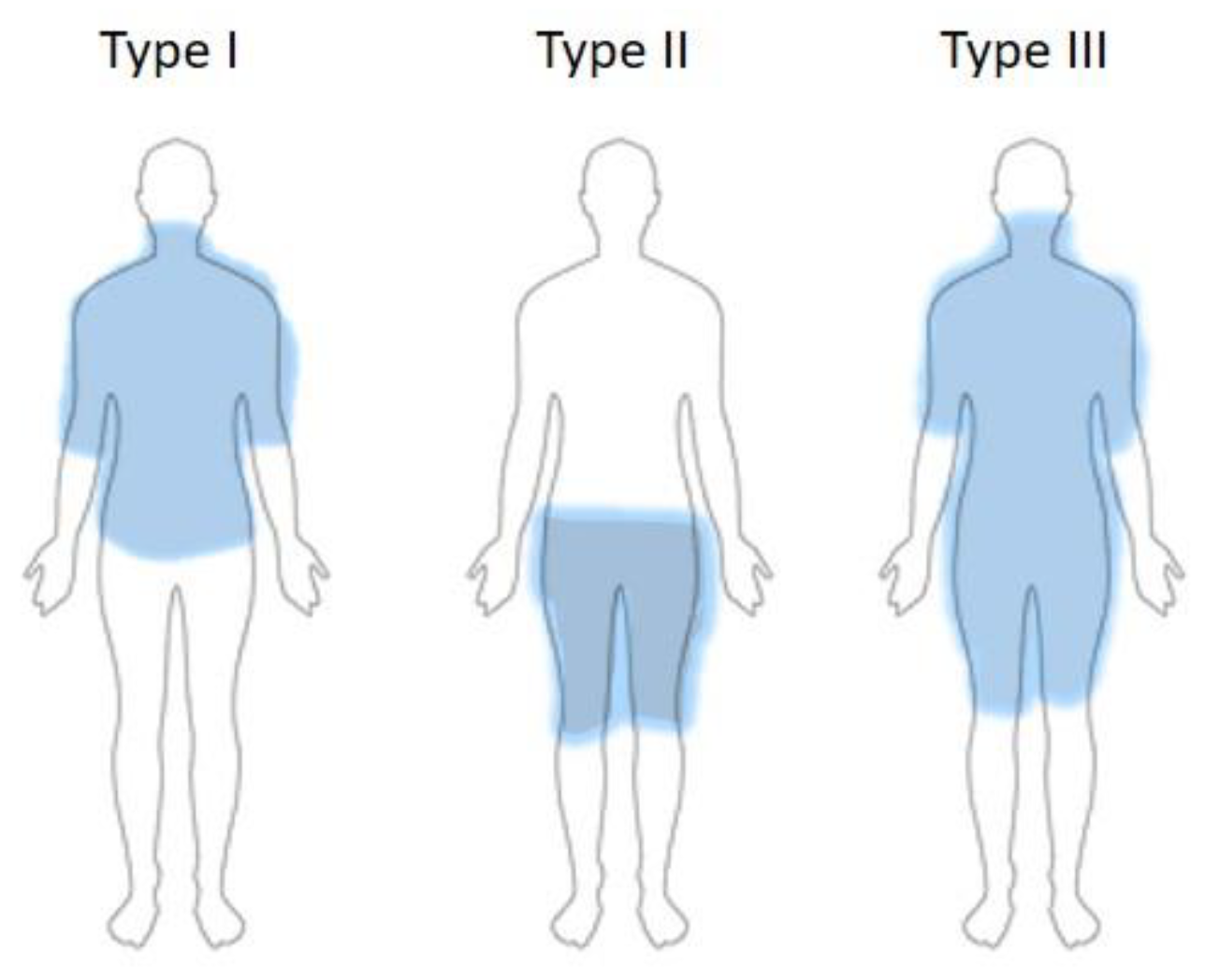
- Type I (Madelung horse collar)—localization of fatty masses in the cervical region, upper arms.
- Type II (Launois–Bensaude “pseudo-athletic type”)—affected body areas are upper arms, thorax, deltoid region; it does not appear to be connected to alcohol abuse.
