
The Contributory Role of Cell Blocks in Salivary Gland Neoplasms Fine Needle Aspirations Classified by the Milan System for Reporting Salivary Gland Cytology



Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Faquin, W.C.; Rossi, E.D.; Baloch, Z.; Barkan, G.A.; Foschini, M.P.; Kurtycz, D.F.; Pusztaszeri, M.; Vielh, P. The Milan System for Reporting Salivary Gland Cytopathology; Springer: Basel, Switzerland, 2018; Volume 1. [Google Scholar]
- Rossi, E.D.; Faquin, W.C. The Milan System for Reporting Salivary Gland Cytopathology (MSRSGC): An international effort toward improved patient care-when the roots might be inspired by Leonardo da Vinci. Cancer Cytopathol. 2018, 126, 756–766. [Google Scholar] [CrossRef] [Green Version]
- Barbarite, E.; Puram, S.V.; Derakhshan, A.; Rossi, E.D.; Faquin, W.C.; Varvares, M.A. A call for universal acceptance of the Milan System for Reporting Salivary Gland Cytopathology. Laryngoscope 2020, 130, 80–85. [Google Scholar] [CrossRef]
- Hirata, Y.; Higuchi, K.; Tamashiro, K.; Koja, K.; Yasutomi, Y.; Matsuzaki, A.; Yoshimi, N. Application of the Milan System for Reporting Salivary Gland Cytopathology: A 10-year experience in a single Japanese institution. Acta Cytol. 2020, 28, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Jalaly, J.B.; Farahani, S.J.; Baloch, Z.W. The Milan System for Reporting Salivary Gland Cytopathology: A comprehensive review of the literature. Diagn. Cytopathol. 2020, 48, 880–889. [Google Scholar] [CrossRef] [PubMed]
- Jha, S.; Mitra, S.; Purkait, S.; Adhya, A.K. The Milan System for Reporting Salivary Gland Cytopathology: Assessment of cytohistological concordance and risk of malignancy. Acta Cytol. 2021, 65, 27–39. [Google Scholar] [CrossRef] [PubMed]
- Tommola, E.; Tommola, S.; Porre, S.; Kholová, I. Salivary gland FNA diagnostics in a real-life setting: One-year-experiences of the implementation of the Milan system in a tertiary care center. Cancers 2019, 11, 1589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krogerus, L.; Kholová, I. Cell block in cytological diagnostics: Review of preparatory techniques. Acta Cytol. 2018, 62, 237–243. [Google Scholar] [CrossRef]
