
The Perioperatively Altered Neutrophil-to-Lymphocyte Ratio Associates with Impaired DNA Damage Response in Liver Transplantation Recipients with Hepatocellular Carcinoma

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients, Study Design, and Clinical Samples
2.2. Data Collection and Assessments
2.3. RNA Isolation and Quantitative RT-PCR
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics and NLR Predictors
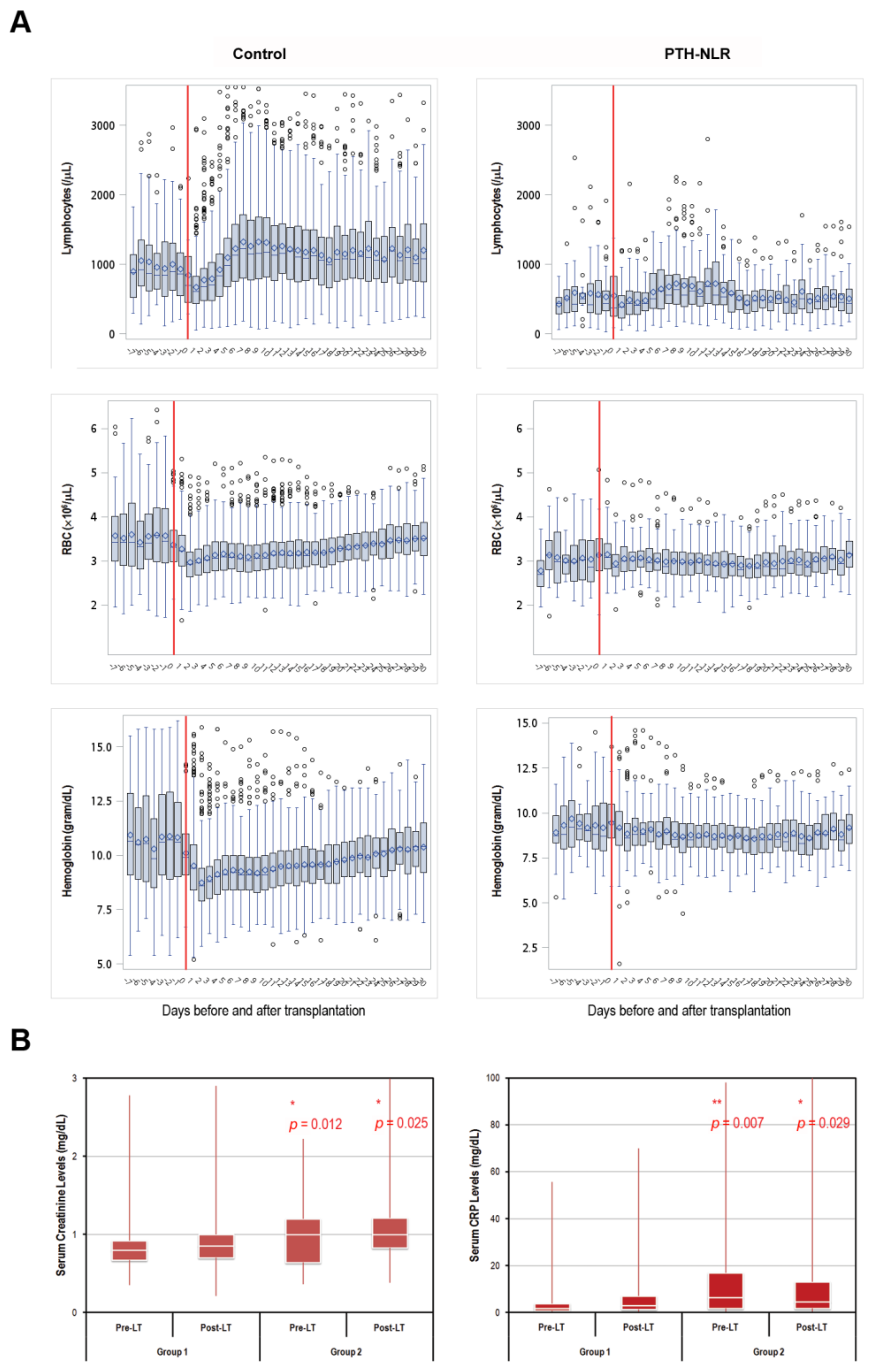
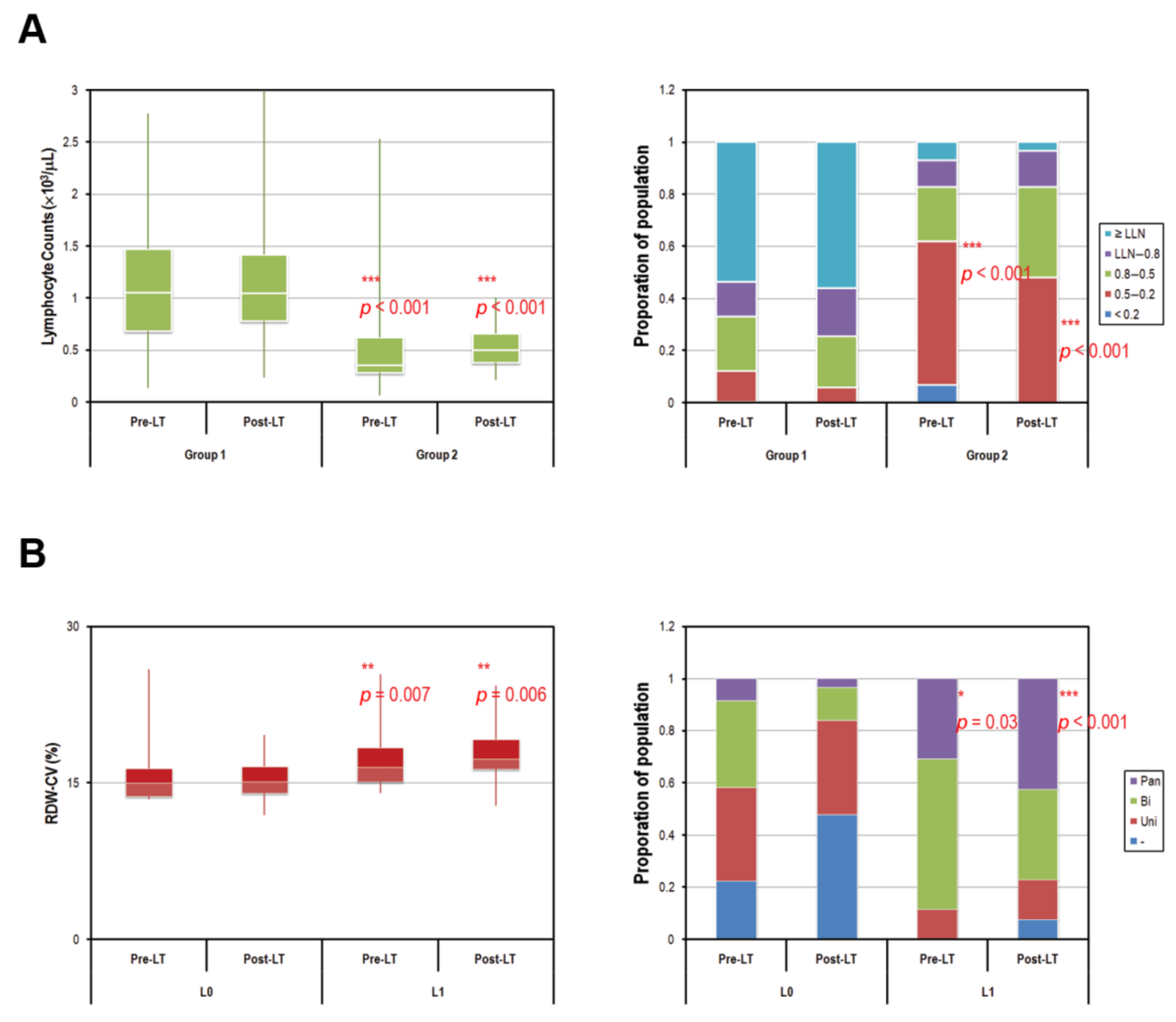
3.2. Peripheral Blood Abnormality in Patients with Persistently High NLR Levels
3.3. Impairment in the Expression of Genes Involved in DNA Damage Repair Pathways in Patients with Persistently High NLR Levels
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Mazzaferro, V.; Llovet, J.M.; Miceli, R.; Bhoori, S.; Schiavo, M.; Mariani, L.; Camerini, T.; Roayaie, S.; Schwartz, M.E.; Grazi, G.L.; et al. Predicting survival after liver transplantation in patients with hepatocellular carcinoma beyond the Milan criteria: A retrospective, exploratory analysis. Lancet Oncol. 2009, 10, 35–43. [Google Scholar] [CrossRef]
- Vitale, A.; Morales, R.R.; Zanus, G.; Farinati, F.; Burra, P.; Angeli, P.; Frigo, A.C.; Del Poggio, P.; Rapaccini, G.; Di Nolfo, M.A.; et al. Barcelona Clinic Liver Cancer staging and transplant survival benefit for patients with hepatocellular carcinoma: A multicentre, cohort study. Lancet Oncol. 2011, 12, 654–662. [Google Scholar] [CrossRef]
- Yong, C.C.; Elsarawy, A.M.; Wang, S.H.; Lin, T.S.; Wang, C.C.; Li, W.F.; Lin, T.L.; Kuo, F.Y.; Cheng, Y.F.; Chen, C.L.; et al. The surgical challenges of salvage living donor liver transplantation for Hepatocellular carcinoma; The cumulative experience of 100 cases—A retrospective cohort study and a propensity score analysis. Int. J. Surg. 2018, 54, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Yoshizumi, T.; Ikegami, T.; Bekki, Y.; Ninomiya, M.; Uchiyama, H.; Iguchi, T.; Yamashita, Y.; Kawanaka, H.; Shirabe, K.; Maehara, Y. Re-evaluation of the predictive score for 6-month graft survival in living donor liver transplantation in the modern era. Liver Transplant. Off. Publ. Am. Assoc. Study Liver Dis. Int. Liver Transplant. Soc. 2014, 20, 323–332. [Google Scholar] [CrossRef] [PubMed]
- Yao, F.Y.; Ferrell, L.; Bass, N.M.; Watson, J.J.; Bacchetti, P.; Venook, A.; Ascher, N.L.; Roberts, J.P. Liver transplantation for hepatocellular carcinoma: Expansion of the tumor size limits does not adversely impact survival. Hepatology 2001, 33, 1394–1403. [Google Scholar] [CrossRef]
