
Predictive Prognostic Factors in Non-Calcific Supraspinatus Tendinopathy Treated with Focused Extracorporeal Shock Wave Therapy: An Artificial Neural Network Approach

 ,
, 

 ,
,  ,
,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
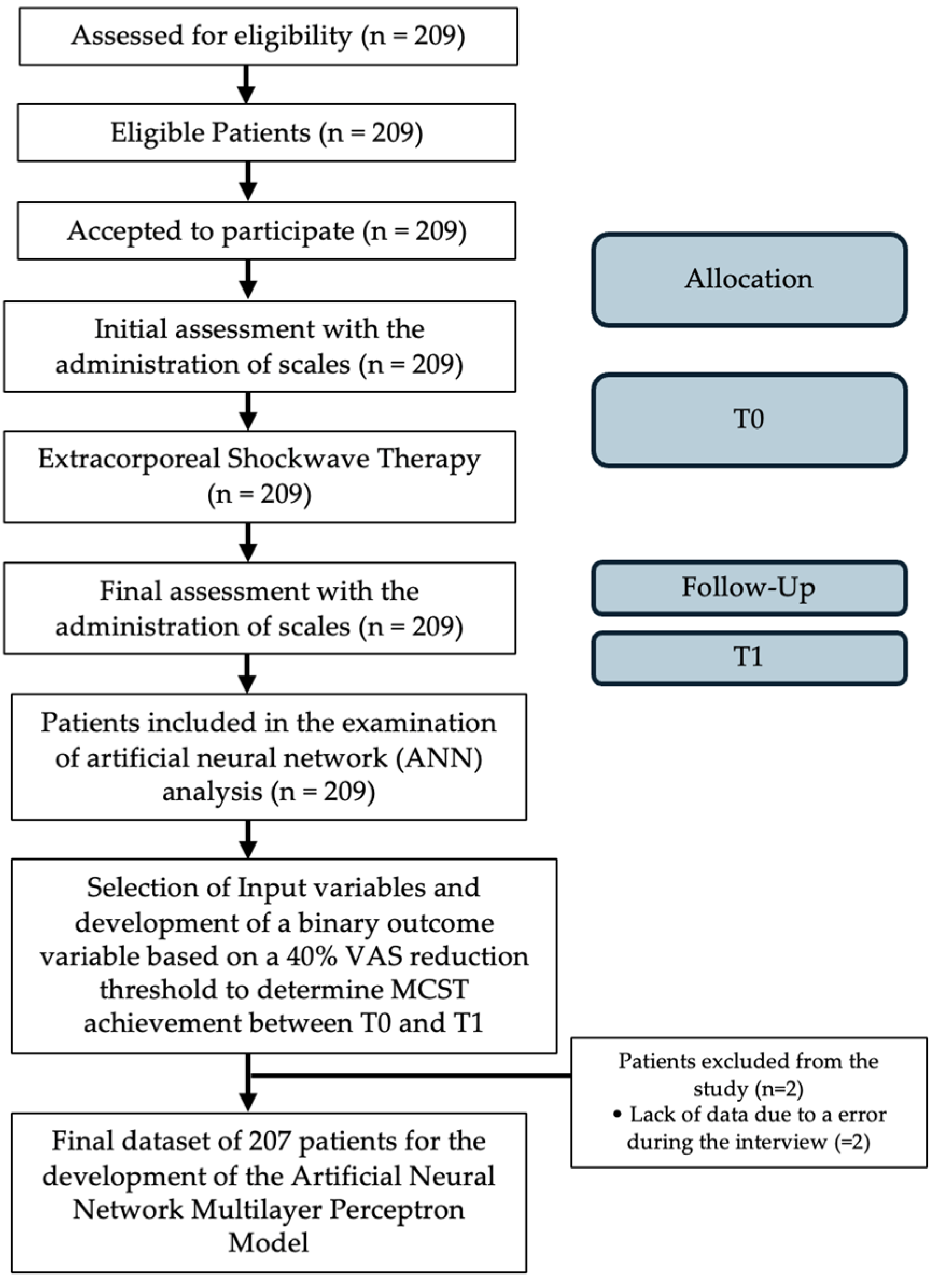
2.1. Study Design and Population
2.2. Intervention
Outcomes
2.3. Artificial Neural Networks
2.4. Statistical Analysis
3. Results
3.1. Patient Demographic and Clinical Characteristics
3.2. ANN Model Analysis
3.3. Accuracy of the Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AI | Artificial intelligence |
| ANN | Artificial neural network |
| CMS | Constant and Murley score |
| DM | Data mining |
| ESWT | Extracorporeal shockwave therapy |
| MLP | Multilayer perceptron |
| RM | Roles and Maudsley Scale |
| RC | Rotator cuff |
| SP | Supraspinatus tendon |
| SNCCT | Supraspinatus non-calcific tendinopathy |
| VAS | Visual Analogue Scale |
References
- Varacallo, M.; El Bitar, Y.; Mair, S.D. Rotator Cuff Syndrome; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Spargoli, G. Supraspinatus tendon pathomechanics: A current concepts review. Int. J. Sports Phys. Ther. 2018, 13, 1083–1094. [Google Scholar] [CrossRef] [PubMed]
- Merolla, G.; Singh, S.; Paladini, P.; Porcellini, G. Calcific tendinitis of the rotator cuff: State of the art in diagnosis and treatment. J. Orthop. Traumatol. 2016, 17, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Chianca, V.; Albano, D.; Messina, C.; Midiri, F.; Mauri, G.; Aliprandi, A.; Catapano, M.; Pescatori, L.C.; Monaco, C.G.; Gitto, S.; et al. Rotator cuff calcific tendinopathy: From diagnosis to treatment. Acta Biomed. 2018, 89, 186–196. [Google Scholar] [PubMed]
- Kaux, J.F.; Forthomme, B.; Goff, C.L.; Crielaard, J.M.; Croisier, J.L. Current opinions on tendinopathy. J. Sports Sci. Med. 2011, 10, 238–253. [Google Scholar] [PubMed]
- Del Buono, A.; Battery, L.; Denaro, V.; Maccauro, G.; Maffulli, N. Tendinopathy and inflammation: Some truths. Int. J. Immunopathol. Pharmacol. 2011, 24 (Suppl. 2), 45–50. [Google Scholar] [CrossRef] [PubMed]
- Riley, G. Tendinopathy—From basic science to treatment. Nat. Clin. Pr. Rheumatol. 2008, 4, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Seitz, A.L.; McClure, P.W.; Finucane, S.; Boardman, N.D., 3rd; Michener, L.A. Mechanisms of rotator cuff tendinopathy: Intrinsic, extrinsic, or both? Clin. Biomech 2011, 26, 1–12. [Google Scholar] [CrossRef]
- Moreno-Fernandez, J.M.; Martinez-Martinez, F.; Santonja- Medina, F. Inter-Observer Reliability of Physical Examination in the Painful Shoulder: Supraspinatus Tendinopathy. Arch. Sports Med. 2019, 3, 129–133. [Google Scholar]