- Nambirajan, A.; Jain, D. Cell blocks in cytopathology: An update. Cytopathology 2018, 29, 505–524. [Google Scholar] [CrossRef]
- Shidham, V.B. CellBlockistry: Chemistry and art of cell-block making—A detailed review of various historical options with recent advances. CytoJournal 2019, 16, 12. [Google Scholar] [CrossRef]
- Hakso-Mäkinen, H.; Kholová, I. New cell block method to enhance the cellular yield in mucous and/or bloody samples. Acta Cytol. 2020, 64, 265–269. [Google Scholar] [CrossRef]
- Nix, J.S.; Rooper, L.M. Navigating small biopsies of salivary gland tumors: A pattern-based approach. J. Am. Soc. Cytopathol. 2020, 9, 369–382. [Google Scholar] [CrossRef]
- Maleki, Z. The Milan System for Reporting Salivary Gland Cytopathology: A universal language to improve patient care. J. Am. Soc. Cytopathol. 2020, 9, 113–115. [Google Scholar] [CrossRef]
- Pusztaszeri, M.; Rossi, E.D.; Baloch, Z.W.; Faquin, W.C. Salivary gland fine needle aspiration and introduction of the Milan reporting system. Adv. Anat. Pathol. 2019, 26, 84–92. [Google Scholar] [CrossRef]
- Tyagi, R.; Dey, P. Diagnostic problems of salivary gland tumors. Diagn. Cytopathol. 2015, 43, 495–509. [Google Scholar] [CrossRef]
- Carter, M.D.; Moore, D.P.; MacIntosh, R.F.; Bullock, M.J. Impact of routine cell block preparation on results of head and neck fine needle aspirates. Diagn. Cytopathol. 2016, 44, 880–887. [Google Scholar] [CrossRef] [PubMed]
- Herbert, A. Cell blocks are not a substitute for cytology: Why pathologists should understand cytopathology particularly in their chosen speciality. Cytopathology 2014, 25, 351–355. [Google Scholar] [CrossRef]
- Jain, D.; Mathur, S.R.; Iyer, V.K. Cell blocks in cytopathology: A review of preparative methods, utility in diagnosis and role in ancillary studies. Cytopathology 2014, 25, 356–371. [Google Scholar] [CrossRef] [PubMed]
- Desai, K.M.; Angadi, P.V.; Kale, A.D.; Hallikerimath, S. Assessment of cell block technique in head and neck pathology diagnoses: A preliminary study. Diagn. Cytopathol. 2019, 47, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Melo, G.; Mello, F.W.; Mesquita, R.A.; Grando, L.J.; Rivero, E.R.C. Cell-block as ancillary tool for the diagnosis of cystic and cyst-like jaw lesions. Diagn. Cytopathol. 2020, 48, 717–723. [Google Scholar] [CrossRef]