- Diakos, C.I.; Charles, K.A.; McMillan, D.C.; Clarke, S.J. Cancer-related inflammation and treatment effectiveness. Lancet Oncol. 2014, 15, e493–e503. [Google Scholar] [CrossRef]
- Prieto, J.; Melero, I.; Sangro, B. Immunological landscape and immunotherapy of hepatocellular carcinoma. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 681–700. [Google Scholar] [CrossRef]
- Motomura, T.; Shirabe, K.; Mano, Y.; Muto, J.; Toshima, T.; Umemoto, Y.; Fukuhara, T.; Uchiyama, H.; Ikegami, T.; Yoshizumi, T.; et al. Neutrophil-lymphocyte ratio reflects hepatocellular carcinoma recurrence after liver transplantation via inflammatory microenvironment. J. Hepatol. 2013, 58, 58–64. [Google Scholar] [CrossRef]
- Mano, Y.; Shirabe, K.; Yamashita, Y.; Harimoto, N.; Tsujita, E.; Takeishi, K.; Aishima, S.; Ikegami, T.; Yoshizumi, T.; Yamanaka, T.; et al. Preoperative neutrophil-to-lymphocyte ratio is a predictor of survival after hepatectomy for hepatocellular carcinoma: A retrospective analysis. Ann. Surg. 2013, 258, 301–305. [Google Scholar] [CrossRef]
- Proctor, M.J.; Talwar, D.; Balmar, S.M.; O’Reilly, D.S.; Foulis, A.K.; Horgan, P.G.; Morrison, D.S.; McMillan, D.C. The relationship between the presence and site of cancer, an inflammation-based prognostic score and biochemical parameters. Initial results of the Glasgow Inflammation Outcome Study. Br. J. Cancer 2010, 103, 870–876. [Google Scholar] [CrossRef]
- Ribezzo, F.; Shiloh, Y.; Schumacher, B. Systemic DNA damage responses in aging and diseases. Semin. Cancer Biol. 2016, 37–38, 26–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jurk, D.; Wilson, C.; Passos, J.F.; Oakley, F.; Correia-Melo, C.; Greaves, L.; Saretzki, G.; Fox, C.; Lawless, C.; Anderson, R.; et al. Chronic inflammation induces telomere dysfunction and accelerates ageing in mice. Nat. Commun. 2014, 2, 4172. [Google Scholar] [CrossRef] [PubMed]
- Rossi, D.J.; Bryder, D.; Seita, J.; Nussenzweig, A.; Hoeijmakers, J.; Weissman, I.L. Deficiencies in DNA damage repair limit the function of haematopoietic stem cells with age. Nature 2007, 447, 725–729. [Google Scholar] [CrossRef] [PubMed]