- Roy, J.S.; Braën, C.; Leblond, J.; Desmeules, F.; E Dionne, C.; MacDermid, J.C.; Bureau, N.J.; Frémont, P. Diagnostic accuracy of ultrasonography, MRI and MR arthrography in the characterisation of rotator cuff disorders: A systematic review and meta-analysis. Br. J. Sports Med. 2015, 49, 1316–1328. [Google Scholar] [CrossRef]
- Louwerens, J.K.; Veltman, E.S.; van Noort, A.; van den Bekerom, M.P. The Effectiveness of High-Energy Extracorporeal Shockwave Therapy Versus Ultrasound-Guided Needling Versus Arthroscopic Surgery in the Management of Chronic Calcific Rotator Cuff Tendinopathy: A Systematic Review. Arthroscopy 2016, 32, 165–175. [Google Scholar] [CrossRef]
- Bannuru, R.R.; Flavin, N.E.; Vaysbrot, E.; Harvey, W.; McAlindon, T. High-energy extracorporeal shockwave therapy for treating chronic calcific tendinitis of the shoulder: A systematic review. Ann. Intern. Med. 2014, 160, 542–549. [Google Scholar] [CrossRef] [PubMed]
- Van Rijn, R.M.; Huisstede, B.M.; Koes, B.W.; Burdorf, A. Associations between work-related factors and specific disorders of the shoulder—A systematic review of the literature. Scand. J. Work. Environ. Health 2010, 36, 189–201. [Google Scholar] [CrossRef]
- Li, W.; Zhang, S.X.; Yang, Q.; Li, B.L.; Meng, Q.G.; Guo, Z.G. Effect of extracorporeal shockwave therapy for treating patients with chronic rotator cuff tendonitis. Medicine 2017, 96, e7940. [Google Scholar] [CrossRef]
- Galasso, O.; Amelio, E.; Riccelli, D.A.; Gasparini, G. Short-term outcomes of extracorporeal shock wave therapy for the treatment of chronic non-calcific tendinopathy of the supraspinatus: A double-blind, randomised, placebo-controlled trial. BMC Musculoskelet. Disord. 2012, 13, 86. [Google Scholar] [CrossRef]
- Hutchinson, J.L.; Gusberti, D.; Saab, G. Changing appearance of intraosseous calcific tendinitis in the shoulder with time: A case report. Radiol. Case Rep. 2019, 14, 1267–1271. [Google Scholar] [CrossRef] [PubMed]
- Heller, G.Z.; Manuguerra, M.; Chow, R. How to analyse the Visual Analogue Scale: Myths, truths and clinical relevance. Scand. J. Pain. 2016, 13, 67–75. [Google Scholar] [CrossRef]
- Vrotsou, K.; AÃÅvila, M.; MachoÃÅn, M.; Mateo-Abad, M.; Pardo, Y.; Garin, O.; Zaror, C.; GonzaÃÅlez, N.; Escobar, A.; CueÃÅllar, R. Constant-Murley Score: Systematic review and standardised evaluation in different shoulder pathologies. Qual. Life Res. 2018, 27, 2217–2226. [Google Scholar] [CrossRef]
- Ibrahim, M.I.; Donatelli, R.A.; Schmitz, C.; Hellman, M.A.; Buxbaum, F. Chronic plantar fasciitis treated with two sessions of radial extracorporeal shock wave therapy. Foot Ankle Int. 2010, 31, 391–397. [Google Scholar] [CrossRef] [PubMed]
