

Exploring New Drug Repurposing Opportunities for MEK Inhibitors in RASopathies: A Comprehensive Review of Safety, Efficacy, and Future Perspectives of Trametinib and Selumetinib

 ,
,  , , ,
, , ,
Abstract
1. Introduction
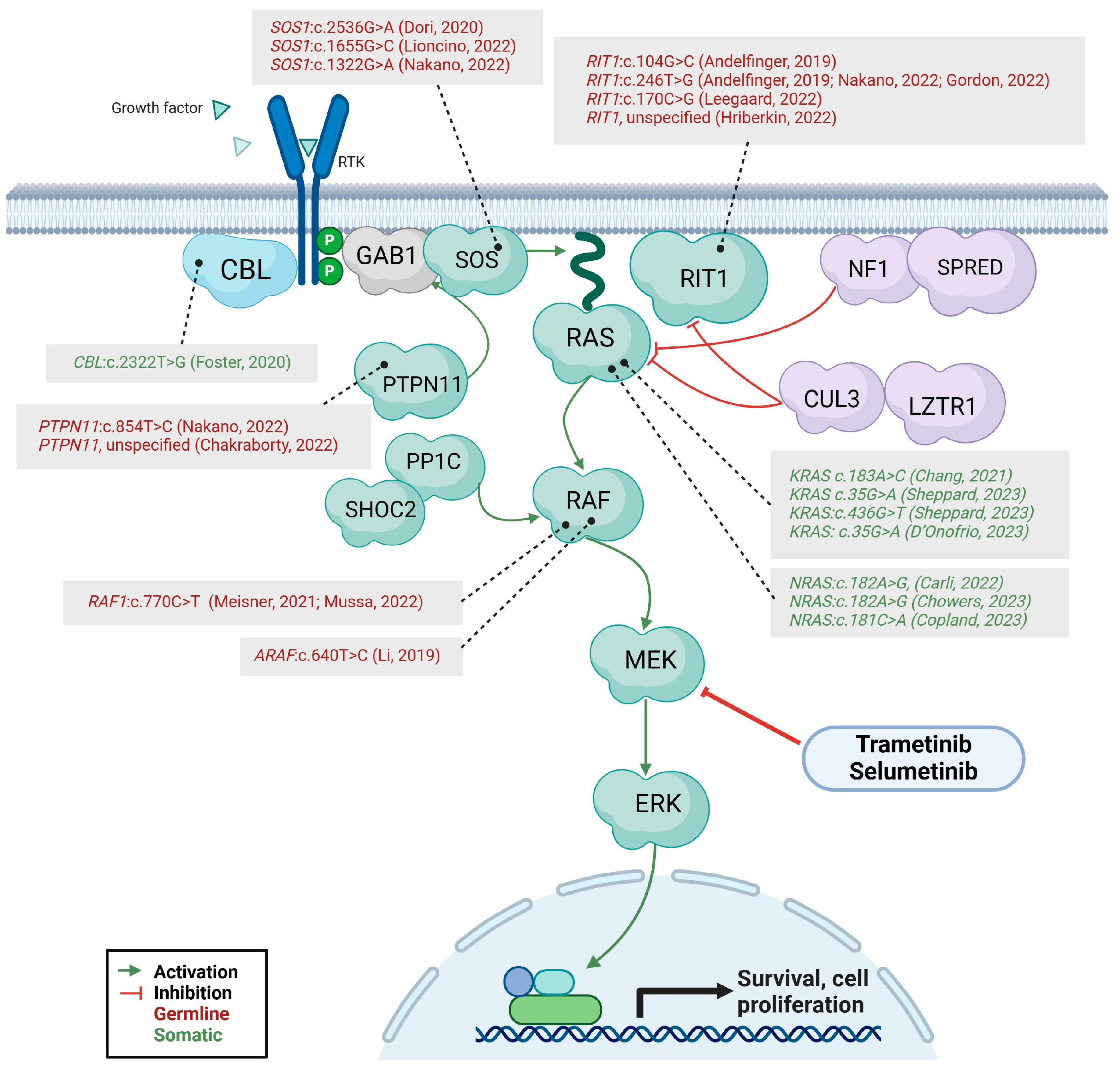
1.1. Ras-MAPK Signaling as Target
1.2. Pre-Clinical Studies
2. Methods
3. Literature Search Results
3.1. Cardiological Use of MEKi
3.2. Lymphatic Use of MEKi
3.3. Neurological Use of MEKi
3.4. MEKi in Mosaic RASopathies
3.5. Indications, Dosage, Timing and Adverse Events
3.6. Monitoring Protocol
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Roberts, A.E.; Allanson, J.E.; Tartaglia, M.; Gelb, B.D. Noonan Syndrome. Lancet 2013, 381, 333–342. [Google Scholar] [CrossRef]
- Tartaglia, M.; Aoki, Y.; Gelb, B.D. The Molecular Genetics of RASopathies: An Update on Novel Disease Genes and New Disorders. Am. J. Med. Genet. C Semin. Med. Genet. 2022, 190, 425–439. [Google Scholar] [CrossRef] [PubMed]
- Rauen, K.A. The RASopathies. Annu. Rev. Genom. Hum. Genet. 2013, 14, 355–369. [Google Scholar] [CrossRef] [PubMed]
- Tartaglia, M.; Gelb, B.D.; Zenker, M. Noonan Syndrome and Clinically Related Disorders. Best. Pract. Res. Clin. Endocrinol. Metab. 2011, 25, 161–179. [Google Scholar] [CrossRef]
- Chacon-Camacho, O.F.; Lopez-Moreno, D.; Morales-Sanchez, M.A.; Hofmann, E.; Pacheco-Quito, M.; Wieland, I.; Cortes-Gonzalez, V.; Villanueva-Mendoza, C.; Zenker, M.; Zenteno, J.C. Expansion of the Phenotypic Spectrum and Description of Molecular Findings in a Cohort of Patients with Oculocutaneous Mosaic RASopathies. Mol. Genet. Genom. Med. 2019, 7, e625. [Google Scholar] [CrossRef] [PubMed]
- Bennett, J.T.; Tan, T.Y.; Alcantara, D.; Tétrault, M.; Timms, A.E.; Jensen, D.; Collins, S.; Nowaczyk, M.J.M.; Lindhurst, M.J.; Christensen, K.M.; et al. Mosaic Activating Mutations in FGFR1 Cause Encephalocraniocutaneous Lipomatosis. Am. J. Hum. Genet. 2016, 98, 579–587. [Google Scholar] [CrossRef] [PubMed]
- Lim, Y.H.; Ovejero, D.; Sugarman, J.S.; DeKlotz, C.M.C.; Maruri, A.; Eichenfield, L.F.; Kelley, P.K.; Jüppner, H.; Gottschalk, M.; Tifft, C.J.; et al. Multilineage Somatic Activating Mutations in HRAS and NRAS Cause Mosaic Cutaneous and Skeletal Lesions, Elevated FGF23 and Hypophosphatemia. Hum. Mol. Genet. 2014, 23, 397–407. [Google Scholar] [CrossRef] [PubMed]
- Ovejero, D.; Lim, Y.H.; Boyce, A.M.; Gafni, R.I.; McCarthy, E.; Nguyen, T.A.; Eichenfield, L.F.; DeKlotz, C.M.C.; Guthrie, L.C.; Tosi, L.L.; et al. Cutaneous Skeletal Hypophosphatemia Syndrome: Clinical Spectrum, Natural History, and Treatment. Osteoporos. Int. 2016, 27, 3615–3626. [Google Scholar] [CrossRef] [PubMed]
- Bourdeaut, F.; Herault, A.; Gentien, D.; Pierron, G.; Ballet, S.; Reynaud, S.; Paris, R.; Schleiermacher, G.; Baumann, C.; Philippe-Chomette, P.; et al. Mosaicism for Oncogenic G12D KRAS Mutation Associated with Epidermal Nevus, Polycystic Kidneys and Rhabdomyosarcoma. J. Med. Genet. 2010, 47, 859–862. [Google Scholar] [CrossRef]
- Mussa, A.; Leoni, C.; Iacoviello, M.; Carli, D.; Ranieri, C.; Pantaleo, A.; Buonuomo, P.S.; Bagnulo, R.; Ferrero, G.B.; Bartuli, A.; et al. Genotypes and Phenotypes Heterogeneity in PIK3CA-Related Overgrowth Spectrum and Overlapping Conditions: 150 Novel Patients and Systematic Review of 1007 Patients with PIK3CA Pathogenetic Variants. J. Med. Genet. 2022, 60, 163–173. [Google Scholar] [CrossRef]
- Farschtschi, S.; Mautner, V.-F.; Hollants, S.; Hagel, C.; Spaepen, M.; Schulte, C.; Legius, E.; Brems, H. Keratinocytic Epidermal Nevus Syndrome with Schwann Cell Proliferation, Lipomatous Tumour and Mosaic KRAS Mutation. BMC Med. Genet. 2015, 16, 6. [Google Scholar] [CrossRef] [PubMed]