- Beerman, I.; Seita, J.; Inlay, M.A.; Weissman, I.L.; Rossi, D.J. Quiescent hematopoietic stem cells accumulate DNA damage during aging that is repaired upon entry into cell cycle. Cell Stem Cell 2014, 15, 37–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clavien, P.A.; Lesurtel, M.; Bossuyt, P.M.; Gores, G.J.; Langer, B.; Perrier, A. OLT for HCC Consensus Group. Recommendations for liver transplantation for hepatocellular carcinoma: An international consensus conference report. Lancet Oncol. 2012, 13, e11–e22. [Google Scholar] [CrossRef] [Green Version]
- Kaido, T.; Ogawa, K.; Mori, A.; Fujimoto, Y.; Ito, T.; Tomiyama, K.; Takada, Y.; Uemoto, S. Usefulness of the Kyoto criteria as expanded selection criteria for liver transplantation for hepatocellular carcinoma. Surgery 2013, 154, 1053–1060. [Google Scholar] [CrossRef]
- Zheng, S.S.; Xu, X.; Wu, J.; Chen, J.; Wang, W.L.; Zhang, M.; Liang, T.B.; Wu, L.M. Liver transplantation for hepatocellular carcinoma: Hangzhou experiences. Transplantation 2008, 85, 1726–1732. [Google Scholar] [CrossRef]
- Na, G.H.; Kim, D.G.; Han, J.H.; Kim, E.Y.; Lee, S.H.; Hong, T.H.; You, Y.K. Inflammatory markers as selection criteria of hepatocellular carcinoma in living-donor liver transplantation. World J. Gastroenterol. 2014, 20, 6594–6601. [Google Scholar] [CrossRef]
- Hayashi, H.; Takamura, H.; Ohbatake, Y.; Nakanuma, S.; Tajima, H.; Fushida, S.; Onishi, I.; Tani, T.; Shimizu, K.; Ohta, T. Postoperative changes in neutrophil-to-lymphocyte ratio and platelet count: A simple prognostic predictor for adult-to-adult living donor liver transplantation. Asian J. Surg. 2018, 41, 341–348. [Google Scholar] [CrossRef]
- Li, X.F.; Chen, D.P.; Ouyang, F.Z.; Chen, M.M.; Wu, Y.; Kuang, D.M.; Zheng, L. Increased autophagy sustains the survival and pro-tumourigenic effects of neutrophils in human hepatocellular carcinoma. J. Hepatol. 2015, 62, 131–139. [Google Scholar] [CrossRef]
- Nagai, S.; Yoshida, A.; Kohno, K.; Altshuler, D.; Nakamura, M.; Brown, K.A.; Abouljoud, M.S.; Moonka, D. Peritransplant absolute lymphocyte count as a predictive factor for advanced recurrence of hepatitis C after liver transplantation. Hepatology 2014, 59, 35–45. [Google Scholar] [CrossRef] [PubMed]
- Marks, P.W. Hematologic manifestations of liver disease. Semin. Hematol. 2013, 50, 216–221. [Google Scholar] [CrossRef] [PubMed]
- Walter, D.; Lier, A.; Geiselhart, A.; Thalheimer, F.B.; Huntscha, S.; Sobotta, M.C.; Moehrle, B.; Brocks, D.; Bayindir, I.; Kaschutnig, P.; et al. Exit from dormancy provokes DNA-damage-induced attrition in haematopoietic stem cells. Nature 2015, 520, 549–552. [Google Scholar] [CrossRef] [PubMed]