- Type III (“gynecoid type”)—fat tissue masses located in the lower body, especially thighs and internal knee side.
- Type IV (“abdominal type”)—abdominal lipomatosis.
- Type Ia—fatty masses around the neck, corresponding to type I (D)—found in 3% in their study group.
- Type Ib—fatty masses on the neck, shoulders, and arms, corresponding to pseudoathletic type II (D)—in 4% of their cohort.
- Type Ic—as per Type Ib, but also including the trunk (new to Donhauser classification).
- Type II—lipomatosis in the lower part of the body, thighs, and pelvis, corresponding to type III (D).
- Type III—generalized disposition of the fatty masses, excluding the head, forearms, and lower legs.
2. Materials and Methods
3. Results
4. Discussion
4.1. Pathogenesis of BSA
4.2. Diagnosis of BSA
4.3. Differential Diagnosis, Comorbidities, and Malignant Transformation in BSA
4.4. Therapy of BSA
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brea-García, B.; Cameselle-Teijeiro, J.; Couto-González, I.; Taboada-Suárez, A.; González-Álvarez, E. Madelung’s disease: Comorbidities, fatty mass distribution, and response to treatment of 22 patients. Aesthetic Plast. Surg. 2013, 37, 409–416. [Google Scholar] [CrossRef]
- Pinto, C.I.; Carvalho, P.J.; Correia, M.M. Madelung’s Disease: Revision of 59 Surgical Cases. Aesthetic Plast. Surg. 2017, 41, 359–368. [Google Scholar] [CrossRef]
- Li, R.; Wang, C.; Bu, Q.; Pu, W.; Zhou, B.; Che, L.; Zhang, H.; Xu, Y.; Luan, H. Madelung’s Disease: Analysis of Clinical Characteristics, Fatty Mass Distribution, Comorbidities and Treatment of 54 Patients in China. Diabetes Metab. Syndr. Obes. 2022, 15, 2365–2375. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.M.; Li, W.Y.; Ni, D.F.; Wei, B.J.; Xu, C.X.; Gao, Z.Q.; He, L.; Chen, Y.N. Diagnosis and treatment of Madelung’s disease. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi (Chin. J. Otorhinolaryngol. Head Neck Surg.) 2006, 41, 524–527. [Google Scholar]
- Brodie, B. Clinical Lectures on Surgery: Delivered at St. George’s Hospital. West. J. Med. Surg. 1846, 5, 409–414. [Google Scholar] [CrossRef]
- Madelung, O.W. Über den Fetthals. Langenbecks Arch. Klin. Chir. Ver. Dtsch. Z. Chir. 1888, 37, 106–130. [Google Scholar]
- Launois, P.E.; Bensaude, R. De l’adéno-lipomatose symétrique. Bull. Mem. Soc. Med. Hop. Paris. 1898, 1, 289–318. [Google Scholar]
- Ruzicka, T.; Vieluf, D.; Landthaler, M.; Braun-Falco, O. Benign symmetric lipomatosis Launois-Bensaude. Report of ten cases and review of the literature. J. Am. Acad. Dermatol. 1987, 17, 663–674. [Google Scholar] [CrossRef] [PubMed]
- Grolleau, J.L.; Rouge, D.; Collin, J.F.; Micheau, P.; Chavoin, J.P.; Costagliola, M. Maladie de Launois Bensaude. Mise au point à propos de 16 cas [Launois Bensaude disease. Focus apropos of 16 cases]. Ann. Chir. Plast. Esthet. 1994, 38, 302–306. [Google Scholar]
- González-García, R.; Rodríguez-Campo, F.J.; Sastre-Pérez, J.; Muñoz-Guerra, M.F. Benign symmetric lipomatosis (Madelung’s disease): Case reports and current management. Aesthetic Plast. Surg. 2004, 28, 108–113. [Google Scholar] [CrossRef]
