Diagnostic Value of Plasma Annexin A2 in Early-Stage High-Grade Serous Ovarian Cancer

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Samples
2.2. Annexin A2 Measurements
2.3. CA125 Measurements
2.4. Statistical Analysis
3. Results
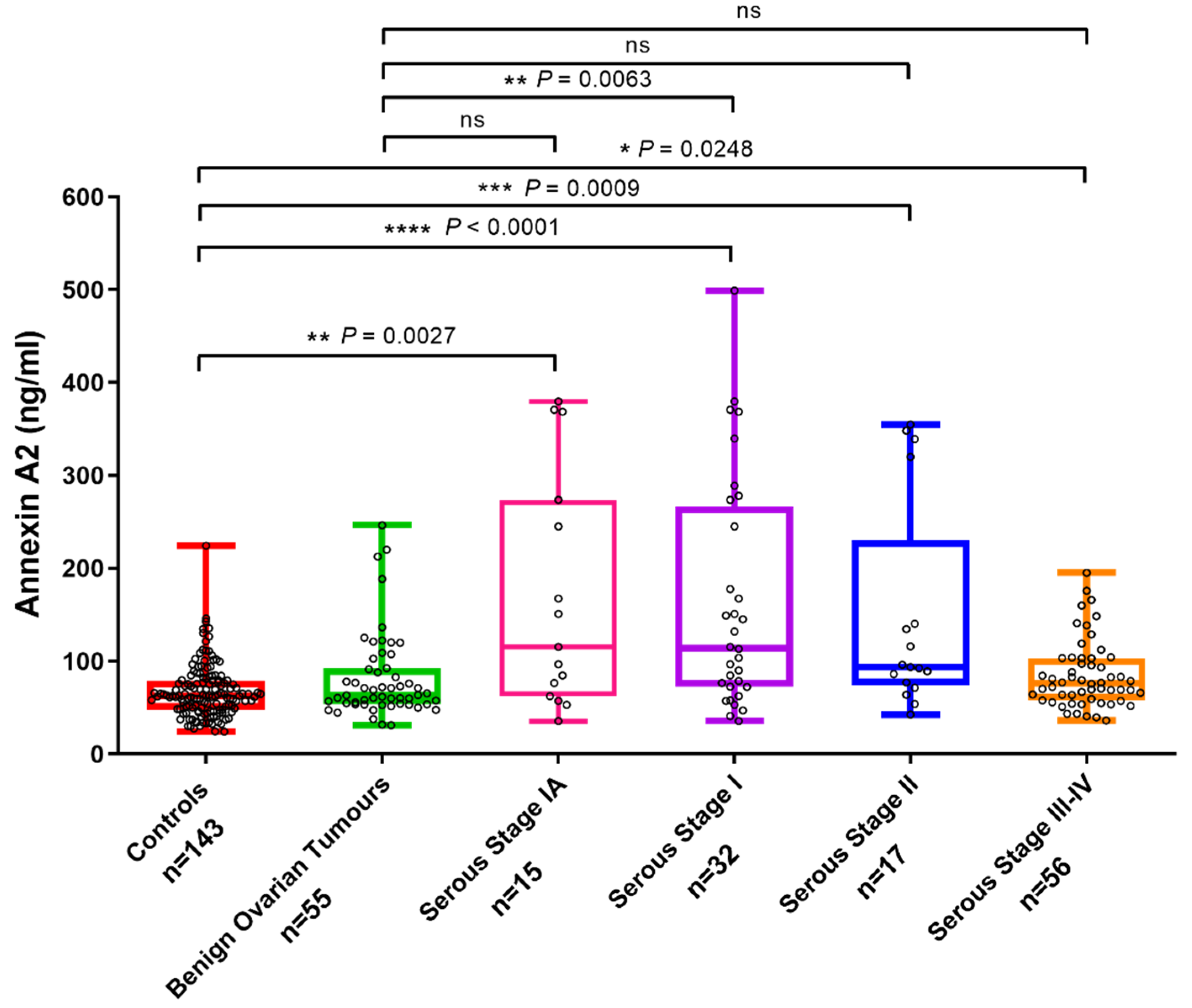
3.1. Plasma Annexin A2 Levels Are Elevated in Stage I Ovarian Cancer
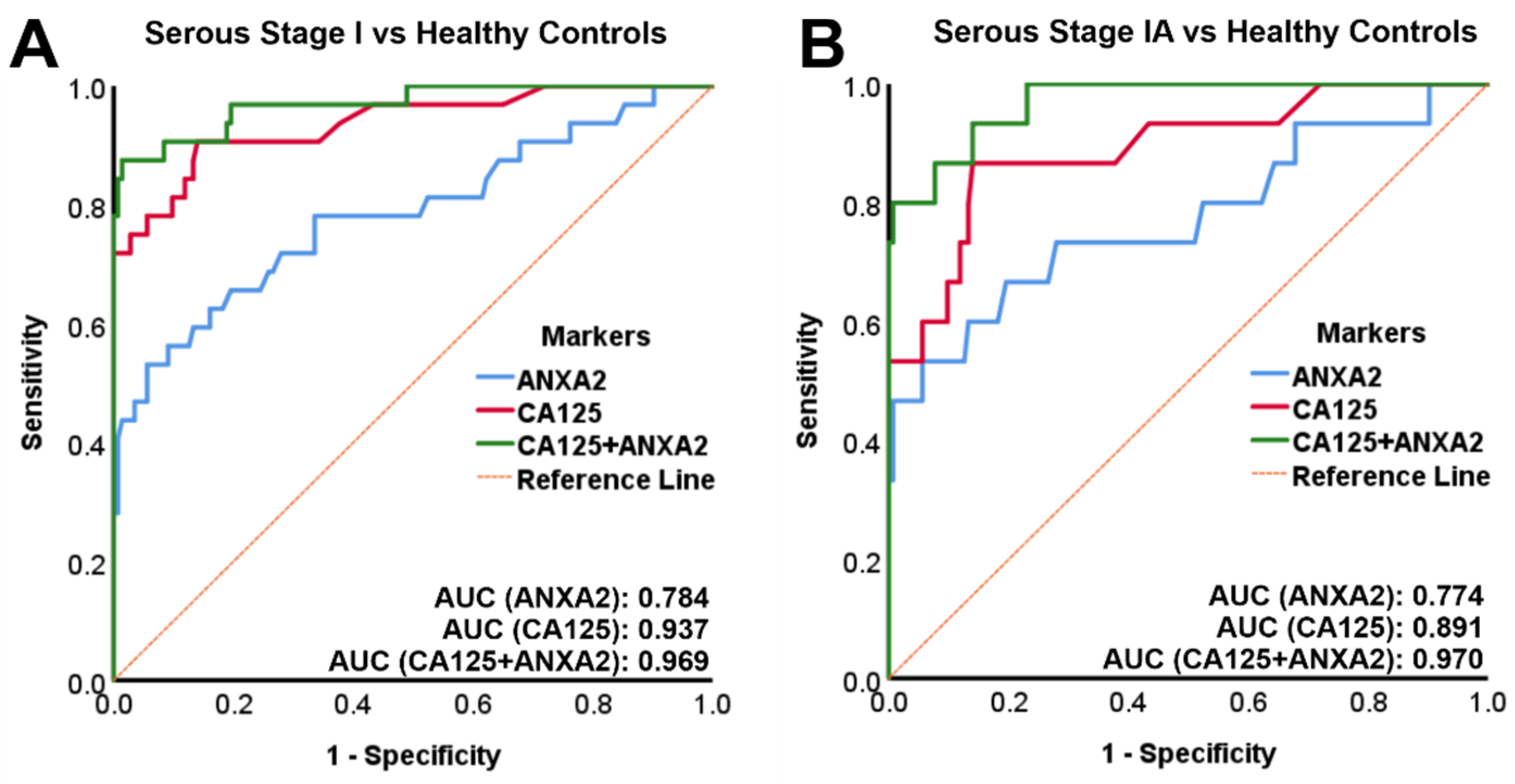
3.2. Combined Annexin A2 and CA125 Has a High Sensitivity and Specificity in Diagnosing Stage I and Stage IA OC versus Healthy Controls
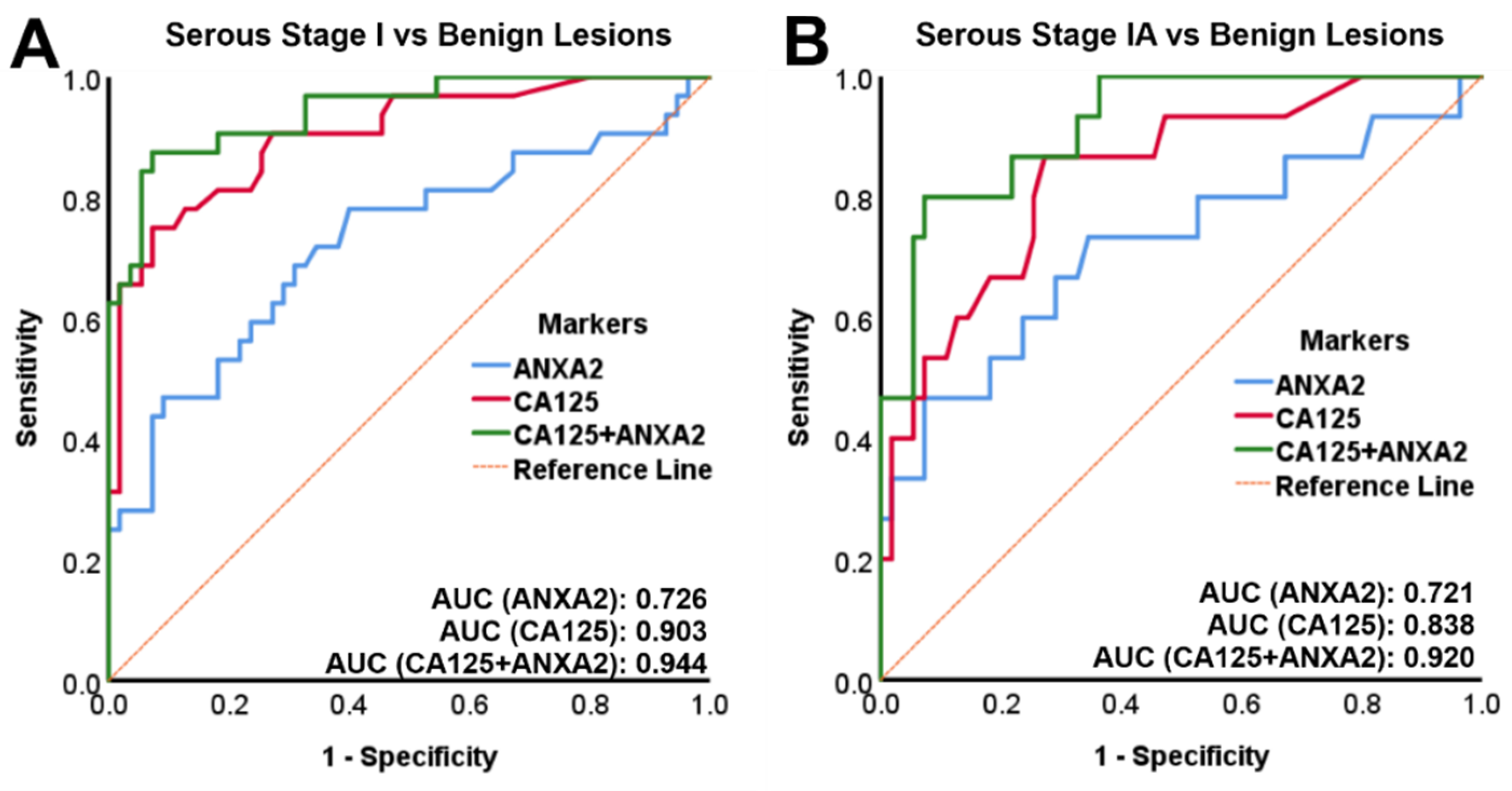
