
The Association of Depression with Obstructive Sleep Apnea in Patients with Cystic and Non-Cystic Fibrosis Bronchiectasis

Abstract
:1. Introduction
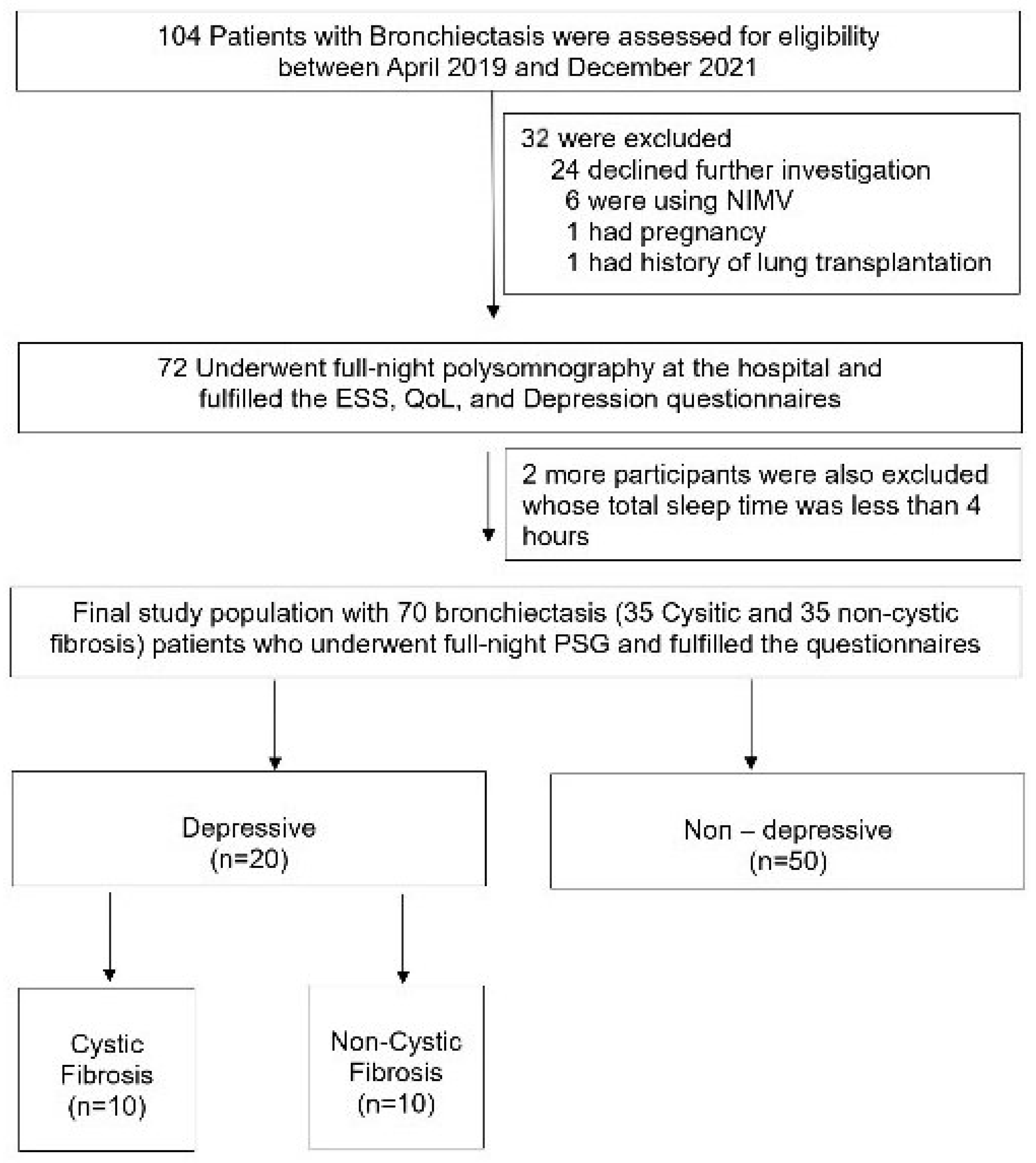
2. Materials and Methods
2.1. Polysomnography
2.2. Comorbidities
2.3. Group Assignment
2.4. Epworth Sleepiness Scale
2.5. Zung Self-Rating Depression Scale
2.6. Pulmonary Function Testing
2.7. The Modified Medical Research Council Dyspnea Scale and Charlson Scores
2.8. Statistics
3. Results
3.1. Demographics, Clinical Characteristics, and Sleep Parameters of All the Participants
3.2. Demographics, Clinical Characteristics, and Sleep Parameters of the CF Patients
3.3. Associates of Depressive Mood among CF and Non-CF Adults
3.4. Factors Affecting Depressive Mood among CF Participants
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bradley, T.D.; Phillipson, E.A. Pathogenesis and pathophysiology of the obstructive sleep apnea syndrome. Med. Clin. N. Am. 1985, 69, 1169–1185. [Google Scholar] [CrossRef] [PubMed]
- Chassagnon, G.; Brun, A.L.; Bennani, S.; Chergui, N.; Freche, G.; Revel, M.-P. Bronchiectasis imaging. Rev. Pneumol. Clin. 2018, 74, 299–314. [Google Scholar] [CrossRef]
- Magis-Escurra, C.; Reijers, M.H. Bronchiectasis. BMJ Clin. Evid. 2015, 2015, 1507. [Google Scholar]
- Radlović, N. Cystic fibrosis. Srp. Arh. Celok. Lek. 2012, 140, 244–249. [Google Scholar] [CrossRef]
- Spicuzza, L.; Sciuto, C.; Leonardi, S.; La Rosa, M. Early occurrence of obstructive sleep apnea in infants and children with cystic fibrosis. Arch. Pediatr. Adolesc. Med. 2012, 166, 1165–1169. [Google Scholar] [CrossRef] [PubMed]