- Levinsohn, J.L.; Tian, L.C.; Boyden, L.M.; McNiff, J.M.; Narayan, D.; Loring, E.S.; Yun, D.; Sugarman, J.L.; Overton, J.D.; Mane, S.M.; et al. Whole-Exome Sequencing Reveals Somatic Mutations in HRAS and KRAS, Which Cause Nevus Sebaceus. J. Investig. Dermatol. 2013, 133, 827–830. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, B.J.; Rogers, G.F.; Wood, B.C. A Patient with Schimmelpenning Syndrome and Mosaic KRAS Mutation. J. Craniofacial Surg. 2019, 30, 184–185. [Google Scholar] [CrossRef] [PubMed]
- Nagatsuma, M.; Takasawa, K.; Yamauchi, T.; Nakagawa, R.; Mizuno, T.; Tanaka, E.; Yamamoto, K.; Uemura, N.; Kashimada, K.; Morio, T. A Postzygotic KRAS Mutation in a Patient with Schimmelpenning Syndrome Presenting with Lipomatosis, Renovascular Hypertension, and Diabetes Mellitus. J. Hum. Genet. 2019, 64, 177–181. [Google Scholar] [CrossRef] [PubMed]
- Vidaurri-de la Cruz, H.; Tamayo-Sánchez, L.; Durán-McKinster, C.; De La Luz Orozco-Covarrubias, M.; Ruiz-Maldonado, R. Epidermal Nevus Syndromes: Clinical Findings in 35 Patients. Pediatr. Dermatol. 2004, 21, 432–439. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Qian, Y.; Wu, B.; Zhang, P.; Zhou, W. KRAS G12D Mosaic Mutation in a Chinese Linear Nevus Sebaceous Syndrome Infant. BMC Med. Genet. 2015, 16, 101. [Google Scholar] [CrossRef] [PubMed]
- Gazzin, A.; Fornari, F.; Niceta, M.; Leoni, C.; Dentici, M.L.; Carli, D.; Villar, A.M.; Calcagni, G.; Banaudi, E.; Massuras, S.; et al. Defining the Variant-Phenotype Correlation in Patients Affected by Noonan Syndrome with the RAF1:C.770C>T Variant. Eur. J. Hum. Genet. 2024, in press. [Google Scholar] [CrossRef] [PubMed]
- Binder, G.; Grathwol, S.; Von Loeper, K.; Blumenstock, G.; Kaulitz, R.; Freiberg, C.; Webel, M.; Lissewski, C.; Zenker, M.; Paul, T. Health and Quality of Life in Adults with Noonan Syndrome. J. Pediatr. 2012, 161, 501–505.e1. [Google Scholar] [CrossRef] [PubMed]
- Romano, A.A.; Allanson, J.E.; Dahlgren, J.; Gelb, B.D.; Hall, B.; Pierpont, M.E.; Roberts, A.E.; Robinson, W.; Takemoto, C.M.; Noonan, J.A. Noonan Syndrome: Clinical Features, Diagnosis, and Management Guidelines. Pediatrics 2010, 126, 746–759. [Google Scholar] [CrossRef]
- Prendiville, T.W.; Gauvreau, K.; Tworog-Dube, E.; Patkin, L.; Kucherlapati, R.S.; Roberts, A.E.; Lacro, R.V. Cardiovascular Disease in Noonan Syndrome. Arch. Dis. Child. 2014, 99, 629–634. [Google Scholar] [CrossRef]
- Calcagni, G.; Adorisio, R.; Martinelli, S.; Grutter, G.; Baban, A.; Versacci, P.; Digilio, M.C.; Drago, F.; Gelb, B.D.; Tartaglia, M.; et al. Clinical Presentation and Natural History of Hypertrophic Cardiomyopathy in RASopathies. Heart Fail. Clin. 2018, 14, 225–235. [Google Scholar] [CrossRef] [PubMed]
- Gelb, B.D.; Yohe, M.E.; Wolf, C.; Andelfinger, G. New Prospectives on Treatment Opportunities in RASopathies. Am. J. Med. Genet. C Semin. Med. Genet. 2022, 190, 541–560. [Google Scholar] [CrossRef] [PubMed]
- Sleutjes, J.; Kleimeier, L.; Leenders, E.; Klein, W.; Draaisma, J. Lymphatic Abnormalities in Noonan Syndrome Spectrum Disorders: A Systematic Review. Mol. Syndromol. 2022, 13, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Bellini, C.; Cabano, R.; De Angelis, L.C.; Bellini, T.; Calevo, M.G.; Gandullia, P.; Ramenghi, L.A. Octreotide for Congenital and Acquired Chylothorax in Newborns: A Systematic Review. J. Paediatr. Child. Health 2018, 54, 840–847. [Google Scholar] [CrossRef] [PubMed]
- Biko, D.M.; Reisen, B.; Otero, H.J.; Ravishankar, C.; Victoria, T.; Glatz, A.C.; Rome, J.J.; Dori, Y. Imaging of Central Lymphatic Abnormalities in Noonan Syndrome. Pediatr. Radiol. 2019, 49, 586–592. [Google Scholar] [CrossRef] [PubMed]
