
The Translational Role of MUC8 in Salivary Glands: A Potential Biomarker for Salivary Stone Disease?

 , ,
, , 
Abstract
1. Introduction
2. Results
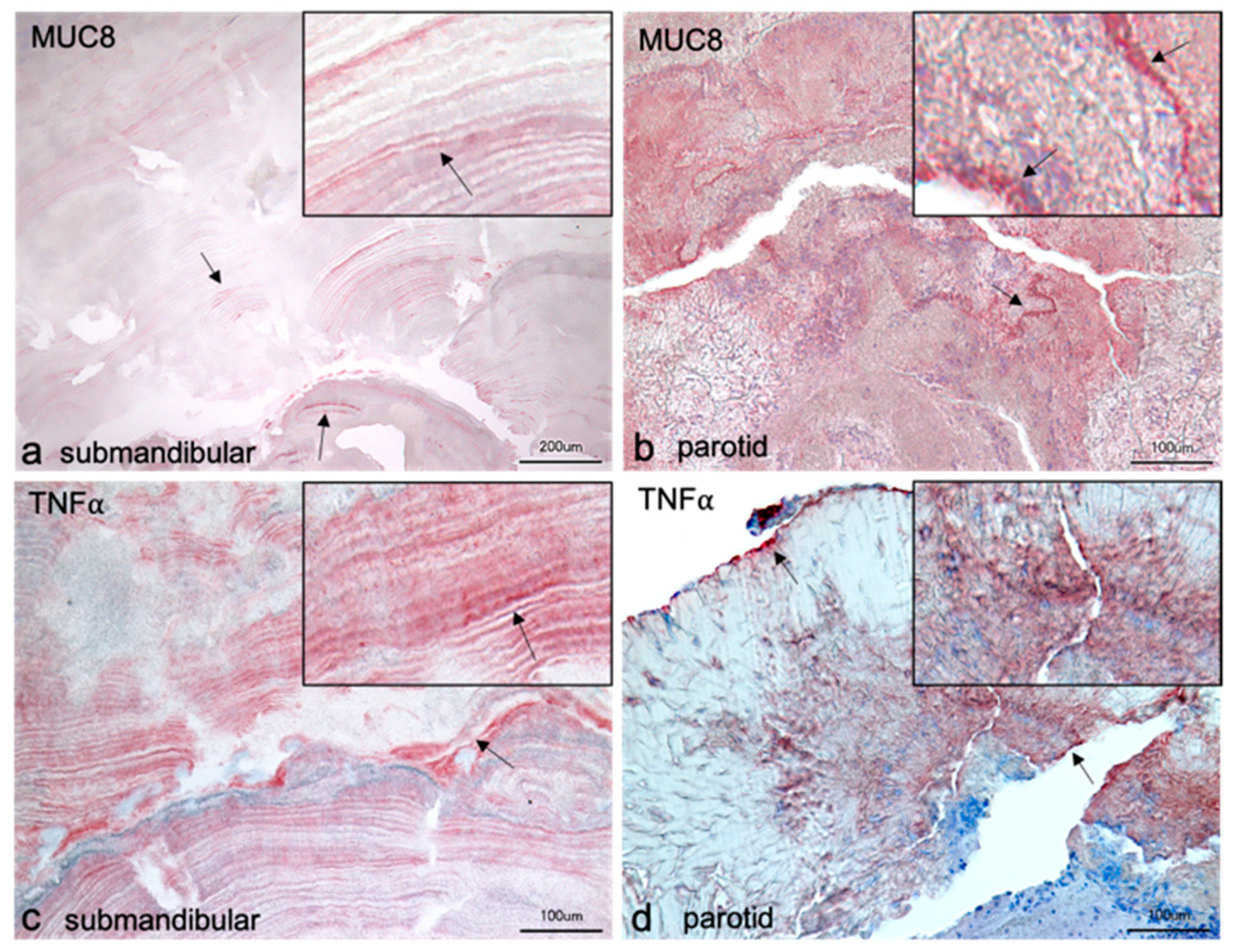
2.1. Localization of MUC8 in Submandibular and Parotid Glands
2.2. Localization of TNFα in Submandibular and Parotid Glands
2.3. Localization of MUC8 and TNFα in Salivary Stones from Submandibular Gland
2.4. Localization of MUC8 and TNFα in Salivary Stones from Parotid Gland
2.5. MUC8 Is Detectable in All Salivary Stones
2.6. MUC8 ELISA of Submandibular Salivary Stones
2.7. MUC8 Is More Abundant in Females
3. Discussion
4. Materials and Methods
4.1. Tissues, Sialoliths, and Saliva
4.1.1. Salivary Gland Tissue
4.1.2. Sialoliths
4.1.3. Saliva
4.2. Immunohistochemistry
4.3. Protein Isolation and Determination of Protein Concentration from Salivary Stones
4.4. Visualization of MUC8 by Immunoblot Analysis
4.5. Enzyme-Linked Immunosorbent Assay (ELISA)
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Kraaij, S.; Karagozoglu, K.H.; Forouzanfar, T.; Veerman, E.C.; Brand, H.S. Salivary stones: Symptoms, aetiology, biochemical composition and treatment. Br. Dent. J. 2014, 217, E23. [Google Scholar] [CrossRef]
- Epivatianos, A.; Harrison, J.D. The presence of microcalculi in normal human submandibular and parotid salivary glands. Arch. Oral Biol. 1989, 34, 261–265. [Google Scholar] [CrossRef]
- Slomiany, B.L.; Murty, V.L.; Aono, M.; Slomiany, A.; Mandel, I.D. Lipid composition of the matrix of human submandibular salivary gland stones. Arch. Oral Biol. 1982, 27, 673–677. [Google Scholar] [CrossRef]
- Slomiany, B.L.; Murty, V.L.; Aono, M.; Slomiany, A.; Mandel, I.D. Lipid composition of human parotid salivary gland stones. J. Dent. Res. 1983, 62, 866–869. [Google Scholar] [CrossRef]
- Huoh, K.C.; Eisele, D.W. Etiologic factors in sialolithiasis. Otolaryngol. Head Neck Surg. 2011, 145, 935–939. [Google Scholar] [CrossRef] [PubMed]
- Ben Lagha, N.; Alantar, A.; Samson, J.; Chapireau, D.; Maman, L. Lithiasis of minor salivary glands: Current data. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2005, 100, 345–348. [Google Scholar] [CrossRef]
- Marchal, F.; Kurt, A.M.; Dulguerov, P.; Becker, M.; Oedman, M.; Lehmann, W. Histopathology of submandibular glands removed for sialolithiasis. Ann. Otol. Rhinol. Laryngol. 2001, 110, 464–469. [Google Scholar] [CrossRef] [PubMed]
- Marchal, F.; Kurt, A.M.; Dulguerov, P.; Lehmann, W. Retrograde theory in sialolithiasis formation. Arch. Otolaryngol. Head Neck Surg. 2001, 127, 66–68. [Google Scholar] [CrossRef] [PubMed]
- Antoniadis, D.; Mendonidou, L.; Papanayotou, P.; Trigonidis, G. Clinical study of sialolithiasis. Findings from 100 cases. Hell. Stomatol. Chron. 1989, 33, 245–251. [Google Scholar]