3.3. Combined Annexin A2 and CA125 Has a High Accuracy in Diagnosing Stage IA OC versus Benign Ovarian Tumors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ANXA2 | Annexin A2 |
| AUC | Area under the curve |
| CA125 | Cancer antigen 125 |
| FIGO | International Federation of Gynecology and Obstetrics |
| HE4 | Human epididymis protein 4 |
| HGSOC | High grade serous ovarian cancer |
| OC | Ovarian cancer |
| PPV | Positive predictive value |
| ROC | Receiver operating characteristics |
| ROMA | Risk of ovarian malignancy algorithm |
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Maringe, C.; Walters, S.; Butler, J.; Coleman, M.P.; Hacker, N.; Hanna, L.; Mosgaard, B.J.; Nordin, A.; Rosen, B.; Engholm, G.; et al. Stage at diagnosis and ovarian cancer survival: Evidence from the International Cancer Benchmarking Partnership. Gynecol. Oncol. 2012, 127, 75–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howlader, N.; Krapcho, M.; Miller, D.; Bishop, K.; Kosary, C.L.; Yu, M.; Ruhl, J.; Tatalovich, Z.; Mariotto, A.; Lewis, D.R.; et al. (Eds.) SEER Cancer Statistics Review, 1975–2014; National Cancer Institute: Bethesda, MD, USA, 2018. Available online: https://seer.cancer.gov/csr/1975_2014/ (accessed on 24 December 2020).