- Jagpal, S.K.; Jobanputra, A.M.; Ahmed, O.H.; Santiago, T.V.; Ramagopal, M. Sleep-disordered breathing in cystic fibrosis. Pediatr. Pulmonol. 2021, 56 (Suppl. S1), S23–S31. [Google Scholar] [CrossRef] [PubMed]
- Welsner, M.; Dietz-Terjung, S.; Stehling, F.; Schulte, T.; Niehammer, U.; Gahbiche, F.-E.; Taube, C.; Strassburg, S.; Schoebel, C.; Weinreich, G.; et al. Obstructive sleep apnea and nocturnal hypoxemia in adult patients with cystic fibrosis. BMC Pulm. Med. 2022, 22, 446. [Google Scholar] [CrossRef]
- Shakkottai, A.; Irani, S.; Nasr, S.Z.; O’Brien, L.M.; Chervin, R.D. Risk factors for obstructive sleep apnea in cystic fibrosis. Pediatr. Pulmonol. 2022, 57, 926–934. [Google Scholar] [CrossRef] [PubMed]
- Dancey, D.R.; Tullis, E.D.; Heslegrave, R.; Thornley, K.; Hanly, P.J. Sleep quality and daytime function in adults with cystic fibrosis and severe lung disease. Eur. Respir. J. 2002, 19, 504–510. [Google Scholar] [CrossRef]
- Kapur, V.K.; Auckley, D.H.; Chowdhuri, S.; Kuhlmann, D.C.; Mehra, R.; Ramar, K.; Harrod, C.G. Clinical Practice Guideline for Diagnostic Testing for Adult Obstructive Sleep Apnea: An American Academy of Sleep Medicine Clinical Practice Guideline. J. Clin. Sleep Med. 2017, 13, 479–504. [Google Scholar] [CrossRef]
- WHO. Obesity: Preventing and Managing the Global Epidemic; Report of a WHO Consultation; WHO Technical Report Series; WHO: Geneva, Switzerland, 2000; Volume 894, pp. 1–252.