- Lustmann, J.; Regev, E.; Melamed, Y. Sialolithiasis. A survey on 245 patients and a review of the literature. Int. J. Oral. Maxillofac. Surg 1990, 19, 135–138. [Google Scholar] [CrossRef]
- Schroder, S.A.; Homoe, P.; Wagner, N.; Bardow, A. Does saliva composition affect the formation of sialolithiasis? J. Laryngol. Otol. 2017, 131, 162–167. [Google Scholar] [CrossRef]
- Harrison, J.D. Causes, natural history, and incidence of salivary stones and obstructions. Otolaryngol. Clin. N. Am. 2009, 42, 927–947. [Google Scholar] [CrossRef]
- Schapher, M.; Koch, M.; Weidner, D.; Scholz, M.; Wirtz, S.; Mahajan, A.; Herrmann, I.; Singh, J.; Knopf, J.; Leppkes, M.; et al. Neutrophil Extracellular Traps Promote the Development and Growth of Human Salivary Stones. Cells 2020, 9, 2139. [Google Scholar] [CrossRef]
- Jayasree, R.S.; Gupta, A.K.; Vivek, V.; Nayar, V.U. Spectroscopic and thermal analysis of a submandibular sialolith of Wharton’s duct resected using Nd:YAG laser. Lasers Med. Sci. 2008, 23, 125–131. [Google Scholar] [CrossRef]
- Osuoji, C.I.; Rowles, S.L. Studies on the organic composition of dental calculus and related calculi. Calcif. Tissue Res. 1974, 16, 193–200. [Google Scholar] [CrossRef]
- Proctor, G.B.; McGurk, M.; Harrison, J.D. Protein composition of submandibular stones. J. Dent. Res. 2005, 84, Ab0218. [Google Scholar]
- Paulsen, F.P.; Berry, M.S. Mucins and TFF peptides of the tear film and lacrimal apparatus. Prog. Histochem. Cytochem. 2006, 41, 1–53. [Google Scholar] [CrossRef]
- Mannweiler, S.; Beham, A.; Langner, C. MUC1 and MUC2 expression in salivary gland tumors and in non-neoplastic salivary gland tissue. APMIS 2003, 111, 978–984. [Google Scholar] [CrossRef]
- Kutta, H.; May, J.; Jaehne, M.; Munscher, A.; Paulsen, F.P. Antimicrobial defence mechanisms of the human parotid duct. J. Anat. 2006, 208, 609–619. [Google Scholar] [CrossRef] [PubMed]
- Carlen, A.; Eliasson, L.; Aronsson, G.; Birkhed, D. Human minor and major gland saliva proteins and ability to mediate Actinomyces naeslundii adherence. Arch. Oral Biol. 2004, 49, 177–181. [Google Scholar] [CrossRef]
- Jagla, W.; Wiede, A.; Hinz, M.; Dietzmann, K.; Gulicher, D.; Gerlach, K.L.; Hoffmann, W. Secretion of TFF-peptides by human salivary glands. Cell Tissue Res. 1999, 298, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Wickstrom, C.; Christersson, C.; Davies, J.R.; Carlstedt, I. Macromolecular organization of saliva: Identification of ‘insoluble’ MUC5B assemblies and non-mucin proteins in the gel phase. Biochem. J. 2000, 351, 421–428. [Google Scholar] [CrossRef]
- Nielsen, P.A.; Bennett, E.P.; Wandall, H.H.; Therkildsen, M.H.; Hannibal, J.; Clausen, H. Identification of a major human high molecular weight salivary mucin (MG1) as tracheobronchial mucin MUC5B. Glycobiology 1997, 7, 413–419. [Google Scholar] [CrossRef] [PubMed]