- Clarke-Pearson, D.L. Clinical practice. Screening for ovarian cancer. N. Engl. J. Med. 2009, 361, 170–177. [Google Scholar] [CrossRef] [PubMed]
- Shiau, C.-S.; Chang, M.-Y.; Chiang, C.-H.; Hsieh, C.-C.; Hsieh, T. Ovarian endometrioma associated with very high serum CA-125 levels. Chang. Gung Med. J. 2003, 26, 695–699. [Google Scholar] [PubMed]
- Buamah, P. Benign conditions associated with raised serum CA-125 concentration. J. Surg. Oncol. 2000, 75, 264–265. [Google Scholar] [CrossRef]
- Muinao, T.; Boruah, H.P.D.; Pal, M. Multi-biomarker panel signature as the key to diagnosis of ovarian cancer. Heliyon 2019, 5, e02826. [Google Scholar] [CrossRef] [Green Version]
- Coticchia, C.M.; Yang, J.; Moses, M.A. Ovarian cancer biomarkers: Current options and future promise. J. Natl. Compr. Cancer Netw. 2008, 6, 795–802. [Google Scholar] [CrossRef]
- Rastogi, M.; Gupta, S.; Sachan, M. Biomarkers towards Ovarian Cancer Diagnostics: Present and Future Prospects. Braz. Arch. Biol. Technol. 2016, 59, 59. [Google Scholar] [CrossRef] [Green Version]
- Bonifácio, V.D.B. Ovarian cancer biomarkers: Moving forward in early detection. In Tumor Microenvironment: The Main Driver of Metabolic Adaptation; Serpa, J., Ed.; Springer International Publishing: Cham, Switzerland, 2020; pp. 355–363. [Google Scholar] [CrossRef]
- Moore, R.G.; McMeekin, D.S.; Brown, A.K.; Di Silvestro, P.; Miller, M.C.; Allard, W.J.; Gajewski, W.; Kurman, R.; Bast, R.C., Jr.; Skates, S.J. A novel multiple marker bioassay utilizing HE4 and CA125 for the prediction of ovarian cancer in patients with a pelvic mass. Gynecol. Oncol. 2009, 112, 40–46. [Google Scholar] [CrossRef] [Green Version]
- Coleman, R.L.; Herzog, T.J.; Chan, D.W.; Munroe, D.G.; Pappas, T.C.; Smith, A.; Zhang, Z.; Wolf, J. Validation of a second-generation multivariate index assay for malignancy risk of adnexal masses. Am. J. Obstet. Gynecol. 2016, 215, 82.e1–82.e11. [Google Scholar] [CrossRef] [Green Version]
- Ueland, F.R.; Desimone, C.P.; Seamon, L.G.; Miller, R.A.; Goodrich, S.; Podzielinski, I.; Sokoll, L.; Smith, A.; van Nagell, J.R., Jr.; Zhang, Z. Effectiveness of a multivariate index assay in the preoperative assessment of ovarian tumors. Obstet. Gynecol. 2011, 117, 1289–1297. [Google Scholar] [CrossRef] [PubMed]
- Mai, J.; Waisman, D.M.; Sloane, B.F. Cell surface complex of cathepsin B/annexin II tetramer in malignant progression. Biochim. Biophys. Acta 2000, 1477, 215–230. [Google Scholar] [CrossRef]
- Sharma, M.C. Annexin A2 (ANX A2): An emerging biomarker and potential therapeutic target for aggressive cancers. Int. J. Cancer 2019, 144, 2074–2081. [Google Scholar] [CrossRef]
