
Radiomics Analysis of Preprocedural CT Imaging for Outcome Prediction after Transjugular Intrahepatic Portosystemic Shunt Creation

 ,
,  ,
,  ,
,  ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
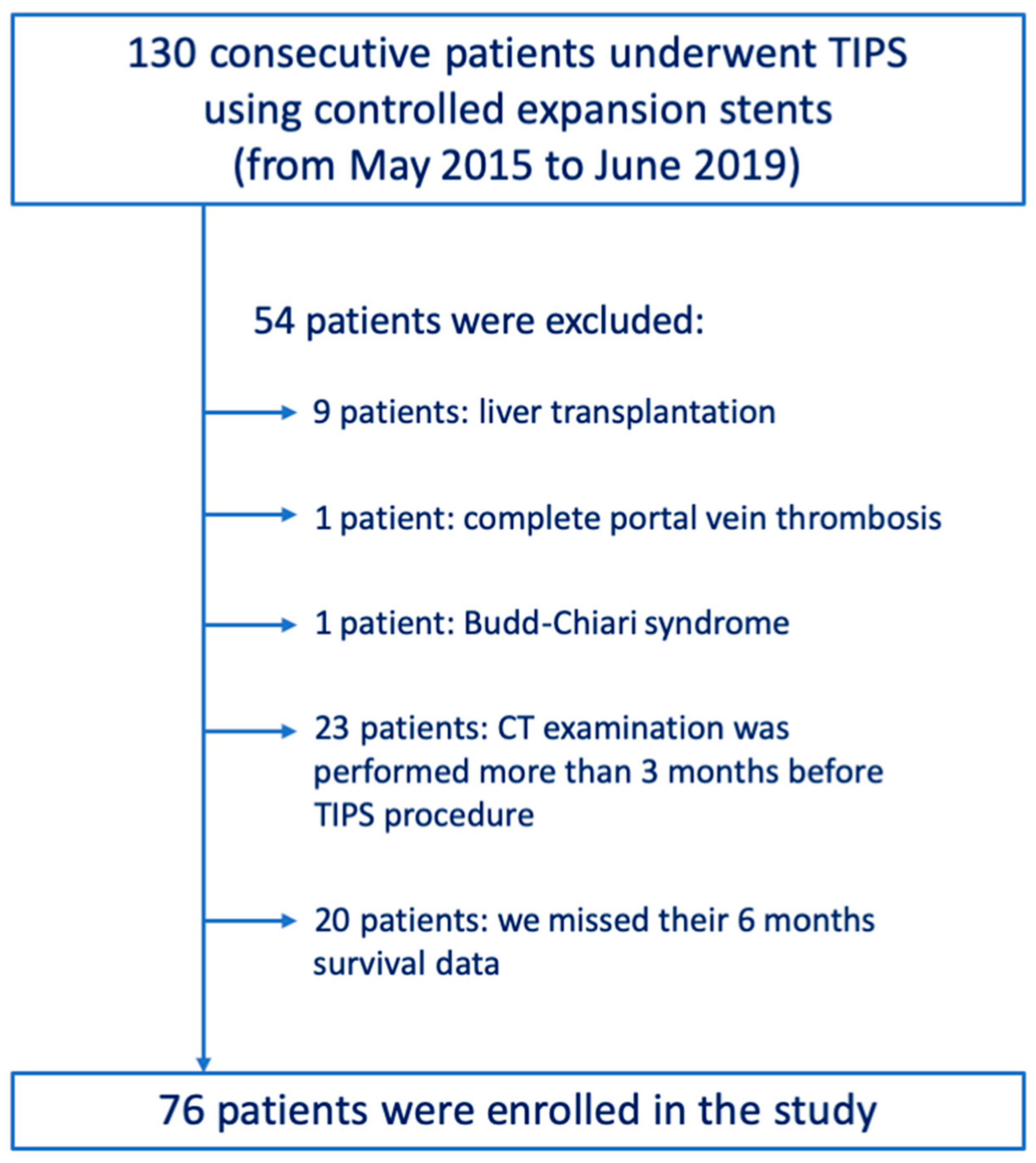
2.1. Patients
2.2. TIPS Procedure
2.3. CT Examination
2.4. Volume of Interest (VOI) Segmentation and Feature Extraction
2.5. Feature Reduction and Selection
2.6. Predictive Model
2.7. Statistical Performance Analysis
3. Results
3.1. Study Population
3.2. Clinical Characteristics
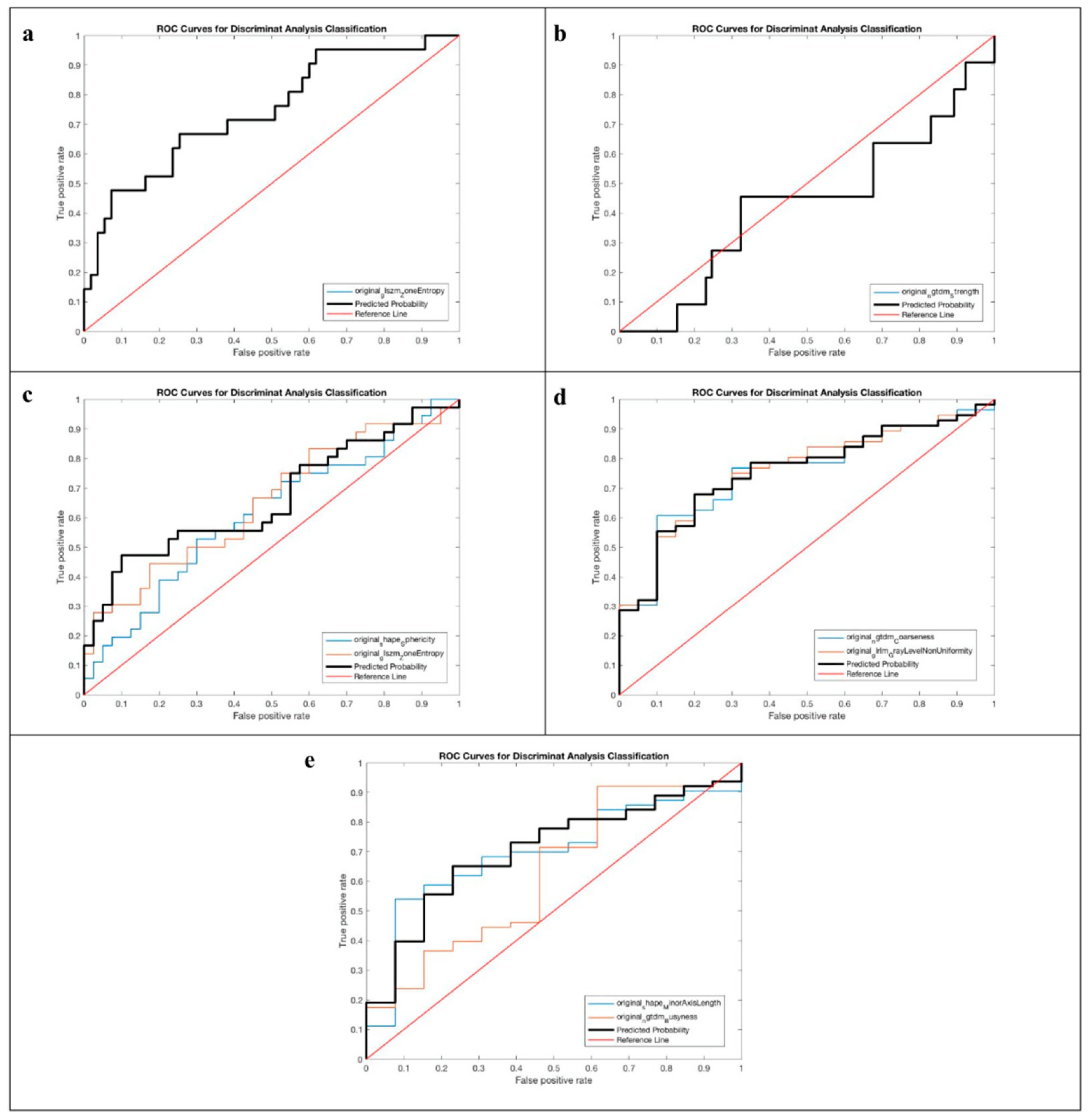
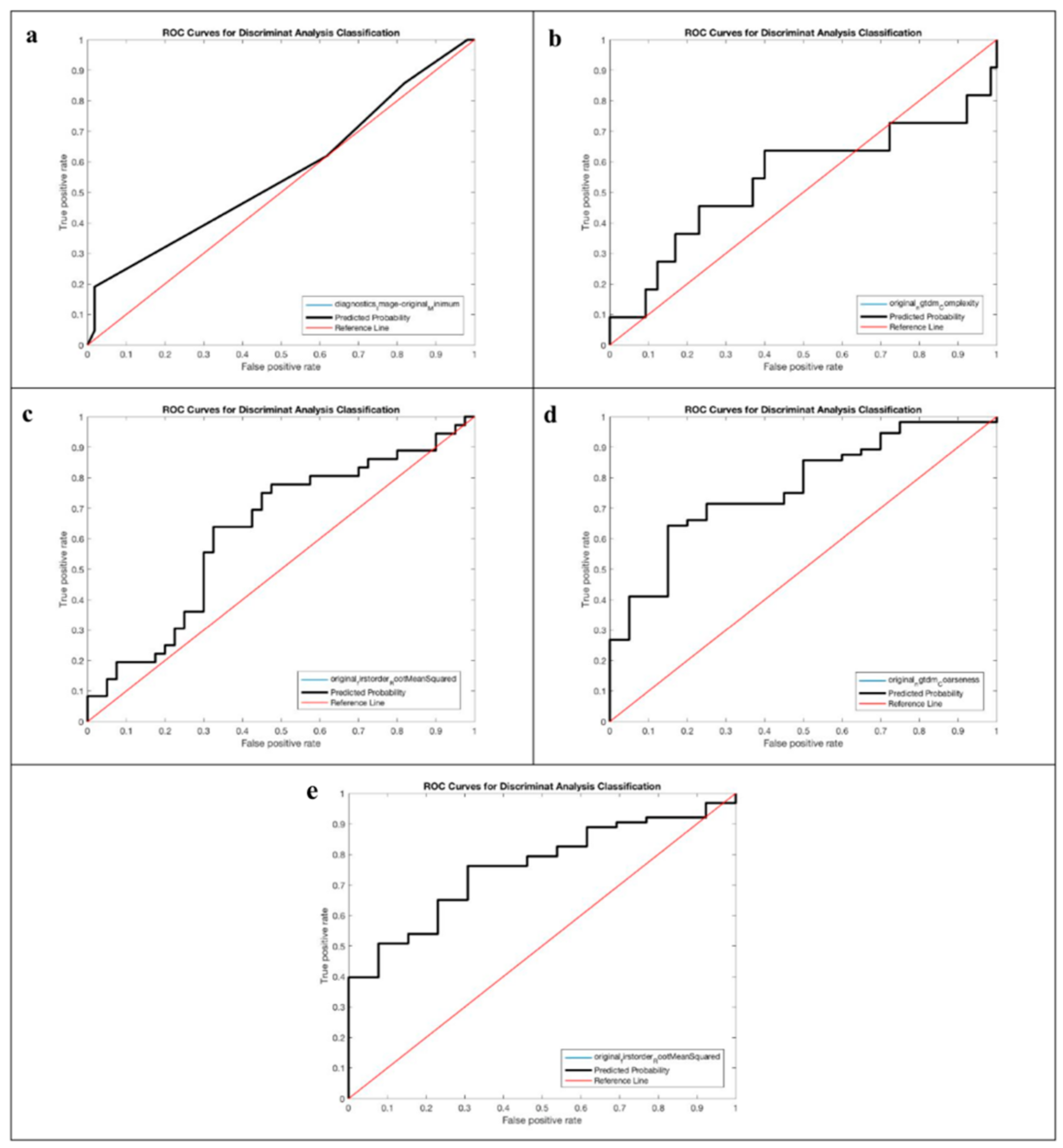
3.3. Performance of the Radiomics Model
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Boyer, T.D.; Haskal, Z.J.; American Association for the Study of Liver Diseases. The role of transjugular intrahepatic portosystemic shunt (TIPS) in the management of portal hypertension: Update 2009. Hepatology 2010, 51, 306. [Google Scholar] [CrossRef] [PubMed]
- Riggio, O.; Angeloni, S.; Salvatori, F.M.; De Santis, A.; Cerini, F.; Farcomeni, A.; Attili, A.F.; Merli, M. Incidence, natural history, and risk factors of hepatic encephalopathy after transjugular intrahepatic portosystemic shunt with polytetrafluoroethylene-covered stent grafts. Am. J. Gastroenterol. 2008, 103, 2738–2746. [Google Scholar] [CrossRef]
- Lambin, P.; Leijenaar, R.T.H.; Deist, T.M.; Peerlings, J.; de Jong, E.E.C.; van Timmeren, J.; Sanduleanu, S.; Larue, R.T.H.M.; Even, A.J.G.; Jochems, A.; et al. Radiomics: The bridge between medical imaging and personalized medicine. Nat. Rev. Clin. Oncol. 2017, 14, 749–762. [Google Scholar] [CrossRef] [PubMed]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images Are More than Pictures, They Are Data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pavone, A.M.; Benfante, V.; Stefano, A.; Mamone, G.; Milazzo, M.; Di Piazza, A.; Parenti, R.; Maruzzelli, L.; Miraglia, R.; Comelli, A. Automatic Liver Segmentation in Pre-TIPS Cirrhotic Patients: A Preliminary Step for Radiomics Studies. In ICIAP 2022 Workshops LNCS; Mazzeo, P.L., Frontoni, E., Sclaroff, S., Distante, C., Eds.; Springer: Cham, Switzerland, 2022; Volume 13373, pp. 1–11. [Google Scholar] [CrossRef]