- Cho, N.S.; Lee, B.G.; Rhee, Y.G. Radiologic course of the calcific deposits in calcific tendinitis of the shoulder: Does the initial radiologic aspect affect the final results? J. Shoulder Elb. Surg. 2010, 19, 267–272. [Google Scholar] [CrossRef]
- Ioppolo, F.; Tattoli, M.; Di Sante, L.; Attanasi, C.; Venditto, T.; Servidio, M.; Cacchio, A.; Santilli, V. Extracorporeal shockwave therapy for supraspinatus calcifying tendinitis: A randomised clinical trial comparing two different energy levels. Phys. Ther. 2012, 92, 1376–1385. [Google Scholar] [CrossRef]
- Yin, M.; Ma, J.; Xu, J.; Li, L.; Chen, G.; Sun, Z.; Liu, Y.; He, S.; Ye, J.; Mo, W. Use of artificial neural networks to identify the predictive factors of extracorporeal shock wave therapy treating patients with chronic plantar fasciitis. Sci. Rep. 2019, 9, 4207. [Google Scholar] [CrossRef] [PubMed]
- Tao, K.; Lei, J.; Huang, J. Physical Integrated Digital twin-based Interaction Mechanism of Artificial Intelligence Rehabilitation Robots Combining Visual Cognition and Motion Control. Wirel. Pers. Commun. 2024. [Google Scholar] [CrossRef]
- Witharana, P.; Chang, L.; Maier, R.; Ogundimu, E.; Wilkinson, C.; Athanasiou, T.; Akowuah, E. Feasibility study of rehabilitation for cardiac patients aided by an artificial intelligence web-based programme: A randomised controlled trial (RECAP trial)-a study protocol. BMJ Open. 2024, 14, e079404. [Google Scholar] [CrossRef] [PubMed]
- Xu, D.; Zhou, H.; Quan, W.; Jiang, X.; Liang, M.; Li, S.; Ugbolue, U.C.; Baker, J.S.; Gusztav, F.; Ma, X.; et al. A new method proposed for realizing human gait pattern recognition: Inspirations for the application of sports and clinical gait analysis. Gait Posture 2024, 107, 293–305. [Google Scholar] [CrossRef] [PubMed]
- Xu, D.; Quan, W.; Zhou, H.; Sun, D.; Baker, J.S.; Gu, Y. Explaining the differences of gait patterns between high and low-mileage runners with machine learning. Sci. Rep. 2022, 12, 2981. [Google Scholar] [CrossRef] [PubMed]
- Yin, M.C.; Yan, Y.J.; Tong, Z.Y.; Xu, C.Q.; Qiao, J.J.; Zhou, X.N.; Ye, J.; Mo, W. Development and Validation of a Novel Scoring System for Severity of Plantar Fasciitis. Orthop. Surg. 2020, 12, 1882–1889. [Google Scholar] [CrossRef] [PubMed]
- Schofer, M.D.; Hinrichs, F.; Peterlein, C.D.; Arendt, M.; Schmitt, J. High- versus low-energy extracorporeal shock wave therapy of rotator cuff tendinopathy: A prospective, randomised, controlled study. Acta Orthop. Belg. 2009, 75, 452–458. [Google Scholar]