- Hou, Y.; Chaudhary, S.; Shen, R.; Li, Z. Fine-needle aspiration of cervical lymph nodes yields adequate materials for accurate HPV testing in metastatic head and neck squamous cell carcinomas. Diagn. Cytopathol. 2016, 44, 792–798. [Google Scholar] [CrossRef]
- Horáková, M.; Porre, S.; Tommola, S.; Baněčková, M.; Skálová, A.; Kholová, I. FNA diagnostics of secondary malignancies in the salivary gland: Bi-institutional experience of 36 cases. Diagn. Cytopathol. 2021, 49, 241–251. [Google Scholar] [CrossRef]
- Behaeghe, M.; Poorten, V.V.; Hermans, R.; Politis, C.; Weynand, B.; Hauben, E. The Milan system for reporting salivary gland cytopathology: Single center experience with cell blocks. Diagn. Cytopathol. 2020, 48, 972–978. [Google Scholar] [CrossRef]
- Miesbauerová, M.; Tommola, S.; Šteiner, P.; Baněčková, M.; Skálová, A.; Kholová, I. Cytopathological features of secretory carcinoma of salivary glands and ancillary techniques in its diagnostics: Impact of new Milan system for reporting salivary gland cytopathology. APMIS 2019, 127, 491–502. [Google Scholar] [CrossRef] [PubMed]
- Viswanathan, K.; Sung, S.; Scognamiglio, T.; Yang, G.C.H.; Siddiqui, M.T.; Rao, R.A. The role of the Milan System for Reporting Salivary Gland Cytopathology: A 5-year institutional experience. Cancer Cytopathol. 2018, 126, 541–551. [Google Scholar] [CrossRef]
- Song, S.J.; Shafique, K.; Wong, L.Q.; LiVolsi, V.A.; Montone, K.T.; Baloch, Z. The utility of the Milan System as a risk stratification tool for salivary gland fine needle aspiration cytology specimens. Cytopathology 2019, 30, 91–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saqi, A. The state of cell blocks and ancillary testing: Past, present, and future. Arch. Pathol. Lab. Med. 2016, 140, 1318–1322. [Google Scholar] [CrossRef] [Green Version]
- Abram, M.; Huhtamella, R.; Kalfert, D.; Hakso-Mäkinen, H.; Ludvíková, M.; Kholová, I. The role of cell blocks and immunohistochemistry in thyroid atypia of undetermined significance/follicular lesion of undetermined significance Bethesda category. Acta Cytol. 2021, 65, 257–263. [Google Scholar] [CrossRef] [PubMed]