- Pauchot, J.; Golay, A.; Gumener, R.; Montandon, D.; Pittet, B. La maladie de Launois-Bensaude: Description, prise en charge. A propos de dix patients opérés [About 10 cases of Launois-Bensaude disease]. Ann. Chir. Plast. Esthet. 2009, 54, 135–145. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.S.; Wang, L.F.; Tsai, K.B.; Tai, C.F.; Kuo, W.R. Multiple symmetric lipomatosis (Madelung’s disease): Report of two cases. Kaohsiung J. Med. Sci. 2004, 20, 133–136. [Google Scholar] [CrossRef] [PubMed]
- Durand, J.; Thomine, J.; Tayrot, J.; Foucault, J. Liposarcome au cours d’une maladie de Launois-Bensaude. Rev. Rhum. Mal. Ostoartic 1973, 40, 287–291. [Google Scholar]
- Tizian, C.; Berger, A.; Vykoupil, K. Malignant degeneration in Madelung’s disease. Br. J. Plast. Surg. 1983, 36, 187–189. [Google Scholar] [CrossRef] [PubMed]
- Borriello, M.; Lucidi, A.; Carbone, A.; Iannone, V.; Ferrandina, G. Malignant transformation of Madelung’s disease in a patient with a coincidental diagnosis of breast cancer: A case report. Diagn. Pathol. 2012, 7, 116. [Google Scholar] [CrossRef] [PubMed]
- Schiltz, D.; Anker, A.; Ortner, C.; Tschernitz, S.; Koller, M.; Klein, S.; Felthaus, O.; Schreml, J.; Schreml, S.; Prante, L. Multiple Symmetric Lipomatose: New Classification System Based on the Largest German Patient Cohort. Plast. Reconstr. Surg.—Glob. Open 2018, 6, e1722. [Google Scholar] [PubMed]
- Plummer, C.; Spring, P.J.; Marotta, R.; Chin, J.; Taylor, G.; Sharpe, D.; Athanasou, N.A.; Thyagarajan, D.; Berkovic, S.F. Multiple symmetrical lipomatosis—A mitochondrial disorder of brown fat. Mitochondrion 2013, 13, 269–276. [Google Scholar] [CrossRef] [PubMed]
- Gámez, J.; Playán, A.; Andreu, A.L.; Bruno, C.; Navaro, C.; Cervera, C.; Arbós, M.A.; Schwartz, S.; Enriquez, J.A.; Montoya, J. Familial multiple symmetric lipomatosis associated with the A8344G mutation of mitochondrial DNA. Neurology 1998, 51, 258–260. [Google Scholar] [CrossRef] [PubMed]
- Medappil, N.; Vasu, T.A. Madelung’s disease: A spot diagnosis. Indian J. Plast. Surg. 2010, 43, 227–228. [Google Scholar] [CrossRef]
- Prahlow, S.P.; Kosciuk, P.; Prahlow, J.A. Multiple symmetric lipomatosis. J. Forensic Sci. 2018, 63, 312–315. [Google Scholar] [CrossRef]
- Sawyer, S.L.; Cheuk-Him Ng, A.; Innes, A.M.; Wagner, J.D.; Dyment, D.A.; Tetreault, M.; Care4Rare Canada Consortium; Majewski, J.; Boycott, K.M.; Screaton, R.A.; et al. Homozygous mutations in MFN2 cause multiple symmetric lipomatosis associated with neuropathy. Hum. Mol. Genet. 2015, 24, 5109–5114. [Google Scholar] [CrossRef] [PubMed]
- Perera, U.; Kennedy, B.A.; Hegele, R.A. Multiple Symmetric Lipomatosis (Madelung Disease) in a Large Canadian Family With the Mitochondrial MTTK c. 8344A> G Variant. J. Investig. Med. High Impact Case Rep. 2018, 6, 2324709618802867. [Google Scholar] [CrossRef] [PubMed]
- Klopstock, T.; Naumann, M.; Seibel, P.; Shalke, B.; Reiners, K.; Reichmann, H. Mitochondrial DNA mutations in multiple symmetric lipomatosis. Mol. Cell Biochem. 1997, 174, 271–275. [Google Scholar] [CrossRef] [PubMed]