- Le Berre, C.; Sandborn, W.J.; Aridhi, S.; Devignes, M.-D.; Fournier, L.; SmaïlTabbone, M.; Danese, S.; Peyrin-Biroulet, L. Application of Artificial Intelligence to Gastroenterology and Hepatology. Gastroenterology 2020, 158, 76–94. [Google Scholar] [CrossRef] [PubMed]
- Ahn, J.C.; Connell, A.; Simonetto, D.A.; Hughes, C.; Shah, V.H. Application of Artificial Intelligence for the Diagnosis and Treatment of Liver Diseases. Hepatology 2021, 73, 2546–2563. [Google Scholar] [CrossRef] [PubMed]
- Su, T.H.; Wu, C.H.; Kao, J.H. Artificial intelligence in precision medicine in hepatology. J. Gastroenterol. Hepatol. 2021, 36, 569–580. [Google Scholar] [CrossRef] [PubMed]
- Cheng, S.; Yu, X.; Chen, X.; Jin, Z.; Xue, H.; Wang, Z.; Xie, P. CT-based radiomics model for preoperative prediction of hepatic encephalopathy after transjugular intrahepatic portosystemic shunt. Br. J. Radiol. 2022, 31, 20210792. [Google Scholar] [CrossRef] [PubMed]
- Vilstrup, H.; Amodio, P.; Bajaj, J.; Cordoba, J.; Ferenci, P.; Mullen, K.D.; Weissenborn, K.; Wong, P. Hepatic encephalopathy in chronic liver disease: 2014 Practice Guideline by the American Association for the Study of Liver Diseases and the European Association for the Study of the Liver. Hepatology 2014, 60, 715–735. [Google Scholar] [CrossRef] [PubMed]
- Miraglia, R.; Maruzzelli, L.; Di Piazza, A.; Mamone, G.; Caruso, S.; Gentile, G.; Tuzzolino, F.; Floridia, G.; Petridis, I.; Volpes, R.; et al. Transjugular Intrahepatic Portosystemic Shunt Using the New Gore Viatorr Controlled Expansion Endoprosthesis: Prospective, Single-Center, Preliminary Experience. Cardiovasc. Interv. Radiol. 2019, 42, 78–86. [Google Scholar] [CrossRef] [PubMed]