- da Cunha Santos, G.; Saieg, M.A. Preanalytic specimen triage: Smears, cell blocks, cytospin preparations, transport media, and cytobanking. Cancer Cytopathol. 2017, 125, 455–464. [Google Scholar] [CrossRef]
- Point du Jour, K.; Griffith, C.C. The role of ancillary techniques in salivary gland cytopathology specimens. Acta Cytol. 2020, 64, 92–102. [Google Scholar] [CrossRef]
- Srebotnik Kirbiš, I.; Rodrigues Roque, R.; Bongiovanni, M.; Strojan Fležar, M.; Cochand-Priollet, B. Immunocytochemistry practices in European cytopathology laboratories-Review of European Federation of Cytology Societies (EFCS) online survey results with best practice recommendations. Cancer Cytopathol. 2020, 128, 757–766. [Google Scholar] [CrossRef]
- Dubucs, C.; Basset, C.; D’Aure, D.; Courtade-Saïdi, M.; Evrard, S.M. A 4-year retrospective analysis of salivary gland cytopathology using the Milan system for reporting salivary gland cytology and ancillary studies. Cancers 2019, 11, 1912. [Google Scholar] [CrossRef] [Green Version]
- Hughes, J.H.; Volk, E.E.; Wilbur, D.C.; Cytopathology Resource Committee; College of American Pathologists. Pitfalls in salivary gland fine-needle aspiration cytology: Lessons from the College of American Pathologists Interlaboratory Comparison Program in Nongynecologic Cytology. Arch. Pathol. Lab. Med. 2005, 129, 26–31. [Google Scholar] [CrossRef]
- Sadullahoğlu, C.; Yıldırım, H.T.; Nergiz, D.; Çekiç, B.; Selçuk, Ö.T.; Osma, Ü.; Alparslan, A.Ş.; Sezer, C. The risk of malignancy according to Milan reporting system of salivary gland fine-needle aspiration with Becton Dickinson SurePath liquid-based processing. Diagn. Cytopathol. 2019, 47, 863–868. [Google Scholar] [CrossRef]
- Rohilla, M.; Singh, P.; Rajwanshi, A.; Gupta, N.; Srinivasan, R.; Dey, P.; Vashishta, R.K. Three-year cytohistological correlation of salivary gland FNA cytology at a tertiary center with the application of the Milan system for risk stratification. Cancer Cytopathol. 2017, 125, 767–775. [Google Scholar] [CrossRef] [Green Version]