- Vogel, E.W.; Barbin, A.; Nivard, M.J.; Stack, H.F.; Waters, M.D.; Lohman, P.H. Heritable and cancer risks of exposures to anticancer drugs: Inter-species comparisons of covalent deoxyribonucleic acid-binding agents. Mutat. Res. 1998, 400, 509–540. [Google Scholar] [CrossRef]
- Singh, S.; Brocker, C.; Koppaka, V.; Chen, Y.; Jackson, B.C.; Matsumoto, A.; Thompson, D.C.; Vasiliou, V. Aldehyde dehydrogenases in cellular responses to oxidative/electrophilic stress. Free Radic. Biol. Med. 2013, 56, 89–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimniak, P. Relationship of electrophilic stress to aging. Free Radic. Biol. Med. 2011, 51, 1087–1105. [Google Scholar] [CrossRef] [Green Version]
- Garaycoechea, J.I.; Crossan, G.P.; Langevin, F.; Daly, M.; Arends, M.J.; Patel, K.J. Genotoxic consequences of endogenous aldehydes on mouse haematopoietic stem cell function. Nature 2012, 489, 571–575. [Google Scholar] [CrossRef]
- Pontel, L.B.; Rosado, I.V.; Burgos-Barragan, G.; Garaycoechea, J.I.; Yu, R.; Arends, M.J.; Chandrasekaran, G.; Broecker, V.; Wei, W.; Liu, L.; et al. Endogenous Formaldehyde Is a Hematopoietic Stem Cell Genotoxin and Metabolic Carcinogen. Mol. Cell 2015, 60, 177–188. [Google Scholar] [CrossRef] [Green Version]
- Garaycoechea, J.I.; Crossan, G.P.; Langevin, F.; Mulderrig, L.; Louzada, S.; Yang, F.; Guilbaud, G.; Park, N.; Roerink, S.; Nik-Zainal, S.; et al. Alcohol and endogenous aldehydes damage chromosomes and mutate stem cells. Nature 2018, 553, 171–177. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Kamath, P.S.; Wiesner, R.H.; Malinchoc, M.; Kremers, W.; Therneau, T.M.; Kosberg, C.L.; D’Amico, G.; Dickson, E.R.; Kim, W.R. A model to predict survival in patients with end-stage liver disease. Hepatology 2001, 33, 464–470. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables ǂ | Observations (%) | Univariate Model | Multivariate Model * | ||||
|---|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | ||
| Male | 290 (83.6) | 1.377 | 0.29–1.85 | 0.502 | 0.745 | 0.28–1.98 | 0.555 |
| Age at LT < 57 yr | 214 (61.7) | 1.381 | 0.70–2.71 | 0.348 | 0.983 | 0.94–1.03 | 0.477 |
| Pre-operative 7 days: | |||||||
| Lymphocytes < 500/μL | 70 (20.2) | 2.176 | 1.12–4.23 | 0.013 | 0.232 | ||
| Sodium < 140 | 99 (28.5) | 1.455 | 0.77–2.74 | 0.247 | |||
| CRP ≥ 1.8 | 190 (54.8) | 1.049 | 0.55–1.99 | 0.884 | |||
| Total Bilirubin ≥ 2.65 | 55 (15.9) | 1.842 | 0.90–3.77 | 0.094 | |||
| Direct Bilirubin ≥ 1.25 | 43 (12.4) | 1.778 | 0.82–3.86 | 0.146 | |||
| Albumin < 3.5 g/dL | 231 (66.6) | 1.816 | 0.84–3.95 | 0.132 | |||