- Klüter, T.; Krath, A.; Stukenberg, M.; Gollwitzer, H.; Harrasser, N.; Knobloch, K.; Maffulli, N.; Hausdorf, J.; Gerdesmeyer, L. Electromagnetic transduction therapy and shockwave therapy in 86 patients with rotator cuff tendinopathy: A prospective randomized controlled trial. Electromagn. Biol. Med. 2018, 37, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, J.; Haake, M.; Tosch, A.; Hildebrand, R.; Deike, B.; Griss, P. Low-energy extracorporeal shock-wave treatment (ESWT) for tendinitis of the supraspinatus. A prospective, randomised study. J. Bone Jt. Surg. Br. 2001, 83, 873–876. [Google Scholar] [CrossRef]
- Sabeti-Aschraf, M.; Dorotka, R.; Goll, A.; Trieb, K. Extracorporeal shock wave therapy in the treatment of calcific tendinitis of the rotator cuff. Am. J. Sports Med. 2005, 33, 1365–1368. [Google Scholar] [CrossRef]
- Carosi, M.; Galeoto, G.; Gennaro, S.D.; Berardi, A.; Valente, D.; Servadio, A. Transcultural reliability and validity of an Italian language version of the Constant–Murley Score. J. Orthop. Trauma Rehabil. 2020, 27, 186–191. [Google Scholar] [CrossRef]
- Constant, C.; Murley, A. A clinical method for functional assessment of the shoulder. Clin. Orthop. Relat. Red. 1987, 214, 160–164. [Google Scholar] [CrossRef]
- IBM Corp. IBM SPSS Statistics for Windows; Version 27.0.; IBM Corp: Armonk, NY, USA, 2020. [Google Scholar]
- Shiri, I.; Salimi, Y.; Pakbin, M.; Hajianfar, G.; Avval, A.H.; Sanaat, A.; Mostafaei, S.; Akhavanallaf, A.; Saberi, A.; Mansouri, Z.; et al. COVID-19 prognostic modeling using CT radiomic features and machine learning algorithms: Analysis of a multi-institutional dataset of 14,339 patients. Comput. Biol. Med. 2022, 145, 105467. [Google Scholar] [CrossRef]
- Zhang, Y.F.; Liu, Y.; Chou, S.W.; Weng, H. Dose-related effects of radial extracorporeal shock wave therapy for knee osteoarthritis: A randomized controlled trial. J. Rehabil. Med. 2021, 53, jrm00144. [Google Scholar] [CrossRef]
- Haque, M.R.; Islam, M.M.; Iqbal, H.; Reza, M.S.; Hasan, M.K. Performance Evaluation of Random Forests and Artificial Neural Networks for the Classification of Liver Disorder. In Proceedings of the 2018 International Conference on Computer, Communication, Chemical, Material and Electronic Engineering (IC4ME2), Rajshahi, Bangladesh, 8–9 February 2018; pp. 1–5. [Google Scholar]
- Montavon, G.; Samek, W.; Müller, K.-R. Methods for interpreting and understanding deep neural networks. Digit. Signal Process. 2018, 73, 1–15. [Google Scholar] [CrossRef]
- Chen, J.; Liu, Z.; Yin, Z.; Liu, X.; Li, X.; Yin, L.; Zheng, W. Predict the effect of meteorological factors on haze using BP neural network. Urban Clim. 2023, 51, 101630. [Google Scholar] [CrossRef]