- Miraglia, R.; Maruzzelli, L.; Cortis, K.; D’Amico, M.; Floridia, G.; Gallo, G.; Tafaro, C.; Luca, A. Radiation Exposure in Transjugular Intrahepatic Portosystemic Shunt Creation. Cardiovasc. Interv. Radiol. 2016, 39, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Van Timmeren, J.E.; Cester, D.; Tanadini-Lang, S.; Alkadhi, H.; Baessler, B. Radiomics in medical imaging-“how-to” guide and critical reflection. Insights Imaging 2020, 11, 91. [Google Scholar] [CrossRef] [PubMed]
- Stefano, A.; Antonio Leal, A.; Richiusa, S.; Trang, P.; Comelli, A.; Benfante, V.; Cosentino, S.; Sabini, M.G.; Tuttolomondo, A.; Altieri, R.; et al. Robustness of PETRadiomics Features: Impact of Co-Registration with, M.R.I. Appl. Sci. 2021, 11, 10170. [Google Scholar] [CrossRef]
- Gotra, A.; Sivakumaran, L.; Chartrand, G.; Vu, K.N.; Vandenbroucke-Menu, F.; Kauffmann, C.; Kadoury, S.; Gallix, B.; de Guise, J.A.; Tang, A. Liver segmentation: Indications, techniques and future directions. Insights Imaging 2017, 8, 377–392. [Google Scholar] [CrossRef] [PubMed]
- Van Griethuysen, J.J.M.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.H.; Fillion-Robin, J.C.; Pieper, S.; Aerts, H.J.W.L. Computational radiomics system to decode the radiographic phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef] [PubMed]
- Zwanenburg, A.; Vallières, M.; Abdalah, M.A.; Aerts, H.J.W.L.; Andrearczyk, V.; Apte, A.; Ashrafinia, S.; Bakas, S.; Beukinga, R.J.; Boellaard, R.; et al. The image biomarker standardization initiative: Standardized quantitative radiomics for high-throughput image-based phenotyping. Radiology 2020, 295, 328–338. [Google Scholar] [CrossRef] [PubMed]
- Barone, S.; Cannella, R.; Comelli, A.; Pellegrino, A.; Salvaggio, G.; Stefano, A.; Vernuccio, F. Hybrid descriptive-inferential method for key feature selection in prostate cancer radiomics. Appl. Stoch. Model. Bus. Ind. 2021, 37, 961–972. [Google Scholar] [CrossRef]