- Johns, M.W. Daytime sleepiness, snoring, and obstructive sleep apnea. The Epworth Sleepiness Scale. Chest 1993, 103, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Zung, W.W.; Richards, C.B.; Short, M.J. Self-rating depression scale in an outpatient clinic. Further validation of the SDS. Arch. Gen. Psychiatry 1965, 13, 508–515. [Google Scholar] [CrossRef] [PubMed]
- Brusasco, V.; Crapo, R.; Viegi, G. Coming together: The ATS/ERS consensus on clinical pulmonary function testing. Eur. Respir. J. 2005, 26, 1–2. [Google Scholar] [CrossRef]
- Fletcher, C.M.; Elmes, P.C.; Fairbairn, A.S.; Wood, C.H. The significance of respiratory symptoms and the diagnosis of chronic bronchitis in a working population. Br. Med. J. 1959, 2, 257–266. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Cruz, I.; Marciel, K.K.; Quittner, A.L.; Schechter, M.S. Anxiety and depression in cystic fibrosis. Semin. Respir. Crit. Care Med. 2009, 30, 569–578. [Google Scholar] [CrossRef]
- Choi, H.; Han, K.; Jung, J.H.; Park, J.; Kim, B.-G.; Yang, B.; Eun, Y.; Kim, H.; Shin, D.W.; Lee, H. Impact of Rheumatoid Arthritis and Seropositivity on the Risk of Non-Cystic Fibrosis Bronchiectasis. Chest 2024, 165, 1330–1340. [Google Scholar] [CrossRef] [PubMed]
- Graziano, S.; Spanò, B.; Majo, F.; Righelli, D.; Vincenzina, L.; Quittner, A.; Tabarini, P. Rates of depression and anxiety in Italian patients with cystic fibrosis and parent caregivers: Im-plementation of the Mental Health Guidelines. Respir. Med. 2020, 172, 106147. [Google Scholar] [CrossRef]
- Hadlandsmyth, K.; Driscoll, M.A.; Johnson, N.L.; Mares, J.G.; Mengeling, M.A.; Thomas, E.B.K.; Norman, S.B.; Lund, B.C. Veterans with chronic pain: Examining gender differences in pain type, overlap, and the impact of post-traumatic stress disorder. Eur. J. Pain 2024. [Google Scholar] [CrossRef]
- Quittner, A.L.; Goldbeck, L.; Abbott, J.; Duff, A.; Lambrecht, P.; Solé, A.; Tibosch, M.M.; Brucefors, A.B.; Yüksel, H.; Catastini, P.; et al. Prevalence of depression and anxiety in patients with cystic fibrosis and parent caregivers: Results of The International Depression Epidemiological Study across nine countries. Thorax 2014, 69, 1090–1097. [Google Scholar] [CrossRef]
- Martinez-Garcia, M.A.; Athanazio, R.A.; Girón, R.; Máiz-Carro, L.; de la Rosa, D.; Olveira, C.; de Gracia, J.; Vendrell, M.; Prados-Sánchez, C.; Gramblicka, G.; et al. Predicting high risk of exacerbations in bronchiectasis: The E-FACED score. Int. J. Chronic Obstruct. Pulmon. Dis. 2017, 12, 275–284. [Google Scholar] [CrossRef] [PubMed]