- Nakano, T.A.; Rankin, A.W.; Annam, A.; Kulungowski, A.M.; McCallen, L.M.; Hill, L.R.; Chatfield, K.C. Trametinib for Refractory Chylous Effusions and Systemic Complications in Children with Noonan Syndrome. J. Pediatr. 2022, 248, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Adams, D.M.; Trenor, C.C.; Hammill, A.M.; Vinks, A.A.; Patel, M.N.; Chaudry, G.; Wentzel, M.S.; Mobberley-Schuman, P.S.; Campbell, L.M.; Brookbank, C.; et al. Efficacy and Safety of Sirolimus in the Treatment of Complicated Vascular Anomalies. Pediatrics 2016, 137, e20153257. [Google Scholar] [CrossRef]
- Hammill, A.M.; Wentzel, M.; Gupta, A.; Nelson, S.; Lucky, A.; Elluru, R.; Dasgupta, R.; Azizkhan, R.G.; Adams, D.M. Sirolimus for the Treatment of Complicated Vascular Anomalies in Children. Pediatr. Blood Cancer 2011, 57, 1018–1024. [Google Scholar] [CrossRef] [PubMed]
- Saibene, A.M.; Rosso, C.; Felisati, G.; Pignataro, L.; Schindler, A.; Ghilardi, G.; Colletti, G.; Gaffuri, M.; Mozzanica, F. Sirolimus Treatment for Paediatric Head and Neck Lymphatic Malformations: A Systematic Review. Eur. Arch. Oto-Rhino-Laryngol. 2023, 280, 3529–3540. [Google Scholar] [CrossRef]
- Rajalingam, K.; Schreck, R.; Rapp, U.R.; Albert, Š. Ras Oncogenes and Their Downstream Targets. Biochim. Et Biophys. Acta (BBA)-Mol. Cell Res. 2007, 1773, 1177–1195. [Google Scholar] [CrossRef]
- Ohren, J.F.; Chen, H.; Pavlovsky, A.; Whitehead, C.; Zhang, E.; Kuffa, P.; Yan, C.; McConnell, P.; Spessard, C.; Banotai, C.; et al. Structures of Human MAP Kinase Kinase 1 (MEK1) and MEK2 Describe Novel Noncompetitive Kinase Inhibition. Nat. Struct. Mol. Biol. 2004, 11, 1192–1197. [Google Scholar] [CrossRef] [PubMed]
- Ullah, R.; Yin, Q.; Snell, A.H.; Wan, L. RAF-MEK-ERK Pathway in Cancer Evolution and Treatment. Semin. Cancer Biol. 2022, 85, 123–154. [Google Scholar] [CrossRef] [PubMed]
- Sheppard, S.E.; March, M.E.; Seiler, C.; Matsuoka, L.S.; Kim, S.E.; Kao, C.; Rubin, A.I.; Battig, M.R.; Khalek, N.; Schindewolf, E.; et al. Lymphatic Disorders Caused by Mosaic, Activating KRAS Variants Respond to MEK Inhibition. JCI Insight 2023, 8, e155888. [Google Scholar] [CrossRef] [PubMed]
- Andelfinger, G.; Marquis, C.; Raboisson, M.-J.; Théoret, Y.; Waldmüller, S.; Wiegand, G.; Gelb, B.D.; Zenker, M.; Delrue, M.-A.; Hofbeck, M. Hypertrophic Cardiomyopathy in Noonan Syndrome Treated by MEK-Inhibition. J. Am. Coll. Cardiol. 2019, 73, 2237–2239. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, A.; Beasley, G.; Martinez, H.; Jesudas, R.; Anton-Martin, P.; Christakopoulos, G.; Kramer, J. Selumetinib for Refractory Pulmonary and Gastrointestinal Bleeding in Noonan Syndrome. Pediatrics 2022, 150, e2022056336. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.A.; Perrier, R.; Kurek, K.C.; Estrada-Veras, J.; Lehman, A.; Yip, S.; Hendson, G.; Diamond, C.; Pinchot, J.W.; Tran, J.M.; et al. Novel Findings and Expansion of Phenotype in a Mosaic RASopathy Caused by Somatic KRAS Variants. Am. J. Med. Genet. A 2021, 185, 2829–2845. [Google Scholar] [CrossRef] [PubMed]
- Copland, E.; Pearson, B. Congenital Melanocytic Naevus Syndrome, Is There a Role for Trametinib Monotherapy? J. Paediatr. Child. Health 2023, 59, 697–699. [Google Scholar] [CrossRef] [PubMed]
- D’Onofrio, G.; Delrue, M.A.; Lortie, A.; Marquis, C.; Striano, P.; Jaworski, M.; Andelfinger, G.; Perreault, S. Treatment of Refractory Epilepsy with MEK Inhibitor in Patients with RASopathy. Pediatr. Neurol. 2023, 148, 148–151. [Google Scholar] [CrossRef] [PubMed]
- Dori, Y.; Smith, C.; Pinto, E.; Snyder, K.; March, M.E.; Hakonarson, H.; Belasco, J. Severe Lymphatic Disorder Resolved with MEK Inhibition in a Patient with Noonan Syndrome and SOS1 Mutation. Pediatrics 2020, 146, e20200167. [Google Scholar] [CrossRef]