- Piludu, M.; Rayment, S.A.; Liu, B.; Offner, G.D.; Oppenheim, F.G.; Troxler, R.F.; Hand, A.R. Electron microscopic immunogold localization of salivary mucins MG1 and MG2 in human submandibular and sublingual glands. J. Histochem. Cytochem. Off. J. Histochem. Soc. 2003, 51, 69–79. [Google Scholar] [CrossRef][Green Version]
- Piras, M.; Hand, A.R.; Piludu, M. Electron microscopic immunogold localization of salivary mucin MUC5B in human buccal and palatal glands. Acta Histochem. 2011, 113, 844–847. [Google Scholar] [CrossRef]
- Sonesson, M.; Wickstrom, C.; Kinnby, B.; Ericson, D.; Matsson, L. Mucins MUC5B and MUC7 in minor salivary gland secretion of children and adults. Arch. Oral Biol. 2008, 53, 523–527. [Google Scholar] [CrossRef]
- Veerman, E.C.; van den Keijbus, P.A.; Nazmi, K.; Vos, W.; van der Wal, J.E.; Bloemena, E.; Bolscher, J.G.; Amerongen, A.V. Distinct localization of MUC5B glycoforms in the human salivary glands. Glycobiology 2003, 13, 363–366. [Google Scholar] [CrossRef]
- Cohen, R.E.; Aguirre, A.; Neiders, M.E.; Levine, M.J.; Jones, P.C.; Reddy, M.S.; Haar, J.G. Immunochemistry and immunogenicity of low molecular weight human salivary mucin. Arch. Oral Biol. 1991, 36, 347–356. [Google Scholar] [CrossRef]
- Shankar, V.; Gilmore, M.S.; Elkins, R.C.; Sachdev, G.P. A novel human airway mucin cDNA encodes a protein with unique tandem-repeat organization. Biochem. J. 1994, 300, 295–298. [Google Scholar] [CrossRef] [PubMed]
- Shankar, V.; Pichan, P.; Eddy, R.L., Jr.; Tonk, V.; Nowak, N.; Sait, S.N.; Shows, T.B.; Schultz, R.E.; Gotway, G.; Elkins, R.C.; et al. Chromosomal localization of a human mucin gene (MUC8) and cloning of the cDNA corresponding to the carboxy terminus. Am. J. Respir. Cell Mol. Biol. 1997, 16, 232–241. [Google Scholar] [CrossRef] [PubMed]
- Cha, H.J.; Song, K.S. Effect of MUC8 on Airway Inflammation: A Friend or a Foe? J. Clin. Med. 2018, 7, 26. [Google Scholar] [CrossRef]
- Seong, J.K.; Koo, J.S.; Lee, W.J.; Kim, H.N.; Park, J.Y.; Song, K.S.; Hong, J.H.; Yoon, J.H. Upregulation of MUC8 and downregulation of MUC5AC by inflammatory mediators in human nasal polyps and cultured nasal epithelium. Acta Otolaryngol. 2002, 122, 401–407. [Google Scholar] [CrossRef]
- Yoon, J.H.; Kim, K.S.; Kim, H.U.; Linton, J.A.; Lee, J.G. Effects of TNF-alpha and IL-1 beta on mucin, lysozyme, IL-6 and IL-8 in passage-2 normal human nasal epithelial cells. Acta Otolaryngol. 1999, 119, 905–910. [Google Scholar]
- Takeshita, H.; Ishihara, A.; Yamashita, T.; Itoh, A.; Yoshida, K.; Fukaya, M. A case of a salivary calculus containing a limb of a shrimp--the structural analysis. Aichi Gakuin Dent. Sci. 1990, 3, 49–58. [Google Scholar]