| SCr ≥ 1.5 mg/dL | 15 (4.4) | 3.250 | 1.27–8.27 | 0.014 | 0.181 | ||
| RDW-CV ≥ 15% | 171 (49.3) | 1.774 | 0.93–3.40 | 0.084 | |||
| Related inflammatory scores: | |||||||
| NLR ≥ 4 | 53 (15.3) | 2.129 | 1.06–4.26 | 0.033 | 0.408 | ||
| PLR ≥ 136 | 38 (11) | 2.203 | 0.93–4.39 | 0.075 | 0.160 | ||
| LMR < 5.7 | 57 (16.4) | 1.587 | 0.31–1.30 | 0.215 | |||
| Post-operative 30 days | |||||||
| Lymphocytes < 1000/μL | 213 (42.7) | 1.654 | 0.84–3.25 | 0.1437 | |||
| Sodium < 138.5 | 90 (25.9) | 2.956 | 1.59–5.51 | <0.001 | 2.515 | 1.347–4.695 | 0.004 |
| CRP ≥ 5.9 | 113 (32.6) | 2.340 | 1.27–4.32 | 0.006 | 0.309 | ||
| Total Bilirubin ≥ 1.2 | 49 (14.1) | 1.696 | 0.81–3.56 | 0.162 | |||
| Direct Bilirubin ≥ 0.3 | 163 (47) | 1.430 | 0.77–2.67 | 0.261 | |||
| Albumin ≥ 4.5 g/dL | 8 (2.3) | 3.215 | 0.99–10.4 | 0.052 | 0.201 | ||
| SCr ≥ 0.8 mg/dL | 234 (67.4) | 1.507 | 0.72–3.17 | 0.279 | |||
| RDW-CV % ≥ 15% | 255 (73.5) | 3.059 | 1.09–8.59 | 0.034 | 0.100 | ||
| Related inflammatory scores: | |||||||
| NLR ≥ 5 | 82 (23.6) | 3.057 | 1.50–6.25 | 0.002 | 0.339 | ||
| PLR ≥ 180 | 111 (32) | 1.942 | 1.05–3.60 | 0.034 | 0.255 | ||
| LMR < 2 | 63 (18.2) | 2.268 | 1.17–4.39 | 0.015 | 0.197 | ||
| Persistent high NLR(pre-LT NLR ≥ 4–post-LT NLR ≥ 5) | 29 (8.4) | 3.193 | 1.04–9.85 | 0.003 | 4.565 | 1.58–13.2 | 0.005 |
| Characteristics | Pre-NLR Level | p-Value | Post-NLR Level | p-Value | ||
|---|---|---|---|---|---|---|
| <4 (n = 283) | ≥4 (n = 64) | <5 (n = 285) | ≥5 (n = 62) | |||
| Gender | ||||||
| Female | 45 (15.9%) | 12 (18.75%) | 0.5785 | 46 (16.14%) | 11 (17.74%) | 0.7577 |
| Male | 238 (84.1%) | 52 (81.25%) | 239 (83.86%) | 51 (82.26%) | ||
| Complete blood count blood test ≤ 7 days before the index date | ||||||
| Lymphocytes | ||||||
| <500 | 38 (13.43%) | 35 (54.69%) | <0.0001 | 48 (16.84%) | 25 (40.32%) | <0.0001 |
| ≥500 | 245 (86.57%) | 29 (45.31%) | 237 (83.16%) | 37 (59.68%) | . | |
| Segment, count | ||||||
| <1000 | 47 (16.61%) | 6 (9.38%) | 0.1463 | 45 (15.79%) | 8 (12.9%) | 0.567 |
| ≥1000 | 236 (83.39%) | 58 (90.63%) | 240 (84.21%) | 54 (87.1%) | ||
| RBC, count | ||||||
| Male < 4.3/Female < 3.9 | 188 (66.43%) | 42 (65.63%) | 0.902 | 184 (64.56%) | 46 (74.19%) | 0.146 |
| Male ≥ 4.3/Female ≥ 3.9 | 95 (33.57%) | 22 (34.38%) | 101 (35.44%) | 16 (25.81%) | ||
| RDW-CV, count | ||||||
| <15 | 143 (50.53%) | 13 (20.31%) | <0.0001 | 138 (48.42%) | 18 (29.03%) | 0.0054 |
| ≥15 | 140 (49.47%) | 51 (79.69%) | 147 (51.58%) | 44 (70.97%) | ||