- Foster, J.B.; Li, D.; March, M.E.; Sheppard, S.E.; Adams, D.M.; Hakonarson, H.; Dori, Y. Kaposiform Lymphangiomatosis Effectively Treated with MEK Inhibition. EMBO Mol. Med. 2020, 12, e12324. [Google Scholar] [CrossRef]
- Gordon, K.; Moore, M.; Van Zanten, M.; Pearce, J.; Itkin, M.; Madden, B.; Ratnam, L.; Mortimer, P.S.; Nagaraja, R.; Mansour, S. Case Report: Progressive Central Conducting Lymphatic Abnormalities in the RASopathies. Two Case Reports, Including Successful Treatment by MEK Inhibition. Front. Genet. 2022, 13, 1001105. [Google Scholar] [CrossRef]
- Hribernik, I.; Brooks, T.; Dunlop-Jones, A.; Bentham, J.R. Successful Treatment of Refractory Chylothorax with MEK Inhibitor Trametinib in a Child with Noonan Syndrome: Case Report. Eur. Heart J. Case Rep. 2023, 7, ytad190. [Google Scholar] [CrossRef] [PubMed]
- Leegaard, A.; Gregersen, P.A.; Nielsen, T.; Bjerre, J.V.; Handrup, M.M. Succesful MEK-Inhibition of Severe Hypertrophic Cardiomyopathy in RIT1-Related Noonan Syndrome. Eur. J. Med. Genet. 2022, 65, 104630. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; March, M.E.; Gutierrez-Uzquiza, A.; Kao, C.; Seiler, C.; Pinto, E.; Matsuoka, L.S.; Battig, M.R.; Bhoj, E.J.; Wenger, T.L.; et al. ARAF Recurrent Mutation Causes Central Conducting Lymphatic Anomaly Treatable with a MEK Inhibitor. Nat. Med. 2019, 25, 1116–1122. [Google Scholar] [CrossRef] [PubMed]
- Lioncino, M.; Fusco, A.; Monda, E.; Colonna, D.; Sibilio, M.; Caiazza, M.; Magri, D.; Borrelli, A.C.; D’Onofrio, B.; Mazzella, M.L.; et al. Severe Lymphatic Disorder and Multifocal Atrial Tachycardia Treated with Trametinib in a Patient with Noonan Syndrome and SOS1 Mutation. Genes 2022, 13, 1503. [Google Scholar] [CrossRef]
- Meisner, J.K.; Bradley, D.J.; Russell, M.W. Molecular Management of Multifocal Atrial Tachycardia in Noonan’s Syndrome with MEK1/2 Inhibitor Trametinib. Circ. Genom. Precis. Med. 2021, 14, E003327. [Google Scholar] [CrossRef]
- Carli, D.; Cardaropoli, S.; Tessaris, D.; Coppo, P.; La Selva, R.; Cesario, C.; Lepri, F.R.; Pullano, V.; Palumbo, M.; Ramenghi, U.; et al. Successful Treatment with MEK-Inhibitor in a Patient with NRAS-Related Cutaneous Skeletal Hypophosphatemia Syndrome. Genes Chromosomes Cancer 2022, 61, 740–746. [Google Scholar] [CrossRef]
- Chowers, G.; Abebe-Campino, G.; Golan, H.; Vivante, A.; Greenberger, S.; Soudack, M.; Barkai, G.; Fox-Fisher, I.; Li, D.; March, M.; et al. Treatment of Severe Kaposiform Lymphangiomatosis Positive for NRAS Mutation by MEK-Inhibition. Pediatr. Res. 2023, 94, 1911–1915. [Google Scholar] [CrossRef]
- Wu, X.; Simpson, J.; Hong, J.H.; Kim, K.H.; Thavarajah, N.K.; Backx, P.H.; Neel, B.G.; Araki, T. MEK-ERK Pathway Modulation Ameliorates Disease Phenotypes in a Mouse Model of Noonan Syndrome Associated with the Raf1L613V Mutation. J. Clin. Investig. 2011, 121, 1009–1025. [Google Scholar] [CrossRef]
- Chen, P.-C.; Wakimoto, H.; Conner, D.; Araki, T.; Yuan, T.; Roberts, A.; Seidman, C.E.; Bronson, R.; Neel, B.G.; Seidman, J.G.; et al. Activation of Multiple Signaling Pathways Causes Developmental Defects in Mice with a Noonan Syndrome–Associated Sos1 Mutation. J. Clin. Investig. 2010, 120, 4353–4365. [Google Scholar] [CrossRef]
- Hernández-Porras, I.; Fabbiano, S.; Schuhmacher, A.J.; Aicher, A.; Cañamero, M.; Cámara, J.A.; Cussó, L.; Desco, M.; Heeschen, C.; Mulero, F.; et al. K-RasV14I Recapitulates Noonan Syndrome in Mice. Proc. Natl. Acad. Sci. USA 2014, 111, 16395–16400. [Google Scholar] [CrossRef] [PubMed]
- Inoue, S.; Moriya, M.; Watanabe, Y.; Miyagawa-Tomita, S.; Niihori, T.; Oba, D.; Ono, M.; Kure, S.; Ogura, T.; Matsubara, Y.; et al. New BRAF Knockin Mice Provide a Pathogenetic Mechanism of Developmental Defects and a Therapeutic Approach in Cardio-Facio-Cutaneous Syndrome. Hum. Mol. Genet. 2014, 23, 6553–6566. [Google Scholar] [CrossRef] [PubMed]