- Mendez, K.M.; Broadhurst, D.I.; Reinke, S.N. The application of artificial neural networks in metabolomics: A historical perspective. Metabolomics 2019, 15, 142. [Google Scholar] [CrossRef]
- Vertuccio, A.; Perugia, D.; Lanzetti, R.M.; Massimiani, A.; Lacopo, A.; Nusca, S.M.; Baldini, R.; Santoboni, F.; Latini, E.; Vetrano, M.; et al. Demographic and Clinical Factors Predict Focused Shockwave Therapy Results on Patients With Plantar Fasciitis. A Multilevel Analysis. MLTJ Muscles Ligaments Tendons J. 2021, 11, 376. [Google Scholar] [CrossRef]
- Notarnicola, A.; Maccagnano, G.; Tafuri, S.; Fiore, A.; Margiotta, C.; Pesce, V.; Moretti, B. Prognostic factors of extracorporeal shock wave therapy for tendinopathies. Musculoskelet. Surg. 2016, 100, 53–61. [Google Scholar] [CrossRef]
- Gerdesmeyer, L.; Wagenpfeil, S.; Haake, M.; Maier, M.; Loew, M.; Wörtler, K.; Lampe, R.; Seil, R.; Handle, G.; Gassel, S.; et al. Extracorporeal Shock Wave Therapy for the Treatment of Chronic Calcifying Tendonitis of the Rotator Cuff. JAMA 2003, 290, 2573. [Google Scholar] [CrossRef]
- Surace, S.J.; Deitch, J.; Johnston, R.V.; Buchbinder, R. Shock wave therapy for rotator cuff disease with or without calcification. Cochrane Database Syst. Rev. 2020, 3, CD008962. [Google Scholar] [CrossRef] [PubMed]
- De Menezes, A.B.; Silva, R.S.; Adala, J.F.; Guidi, R.M.; Liebano, R.E. Shockwave therapy associated with progressive exercises in rotator cuff tendinopathy: A clinical trial protocol. Pain. Manag. 2021, 11, 639–646. [Google Scholar] [CrossRef]
- Speed, C.A.; Richards, C.; Nichols, D.; Burnet, S.; Wies, J.T.; Humphreys, H.; Hazleman, B.L. Extracorporeal shockwave therapy for tendonitis of the rotator cuff: A double-blind, randomised, controlled trial. The Journal of Bone and Joint Surgery. Br. Vol. 2002, 84, 509–512. [Google Scholar]
- De la Corte-Rodríguez, H.; Román-Belmonte, J.M.; Rodríguez-Damiani, B.A.; Vázquez-Sasot, A.; Rodríguez-Merchán, E.C. Extracorporeal Shock Wave Therapy for the Treatment of Musculoskeletal Pain: A Narrative Review. Healthcare 2023, 11, 2830. [Google Scholar] [CrossRef] [PubMed]
- Taylor, J.; Dunkerley, S.; Silver, D.; Redfern, A.; Talbot, N.; Sharpe, I.; Guyver, P. Extracorporeal shockwave therapy (ESWT) for refractory Achilles tendinopathy: A prospective audit with 2-year follow up. Foot 2016, 26, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Burton, I. Combined extracorporeal shockwave therapy and exercise for the treatment of tendinopathy: A narrative review. Sports Med. Health Sci. 2021, 4, 8–17. [Google Scholar] [CrossRef] [PubMed]