| HCT | ||||||
| Male < 41/Female < 36 | 224 (79.15%) | 50 (78.13%) | 0.8556 | 225 (78.95%) | 49 (79.03%) | 0.9881 |
| Male ≥ 41/Female ≥ 36 | 59 (20.85%) | 14 (21.88%) | 60 (21.05%) | 13 (20.97%) | ||
| MCV | ||||||
| <80 | 30 (10.6%) | 7 (10.94%) | 0.9372 | 32 (11.23%) | 5 (8.06%) | 0.4645 |
| ≥80 | 253 (89.4%) | 57 (89.06%) | 253 (88.77%) | 57 (91.94%) | ||
| MCH | ||||||
| <26 | 34 (12.01%) | 8 (12.5%) | 0.9143 | 35 (12.28%) | 7 (11.29%) | 0.8285 |
| ≥26 | 249 (87.99%) | 56 (87.5%) | 250 (87.72%) | 55 (88.71%) | ||
| MCHC | ||||||
| <31 | 13 (4.59%) | 6 (9.38%) | 0.1289 | 13 (4.56%) | 6 (9.68%) | 0.1086 |
| ≥31 | 270 (95.41%) | 58 (90.63%) | 272 (95.44%) | 56 (90.32%) | ||
| Hemoglobin, g/dL | ||||||
| Male < 13.5/Female < 12 | 193 (68.2%) | 57 (89.06%) | 0.0008 | 195 (68.42%) | 55 (88.71%) | 0.0013 |
| Male ≥ 13.5/Female ≥ 12 | 90 (31.8%) | 7 (10.94%) | 90 (31.58%) | 7 (11.29%) | ||
| Platelet (×1000/μL) | ||||||
| <40 | 63 (22.26%) | 18 (28.13%) | 0.3166 | 65 (22.81%) | 16 (25.81%) | 0.6129 |
| ≥40 | 220 (77.74%) | 46 (71.88%) | 220 (77.19%) | 46 (74.19%) | ||
| Liver function (≤7 days) before the index date | ||||||
| Total bilirubin (mg/dL) | ||||||
| <1.4 | 133 (47%) | 37 (57.81%) | 0.118 | 136 (47.72%) | 34 (54.84%) | 0.3095 |
| ≥1.4 | 150 (53%) | 27 (42.19%) | 149 (52.28%) | 28 (45.16%) | ||
| Differential bilirubin (mg/dL) | ||||||
| <0.4 | 99 (35.74%) | 21 (32.81%) | 0.6585 | 97 (34.77%) | 23 (37.1%) | 0.7283 |
| ≥0.4 | 178 (64.26%) | 43 (67.19%) | 182 (65.23%) | 39 (62.9%) | ||
| LDH | ||||||
| Male < 225/Female < 214 | 181 (69.88%) | 40 (65.57%) | 0.5123 | 185 (71.15%) | 36 (60%) | 0.092 |
| Male ≥ 225/Female ≥ 214 | 78 (30.12%) | 21 (34.43%) | 75 (28.85%) | 24 (40%) | ||
| AST | ||||||
| <37 | 83 (29.33%) | 18 (28.13%) | 0.0055 | 82 (28.77%) | 19 (30.65%) | 0.5047 |
| 37−111 | 187 (66.08%) | 36 (56.25%) | 186 (65.26%) | 37 (59.68%) | ||
| ≥111 | 13 (4.59%) | 10 (15.63%) | 17 (5.96%) | 6 (9.68%) | ||
| ALT | ||||||
| <40 | 169 (59.72%) | 37 (57.81%) | 0.0299 | 168 (58.95%) | 38 (61.29%) | 0.7891 |
| 40~120 | 107 (37.81%) | 21 (32.81%) | 107 (37.54%) | 21 (33.87%) | ||
| ≥120 | 7 (2.47%) | 6 (9.38%) | 10 (3.51%) | 3 (4.84%) | ||
| CRP | ||||||
| <5 | 223 (81.39%) | 28 (43.75%) | <0.0001 | 214 (77.54%) | 37 (59.68%) | 0.0037 |
| ≥5 | 51 (18.61%) | 36 (56.25%) | 62 (22.46%) | 25 (40.32%) | ||
| Albumin, mg/dL | ||||||
| <3.5 | 140 (49.47%) | 53 (82.81%) | <0.0001 | 148 (51.93%) | 45 (72.58%) | 0.003 |