- Ujpal, M.; Nemeth, Z.S.; Reichwein, A.; Szabo, G.Z. Long-term results following surgical treatment of benign symmetric lipomatosis. Int. J. Oral. Maxillofac. Surg. 2001, 30, 479–483. [Google Scholar] [CrossRef] [PubMed]
- Enzi, G.; Inelmen, E.M.; Baritussio, A.; Dorigo, P.; Prosdomici, M.; Mazzoleni, F. Multiple symmetric lipomatosis: A defect in adrenergic-stimulated lipolysis. J. Clin. Investig. 1977, 60, 1221–1229. [Google Scholar] [CrossRef] [PubMed]
- Enzi, G.; Busetto, L.; Ceschin, E.; Coin, A.; Digito, M.; Pigozzo, S. Multiple symmetric lipomatosis: Clinical aspects and outcome in a long-term longitudinal study. Int. J. Obes. Relat. Metab. Disord. 2002, 26, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Donhauser, G.; Vieluf, D.; Ruzicka, T.; Braun-Falco, O. [Benign symmetric Launois-Bensaude type III lipomatosis and Bureau-Barrière syndrome]. Hautarzt 1991, 42, 311–314. [Google Scholar] [PubMed]
- Jung, K.; Lee, S. A case report of Multiple Symmetric Lipomatosis (MSL) in an East Asian Female. BMC Womens Health 2020, 20, 200. [Google Scholar] [CrossRef] [PubMed]
- Rebegea, L.; Firescu, D.; Baciu, G.; Ciubara, A. Psycho-Oncology Support. Brain 2019, 10, 77–88. [Google Scholar]
- Schiltz, D.; Mueller, K.; Ortner, C.; Tschernitz, S.; Anker, A.; Felthaus, O.; Schreml, J.; Koller, M.; Prantl, L.; Schreml, S. Multiple Symmetric Lipomatosis: A Cross-Sectional Study to Investigate Clinical Features and Patients’ Quality of Life. Symmetry 2021, 13, 1823. [Google Scholar] [CrossRef]
- Becerra-Bolaños, Á.; Valencia, L.; Cabrera-Ramírez, L.; Rodriguez-Perez, A. Madelung’s disease and airway management. Anesthesiology 2019, 130, 313. [Google Scholar] [CrossRef] [PubMed]
- Suito, M.; Kitazawa, T.; Takashimizu, I.; Ikeda, T. Madelung’s disease: Long-term follow-up. J. Surg. Case Rep. 2019, 2019, rjy356. [Google Scholar] [CrossRef]
- Zolotov, S.; Xing, C.; Mahamid, R.; Shalata, A.; Sheikh-Ahmad, M.; Garg, A. Homozygous LIPE mutation in siblings with multiple symmetric lipomatosis, partial lipodystrophy, and myopathy. Am. J. Med. Genet. A 2017, 173, 190–194. [Google Scholar] [CrossRef] [PubMed]
- Chong, P.S.; Vucic, S.; Hedley-Whyte, E.T.; Dreyer, M.; Cros, D. Multiple Symmetric Lipomatosis (Madelung’s Disease) Caused by the MERRF (A8344G) Mutation: A Report of Two Cases and Review of the Literature. J. Clin. Neuromuscul. Dis. 2003, 5, 1–7. [Google Scholar] [CrossRef]
- Campos, Y.; Martin, M.A.; Navarro, C.; Gordo, P.; Arenas, J. Single large-scale mitochondrial DNA deletion in a patient with mitochondrial myopathy associated with multiple symmetric lipomatosis. Neurology 1996, 47, 1012–1014. [Google Scholar] [CrossRef] [PubMed]
- Pasmatzi, E.; Monastirli, A.; Chroni, E.; Georgiou, S.; Habeos, J.; Stefanou, E.G.; Fratter, C.; Papathanasopoulos, P.; Tsambaos, D. Multiple symmetric lipomatosis type I in a female patient with neuropathy: No association with alcoholism or mitochondrial DNA m.8344A>G mutation. QJM Int. J. Med. 2015, 108, 503–505. [Google Scholar] [CrossRef][Green Version]
- Schiller, H. Lipomata in sarcomatous transformation. Surg. Gynecol. Obstet. 1918, 27, 218–219. [Google Scholar]
- Wright, C.J.E. Liposarcoma arising in a simple lipoma. J. Pathol. Bacteriol. 1948, 60, 483. [Google Scholar] [CrossRef]