- Pujani, M.; Chauhan, V.; Agarwal, C.; Raychaudhuri, S.; Singh, K. A critical appraisal of the Milan system for reporting salivary gland cytology (MSRSGC) with histological correlation over a 3-year period: Indian scenario. Diagn. Cytopathol. 2019, 47, 382–388. [Google Scholar] [CrossRef] [PubMed]
- Miller, J.A.; An, D.; Shafique, K.; Song, S.; Rao, R.A.; Viswanathan, K.; Eykman, E.; Wiles, A.; Ali, S.Z.; Field, A.; et al. Mucoepidermoid carcinoma, acinic cell carcinoma, and adenoid cystic carcinoma on fine-needle aspiration biopsy and The Milan System: An international multi-institutional study. J. Am. Soc. Cytopathol. 2019, 8, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Lubin, D.; Buonocore, D.; Wei, X.J.; Cohen, J.M.; Lin, O. The Milan System at Memorial Sloan Kettering: Utility of the categorization system for in-house salivary gland fine-needle aspiration cytology at a comprehensive cancer center. Diagn. Cytopathol. 2020, 48, 183–190. [Google Scholar] [CrossRef]
- Poller, D.N.; Schmitt, F. Should uncertainty concerning the risk of malignancy be included in diagnostic (nongynecologic) cytopathology reports? Cancer Cytopathol. 2021, 129, 16–21. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MSRSGC Category | Patient Age Mean (Range) | Lesion Size Mean (Range) | No./Total No. (%) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Cases with Follow-Up | Risk of Neoplasm | Risk of Malignancy | Overall Risk of Malignancy | |||||||
| Non-Diagnostic | 62.6 (20–95) | 2.1 (0.8–4.3) | 52/139 | (37.4) | 32/52 | (61.5) | 12/52 | (23.1) | 12/139 | (8.6) |
| Non-Neoplastic | 36.3 (29–44) | 1.9 (1.1–2.5) | 4/16 | (25.0) | 2/4 | (50.0) | 1/4 | (25.0) | 1/16 | (6.3) |
| AUS | 53.6 (25–73) | 2.5 (0.9–4.0) | 16/45 | (25.6) | 12/16 | (75.0) | 1/25 | (4.0) | 1/45 | (2.2) |
| Benign Neoplasm | 54.0 (13–85) | 2.6 (0.9–5.0) | 53/105 | (50.5) | 53/53 | (100) | 0/53 | (0.0) | 0/53 | (0.0) |
| SUMP | 63.3 (24–88) | 2.1 (1.3–5.2) | 27/37 | (73.0) | 26/27 | (96.3) | 8/27 | (29.6) | 8/37 | (21.6) |
| Suspicious for Malignancy | 62.4 (48–79) | 1.9 (1.0–3.0) | 6/10 | (60.0) | 5/6 | (83.3) | 5/6 | (83.3) | 5/10 | (50.0) |
| Malignant Neoplasm | 67.0 (59–73) | 2.1 (2.7–5.0) | 6/14 | (42.9) | 6/6 | (100) | 6/6 | (100) | 6/14 | (42.9) |