- Nakhaei-Rad, S.; Haghighi, F.; Bazgir, F.; Dahlmann, J.; Busley, A.V.; Buchholzer, M.; Kleemann, K.; Schänzer, A.; Borchardt, A.; Hahn, A.; et al. Molecular and Cellular Evidence for the Impact of a Hypertrophic Cardiomyopathy-Associated RAF1 Variant on the Structure and Function of Contractile Machinery in Bioartificial Cardiac Tissues. Commun. Biol. 2023, 6, 657. [Google Scholar] [CrossRef]
- Goodwin, A.F.; Tidyman, W.E.; Jheon, A.H.; Sharir, A.; Zheng, X.; Charles, C.; Fagin, J.A.; McMahon, M.; Diekwisch, T.G.H.; Ganss, B.; et al. Abnormal Ras Signaling in Costello Syndrome (CS) Negatively Regulates Enamel Formation. Hum. Mol. Genet. 2014, 23, 682–692. [Google Scholar] [CrossRef] [PubMed]
- Anastasaki, C.; Rauen, K.A.; Patton, E.E. Continual and Partial MEK Inhibition Ameliorates Cardio-Facio-Cutaneous Phenotypes in Zebrafish. Dis. Model. Mech. 2012, 5, 546–552. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.-S.; Ehninger, D.; Zhou, M.; Oh, J.-Y.; Kang, M.; Kwak, C.; Ryu, H.-H.; Butz, D.; Araki, T.; Cai, Y.; et al. Mechanism and Treatment for Learning and Memory Deficits in Mouse Models of Noonan Syndrome. Nat. Neurosci. 2014, 17, 1736–1743. [Google Scholar] [CrossRef] [PubMed]
- Gross, A.M.; Frone, M.; Gripp, K.W.; Gelb, B.D.; Schoyer, L.; Schill, L.; Stronach, B.; Biesecker, L.G.; Esposito, D.; Hernandez, E.R.; et al. Advancing RAS/RASopathy Therapies: An NCI-sponsored Intramural and Extramural Collaboration for the Study of RASopathies. Am. J. Med. Genet. A 2020, 182, 866–876. [Google Scholar] [CrossRef] [PubMed]
- Mussa, A.; Carli, D.; Giorgio, E.; Villar, A.M.; Cardaropoli, S.; Carbonara, C.; Campagnoli, M.F.; Galletto, P.; Palumbo, M.; Olivieri, S.; et al. Mek Inhibition in a Newborn with Raf1-Associated Noonan Syndrome Ameliorates Hypertrophic Cardiomyopathy but Is Insufficient to Revert Pulmonary Vascular Disease. Genes 2022, 13, 6. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, C.L.; Flanagan, S.; Murati, M.; Boull, C.; McGough, E.; Ameduri, R.; Weigel, B.; Maguiness, S. Successful Management of an Arteriovenous Malformation with Trametinib in a Patient with Capillary-Malformation Arteriovenous Malformation Syndrome and Cardiac Compromise. Pediatr. Dermatol. 2022, 39, 316–319. [Google Scholar] [CrossRef]
- Walsh, K.S.; Wolters, P.L.; Widemann, B.C.; del Castillo, A.; Sady, M.D.; Inker, T.; Roderick, M.C.; Martin, S.; Toledo-Tamula, M.A.; Struemph, K.; et al. Impact of MEK Inhibitor Therapy on Neurocognitive Functioning in NF1. Neurol. Genet. 2021, 7, e616. [Google Scholar] [CrossRef]
- Geoerger, B.; Moertel, C.L.; Whitlock, J.; McCowage, G.B.; Kieran, M.W.; Broniscer, A.; Hargrave, D.R.; Hingorani, P.; Kilburn, L.B.; Mueller, S.; et al. Phase 1 Trial of Trametinib Alone and in Combination with Dabrafenib in Children and Adolescents with Relapsed Solid Tumors or Neurofibromatosis Type 1 (NF1) Progressive Plexiform Neurofibromas (PN). J. Clin. Oncol. 2018, 36, 10537. [Google Scholar] [CrossRef]
- Casey, D.; Demko, S.; Sinha, A.; Mishra-Kalyani, P.S.; Shen, Y.; Khasar, S.; Goheer, M.A.; Helms, W.S.; Pan, L.; Xu, Y.; et al. FDA Approval Summary: Selumetinib for Plexiform Neurofibroma. Clin. Cancer Res. 2021, 27, 4142–4146. [Google Scholar] [CrossRef] [PubMed]
- de Blank, P.M.K.; Gross, A.M.; Akshintala, S.; Blakeley, J.O.; Bollag, G.; Cannon, A.; Dombi, E.; Fangusaro, J.; Gelb, B.D.; Hargrave, D.; et al. MEK Inhibitors for Neurofibromatosis Type 1 Manifestations: Clinical Evidence and Consensus. Neuro Oncol. 2022, 24, 1845–1856. [Google Scholar] [CrossRef] [PubMed]