- Di Renzi, D.; Zavaroni, S.; Mazzola, M.; Petroselli, L.; Bruno, A.A.; Trischitta, D.; Vulpiani, M.C.; Vetrano, M. Treatment for Symptomatic Calcific Tendinopathy of the Shoulder: Ultrasound-Guided Needling Lavage and Extracorporeal Shock Wave Therapy vs Extracorporeal Shock Wave Therapy. A prospective observational study. Muscles Ligaments Tendons J. 2023, 13, 440–448. [Google Scholar] [CrossRef]
- Zhao, J.; Jiang, Y. The therapeutic effect of extracorporeal shock wave therapy combined with Kinesio Tape on plantar fasciitis. J. Back Musculoskelet. Rehabil. 2023, 36, 1203–1211. [Google Scholar] [CrossRef]
- Cheema, A.S.; Doyon, J.; Lapner, P. Transcutaneous electrical nerve stimulation (TENS) and extracorporeal shockwave therapy (ESWT) in lateral epicondylitis: A systematic review and meta-analysis. JSES Int. 2022, 7, 351–356. [Google Scholar] [CrossRef]
- Elsayed, R.M.; Elghaweet, A.E.; Eldawoody, A.A.F. Effect of Shockwave Therapy and Home Exercises for Treatment of Chronic Supraspinatus Tendinitis. Egypt. J. Hosp. Med. 2023, 92, 6276–6286. [Google Scholar]
- Liu, K.; Yin, L.; Zhang, Y.; Huang, L.; Liu, G.; Zhu, R.; Fang, P.; Ma, Y.; Ma, Z. Effect of extracorporeal shock wave combined with Kinesio taping on upper limb function during individuals with biceps brachii tendinopathy: Protocol for a double-blind, randomised controlled trial. BMJ Open. 2024, 14, e071967. [Google Scholar] [CrossRef] [PubMed]
- On, H.; Yim, J. Effects of local vibration combined with extracorporeal shock wave therapy in plantar fasciitis: A randomized controlled trial. J. Rehabil. Med. 2023, 55, jrm12405. [Google Scholar] [CrossRef] [PubMed]
- ElGendy, M.H.; Mazen, M.M.; Saied, A.M.; ElMeligie, M.M.; Aneis, Y. Extracorporeal Shock Wave Therapy vs. Corticosteroid Local Injection in Shoulder Impingement Syndrome : A Three-Arm Randomized Controlled Trial. Am. J. Phys. Med. Rehabil. 2023, 102, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Zhu, T.; Liu, K.; Ni, B.Y.; Li, L.; Jin, H.P.; Wu, W. Effects of extracorporeal shock wave therapy combined with isokinetic strength training on spastic calf triceps in patients after a stroke: A double-blinded randomised controlled trial. Neurol. Res. 2023, 45, 1019–1025. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.J.; Moon, Y.S.; Kwon, D.R.; Cho, S.C.; Kim, E.H. Polydeoxyribonucleotide and Shock Wave Therapy Sequence Efficacy in Regenerating Immobilized Rabbit Calf Muscles. Int. J. Mol. Sci. 2023, 24, 12820. [Google Scholar] [CrossRef] [PubMed]