| Total | 58.3 (13–95) | 2.3 (0.8–5.0) | 164/365 | (44.9) | 136/164 | (82.9) | 36/164 | (22.0) | 36/365 | (9.9) |
| n | Accuracy | Sensitivity | Specificity | PPV | NPV | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| (%) | 95%CI (%) | (%) | 95%CI (%) | (%) | 95% CI (%) | (%) | 95%CI (%) | (%) | 95%CI (%) | ||
| All Categories | 112 | 87.5 | 79.9–93.0 | 45.8 | 25.6–67.2 | 98.9 | 93.8–100.0 | 91.7 | 59.9–98.8 | 87.0 | 82.2–90.6 |
| Diagnostic Categories 1 | 63 | 98.4 | 91.5–100.0 | 85.7 | 42.1–99.6 | 100.0 | 93.6–100.0 | 100.0 | - | 98.2 | 90.1–99.7 |
| Undetermined Categories 2 | 49 | 73.5 | 58.9–85.1 | 29.4 | 10.3–56.0 | 96.9 | 83.8–99.9 | 83.3 | 38.8–97.5 | 72.1 | 65.4–77.9 |
| Group for Analysis | n | Cell Block Contribution for dg n (%) | p Value | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Non-Contributory | Support dg | Crucial for dg | Contributory | |||||||||
| 1 | Cellularity | <10 | 28 | 28 | (100%) | 0 | (0%) | 0 | (0%) | 0 | (0%) | <0.001 |
| 10–50 | 24 | 1 | (4%) | 18 | (75%) | 5 | (21%) | 23 | (96%) | |||
| >50 | 59 | 0 | (0%) | 30 | (51%) | 29 | (49%) | 59 | (100%) | |||
| 2 | Cell Block Method | Plasma-thrombin | 53 | 14 | (26%) | 25 | (47%) | 14 | (26%) | 39 | (74%) | 1.000 |
| Visible Fragments 1 | 42 | 8 | (19%) | 18 | (43%) | 16 | (38%) | 34 | (81%) | 0.263 | ||
| Shandon | 9 | 5 | (56%) | 4 | (44%) | 0 | (0%) | 4 | (44%) | 0.047 | ||
| In-house method | 5 | 1 | (20%) | 1 | (20%) | 3 | (60%) | 4 | (80%) | 1.000 | ||
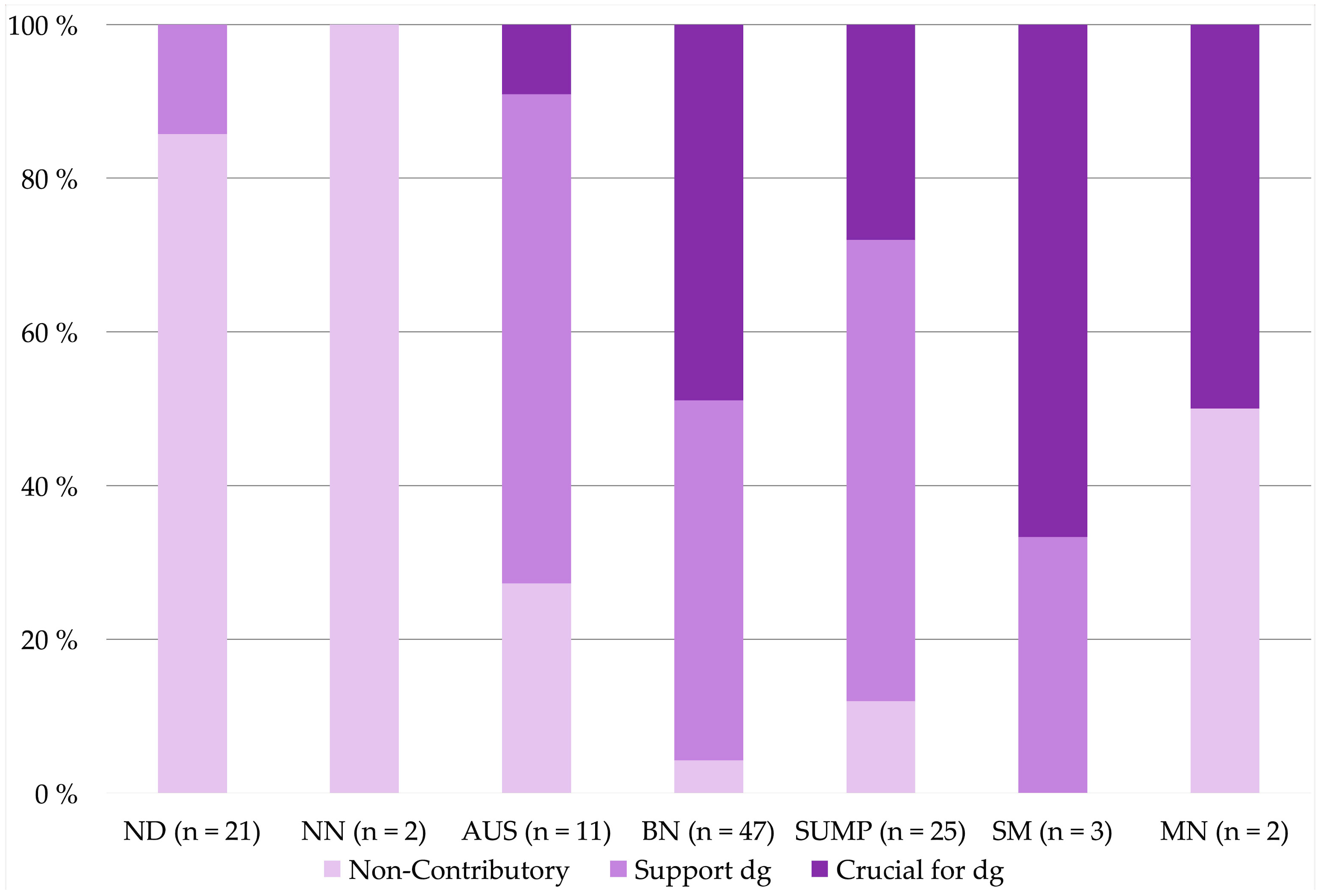
| 3 | MSRSGC Categories | Non-Diagnostic | 21 | 18 | (86%) | 3 | (14%) | 0 | (0%) | 3 | (14%) | <0.001 |
| Non-Neoplastic | 2 | 2 | (100%) | 0 | (0%) | 0 | (0%) | 0 | (0%) | 0.067 | ||
| AUS | 11 | 3 | (27%) | 7 | (64%) | 1 | (9%) | 8 | (73%) | 1.000 | ||
| Benign Neoplasm | 47 | 2 | (4%) | 22 | (47%) | 23 | (49%) | 45 | (96%) | <0.001 | ||
| SUMP | 25 | 3 | (12%) | 15 | (60%) | 7 | (28%) | 22 | (88%) | 0.076 | ||
| Suspicious for Malignancy | 3 | 0 | (0%) | 1 | (33%) | 2 | (67%) | 3 | (100%) | 0.566 | ||
| Malignant Neoplasm | 2 | 1 | (50%) | 0 | (0%) | 1 | (50%) | 1 | (50%) | 0 | ||
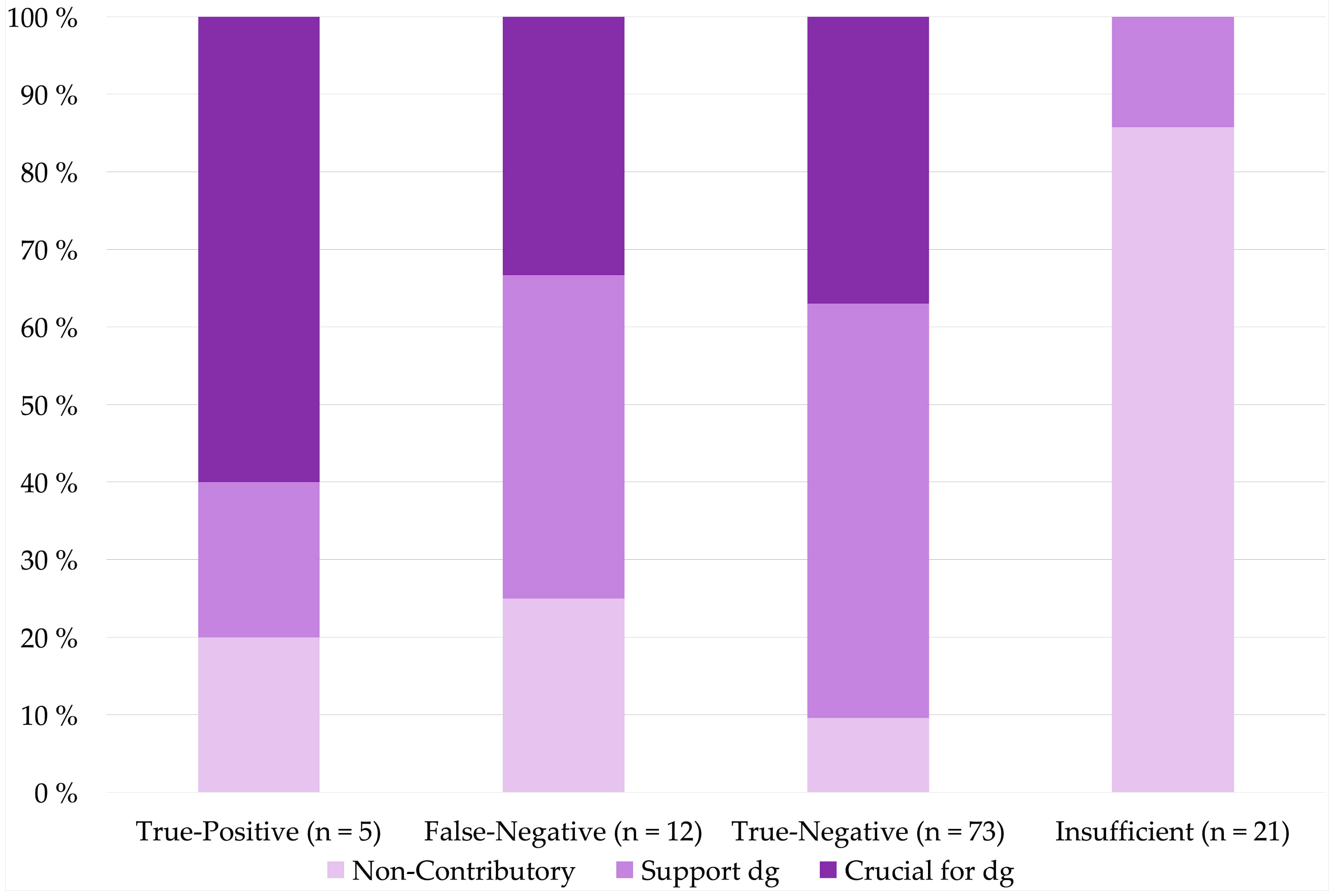