- Marin, T.M.; Keith, K.; Davies, B.; Conner, D.A.; Guha, P.; Kalaitzidis, D.; Wu, X.; Lauriol, J.; Wang, B.; Bauer, M.; et al. Rapamycin Reverses Hypertrophic Cardiomyopathy in a Mouse Model of LEOPARD Syndrome–Associated PTPN11 Mutation. J. Clin. Investig. 2011, 121, 1026–1043. [Google Scholar] [CrossRef] [PubMed]
- Monda, E.; Rubino, M.; Lioncino, M.; Di Fraia, F.; Pacileo, R.; Verrillo, F.; Cirillo, A.; Caiazza, M.; Fusco, A.; Esposito, A.; et al. Hypertrophic Cardiomyopathy in Children: Pathophysiology, Diagnosis, and Treatment of Non-Sarcomeric Causes. Front. Pediatr. 2021, 9, 632293. [Google Scholar] [CrossRef] [PubMed]
- Saint-Laurent, C.; Mazeyrie, L.; Yart, A.; Edouard, T. Novel Therapeutic Perspectives in Noonan Syndrome and RASopathies. Eur. J. Pediatr. 2023, 183, 1011–1019. [Google Scholar] [CrossRef] [PubMed]
- Hahn, A.; Lauriol, J.; Thul, J.; Behnke-Hall, K.; Logeswaran, T.; Schänzer, A.; Böğürcü, N.; Garvalov, B.K.; Zenker, M.; Gelb, B.D.; et al. Rapidly Progressive Hypertrophic Cardiomyopathy in an Infant with Noonan Syndrome with Multiple Lentigines: Palliative Treatment with a Rapamycin Analog. Am. J. Med. Genet. A 2015, 167, 744–751. [Google Scholar] [CrossRef]
- Sideris, E.; Tng, E.T.V.; Chee, P. Lymphatic Malformation Responsive to Sirolimus in Keratinocytic Epidermal Nevus Syndrome with KRAS Mutation: A Case and Brief Literature Discussion. Case Rep. Dermatol. 2021, 13, 195–201. [Google Scholar] [CrossRef]

{kind=link}
| First Author and Year of Publication | Clinical Diagnosis | Genotype | Age | Drug | Dose | First Improvement | Chief Indication | Observation Period | Therapeutic Effect | Exitus | AE |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Andelfinger, 2019 [34] | NS | RIT1:c.104G>C p.Ser35Thr, Heterozygous | 14 weeks | Trametinib | 0.020 mg/kg/day | 3 months | HCM | 17 months | HCM and NT-pro-BNP normalization. Valvular and subvalvular obstruction improved. Growth improvement. | - | - |
| Andelfinger, 2019 [34] | NS | RIT1:c.246T>G, p.Phe82Leu, Heterozygous | 13 weeks | Trametinib | 0.027 mg/kg/day | 3 months | HCM | 17 months | HCM and NT-pro-BNP normalization, valvular and subvalvular obstruction improved. Chylous effusions ceased. Growth improvement. | - | - |
| Li, 2019 [44] | GLA | ARAF:c.640T>C p.Ser214Pro, Heterozygous | 13 years | Trametinib | 1 mg/day | 2 months | CCLA | 1 year | Pulmonary function test improvement. Hyponatriemia and hypokaliemia resolution. Lymphatic remodeling with restructuring of lymphatic system. | - | - |
| Dori, 2020 [39] | NS | SOS1:c.2536G>A p.Glu846Lys, Heterozygous | 5 years | Trametinib | 0.010 mg/kg/day escalated to 0.02 mg/kg/day | - | Bleeding retroperitoneal and duodenal lymphangiectasia, chylothorax. | - | Symptom resolution. Improvement in chest radiograph signs. Normalization of albumin and hemoglobin levels without need for transfusion. Pulmonary edema and intestinal leakage reduction. Complete normalization of the duodenal mucosa. | - | - |
| Foster, 2020 [40] | KLA | CBL:c.2322T>G p.Tyr774*, VAF 4% frequency (pleural effusion fluid) | 18 years | Trametinib | 0.010 mg/kg/day in 28 day cycles, than daily | 1 week | KLA with severe bilateral pulmonary interstitial and mediastinal perfusion | 12 months | Subjectively improved symptoms. Improved restrictive lung disease. D-dimer value normalization. Complete resolution of pleural effusions and pulmonary interstitial edema. | - | Grade 1 acneiform rash, brief eosinophilia, and brief hematuria and proteinuria. |
| Meisner, 2021 [46] | NS | RAF1:c.770C>T p.Ser257Leu, Heterozygous | 20 weeks | Trametinib | 0.025 mg/kg/day de-escalated to 0.01875 mg/kg/day | 2 days | MAT, HCM, and chylothorax | - | MAT episodes resolution. HCM improvement. Amiodarone and diltiazem weaning. | - | Severe diarrhea. |