- Pasini, G. Assessing the Robustness and Reproducibility of CT Radiomics Features in Non-small-cell Lung Carcinoma. In Image Analysis and Processing—ICIAP 2023 Workshops, ICIAP 2023; Lecture Notes in Computer Science; Foresti, G.L., Fusiello, A., Hancock, E., Eds.; Springer: Cham, Switzerland, 2023; Volume 14366. [Google Scholar] [CrossRef]
- Laudicella, R.; Comelli, A.; Liberini, V.; Vento, A.; Stefano, A.; Spataro, A.; Crocè, L.; Baldari, S.; Bambaci, M.; Deandreis, D.; et al. [68 Ga] DOTATOC PET/CT Radiomics to Predict the Response in GEP-NETs Undergoing [177 Lu] DOTATOC PRRT: The “Theragnomics” Concept. Cancers 2022, 14, 984. [Google Scholar] [CrossRef] [PubMed]
- Xue, J.H.; Titterington, D.M. Do un-balanced data have a negative effect on LDA? Pattern Recognit. 2008, 41, 1558–1571. [Google Scholar] [CrossRef]
- Russo, G.; Stefano, A.; Alongi, P.; Comelli, A.; Catalfamo, B.; Mantarro, C.; Longo, C.; Altieri, R.; Certo, F.; Cosentino, S.; et al. Feasibility on the use of radiomics features of 11[C]-MET PET/CT in central nervous system tumours: Preliminary results on potential grading discrimination using a machine learning model. Curr. Oncol. 2021, 28, 5318–5331. [Google Scholar] [CrossRef]
- Cannella, R.; Cammà, C.; Matteini, F.; Celsa, C.; Giuffrida, P.; Enea, M.; Comelli, A.; Stefano, A.; Cammà, C.; Midiri, M.; et al. Radiomics Analysis on Gadoxetate Disodium-Enhanced MRI Predicts Response to Transarterial Embolization in Patients with HCC. Diagnostics 2022, 12, 1308. [Google Scholar] [CrossRef]
- Dissegna, D.; Sponza, M.; Falleti, E.; Fabris, C.; Vit, A.; Angeli, P.; Piano, S.; Cussigh, A.; Cmet, S.; Toniutto, P. Morbidity and mortality after transjugular intrahepatic portosystemic shunt placement in patients with cirrhosis. Eur. J. Gastroenterol. Hepatol. 2019, 31, 626–632. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, G.; Maruzzelli, L.; Airoldi, A.; Petridis, I.; Tosetti, G.; Rampoldi, A.; D’Amico, M.; Miraglia, R.; De Nicola, S.; La Mura, V.; et al. Performance of the model for end-stage liver disease score for mortality prediction and the potential role of etiology. J. Hepatol. 2021, 75, 1355–1366. [Google Scholar] [CrossRef] [PubMed]
- Cao, J.M.; Yang, J.Q.; Ming, Z.Q.; Wu, J.L.; Yang, L.Q.; Chen, T.W.; Li, R.; Ou, J.; Zhang, X.M.; Mu, Q.W.; et al. A radiomics model of liver CT to predict risk of hepatic encephalopathy secondary to hepatitis B related cirrhosis. Eur. J. Radiol. 2020, 130, 109201. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Outcome | Positive | Negative |
|---|---|---|
| Hepatic Encephalopathy ≥2 | 21 | 55 |
| Pre-TIPS Hepatic Encephalopathy | 11 | 65 |
| Hepatic Encephalopathy | 36 | 40 |
| Clinical response | 56 | 20 |
| Survival at 6 months | 63 | 13 |
| Basal CT | Portal CT | |||
|---|---|---|---|---|
| Hepatic Encephalopathy ≥2 | Feature | original_glszm_ZoneEntropy | diagnostics_Image-original_Minimum | |
| p-value | <0.001 | 0.008 | ||
| pre-TIPS Hepatic Encephalopathy | Feature | original_ngtdm_Strength | original_ngtdm_Complexity | |
| p-value | 0.081 | 0.036 | ||
| Hepatic Encephalopathy | Feature | original_shape_Sphericity | original_glszm_ZoneEntropy | original_firstorder_RootMeanSquared |
| p-value | 0.026 | 0.020 | 0.023 | |
| Clinical response | Feature | original_ngtdm_Coarseness | original_glrlm_GrayLevelNonUniformity | original_ngtdm_Coarseness |
| p-value | 0.002 | <0.001 | <0.001 | |
| Survival at 6 month | Feature | original_shape_MinorAxisLength | original_ngtdm_Busyness | original_firstorder_RootMeanSquared |
| p-value | 0.050 | 0.020 | 0.013 | |
| Sensitivity [%] | Specificity [%] | PPV [%] | Accuracy [%] | AUROC | p-Value | |
|---|---|---|---|---|---|---|
| Basal CT | ||||||
| Hepatic Encephalopathy ≥2 | 80.67 | 52.80 | 82.52 | 73.21 | 0.744 (0.615–0.874) | 0.002 |