| 4 | Accuracy | True-Positive | 5 | 1 | (20%) | 1 | (20%) | 3 | (60%) | 4 | (80%) | 1.000 |
| False-Negative | 12 | 3 | (25%) | 5 | (42%) | 4 | (33%) | 9 | (75%) | 1.000 | ||
| True-Negative | 73 | 7 | (10%) | 39 | (53%) | 27 | (37%) | 66 | (90%) | <0.001 | ||
| Insufficient | 21 | 18 | (86%) | 3 | (14%) | 0 | (0%) | 3 | (14%) | <0.001 | ||
| n | Cytology Determining Malignancy n (%) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| True-Positive | False Positive | True-Negative | False-Negative | Insufficient | ||||||||
| Cell Block Method | Plasma-thrombin | 53 | 5 | (9%) | N.D. | 30 | (57%) | 8 | (15%) | 10 | (19%) | |
| Visible Fragments 1 | 42 | 0 | (0%) | N.D. | 32 | (76%) | 3 | (7%) | 7 | (17%) | ||
| Shandon | 9 | 0 | (0%) | N.D. | 6 | (67%) | 1 | (11%) | 2 | (22%) | ||
| In-house method | 5 | 0 | (0%) | N.D. | 4 | (80%) | 0 | (0%) | 1 | (20%) | ||
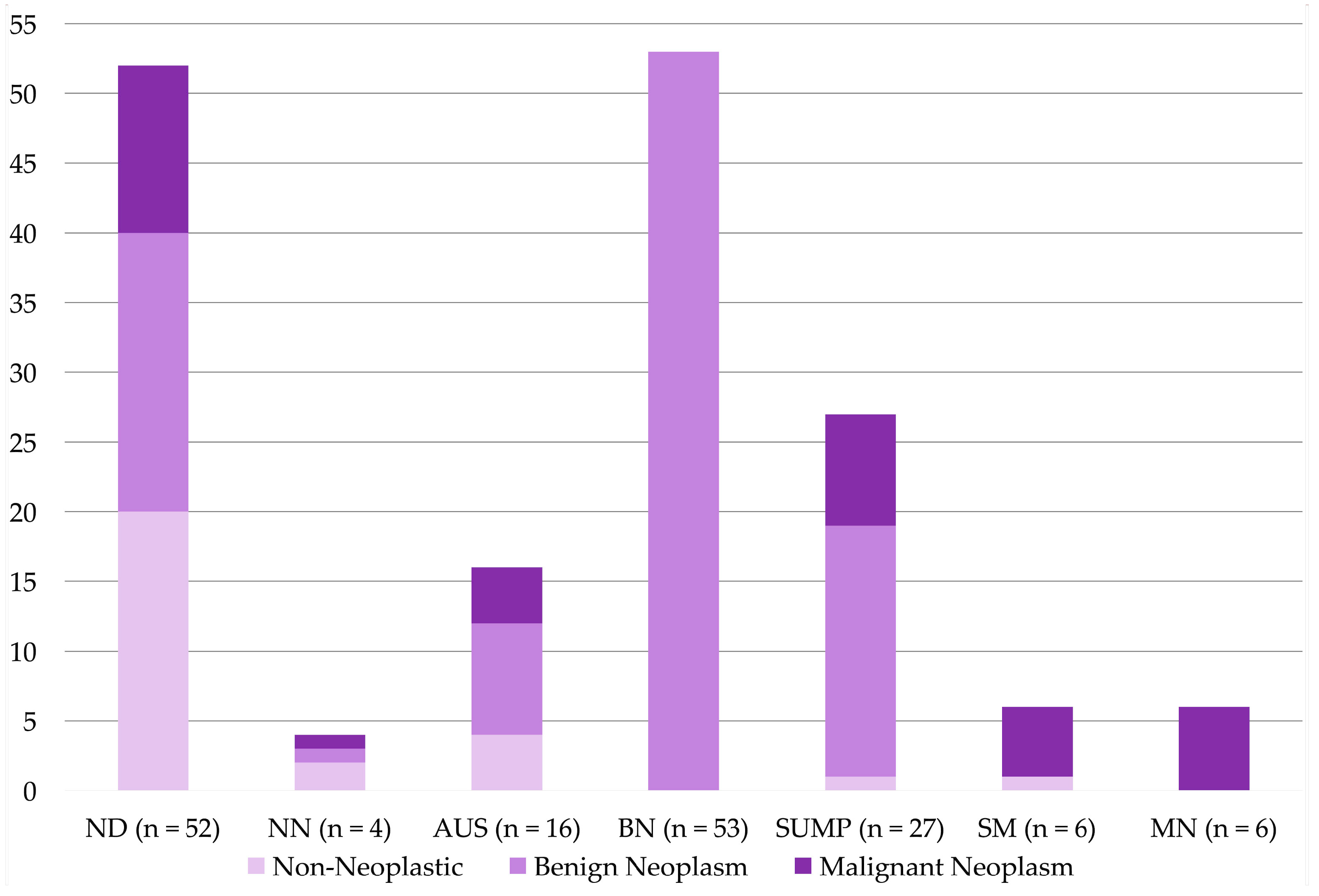
| MSRSGC Categories | Non-Diagnostic | 52 | N.D. | N.D. | N.D. | N.D. | 52 | (100%) | ||||
| Non-Neoplastic | 4 | N.D. | N.D. | 3 | (75%) | 1 | (25%) | N.D. | ||||
| AUS | 16 | N.D. | N.D. | 12 | (75%) | 4 | (25%) | N.D. | ||||
| Benign Neoplasm | 53 | N.D. | N.D. | 53 | (100%) | 0 | (0%) | N.D. | ||||
| SUMP | 27 | N.D. | N.D. | 19 | (70%) | 8 | (30%) | N.D. | ||||
| Suspicious for Malignancy | 6 | 5 | (83%) | 1 | (17%) | N.D. | N.D. | N.D. | ||||
| Malignant Neoplasm | 6 | 6 | (100%) | 0 | (0%) | N.D. | N.D. | N.D. | ||||
| Group for Analyses | n | ICC Contribution for dg n (%) | p-Value | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| No ICC | Supporting dg | Crucial for dg | Contributory | ||||||||
| 1 | Cellularity | <10 | 28 | 28 | (100%) | 0 | (0%) | 0 | (0%) | 0 (0%) | |
| 10–50 | 24 | 19 | (79%) | 4 | (17%) | 1 | (4%) | 5 (21%) | <0.001 | ||
| >50 | 59 | 33 | (56%) | 23 | (39%) | 3 | (5%) | 26 (44%) | |||
| 2 | Cell Block Method | Plasma-thrombin | 53 | 36 | (68%) | 13 | (25%) | 4 | (8%) | 17 (33%) | 0.525 |
| Visible Fragments 1 | 42 | 29 | (69%) | 13 | (31%) | 0 | (0%) | 13 (31%) | 0.668 | ||
| Shandon | 9 | 8 | (89%) | 1 | (11%) | 0 | (0%) | 1 (11%) | 0.285 | ||
| In-house method | 5 | 5 | (100%) | 0 | (0%) | 0 | (0%) | 0 (0%) | 0.319 | ||