| Chang, 2021 [36] | CM-AVM | KRAS p.Gln61His, low allele frequency consistent with mosaic origin (nasal epithelium) | 15 years | Trametinib | uptitration to 1.5 mg/day | - | High-flow facial AVM with epistaxis | - | Clinical improvement and decreased epistaxis and need for RBC transfusion. | - | Acneiform eruptions and intermittent paronychia. |
| Nicholson, 2022 [59] | CM-AVM | EPHB4:c.2173G>A p.Ala725Thr (unspecified sample) | 16 years | Trametinib | 2 mg/day in 13 cycles of 28 days de escalated to 0.5 mg/day | - | Cardiac compromise in CM-AVM | - | Shunting improvement. | - | Acneiform eruptions, paronychia, air lightning. |
| Leegaard, 2022 [43] | NS | RIT1:c.170C>G p.Ala57Gly, Heterozygous | 6 months | Trametinib | 0.025 mg/kg/day escalated to 0.04 mg/kg/day | 1 month | HCM | 21 months | Complete regression of HCM | - | Dry skin and skin rash. |
| Mussa, 2022 [10] | NS | RAF1:c.770C>T p.Ser257Leu, Heterozygous | 47 days | Trametinib | 0.022 mg/kg/day | 4 days | HCM | 57 days | Weaning from mechanical ventilation, inotrope demand reduction, NT-proBNP values reduction, Ross score improvement, echocardiographic improvement with septal thickness reduction. | Refractory congestive heart failure due to pulmonary hypertension and pulmonary artery dilatation. | - |
| Lioncino, 2022 [45] | NS | SOS1:c.1655G>C p.Arg552Thr, Heterozygous | 9 weeks | Trametinib | 0.020 mg/kg/day | 4 days | MAT and pleural effusion | 4 months | Pleural effusion resolution, incessant MAT episodes resolution with anti-arrhythmic withdrawn, improvement in respiratory parameters with ventilation weaning, significant reduction in consolidation areas. | - | - |
| Nakano, 2022 [26] | NS | RIT1:c.246T>G p.Phe82Leu, Heterozygous | 4 years | Trametinib | 0.025 mg/kg/day | 1 month | Chylotorax and HCM | 2 years (administration time 1 year) | Chylotorax reduction, slight decline in NT-pro-BNP value. Growth improvement. | - | - |
| Nakano, 2022 [26] | NS | SOS1:c.1322G>A p.Cys441Tyr, Heterozygous | 3 months | Trametinib | 0.026 mg/kg/day de-escalated to 0.013 mg/kg/day | 1 month | Chilotorax and ascites | 2 y (administration time 1 year) | Chylotorax reduction, ventilation weaning, gradual improvement in pulmonary valve stenosis. Growth improvement. | - | Grade 2 skin irritation. |
| Nakano, 2022 [26] | NS | PTPN11:c.854T>C p.Phe285Ser, Heterozygous | 4 months | Trametinib | 0.023 mg/kg/day | 1 month | HCM and chylotorax | few months | Chylous effusions and ascites improvement. Cardiac function stabilization, NT-proBNP reduction, HCM partial improvement, slight improvement in the pulmonary valve gradient. Mechanical ventilation weaning. | Yes. Acute cardiorespiratory event. The suspected cause was a sudden cardiac event. | - |
| Chakraborty, 2022 [35] | NS | PTPN11(unspecified) p.Gln510Glu | 15 years | Selumetinib | 6.7 mg/m2 twice a day | - | Refractory pulmonary and gastrointestinal bleeding | 1 year | Bleeding resolution. | - | - |
| Hribernik, 2022 [42] | NS | RIT1 variant (unspecified), Heterozygous | 3 years | Trametinib | 0.032 mg/kg/day | - | Chylothorax and HCM | 8 months (Administration time 3 months) | Reduction in chest drainage frequency. HCM improvement. | - | Severe eczema and increased stoma output. |
| Gordon, 2022 [41] | NS | RIT1:c.246T>G p.Phe82Leu, Heterozygous | 22 years | Trametinib | 1 mg/day escalated to 2 mg/day | 3 months | CCLA | 28 months | Dramatic and sustained clinical improvement. He showed a total resolution of ascites within 3 months and pericardial effusion resolve 18 months into treatment | - | Mild nausea, gastritis, constipation, and eczema of the lower legs. Iron deficiency anemia requiring an iron infusion. |