- McDonnell, M.J.; Aliberti, S.; Goeminne, P.C.; Dimakou, K.; Zucchetti, S.C.; Davidson, J.; Ward, C.; Laffey, J.G.; Finch, S.; Pesci, A.; et al. Multidimensional severity assessment in bronchiectasis: An analysis of seven European cohorts. Thorax 2016, 71, 1110–1118. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Zhou, R.; Peng, X.; Zhu, T.; Wei, W.; Hao, X. Relationship between depressive symptoms and anemia among the middle-aged and elderly: A cohort study over 4-year period. BMC Psychiatry 2023, 23, 572. [Google Scholar] [CrossRef] [PubMed]
- Nam, H.K.; Park, J.; Cho, S.I. Association between depression, anemia and physical activity using isotemporal substitution analysis. BMC Public Health 2023, 23, 2236. [Google Scholar] [CrossRef] [PubMed]
- Yohannes, A.M.; Ershler, W.B. Anemia in COPD: A systematic review of the prevalence, quality of life, and mortality. Respir. Care 2011, 56, 644–652. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.L.; Gozal, D.; Hunter, S.J.; Philby, M.F.; Kaylegian, J.; Kheirandish-Gozal, L. Impact of sleep disordered breathing on behaviour among elementary school-aged children: A cross-sectional analysis of a large community-based sample. Eur. Respir. J. 2016, 48, 1631–1639. [Google Scholar] [CrossRef] [PubMed]
- Faria Júnior, N.S.; Urbano, J.J.; Santos, I.R.; Silva, A.S.; Perez, E.A.; Souza, Â.H.; Nascimento, O.A.; Jardim, J.R.; Insalaco, G.; Franco Oliveira, L.V.; et al. Evaluation of obstructive sleep apnea in non-cystic fibrosis bronchiectasis: A cross-sectional study. PLoS ONE 2017, 12, e0185413. [Google Scholar] [CrossRef] [PubMed]
- Goldbeck, L.; Besier, T.; Hinz, A.; Singer, S.; Quittner, A.L.; TIDES Group. Prevalence of symptoms of anxiety and depression in German patients with cystic fibrosis. Chest 2010, 138, 929–936. [Google Scholar] [CrossRef]
- Snell, C.; Fernandes, S.; Bujoreanu, I.S.; Garcia, G. Depression, illness severity, and healthcare utilization in cystic fibrosis. Pediatr. Pulmonol. 2014, 49, 1177–1181. [Google Scholar] [CrossRef]

{kind=link}
| Depressive (n = 20) | Non-Depressive (n = 50) | p Value | |
|---|---|---|---|
| Age, years | 29.65 ± 11.50 | 29.82 ± 11.94 | 0.957 |
| BMI | 22.77 ± 5.24 | 22.36 ± 3.78 | 0.750 |
| Female sex, % | 41.0 | 59.0 | 0.010 |
| Smoker, % | 15.0 | 12.0 | 0.735 |
| Disease duration, years | 16.50 ± 8.58 | 18.28 ± 8.30 | 0.434 |
| Exacerbation count per year | 1.80 ± 1.44 | 1.58 ± 1.33 | 0.542 |
| Hospitalization count per year | 0.85 ± 0.30 | 0.60 ± 0.15 | 0.411 |
| mMRC score | 1.60 ± 0.50 | 1.20 ± 0.45 | 0.004 |
| Charlson score | 0.35 ± 0.18 | 0.36 ± 0.09 | 0.459 |
| Anemia, % | 40.0 | 18.0 | 0.052 |
| Diabetes mellitus, % | 10.0 | 16.0 | 0.517 |
| Pancreatic disease, % | 40.0 | 40.0 | 1.000 |
| Cardiac disease, % | 5.0 | 2.0 | 0.496 |