| 3 | MSRSGC Categories | Non-Diagnostic | 21 | 21 | (100%) | 0 | (0%) | 0 | (0%) | 0 (0%) | 0.002 |
| Non-Neoplastic | 2 | 2 | (100%) | 0 | (0%) | 0 | (0%) | 0 (0%) | 1.000 | ||
| AUS | 11 | 9 | (82%) | 2 | (18%) | 0 | (0%) | 2 (18%) | 0.514 | ||
| Benign Neoplasm | 47 | 41 | (87%) | 5 | (11%) | 1 | (2%) | 6 (13%) | 0.003 | ||
| SUMP | 25 | 5 | (20%) | 20 | (80%) | 0 | (0%) | 20 (80%) | <0.001 | ||
| Suspicious for Malignancy | 3 | 1 | (33%) | 0 | (0%) | 2 | (67%) | 2 (67%) | 0.065 | ||
| Malignant Neoplasm | 2 | 1 | (50%) | 0 | (0%) | 1 | (50%) | 1 (50%) | 1.000 | ||
| 4 | Accuracy | True-Positive | 5 | 2 | (40%) | 0 | (0%) | 3 | (60%) | 3 (60%) | 0.132 |
| False-Negative | 12 | 4 | (33%) | 8 | (67%) | 0 | (0%) | 8 (67%) | 0.004 | ||
| True-Negative | 73 | 53 | (73%) | 19 | (26%) | 1 | (1%) | 20 (27%) | 1.000 | ||
| Insufficient | 21 | 21 | (100%) | 0 | (0%) | 0 | (0%) | 0 (0%) | 0.002 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tommola, E.; Kalfert, D.; Hakso-Mäkinen, H.; Kholová, I. The Contributory Role of Cell Blocks in Salivary Gland Neoplasms Fine Needle Aspirations Classified by the Milan System for Reporting Salivary Gland Cytology. Diagnostics 2021, 11, 1778. https://doi.org/10.3390/diagnostics11101778
Tommola E, Kalfert D, Hakso-Mäkinen H, Kholová I. The Contributory Role of Cell Blocks in Salivary Gland Neoplasms Fine Needle Aspirations Classified by the Milan System for Reporting Salivary Gland Cytology. Diagnostics. 2021; 11(10):1778. https://doi.org/10.3390/diagnostics11101778
Chicago/Turabian StyleTommola, Erkka, David Kalfert, Heli Hakso-Mäkinen, and Ivana Kholová. 2021. "The Contributory Role of Cell Blocks in Salivary Gland Neoplasms Fine Needle Aspirations Classified by the Milan System for Reporting Salivary Gland Cytology" Diagnostics 11, no. 10: 1778. https://doi.org/10.3390/diagnostics11101778
APA StyleTommola, E., Kalfert, D., Hakso-Mäkinen, H., & Kholová, I. (2021). The Contributory Role of Cell Blocks in Salivary Gland Neoplasms Fine Needle Aspirations Classified by the Milan System for Reporting Salivary Gland Cytology. Diagnostics, 11(10), 1778. https://doi.org/10.3390/diagnostics11101778