| ≥3.5 | 143 (50.53%) | 11 (17.19%) | 137 (48.07%) | 17 (27.42%) | ||
| Renal function (≤ 7 days) before the index date | ||||||
| eGFR, mL/min/1.73 m2 | 0.9752 | 0.4889 | ||||
| <60 | 27 (14.14%) | 6 (13.95%) | 29 (14.8%) | 4 (10.53%) | ||
| ≥60 | 164 (85.86%) | 37 (86.05%) | 167 (85.2%) | 34 (89.47%) | ||
| Electrolytes (≤ 7 days) before the index date | ||||||
| Sodium (Na), mg/dL | ||||||
| <148 | 274 (97.16%) | 62 (98.41%) | 0.5737 | 277 (97.54%) | 59 (96.72%) | 0.7175 |
| ≥148 | 8 (2.84%) | 1 (1.59%) | 7 (2.46%) | 2 (3.28%) | ||
| Calcium (Ca), mg/dL | ||||||
| <10 | 266 (99.63%) | 63 (100%) | 0.6266 | 269 (99.63%) | 60 (100%) | 0.6368 |
| ≥10 | 1 (0.37%) | 0 (0%) | 1 (0.37%) | 0 (0%) | ||
| Chloride (Cl), mg/dL | ||||||
| <112 | 219 (79.35%) | 51 (80.95%) | 0.7753 | 227 (81.65%) | 43 (70.49%) | 0.0599 |
| ≥112 | 57 (20.65%) | 12 (19.05%) | 51 (18.35%) | 18 (29.51%) | ||
| Potassium (K), mg/dL | ||||||
| <3.6 | 81 (28.83%) | 17 (26.56%) | 0.6508 | 79 (27.82%) | 19 (31.15%) | 0.6449 |
| 3.6~5 | 197 (70.11%) | 47 (73.44%) | 202 (71.13%) | 42 (68.85%) | ||
| ≥5 | 3 (1.07%) | 0 (0%) | 3 (1.06%) | 0 (0%) | ||
| Comorbid conditions (≤1 year before the index date) | ||||||
| CCI score | ||||||
| 0 | 4 (1.41%) | 5 (7.81%) | 0.0082 | 5 (1.75%) | 4 (6.45%) | 0.0007 |
| 1–2 | 21 (7.42%) | 7 (10.94%) | 17 (5.96%) | 11 (17.74%) | ||
| ≥3 | 258 (91.17%) | 52 (81.25%) | 263 (92.28%) | 47 (75.81%) | ||
| Congestive heart failure | 1 (0.35%) | 0 (0%) | 0.6339 | 0 (0%) | 1 (1.61%) | 0.0318 |
| Cerebral vascular disease | 1 (0.35%) | 0 (0%) | 0.6339 | 1 (0.35%) | 0 (0%) | 0.6404 |
| Chronic pulmonary diseases | 5 (1.77%) | 2 (3.13%) | 0.4852 | 5 (1.75%) | 2 (3.23%) | 0.4552 |
| Ulcer | 35 (12.37%) | 4 (6.25%) | 0.1617 | 30 (10.53%) | 9 (14.52%) | 0.3674 |
| Liver disease | 271 (95.76%) | 57 (89.06%) | 0.0334 | 273 (95.79%) | 55 (88.71%) | 0.0264 |
| Diabetes without complications | 43 (15.19%) | 8 (12.5%) | 0.5825 | 43 (15.09%) | 8 (12.9%) | 0.6598 |
| Diabetes with complications | 2 (0.71%) | 1 (1.56%) | 0.5042 | 3 (1.05%) | 0 (0%) | 0.4172 |
| Chronic kidney disease | 7 (2.47%) | 3 (4.69%) | 0.339 | 6 (2.11%) | 4 (6.45%) | 0.0638 |
| Severe liver diseases | 38 (13.43%) | 10 (15.63%) | 0.6456 | 40 (14.04%) | 8 (12.9%) | 0.815 |
| Decompensated cirrhosis | 120 (42.4%) | 45 (70.31%) | <0.0001 | 131 (45.96%) | 34 (54.84%) | 0.2048 |
| Basal characteristics | ||||||
| n | 283 | 64 | 285 | 62 | ||
| Age at the index date | ||||||