- Lokman, N.A.; Elder, A.S.; Ween, M.P.; Pyragius, C.E.; Hoffmann, P.; Oehler, M.K.; Ricciardelli, C. Annexin A2 is regulated by ovarian cancer-peritoneal cell interactions and promotes metastasis. Oncotarget 2013, 4, 1199–1211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lokman, N.A.; Pyragius, C.E.; Ruszkiewicz, A.; Oehler, M.K.; Ricciardelli, C. Annexin A2 and S100A10 are independent predictors of serous ovarian cancer outcome. Transl. Res. 2016, 171, 83–95.e2. [Google Scholar] [CrossRef]
- Woolas, R.P.; Xu, F.J.; Jacobs, I.J.; Yu, Y.H.; Daly, L.; Berchuck, A.; Soper, J.T.; Clarke-Pearson, D.L.; Oram, D.H.; Bast, R.C., Jr. Elevation of multiple serum markers in patients with stage I ovarian cancer. J. Natl. Cancer Inst. 1993, 85, 1748–1751. [Google Scholar] [CrossRef]
- Jacobs, I.; Bast, R.C., Jr. The CA 125 tumour-associated antigen: A review of the literature. Hum. Reprod. 1989, 4, 1–12. [Google Scholar] [CrossRef]
- Ween, M.P.; Lokman, N.A.; Hoffmann, P.; Rodgers, R.J.; Ricciardelli, C.; Oehler, M.K. Transforming growth factor-beta-induced protein secreted by peritoneal cells increases the metastatic potential of ovarian cancer cells. Int. J. Cancer 2011, 128, 1570–1584. [Google Scholar] [CrossRef] [Green Version]
- Lokman, N.A.; Ween, M.P.; Oehler, M.K.; Ricciardelli, C. The role of annexin A2 in tumorigenesis and cancer progression. Cancer Microenviron. 2011, 4, 199–208. [Google Scholar] [CrossRef] [Green Version]
- RCOG. Management of suspected ovarian masses in premenopausal women. In Green-Top Guideline No. 62; RCOG: London, UK, 2011. [Google Scholar]
- Sun, Y.; Gao, G.; Cai, J.; Wang, Y.; Qu, X.; He, L.; Liu, F.; Zhang, Y.; Lin, K.; Ma, S.; et al. Annexin A2 is a discriminative serological candidate in early hepatocellular carcinoma. Carcinogenesis 2013, 34, 595–604. [Google Scholar] [CrossRef] [Green Version]
- Ji, N.Y.; Park, M.Y.; Kang, Y.H.; Lee, C.I.; Kim, D.G.; Yeom, Y.I.; Jang, Y.J.; Myung, P.K.; Kim, J.W.; Lee, H.G.; et al. Evaluation of annexin II as a potential serum marker for hepatocellular carcinoma using a developed sandwich ELISA method. Int. J. Mol. Med. 2009, 24, 765–771. [Google Scholar] [PubMed] [Green Version]
- El-Abd, N.; Fawzy, A.; Elbaz, T.; Hamdy, S. Evaluation of annexin A2 and as potential biomarkers for hepatocellular carcinoma. Tumour Biol. 2016, 37, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Shetty, P.; Patil, V.S.; Mohan, R.; D’Souza, L.C.; Bargale, A.; Patil, B.R.; Dinesh, U.S.; Haridas, V.; Kulkarni, S.P. Annexin A2 and its downstream IL-6 and HB-EGF as secretory biomarkers in the differential diagnosis of Her-2 negative breast cancer. Ann. Clin. Biochem. Int. J. Lab. Med. 2017, 54, 463–471. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Yang, F.; Nie, J.; Zou, X.; Tian, H.; Qin, Y.; Liu, C. Evaluation of annexin A2 as a novel diagnostic serum biomarker for lung cancer. Cancer Biomark. 2015, 15, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Tas, F.; Tilgen Yasasever, C.; Karabulut, S.; Tastekin, D.; Duranyildiz, D. Circulating annexin A2 as a biomarker in gastric cancer patients: Correlation with clinical variables. Biomed. Pharmacother. 2015, 69, 237–241. [Google Scholar] [CrossRef] [PubMed]