| Osteoporosis, % | 0.0 | 6.0 | 0.263 |
| O2 support, % | 5.0 | 4.0 | 0.852 |
| ESS | 5.75 ± 3.65 | 3.72 ± 3.38 | 0.030 |
| Sleepy, % | 10.0 | 6.0 | 0.557 |
| OSA, % | 55.0 | 52.0 | 0.820 |
| Nutrition support, % | 40.0 | 22.7 | 0.126 |
| FEV1, L | 1.81 ± 0.88 | 2.15 ± 0.84 | 0.151 |
| FEV1, % | 59.15 ± 23.95 | 60.59 ± 22.47 | 0.817 |
| FVC, L | 2.40 ± 1.08 | 3.02 ± 0.94 | 0.022 |
| FVC, % | 66.67 ± 20.95 | 72.78 ± 20.26 | 0.137 |
| FEV1/FVC | 74.70 ± 12.90 | 70.90 ± 14.00 | 0.310 |
| TST, min | 351.37 ± 86.07 | 360.80 ± 61.37 | 0.659 |
| Sleep efficiency, % | 79.22 ± 13.32 | 80.30 ± 12.77 | 0.753 |
| Sleep latency | 31.33 ± 5.58 | 34.04 ± 5.94 | 0.789 |
| WASO | 57.72 ± 9.31 | 54.50 ± 5.81 | 0.769 |
| REM latency | 149.33 ± 74.07 | 139.84 ± 73.42 | 0.627 |
| AHI | 6.94 ± 5.75 | 6.83 ± 6.39 | 0.948 |
| ODI | 5.80 ± 5.36 | 5.74 ± 4.42 | 0.977 |
| N1, min | 19.90 ± 8.83 | 18.27 ± 12.01 | 0.586 |
| N1, perc | 6.03 ± 3.06 | 5.18 ± 3.19 | 0.317 |
| N2, min | 168.35 ± 57.90 | 173.90 ± 62.68 | 0.733 |
| N2, perc | 48.11 ± 11.61 | 49.66 ± 17.49 | 0.716 |
| N3, min | 104.06 ± 40.18 | 102.19 ± 43.29 | 0.868 |
| N3, perc | 29.80 ± 9.14 | 31.28 ± 14.34 | 0.670 |
| REM, min | 59.09 ± 35.42 | 57.45 ± 29.99 | 0.844 |
| REM, perc | 16.04 ± 8.40 | 15.62 ± 7.57 | 0.843 |
| Depressive (n = 10) | Non-Depressive (n = 25) | p Value | |
|---|---|---|---|
| Age, years | 25.90 ± 4.41 | 27.04 ± 5.01 | 0.276 |
| BMI | 20.54 ± 3.32 | 21.75 ± 2.79 | 0.139 |
| Female sex, % | 40.0 | 60.0 | 0.084 |
| Smoker, % | 4.0 | 10.0 | 0.490 |
| Disease duration, years | 22.12 ± 5.43 | 17.90 ± 8.53 | 0.044 |
| Exacerbation count per year | 2.40 ± 1.17 | 1.84 ± 1.14 | 0.049 |
| Hospitalization count per year | 1.10 ± 0.44 | 0.92 ± 0.24 | 0.280 |
| mMRC score | 1.40 ± 0.52 | 1.20 ± 0.50 | 0.149 |
| Charlson score | 0.00 | 0.32 ± 0.09 | 0.001 |
| Anemia, % | 60.0 | 16.0 | 0.009 |
| Diabetes mellitus, % | 32.0 | 0.0 | 0.042 |
| Pancreatic disease, % | 80.0 | 80.0 | 1.000 |
| Osteoporosis, % | 0.0 | 12.0 | 0.252 |
| O2 support, % | 10.0 | 4.0 | 0.490 |
| ESS | 6.00 ± 3.62 | 3.76 ± 2.85 | 0.051 |
| Sleepy, % | 10.0 | 8.0 | 0.849 |
| OSA, % | 70.0 | 48.0 | 0.283 |
| Nutrition support, % | 60.0 | 40.0 | 0.283 |
| FEV1, L | 1.59 ± 0.80 | 1.95 ± 0.87 | 0.142 |
| FEV1, % | 46.44 ± 16.59 | 54.47 ± 23.82 | 0.180 |
| FVC, L | 2.25 ± 1.17 | 2.79 ± 1.02 | 0.097 |
| FVC, % | 56.55 ± 18.74 | 66.40 ± 22.79 | 0.225 |
| FEV1/FVC | 71.29 ± 9.27 | 70.28 ± 13.17 | 0.417 |
| TST, min | 358.32 ± 85.33 | 355.71 ± 51.86 | 0.457 |
| Sleep efficiency, % | 80.02 ± 14.39 | 78.69 ± 12.87 | 0.396 |
| Sleep latency | 32.44 ± 7.57 | 35.01 ± 10.34 | 0.440 |
| WASO | 56.52 ± 15.25 | 62.86 ± 9.11 | 0.358 |