- Ali, M.J.; Scholz, M.; Singh, S.; Heichel, J.; Paulsen, F. Etiopathogenesis of lacrimal sac mucopeptide concretions: Insights from cinematic rendering techniques. Graefe’s Arch. Clin. Exp. Ophthalmol. 2020, 258, 2299–2303. [Google Scholar] [CrossRef]
- Lau, I.; Potluri, A.; Ibeh, C.L.; Redman, R.S.; Paal, E.; Bandyopadhyay, B.C. Microcalcifications in stone-obstructed human submandibular gland are associated with apoptosis and cell proliferation. Arch. Oral Biol. 2017, 82, 99–108. [Google Scholar] [CrossRef]
- Kim, C.H.; Kim, H.J.; Song, K.S.; Seong, J.K.; Kim, K.S.; Lee, J.G.; Yoon, J.H. MUC8 as a ciliated cell marker in human nasal epithelium. Acta Otolaryngol. 2005, 125, 76–81. [Google Scholar] [CrossRef]
- Choi, J.Y.; Kim, J.Y.; Kim, C.W.; Ho, J.S.; Lee, K.D.; Yoo, J.B.; Ahn, Y.E.; Yoon, J.H. IL-1beta promotes the ciliogenesis of human middle ear epithelial cells: Possible linkage with the expression of mucin gene 8. Acta Otolaryngol. 2005, 125, 260–265. [Google Scholar] [CrossRef]
- Kim, C.H.; Song, K.S.; Koo, J.S.; Kim, H.U.; Cho, J.Y.; Kim, H.J.; Yoon, J.H. IL-13 suppresses MUC5AC gene expression and mucin secretion in nasal epithelial cells. Acta Otolaryngol. 2002, 122, 638–643. [Google Scholar] [CrossRef]
- Lee, H.M.; Kim, D.H.; Kim, J.M.; Lee, S.H.; Hwang, S.J. MUC8 mucin gene up-regulation in chronic rhinosinusitis. Ann. Otol. Rhinol. Laryngol. 2004, 113, 662–666. [Google Scholar] [CrossRef]
- Finkbeiner, W.E.; Zlock, L.T.; Morikawa, M.; Lao, A.Y.; Dasari, V.; Widdicombe, J.H. Cystic fibrosis and the relationship between mucin and chloride secretion by cultures of human airway gland mucous cells. Am. J. Physiol. Lung Cell Mol. Physiol. 2011, 301, L402–L414. [Google Scholar] [CrossRef]
- Lee, S.R.; Kim, W.T.; Kim, T.N.; Nam, J.K.; Kim, W.J.; Leem, S.H. Association between the length of the MUC8-minisatellite 5 region and susceptibility to chronic obstructive pulmonary disease (COPD). Genes Genom. 2018, 40, 123–127. [Google Scholar] [CrossRef]
- Leikauf, G.D.; Borchers, M.T.; Prows, D.R.; Simpson, L.G. Mucin apoprotein expression in COPD. Chest 2002, 121, 166S–182S. [Google Scholar] [CrossRef] [PubMed]
- Cha, H.J.; Jung, M.S.; Ahn, D.W.; Choi, J.K.; Ock, M.S.; Kim, K.S.; Yoon, J.H.; Song, E.J.; Song, K.S. Silencing of MUC8 by siRNA increases P2Y(2)-induced airway inflammation. Am. J. Physiol. Lung Cell Mol. Physiol. 2015, 308, L495–L502. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Kim, Y.I.; Im, C.N.; Kim, S.W.; Kim, S.J.; Min, S.; Joo, Y.H.; Yim, S.V.; Chung, N. Grape Seed Proanthocyanidin Inhibits Mucin Synthesis and Viral Replication by Suppression of AP-1 and NF-kappaB via p38 MAPKs/JNK Signaling Pathways in Respiratory Syncytial Virus-Infected A549 Cells. J. Agric. Food Chem. 2017, 65, 4472–4483. [Google Scholar] [CrossRef]