- Ryskalin, L.; Morucci, G.; Natale, G.; Soldani, P.; Gesi, M. Molecular Mechanisms Underlying the Pain-Relieving Effects of Extracorporeal Shock Wave Therapy: A Focus on Fascia Nociceptors. Life 2022, 12, 743. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Wang, F.; Yang, K. Shock wave therapy induces neovascularisation at the tendon-bone junction. A study in rabbits. J. Orthop. Res. 2003, 21, 984–989. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Wang, F.; Yang, K. Biological effects of extracorporeal shockwave in bone healing: A study in rabbits. Arch. Orthop. Trauma. Surg. 2008, 128, 879–884. [Google Scholar] [CrossRef] [PubMed]
- Perroni, F.; Migliaccio, S.; Borrione, P.; Vetrano, M.; Amatori, S.; Sisti, D.; Rocchi, M.B.L.; Salerno, G.; Vescovo, R.D.; Cavarretta, E.; et al. Can Haematological and Hormonal Biomarkers Predict Fitness Parameters in Youth Soccer Players? A Pilot Study. Int. J. Environ. Res. Public Health 2020, 17, 6294. [Google Scholar] [CrossRef]
- Chen, Y.J.; Wang, C.J.; Yang, K.D.; Kuo, Y.R.; Huang, H.C.; Huang, Y.T.; Sun, Y.C.; Wang, F.S. Extracorporeal shock waves promote healing of collagenase-induced Achilles tendinitis and increase TGF-beta1 and IGF-I expression. J. Orthop. Res. 2004, 22, 854–861. [Google Scholar] [CrossRef]
- Zhang, D.; Kearney, C.J.; Cheriyan, T.; Schmid, T.M.; Spector, M. Extracorporeal shockwave-induced expression of lubricin in tendons and septa. Cell Tissue Res. 2011, 346, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Visco, V.; Vulpiani, M.C.; Torrisi, M.R.; Ferretti, A.; Pavan, A.; Vetrano, M. Experimental studies on the biological effects of extracorporeal shock wave therapy on tendon models. A review of the literature. Muscles Ligaments Tendons J. 2014, 4, 357–361. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Group 0 (n = 71) | Group 1 (n = 138) | |
|---|---|---|
| Gender | ||
| M | 27 (38.0%) | 61 (44.2%) |
| F | 44 (62.0%) | 77 (55.8%) |
| Affected Side | ||
| Right | 46 (64.8%) | 82 (59.4%) |
| Left | 25 (35.2%) | 56 (40.6%) |
| RM Score T0 | ||
| 1 | 15 (21.1%) | 32 (23.2%) |
| 2 | 24 (33.8%) | 58 (42.0%) |
| 3 | 28 (39.4%) | 37 (26.8%) |
| 4 | 4 (5.6%) | 9 (6.5%) |
| Age | 60.62 (±10.6) | 58.9 (±10.1) |
| CMS Score T0 | 62.2 (±16.6) | 64.6 (±15.1) |
| VAS T0 | 6.1 (±1.9) | 6.1 (±1.6) |
| Assessments | Total 209 |
|---|---|
| Age (mean ± SD), years | 59.5 ± 10.2 |
| Gender: Male | 88 (42.1%) |
| Gender: Female | 121 (57.9%) |
| Right Side Affected | 128 (61.2%) |
| Left Side Affected | 81 (38.8%) |
| VAS (mean ± SD) | 6.1 ±1.7 |
| Roles and Maudsley Score (mean ± SD) | 2.2 ± 0.9 |
| Constant and Murley Score (mean ± SD) | 63.8 ± 15.6 |
| Training Sample | Testing Sample | Exclusion | Total | |
|---|---|---|---|---|
| Number | 140 | 67 | 2 | 209 |
| Percentage | 67.6% | 32.4% | / | 100% |
| VAS Score | Constant and Murley Score | Roles and Maudsley | |
|---|---|---|---|