- Sternberg, S.S. Liposarcoma arising within a subcutaneous lipoma. Cancer 1952, 5, 975–978. [Google Scholar] [CrossRef]
- Sampson, C.C.; Saunders, E.H.; Green, W.E.; Laurey, J.R. Liposarcoma developing in a lipoma. Arch. Pathol. 1960, 69, 506–510. [Google Scholar]
- Zancanaro, C. Multiple symmetric lipomatosis- ultrastructural investigation of the tissue and preadipocytes in primary culture. Lab. Investig. 1990, 63, 253–258. [Google Scholar] [PubMed]
- Hengel, R.L.; Watts, N.B.; Lennox, J.I. Benign symmetric lipomatosis associated with protease inhibitors. Lancet 1997, 350, 1596. [Google Scholar] [CrossRef] [PubMed]
- Fischer, T.; Schwörer, H.; Ramadori, G. Benign symmetrical lipomatosis (peripheral lipodystrophy) during antiretroviral treatment of HIV infection. Dtsch. Med. Wochenschr. 1998, 123, 1512–1518. [Google Scholar] [CrossRef] [PubMed]
- Grunfeld, C. Lipids, lipoproteins, tryglicerid clearance and cytokines in human immunodeficiency virus infection. J. Din. Endocrin. 1993, 74, 1045–1052. [Google Scholar]
- Jaźwiec, P.; Pawłowska, M.; Czerwińska, K.; Poręba, M.; Gać, P.; Poręba, R. Madelung’s Disease as an Example of a Metabolic Disease Associated with Alcohol Abuse—Diagnostic Importance of Computed Tomography. Int. J. Environ. Res. Public Health 2022, 19, 5168. [Google Scholar] [CrossRef] [PubMed]
- Rebegea, L.F.; Firescu, D.; Dumitru, M.; Patrascu, A. Skin spiradenocarcinoma—Case presentation. Rom. J. Morphol. Embryol. 2016, 57, 327–330. [Google Scholar] [PubMed]
- Sedaghat, S.; Sedaghat, M.; Krohn, S.; Jansen, O.; Freund, K.; Streitbürger, A.; Reichardt, B. Long-term diagnostic value of MRI in detecting recurrent aggressive fibromatosis at two multidisciplinary sarcoma centers. Eur. J. Radiol. 2021, 134, 109406. [Google Scholar] [CrossRef] [PubMed]
- Sedaghat, S.; Sedaghat, M.; Meschede, J.; Jansen, O.; Both, M. Diagnostic value of MRI for detecting recurrent soft-tissue sarcoma in a long-term analysis at a multidisciplinary sarcoma center. BMC Cancer 2021, 21, 398. [Google Scholar] [CrossRef] [PubMed]
- Constantinidis, J.; Steinhart, H.; Zenk, J.; Bohlender, J.; Iro, H. Surgical therapy of Madelung’s disease in the head and neck area. HNO 2003, 51, 216–220. [Google Scholar] [CrossRef]
- Cojocaru, D.C.; Dima Cozma, C.; Postolache, P. Markers of insulin resistance in a case of Launois-Bensaude syndrome. Rev. Med. Chir. Soc. Med. Nat. Iasi 2013, 117, 404–408. [Google Scholar]
- Bejan, C.; Matei, M.N.; Dorobat, C.; Juganariu, G.; Dorobat, G.; Constantinescu, S.; Nechita, A.; Earar, K. Biochemical Features in Hepato-renal Dysfunctions. Rev. Chim. Bucharest 2015, 66, 282–284. [Google Scholar]
- Ohkura, N.; Sakaguchi, S. Transcriptional and epigenetic basis of Treg cell development and function: Its genetic anomalies or variations in autoimmune diseases. Cell Res. 2020, 30, 465–474. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, M.; Beal, B.T.; Khetarpal, S.; Vidimos, A. Madelung Disease Treated With Deoxycholic Acid. Dermatol. Surg. 2021, 47, 879–880. [Google Scholar] [CrossRef] [PubMed]