- Gurluler, E.; Guner, O.S.; Tumay, L.V.; Turkel Kucukmetin, N.; Hizli, B.; Zorluoglu, A. Serum annexin A2 levels in patients with colon cancer in comparison to healthy controls and in relation to tumor pathology. Med. Sci. Monit. 2014, 20, 1801–1807. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeon, Y.R.; Kim, S.Y.; Lee, E.J.; Kim, Y.N.; Noh, D.-Y.; Park, S.Y.; Moon, A. Identification of annexin II as a novel secretory biomarker for breast cancer. Proteomics 2013, 13, 3145–3156. [Google Scholar] [CrossRef]
- Ulvestad, E.; Kristoffersen, E.K.; Jensen, T.S.; Matre, R. Identification of a soluble Fc gamma-binding molecule (annexin II) in human serum using a competitive ELISA. Apmis 1994, 102, 667–673. [Google Scholar] [CrossRef]
- Bystricky, B.; Cierna, Z.; Sieberova, G.; Janega, P.; Karaba, M.; Minarik, G.; Benca, J.; Sedlackova, T.; Jurisova, S.; Gronesova, P.; et al. Relationship between circulating tumor cells and annexin A2 in early breast cancer patients. Anticancer Res. 2017, 37, 2727–2734. [Google Scholar] [CrossRef] [Green Version]
- Herrero, C.; de la Fuente, A.; Casas-Arozamena, C.; Sebastian, V.; Prieto, M.; Arruebo, M.; Abalo, A.; Colas, E.; Moreno-Bueno, G.; Gil-Moreno, A.; et al. Extracellular vesicles-based biomarkers represent a promising liquid biopsy in endometrial cancer. Cancers 2019, 11, 2000. [Google Scholar] [CrossRef] [Green Version]
- Flood, E.C.; Hajjar, K.A. The annexin A2 system and vascular homeostasis. Vasc. Pharmacol. 2011, 54, 59–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laumonnier, Y.; Syrovets, T.; Burysek, L.; Simmet, T. Identification of the annexin A2 heterotetramer as a receptor for the plasmin-induced signaling in human peripheral monocytes. Blood 2006, 107, 3342–3349. [Google Scholar] [CrossRef] [PubMed]
- Tsunezumi, J.; Yamamoto, K.; Higashi, S.; Miyazaki, K. Matrilysin (matrix metalloprotease-7) cleaves membrane-bound annexin II and enhances binding of tissue-type plasminogen activator to cancer cell surfaces. FEBS J. 2008, 275, 4810–4823. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Marker | FIGO Stage | Sensitivity (100% Specificity) | Sensitivity (99.6% Specificity) | Sensitivity (98% Specificity) | Specificity (75% Sensitivity) | AUC |
|---|---|---|---|---|---|---|
| ANXA2 | IA | 33.3 | 46.7 | 46.7 | 72.0 | 0.774 |
| IA + IB | 35.3 | 47.1 | 47.1 | 72.0 | 0.786 | |
| IC | 20.0 | 33.3 | 40.0 | 64.3 | 0.782 | |
| I | 28.1 | 40.6 | 43.8 | 66.4 | 0.784 | |
| II | 23.5 | 23.5 | 29.4 | 73.4 | 0.796 | |
| III-IV | 0 | 8.9 | 12.5 | 39.9 | 0.656 | |
| I-IV | 12.4 | 21.0 | 24.8 | 53.1 | 0.718 | |
| CA125 | IA | 53.3 | 53.3 | 53.3 | 88.1 | 0.891 |
| IA + IB | 58.8 | 58.8 | 58.8 | 88.1 | 0.904 | |