- Song, S.Y.; Bae, C.H.; Choi, Y.S.; Kim, Y.D. Cadmium induces mucin 8 expression via Toll-like receptor 4-mediated extracellular signal related kinase 1/2 and p38 mitogen-activated protein kinase in human airway epithelial cells. Int. Forum Allergy Rhinol. 2016, 6, 638–645. [Google Scholar] [CrossRef]
- Bae, C.H.; Jeon, B.S.; Choi, Y.S.; Song, S.Y.; Kim, Y.D. Delphinidin Inhibits LPS-Induced MUC8 and MUC5B Expression Through Toll-like Receptor 4-Mediated ERK1/2 and p38 MAPK in Human Airway Epithelial Cells. Clin. Exp. Otorhinolaryngol. 2014, 7, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Song, S.Y.; Jung, E.C.; Bae, C.H.; Choi, Y.S.; Kim, Y.D. Visfatin induces MUC8 and MUC5B expression via p38 MAPK/ROS/NF-kappaB in human airway epithelial cells. J. Biomed. Sci. 2014, 21, 49. [Google Scholar] [CrossRef]
- Bae, C.H.; Kim, J.S.; Song, S.Y.; Kim, Y.W.; Park, S.Y.; Kim, Y.D. Insulin-like growth factor-1 induces MUC8 and MUC5B expression via ERK1 and p38 MAPK in human airway epithelial cells. Biochem. Biophys. Res. Commun. 2013, 430, 683–688. [Google Scholar] [CrossRef]
- Cho, K.N.; Choi, J.Y.; Kim, C.H.; Baek, S.J.; Chung, K.C.; Moon, U.Y.; Kim, K.S.; Lee, W.J.; Koo, J.S.; Yoon, J.H. Prostaglandin E2 induces MUC8 gene expression via a mechanism involving ERK MAPK/RSK1/cAMP response element binding protein activation in human airway epithelial cells. J. Biol. Chem. 2005, 280, 6676–6681. [Google Scholar] [CrossRef] [PubMed]
- Moon, U.Y.; Kim, C.H.; Choi, J.Y.; Kim, Y.J.; Choi, Y.H.; Yoon, H.G.; Kim, H.; Yoon, J.H. AP2alpha is essential for MUC8 gene expression in human airway epithelial cells. J. Cell Biochem. 2010, 110, 1386–1398. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.S.; Bae, C.H.; Song, S.Y.; Kim, Y.D. Asian sand dust increases MUC8 and MUC5B expressions via TLR4-dependent ERK2 and p38 MAPK in human airway epithelial cells. Am. J. Rhinol. Allergy 2015, 29, 161–165. [Google Scholar] [CrossRef] [PubMed]
- Song, K.S.; Seong, J.K.; Chung, K.C.; Lee, W.J.; Kim, C.H.; Cho, K.N.; Kang, C.D.; Koo, J.S.; Yoon, J.H. Induction of MUC8 gene expression by interleukin-1 beta is mediated by a sequential ERK MAPK/RSK1/CREB cascade pathway in human airway epithelial cells. J. Biol. Chem. 2003, 278, 34890–34896. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Kim, C.H.; Ryu, J.H.; Joo, J.H.; Lee, S.N.; Kim, M.J.; Lee, J.G.; Bae, Y.S.; Yoon, J.H. Crosstalk between platelet-derived growth factor-induced Nox4 activation and MUC8 gene overexpression in human airway epithelial cells. Free Radic. Biol. Med. 2011, 50, 1039–1052. [Google Scholar] [CrossRef]
- Yamamoto, M.; Nakata, H.; Kumchantuek, T.; Adhapanyawanich, K.; Iseki, S. Distinct hormonal regulation of two types of sexual dimorphism in submandibular gland of mice. Cell Tissue Res. 2018, 371, 261–272. [Google Scholar] [CrossRef] [PubMed]