| Baseline T0 | 6.1 ± 1.7 | 63.8 ± 15.6 | 2.2 ± 0.9 |
| Follow-up T1 | 3.1 ± 2.3 | 79.8 ± 16 | 1.2 ± 0.7 |
| Variable | Definition of Neurons | Type | Value |
|---|---|---|---|
| Age | The years of old | Continuous | 29–85 |
| Gender | Male/Female | Categorical | 0, 1 |
| Affected Side | Right/Left | Categorical | 0, 1 |
| RM Score T0 | The number of RM score | Categorical | 1, 2, 3, 4 |
| CMS Score T0 | The number of CMS score | Continuous | 12–94 |
| VAS T0 | The number of VAS | Continuous | 0–10 |
| No | Variable | Importance | Normalized Importance | p-Value | Bivariate Correlations |
|---|---|---|---|---|---|
| 1 | Age | 0.281 | 100% | 0.375 | −0.62 |
| 2 | CMS Score | 0.224 | 79.6% | 0.002 | 0.211 |
| 3 | VAS | 0.210 | 74.8% | 0.027 | −0.154 |
| 4 | RM Score | 0.149 | 52.9% | 0.037 | −0.145 |
| 5 | Gender | 0.104 | 37.0% | 0.001 | −0.264 |
| 6 | Affected Side | 0.31 | 11.1% | 0.408 | −0.058 |
| Model Target | Sensitivity (%) | Specificity (%) | AUC (95%CI) | NPV |
|---|---|---|---|---|
| Vas < 40% | 80.7% | 72.3% | 0.701 | 96.3% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santilli, G.; Vetrano, M.; Mangone, M.; Agostini, F.; Bernetti, A.; Coraci, D.; Paoloni, M.; de Sire, A.; Paolucci, T.; Latini, E.; et al. Predictive Prognostic Factors in Non-Calcific Supraspinatus Tendinopathy Treated with Focused Extracorporeal Shock Wave Therapy: An Artificial Neural Network Approach. Life 2024, 14, 681. https://doi.org/10.3390/life14060681
Santilli G, Vetrano M, Mangone M, Agostini F, Bernetti A, Coraci D, Paoloni M, de Sire A, Paolucci T, Latini E, et al. Predictive Prognostic Factors in Non-Calcific Supraspinatus Tendinopathy Treated with Focused Extracorporeal Shock Wave Therapy: An Artificial Neural Network Approach. Life. 2024; 14(6):681. https://doi.org/10.3390/life14060681
Chicago/Turabian StyleSantilli, Gabriele, Mario Vetrano, Massimiliano Mangone, Francesco Agostini, Andrea Bernetti, Daniele Coraci, Marco Paoloni, Alessandro de Sire, Teresa Paolucci, Eleonora Latini, and et al. 2024. "Predictive Prognostic Factors in Non-Calcific Supraspinatus Tendinopathy Treated with Focused Extracorporeal Shock Wave Therapy: An Artificial Neural Network Approach" Life 14, no. 6: 681. https://doi.org/10.3390/life14060681
APA StyleSantilli, G., Vetrano, M., Mangone, M., Agostini, F., Bernetti, A., Coraci, D., Paoloni, M., de Sire, A., Paolucci, T., Latini, E., Santoboni, F., Nusca, S. M., & Vulpiani, M. C. (2024). Predictive Prognostic Factors in Non-Calcific Supraspinatus Tendinopathy Treated with Focused Extracorporeal Shock Wave Therapy: An Artificial Neural Network Approach. Life, 14(6), 681. https://doi.org/10.3390/life14060681