| pre-TIPS Hepatic Encephalopathy | 89.31 | 4.32 | 85.58 | 77.81 | 0.429 (0.229–0.629) | 0.484 |
| Hepatic Encephalopathy | 66.75 | 51.11 | 61.13 | 59.44 | 0.664 (0.538–0.790) | 0.038 |
| Clinical response | 73.75 | 63.93 | 42.77 | 66.42 | 0.755 (0.640–0.870) | <0.001 |
| Survival at 6 month | 76.53 | 58.15 | 25.93 | 61.21 | 0.704 (0.563–0.845) | 0.017 |
| Portal CT | ||||||
| Hepatic Encephalopathy ≥2 | 97.67 | 23.81 | 77.73 | 77.82 | 0.559 (0.385–0.733) | 0.406 |
| pre-TIPS Hepatic Encephalopathy | 88.59 | 19.62 | 87.64 | 79.26 | 0.544 (0.312–0.775) | 0.710 |
| Hepatic Encephalopathy | 73.08 | 50.32 | 62.66 | 62.45 | 0.627 (0.499–0.756) | 0.044 |
| Clinical response | 74.00 | 62.38 | 41.71 | 65.34 | 0.767 (0.651–0.882) | <0.001 |
| Survival at 6 month | 82.99 | 69.11 | 33.78 | 71.23 | 0.757 (0.633–0.880) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mamone, G.; Comelli, A.; Porrello, G.; Milazzo, M.; Di Piazza, A.; Stefano, A.; Benfante, V.; Tuttolomondo, A.; Sparacia, G.; Maruzzelli, L.; et al. Radiomics Analysis of Preprocedural CT Imaging for Outcome Prediction after Transjugular Intrahepatic Portosystemic Shunt Creation. Life 2024, 14, 726. https://doi.org/10.3390/life14060726
Mamone G, Comelli A, Porrello G, Milazzo M, Di Piazza A, Stefano A, Benfante V, Tuttolomondo A, Sparacia G, Maruzzelli L, et al. Radiomics Analysis of Preprocedural CT Imaging for Outcome Prediction after Transjugular Intrahepatic Portosystemic Shunt Creation. Life. 2024; 14(6):726. https://doi.org/10.3390/life14060726
Chicago/Turabian StyleMamone, Giuseppe, Albert Comelli, Giorgia Porrello, Mariapina Milazzo, Ambra Di Piazza, Alessandro Stefano, Viviana Benfante, Antonino Tuttolomondo, Gianvincenzo Sparacia, Luigi Maruzzelli, and et al. 2024. "Radiomics Analysis of Preprocedural CT Imaging for Outcome Prediction after Transjugular Intrahepatic Portosystemic Shunt Creation" Life 14, no. 6: 726. https://doi.org/10.3390/life14060726