- Kusakabe, Y.; Shindo, Y.; Kawai, T.; Takahashi, Y.; Kobori, M.; Inoue, H.; Saito, I. Sex-Based Differences in Smgc Expression in the Submandibular Gland of C57BL/6 Mice. Pathobiology 2016, 83, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Afanas’ev, V.V.; Tkalenko, A.F.; Abdusalamov, M.R. Analysis of salivary pool composition in patients with different results of sialolithiasis treatment by sialo-lithotripsy. Stomatologiia 2003, 82, 36–38. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Salivary Stone No. | MUC8 Concentration in ng/mL | Patient Age at Collection | Sex |
|---|---|---|---|
| 1 | 12.09 | 72 | m |
| 2 | 184.568 | 62 | f |
| 3 | 33.141 | 52 | f |
| 4 | 4.69 | 51 | m |
| 5 | 13.588 | 48 | m |
| 6 | 126.208 | 42 | m |
| 7 | 105.362 | 55 | m |
| 8 | 78.833 | 58 | m |
| 9 | 158.369 | 25 | f |
| 10 | 11.258 | 34 | m |
| 11 | 131.549 | 44 | m |
| 12 | 37.755 | 31 | m |
| 13 | 202.827 | 53 | f |
| 14 | 108.531 | 54 | m |
| Sample | MUC8 Concentration in ng/mL | Salivary Stone | Patient Age at Collection | Sex |
|---|---|---|---|---|
| r1 | 74.813 | 59 | f | |
| l1 | 130.928 | x | ||
| r2 | 50.666 | x | 62 | m |
| l2 | 14.565 | |||
| r3 | 2.531 | 51 | m | |
| l3 | 46.494 | x | ||
| r4 | 1.561 | 64 | m | |
| l4 | 112.571 | x | ||
| r5 | 30.051 | x | 66 | m |
| l5 | 2.05 | |||
| r6 | 5.284 | x | 73 | m |
| l6 | 10.769 | |||
| r7 | 2.749 | 61 | f | |
| l7 | 143.952 | x | ||
| r8 | 2.525 | 60 | f | |
| l8 | 142.044 | x | ||
| r9 | 98.49 | x | 59 | m |
| l9 | 1.026 | |||
| r10 | 1.994 | 72 | f | |
| l10 | 48.113 | x |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schicht, M.; Reichle, A.; Schapher, M.; Garreis, F.; Kleinsasser, B.; Aydin, M.; Sahin, A.; Iro, H.; Paulsen, F. The Translational Role of MUC8 in Salivary Glands: A Potential Biomarker for Salivary Stone Disease? Diagnostics 2021, 11, 2330. https://doi.org/10.3390/diagnostics11122330
Schicht M, Reichle A, Schapher M, Garreis F, Kleinsasser B, Aydin M, Sahin A, Iro H, Paulsen F. The Translational Role of MUC8 in Salivary Glands: A Potential Biomarker for Salivary Stone Disease? Diagnostics. 2021; 11(12):2330. https://doi.org/10.3390/diagnostics11122330
Chicago/Turabian StyleSchicht, Martin, Adrian Reichle, Mirco Schapher, Fabian Garreis, Benedikt Kleinsasser, Malik Aydin, Afsun Sahin, Heinrich Iro, and Friedrich Paulsen. 2021. "The Translational Role of MUC8 in Salivary Glands: A Potential Biomarker for Salivary Stone Disease?" Diagnostics 11, no. 12: 2330. https://doi.org/10.3390/diagnostics11122330
APA StyleSchicht, M., Reichle, A., Schapher, M., Garreis, F., Kleinsasser, B., Aydin, M., Sahin, A., Iro, H., & Paulsen, F. (2021). The Translational Role of MUC8 in Salivary Glands: A Potential Biomarker for Salivary Stone Disease? Diagnostics, 11(12), 2330. https://doi.org/10.3390/diagnostics11122330