| REM latency | 126.02 ± 69.91 | 156.62 ± 86.80 | 0.165 |
| AHI | 7.83 ± 4.99 | 6.95 ± 4.42 | 0.376 |
| ODI | 6.97 ± 4.48 | 7.12 ± 5.59 | 0.483 |
| N1, min | 19.15 ± 8.99 | 18.04 ± 12.28 | 0.399 |
| N1, perc | 5.65 ± 3.10 | 5.28 ± 3.58 | 0.388 |
| N2, min | 151.34 ± 54.34 | 162.27 ± 59.98 | 0.310 |
| N2, perc | 42.53 ± 10.95 | 46.37 ± 16.27 | 0.499 |
| N3, min | 117.08 ± 42.21 | 104.64 ± 49.25 | 0.244 |
| N3, perc | 33.06 ± 8.75 | 32.27 ± 16.52 | 0.444 |
| REM, min | 70.09 ± 40.61 | 58.38 ± 31.51 | 0.170 |
| REM, perc | 18.73 ± 10.01 | 16.06 ± 8.06 | 0.208 |
| Average heart rate/min | 75.57 ± 8.46 | 70.11 ± 8.05 | 0.041 |
| OR | 95% CI | p Value | |
|---|---|---|---|
| Univariate | |||
| Age | 0.99 | 0.99–1.04 | 0.956 |
| Female sex | 4.69 | 1.37–16.04 | 0.014 |
| BMI | 1.02 | 0.91–1.16 | 0.708 |
| Smoking | 1.29 | 0.29–5.77 | 0.735 |
| Disease duration | 0.97 | 0.91–1.04 | 0.420 |
| mMRC | 5.28 | 1.75–15.95 | 0.003 |
| Exacerbation count | 1.13 | 0.77–1.65 | 0.537 |
| Hospitalization | 1.20 | 0.78–1.86 | 0.408 |
| Nutrition support | 2.36 | 0.77–7.22 | 0.131 |
| Anemia | 3.04 | 0.96–9.86 | 0.048 |
| Diabetes | 0.58 | 0.11–3.02 | 0.521 |
| Cardiac disease | 2.57 | 0.15–43.35 | 0.511 |
| Charlson score | 0.98 | 0.47–2.10 | 0.958 |
| Oxygen support | 1.26 | 0.11–14.76 | 0.852 |
| Sleepy | 1.74 | 0.27–11.29 | 0.561 |
| ESS | 1.16 | 1.01–1.36 | 0.038 |
| FEV1/L | 0.61 | 0.31–1.20 | 0.153 |
| FEV1% | 0.99 | 0.97–1.02 | 0.813 |
| FVC/L | 0.49 | 0.27–0.93 | 0.028 |
| FVC% | 0.99 | 0.96–1.01 | 0.272 |
| FEV1/FVC | 1.02 | 0.98–1.07 | 0.307 |
| Mmf% | 1.00 | 0.98–1.02 | 0.835 |
| TST | 0.99 | 0.99–1.01 | 0.604 |
| Sleep efficiency | 0.99 | 0.95–1.03 | 0.749 |
| Sleep latency | 0.98 | 0.98–1.01 | 0.786 |
| WASO | 1.01 | 0.98–1.02 | 0.765 |
| REM latency | 1.00 | 0.99–1.01 | 0.622 |
| AHI | 1.03 | 0.92–1.09 | 0.947 |
| ODI | 1.00 | 0.94–1.07 | 0.977 |
| OSA | 1.13 | 0.39–3.19 | 0.820 |
| N1 min | 1.01 | 0.97–1.06 | 0.581 |
| N1% | 1.09 | 0.93–1.28 | 0.316 |
| N2 min | 0.99 | 0.99–1.01 | 0.728 |
| N2% | 0.99 | 0.96–1.03 | 0.712 |
| N3 min | 1.00 | 0.99–1.01 | 0.866 |
| N3% | 0.99 | 0.95–1.03 | 0.665 |
| REM min | 1.01 | 0.98–1.03 | 0.346 |
| REM% | 1.01 | 0.95–1.06 | 0.456 |
| Heart rate | 1.05 | 0.99–1.12 | 0.077 |
| Multivariate | |||
| Age | 0.96 | 0.89–1.03 | 0.957 |
| Female sex | 3.27 | 0.57–18.79 | 0.183 |
| mMRC | 12.43 | 1.92–80.18 | 0.008 |
| Anemia | 3.26 | 0.65–16.26 | 0.151 |
| ESS | 1.09 | 0.91–1.30 | 0.333 |
| FVC/L | 1.05 | 0.44–2.50 | 0.910 |
| OR | 95% CI | p Value | |
|---|---|---|---|
| Univariate | |||
| Age | 0.95 | 0.81–1.11 | 0.523 |
| Female sex | 4.28 | 1.27–12.04 | 0.018 |
| BMI | 0.86 | 0.66–1.12 | 0.272 |