| IC | 86.7 | 86.7 | 86.7 | 100 | 0.974 | |
| I | 71.9 | 71.9 | 71.9 | 97.2 | 0.937 | |
| II | 82.4 | 82.4 | 82.4 | 100 | 0.978 | |
| III-IV | 98.2 | 98.2 | 98.2 | 100 | 1.000 | |
| I-IV | 87.6 | 87.6 | 87.6 | 100 | 0.977 | |
| ANXA2+ CA125 | IA | 73.3 | 80.0 | 80.0 | 100 | 0.970 |
| IA + IB | 70.6 | 82.4 | 82.4 | 99.3 | 0.973 | |
| IC | 86.7 | 93.3 | 93.3 | 100 | 0.975 | |
| I | 78.1 | 84.4 | 87.5 | 100 | 0.969 | |
| II | 82.4 | 82.4 | 82.4 | 100 | 0.975 | |
| III-IV | 98.2 | 98.2 | 100 | 100 | 1.000 | |
| I-IV | 87.6 | 89.5 | 92.4 | 100 | 0.986 |
| Marker | True Positive (TP) | True Negative (TN) | False Positive (FP) | False Negative (FN) | Accuracy (%) |
|---|---|---|---|---|---|
| ANXA2 | 5 | 143 | 0 | 10 | 93.7 |
| CA125 | 8 | 143 | 0 | 7 | 95.6 |
| ANXA2 + CA125 | 11 | 143 | 0 | 4 | 97.5 |
| Marker | FIGO Stage | Specificity (100% Sensitivity) | Specificity (94% Sensitivity) | Specificity (75% Sensitivity) | AUC |
|---|---|---|---|---|---|
| ANXA2 | IA | 3.6 | 18.2 | 65.5 | 0.721 |
| IA + IB | 3.6 | 18.2 | 65.5 | 0.736 | |
| IC | 5.5 | 7.3 | 60.0 | 0.714 | |
| I | 3.6 | 7.3 | 60.0 | 0.726 | |
| II | 5.5 | 25.5 | 67.3 | 0.733 | |
| III-IV | 3.6 | 5.5 | 36.4 | 0.573 | |
| I-IV | 3.6 | 5.5 | 50.9 | 0.646 | |
| CA125 | IA | 20.0 | 52.7 | 74.5 | 0.838 |
| IA + IB | 20.0 | 52.7 | 74.5 | 0.856 | |
| IC | 54.5 | 92.7 | 98.2 | 0.956 | |
| I | 20.0 | 54.5 | 92.7 | 0.903 | |
| II | 72.7 | 74.5 | 98.2 | 0.951 | |
| III-IV | 92.7 | 94.5 | 98.2 | 0.991 | |
| I-IV | 20.0 | 74.5 | 98.2 | 0.958 | |
| ANXA2 + CA125 | IA | 63.6 | 67.3 | 94.5 | 0.920 |
| IA + IB | 63.6 | 67.3 | 94.5 | 0.928 | |
| IC | 49.1 | 92.7 | 98.2 | 0.958 | |
| I | 45.5 | 67.3 | 94.5 | 0.944 | |
| II | 58.2 | 78.2 | 98.2 | 0.949 | |
| III-IV | 92.7 | 94.5 | 98.2 | 0.990 | |
| I-IV | 47.3 | 81.8 | 98.2 | 0.967 |
| Marker | True Positive (TP) | True Negative (TN) | False Positive (FP) | False Negative (FN) | Accuracy (%) |
|---|---|---|---|---|---|
| ANXA2 | 15 | 2 | 53 | 0 | 24.3 |
| CA125 | 15 | 11 | 44 | 0 | 37.1 |
| ANXA2 + CA125 | 15 | 35 | 20 | 0 | 71.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lokman, N.A.; Ricciardelli, C.; Stephens, A.N.; Jobling, T.W.; Hoffmann, P.; Oehler, M.K. Diagnostic Value of Plasma Annexin A2 in Early-Stage High-Grade Serous Ovarian Cancer. Diagnostics 2021, 11, 69. https://doi.org/10.3390/diagnostics11010069
Lokman NA, Ricciardelli C, Stephens AN, Jobling TW, Hoffmann P, Oehler MK. Diagnostic Value of Plasma Annexin A2 in Early-Stage High-Grade Serous Ovarian Cancer. Diagnostics. 2021; 11(1):69. https://doi.org/10.3390/diagnostics11010069
Chicago/Turabian StyleLokman, Noor A., Carmela Ricciardelli, Andrew N. Stephens, Thomas W. Jobling, Peter Hoffmann, and Martin K. Oehler. 2021. "Diagnostic Value of Plasma Annexin A2 in Early-Stage High-Grade Serous Ovarian Cancer" Diagnostics 11, no. 1: 69. https://doi.org/10.3390/diagnostics11010069