- Scevola, S.; Nicoletti, G.; Neri, A.; Faga, A. Long term assessment of intralipotherapy in Madelung’s disease. Indian J. Plast. Surg. 2014, 47, 427–431. [Google Scholar] [CrossRef] [PubMed]
- So, T.; Ishii, N. The TNF–TNFR Family of Co-signal Molecules. In Co-Signal Molecules in T Cell Activation; Azuma, M., Yagita, H., Eds.; Advances in Experimental Medicine and Biology; Springer: Singapore, 2019; Volume 1189. [Google Scholar] [CrossRef]
- Sanna, M.; Borgo, C.; Compagnin, C.; Favaretto, F.; Vindigni, V.; Trento, M.; Bettini, S.; Comin, A.; Belligoli, A.; Rugge, M.; et al. White Adipose Tissue Expansion in Multiple Symmetric Lipomatosis Is Associated with Upregulation of CK2, AKT and ERK1/2. Int. J. Mol. Sci. 2020, 21, 7933. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Ma, S.; Cai, D.; Wang, C.; Yu, H.; Xie, J.; Cheng, W. Analysis of Madelung disease based on sc-RNA sequencing: A case report and literature review. Mol. Immunol. 2023, 157, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Caponnetto, F.; Manini, I.; Bulfoni, M.; Zingaretti, N.; Miotti, G.; Di Loreto, C.; Cesselli, D.; Mariuzzi, L.; Parodi, P.C. Human adipose-derived stem cells in Madelung’s disease: Morphological and functional characterization. Cells 2020, 10, 44. [Google Scholar] [CrossRef] [PubMed]
- El Ouahabi, H.; Doubi, S.; Lahlou, K.; Boujraf, S.; Ajdi, F. Launois-bensaude syndrome: A benign symmetric lipomatosis without alcohol association. Ann. Afr. Med. 2017, 16, 33. [Google Scholar] [PubMed]
- Liu, J.; Li, J.; Wang, K.; Liu, H.; Sun, J.; Zhao, X.; Yu, Y.; Qiao, Y.; Wu, Y.; Zhang, X.; et al. Aberrantly high activation of a FoxM1–STMN1 axis contributes to progression and tumorigenesis in FoxM1-driven cancers. Signal Transduct. Target. Ther. 2021, 6, 42. [Google Scholar] [CrossRef]
- Szewc, M.; Sitarz, R.; Moroz, N.; Maciejewski, R.; Wierzbicki, R. Madelung’s disease–progressive, excessive, and symmetrical deposition of adipose tissue in the subcutaneous layer: Case report and literature review. Diabetes Metab. Syndr. Obes. Targets Ther. 2018, 11, 819–825. [Google Scholar] [CrossRef]
- Tawara, J.; Ishizuka, K.; Enomoto, K.; Kamata, M.; Katayama, K.; Kaji, Y.; Ohira, Y. Madelung Disease. Am. J. Med. 2022, 135, e214–e215. [Google Scholar] [CrossRef]
- Hirose, A.; Okada, Y.; Morita, E.; Tanaka, Y. Benign symmetric lipomatosis associated with alcoholism. Intern. Med. 2006, 45, 1001–1005. [Google Scholar] [CrossRef] [PubMed]
- Şükün, A.; Demirci, M.F.; Akbay, E. Type 1C Multiple Symmetrical Lipomatosis: A Cause of Misdiagnosis in Females. Cureus 2023, 15, e40970. [Google Scholar] [CrossRef]
- Vassallo, G.A.; Mirijello, A.; Tarli, C.; Rando, M.M.; Antonelli, M.; Garcovich, M.; Zocco, M.A.; Sestito, L.; Mosoni, C.; Dionisi, T.; et al. Madelung’s disease and acute alcoholic hepatitis: Case report and review of literature. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 6272–6276. [Google Scholar]
- Herbst, K.L. Rare adipose disorders (RADs) masquerading as obesity. Acta Pharmacol. Sin. 2012, 33, 155–172. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.; Gu, L.; Liu, K. Madelung’s disease with fibrolipoma in the neck: A case report. Chin. J. Otorhinolaryngol. Head Neck Surg. 2020, 55, 792–794. [Google Scholar]