| Carli, 2022 [47] | CSHS | NRAS:c.182A > G, p.Gln61Arg, VAF 29% (epidermal nevus) | 4 years | Trametinib | 0.032 mg/kg/day de-escalated to 0.025 mg/kg/day | 11 days | Hypophosphatemic rickets and chylotorax | - | Normalization of serum phosphate and renal reabsorption., catch-up growth skin lesions, X-ray and densitometry bone mineralization improvement. | - | Hungry bone syndrome, asymptomatic hyperkaliemia and mild asymptomatic creatinine phosphokinase (CPK) elevation. |
| Sheppard, 2023 [33] | Oculoectodermal syndrome | KRAS p.Gly13Asp, VAF 10.3–38.8% (hyperpigmented skin, periosteum, muscle, and humerus samples) | - | Trametinib | 0.025 mg/kg/day | - | CCLA | - | - | - | - |
| Sheppard, 2023 [33] | Mosaic KRAS-opathy | KRAS:c.436G > T p.Ala146Thr, VAF at 3.3–3.4% (scrotal tissue) | - | Trametinib | 0.005 mg/kg/day | - | CCLA | - | - | - | Rhabdomyolysis |
| Chowers, 2023 [48] | KLA | NRAS:c.182A>G, p.Gln61Arg, VAF 0.2% (unspecified sample) | 9 years | Trametinib | 0.025 mg/kg/day | - | Pericardial and pleural chylous effusions | 11 months | Symptoms and signs improvement, increased Lansky performance test, increased body weight, improvement in lung function tests, radiological improvement, wean off nocturnal oxygen supplementation, platelets count normalization and D-dimer decrease, weaning of steroid therapy. | - | Mild facial acneiform rash and hair loss. |
| D’onofrio, 2023 [38] | CFC | BRAF p.Phe595Leu, Heterozygous | 7 years | Trametinib | 0.025 mg/kg/day | 3 months | Drug-resistant, recurrent tonic-colonic seizures | 6 months | Dramatic reduction in electroencephalographic anomalies, marked clinical improvement. | - | - |
| D’onofrio, 2023 [38] | Schimmelpenning syndrome | KRAS p.Gly12Asp, postzygotic somatic (skin) | 26 months | Trametinib | 0.025 mg/kg/day escalated to 0.0375 mg/kg/day de-escalated to 0.025 mg/kg/day | - | Right focal motor seizures | 22 months | Seizure frequency and skin lesions dimension reduction. | - | Suspected drug induced inflammatory colitis and hypovolemic shock during viral gastroenteritis. Eczematous skin lesions. |
| Copland, 2023 [37] | Congenital melanocytic naevus syndrome | NRAS Gln61Lys (skin) | 13 months | Trametinib | 0.032 mg/kg/die | 28 days | Focal seizures | 1 year | Transient seizure activity resolution, antiepileptic weaning, progression of motor skills, reduction in nevus pigmentation intensity. Progression of symptoms after 10 weeks of therapy. | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gazzin, A.; Fornari, F.; Cardaropoli, S.; Carli, D.; Tartaglia, M.; Ferrero, G.B.; Mussa, A. Exploring New Drug Repurposing Opportunities for MEK Inhibitors in RASopathies: A Comprehensive Review of Safety, Efficacy, and Future Perspectives of Trametinib and Selumetinib. Life 2024, 14, 731. https://doi.org/10.3390/life14060731
Gazzin A, Fornari F, Cardaropoli S, Carli D, Tartaglia M, Ferrero GB, Mussa A. Exploring New Drug Repurposing Opportunities for MEK Inhibitors in RASopathies: A Comprehensive Review of Safety, Efficacy, and Future Perspectives of Trametinib and Selumetinib. Life. 2024; 14(6):731. https://doi.org/10.3390/life14060731
Chicago/Turabian StyleGazzin, Andrea, Federico Fornari, Simona Cardaropoli, Diana Carli, Marco Tartaglia, Giovanni Battista Ferrero, and Alessandro Mussa. 2024. "Exploring New Drug Repurposing Opportunities for MEK Inhibitors in RASopathies: A Comprehensive Review of Safety, Efficacy, and Future Perspectives of Trametinib and Selumetinib" Life 14, no. 6: 731. https://doi.org/10.3390/life14060731
APA StyleGazzin, A., Fornari, F., Cardaropoli, S., Carli, D., Tartaglia, M., Ferrero, G. B., & Mussa, A. (2024). Exploring New Drug Repurposing Opportunities for MEK Inhibitors in RASopathies: A Comprehensive Review of Safety, Efficacy, and Future Perspectives of Trametinib and Selumetinib. Life, 14(6), 731. https://doi.org/10.3390/life14060731