| Smoking | 2.66 | 0.15–47.03 | 0.504 |
| Disease duration | 0.90 | 0.80–1.02 | 0.100 |
| mMRC | 2.27 | 0.51–9.77 | 0.289 |
| Exacerbation count | 1.51 | 0.79–2.87 | 0.206 |
| Hospitalization | 1.19 | 0.67–2.09 | 0.550 |
| Nutrition support | 2.25 | 0.50–10.03 | 0.288 |
| Anemia | 7.87 | 1.50–41.27 | 0.015 |
| Cardiac disease | 2.66 | 0.15–47.03 | 0.504 |
| Charlson score | 1.01 | 0.98–1.02 | 0.512 |
| Oxygen support | 2.67 | 0.16–41.03 | 0.504 |
| Sleepy | 1.28 | 0.10–15.90 | 0.849 |
| ESS | 1.16 | 0.96–1.41 | 0.031 |
| FEV1/L | 056 | 0.19–1.60 | 0.280 |
| FEV1% | 0.98 | 0.95–1.02 | 0.352 |
| FVC/L | 0.58 | 0.25–1.33 | 0.195 |
| FVC% | 0.98 | 0.94–1.02 | 0.251 |
| FEV1/FVC | 0.98 | 0.93–1.03 | 0.513 |
| Mmf% | 0.98 | 0.94–1.02 | 0.353 |
| TST | 1.00 | 0.99–1.01 | 0.910 |
| Sleep efficiency | 1.01 | 0.95–1.07 | 0.785 |
| Sleep latency | 0.99 | 0.98–1.02 | 0.876 |
| WASO | 0.98 | 0.98–1.01 | 0.707 |
| REM latency | 0.99 | 0.98–1.01 | 0.321 |
| AHI | 1.02 | 0.92–1.13 | 0.726 |
| ODI | 0.99 | 0.92–1.08 | 0.965 |
| OSA | 2.53 | 0.53–12.07 | 0.245 |
| N1 min | 1.01 | 0.95–1.08 | 0.791 |
| N1% | 1.03 | 0.83–1.28 | 0.769 |
| N2 min | 0.99 | 0.98–1.01 | 0.610 |
| N2% | 0.98 | 0.93–1.03 | 0.488 |
| N3 min | 1.01 | 0.96–1.05 | 0.902 |
| N3% | 1.00 | 0.96–1.06 | 0.884 |
| REM min | 1.01 | 0.98–1.04 | 0.331 |
| REM% | 1.01 | 0.95–1.08 | 0.691 |
| Heart rate | 1.07 | 0.99–1.19 | 0.072 |
| Multivariate | |||
| Age | 0.98 | 0.92–1.04 | 0.476 |
| Female sex | 4.12 | 1.37–45.68 | 0.026 |
| Anemia | 0.22 | 0.02–2.07 | 0.184 |
| ESS | 1.29 | 0.99–1.69 | 0.045 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balcan, B.; Vezir, D.; Olgun Yildizeli, S.; Kocakaya, D.; Ceyhan, B. The Association of Depression with Obstructive Sleep Apnea in Patients with Cystic and Non-Cystic Fibrosis Bronchiectasis. Life 2024, 14, 1026. https://doi.org/10.3390/life14081026
Balcan B, Vezir D, Olgun Yildizeli S, Kocakaya D, Ceyhan B. The Association of Depression with Obstructive Sleep Apnea in Patients with Cystic and Non-Cystic Fibrosis Bronchiectasis. Life. 2024; 14(8):1026. https://doi.org/10.3390/life14081026
Chicago/Turabian StyleBalcan, Baran, Duygu Vezir, Sehnaz Olgun Yildizeli, Derya Kocakaya, and Berrin Ceyhan. 2024. "The Association of Depression with Obstructive Sleep Apnea in Patients with Cystic and Non-Cystic Fibrosis Bronchiectasis" Life 14, no. 8: 1026. https://doi.org/10.3390/life14081026
APA StyleBalcan, B., Vezir, D., Olgun Yildizeli, S., Kocakaya, D., & Ceyhan, B. (2024). The Association of Depression with Obstructive Sleep Apnea in Patients with Cystic and Non-Cystic Fibrosis Bronchiectasis. Life, 14(8), 1026. https://doi.org/10.3390/life14081026