| mean | 53.83 (7.59) | 55.03 (5.83) | 0.1638. | 54.05 (7.32) | 54.06 (7.32) | 0.988 |
| median | 55 (49–59) | 54 (51–59.5) | 55 (50–59) | 55 (50–60) | ||
| Lymphocytes | ||||||
| mean | 1070 (500) | 579 (400) | <0.0001 | 1033 (510) | 732 (491) | <0.0001 |
| median | 1010 (688–1440) | 454 (307–754) | 983 (608–1426) | 629 (345–963) | ||
| Segment, count | ||||||
| mean | 1893 (951) | 2981 (2509) | 0.001 | 2056 (1209) | 2269 (2202) | 0.828 |
| median | 1806 (1135–2426) | 2449 (1325–3829) | 1836 (1172–2601) | 1665 (1224–2690) | ||
| SCr | ||||||
| mean | 0.85 (0.3) | 0.84 (0.37) | 0.9322 | 0.86 (0.31) | 0.81 (0.34) | 0.2671 |
| median | 0.8 (0.65–0.95) | 0.8 (0.61–0.97) | 0.8 (0.67–0.95) | 0.78 (0.54–0.94) | ||
| MELDScore | ||||||
| mean | 10.04 (2.99) | 13.17 (5.29) | <0.0001 | 10.33 (3.3) | 11.92 (5.11) | 0.0215 |
| median | 9.28 (7.7–11.84) | 11.57 (9.71–15.8) | 9.46 (7.76–12.04) | 10.34 (8.45–13.93) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, K.-D.; Hsu, C.-N.; Wu, Y.-J.; Chu, C.-H.; Huang, K.-T.; Tsai, M.-C.; Chiu, K.-W.; Cheng, B.-C.; Chiu, C.-H.; Chen, C.-L.; et al. The Perioperatively Altered Neutrophil-to-Lymphocyte Ratio Associates with Impaired DNA Damage Response in Liver Transplantation Recipients with Hepatocellular Carcinoma. Diagnostics 2021, 11, 209. https://doi.org/10.3390/diagnostics11020209
Chen K-D, Hsu C-N, Wu Y-J, Chu C-H, Huang K-T, Tsai M-C, Chiu K-W, Cheng B-C, Chiu C-H, Chen C-L, et al. The Perioperatively Altered Neutrophil-to-Lymphocyte Ratio Associates with Impaired DNA Damage Response in Liver Transplantation Recipients with Hepatocellular Carcinoma. Diagnostics. 2021; 11(2):209. https://doi.org/10.3390/diagnostics11020209
Chicago/Turabian StyleChen, Kuang-Den, Chien-Ning Hsu, Yi-Ju Wu, Chi-Hsiang Chu, Kuang-Tzu Huang, Ming-Chao Tsai, King-Wah Chiu, Ben-Chung Cheng, Chien-Hua Chiu, Chao-Long Chen, and et al. 2021. "The Perioperatively Altered Neutrophil-to-Lymphocyte Ratio Associates with Impaired DNA Damage Response in Liver Transplantation Recipients with Hepatocellular Carcinoma" Diagnostics 11, no. 2: 209. https://doi.org/10.3390/diagnostics11020209
APA StyleChen, K.-D., Hsu, C.-N., Wu, Y.-J., Chu, C.-H., Huang, K.-T., Tsai, M.-C., Chiu, K.-W., Cheng, B.-C., Chiu, C.-H., Chen, C.-L., & Lin, C.-C. (2021). The Perioperatively Altered Neutrophil-to-Lymphocyte Ratio Associates with Impaired DNA Damage Response in Liver Transplantation Recipients with Hepatocellular Carcinoma. Diagnostics, 11(2), 209. https://doi.org/10.3390/diagnostics11020209