- Xing, X.; Yang, F.; Huang, Q.; Guo, H.; Li, J.; Qiu, M.; Bai, F.; Wang, J. Decoding the multicellular ecosystem of lung adenocarcinoma manifested as pulmonary subsolid nodules by single-cell RNA sequencing. Sci. Adv. 2021, 7, eabd9738. [Google Scholar] [CrossRef] [PubMed]
- Ardeleanu, V.; Jecan, R.C.; Moroianu, M.; Teodoreanu, R.N.; Tebeica, T.; Moroianu, L.A.; Bujoreanu, F.C.; Nwabudike, L.C.; Tatu, A.L. Case report: Abrikossoff’s tumor of the facial skin. Front. Med. 2023, 10, 1149735. [Google Scholar] [CrossRef]
- Branisteanu, D.E.; Pintilie, A.; Dumitriu, A.; Cerbu, A.; Ciobanu, D.; Oanta, A.; Tatu, A.L. Clinical, laboratory and therapeutic profile of lichen planus. Med.-Surg. J. 2017, 121, 25–32. [Google Scholar]
- Lee, Y.J.; Jeong, Y.J.; Lee, J.H.; Jun, Y.J.; Kim, Y.J. Liposarcoma in the axilla developed from a longstanding lipoma. Arch. Plast. Surg. 2014, 41, 600–602. [Google Scholar] [CrossRef][Green Version]
- Nwabudike, L.C.; Tatu, A.L. Reply to Happle R. et al. Koebner’s sheep in Wolf’s clothing: Does the isotopic response exists as a distinct phenomenon? J. Eur. Acad. Dermatol. Venereol. 2018, 32, e336–e337. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Lyu, H.; Xu, B.; Lee, J.H. Madelung Disease Epidemiology and Clinical Characteristics: A Systemic Review. Aesthetic Plast. Surg. 2021, 45, 977–986. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.Y.; Fang, Q.Q.; Wang, X.F.; Zhang, M.X.; Zhao, W.Y.; Shi, B.H.; Wu, L.H.; Zhang, L.Y.; Tan, W.Q. Madelung’s disease: Lipectomy or liposuction? Biomed. Res. Int. 2018, 2018, 3975974. [Google Scholar] [CrossRef] [PubMed]
- Leung, N.W.; Gaer, J.; Beggs, D.; Kark, A.E.; Holloway, B.; Peters, T.J. Multiple symmetrical Lipomatosis: Effect of oral salbutamol. Clin. Endocrinol. 1987, 27, 601–606. [Google Scholar] [CrossRef]
- Jung, H. Hyaluronidase: An overview of its properties, applications, and side effects. Arch. Plast. Surg. 2020, 47, 297–300. [Google Scholar] [CrossRef]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lungu, M.; Oprea, V.D.; Stoleriu, G.; Ionescu, A.-M.; Zaharia, A.L.; Croitoru, A.; Stan, B.; Niculet, E. Madelung’s Disease Evolving to Liposarcoma: An Uncommon Encounter. Life 2024, 14, 521. https://doi.org/10.3390/life14040521
Lungu M, Oprea VD, Stoleriu G, Ionescu A-M, Zaharia AL, Croitoru A, Stan B, Niculet E. Madelung’s Disease Evolving to Liposarcoma: An Uncommon Encounter. Life. 2024; 14(4):521. https://doi.org/10.3390/life14040521
Chicago/Turabian StyleLungu, Mihaiela, Violeta Diana Oprea, Gabriela Stoleriu, Ana-Maria Ionescu, Andrei Lucian Zaharia, Ana Croitoru, Bianca Stan, and Elena Niculet. 2024. "Madelung’s Disease Evolving to Liposarcoma: An Uncommon Encounter" Life 14, no. 4: 521. https://doi.org/10.3390/life14040521
APA StyleLungu, M., Oprea, V. D., Stoleriu, G., Ionescu, A.-M., Zaharia, A. L., Croitoru, A., Stan, B., & Niculet, E. (2024). Madelung’s Disease Evolving to Liposarcoma: An Uncommon Encounter. Life, 14(4), 521. https://doi.org/10.3390/life14040521