
Microbiota Biomarkers for Lung Cancer


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Collection and Preparation of Sputum
2.3. Genomic DNA Isolation
2.4. Detection and Quantification of Bacterial Abundances Using Droplet Digital PCR (Ddpcr)
2.5. Statistical Analysis
3. Results
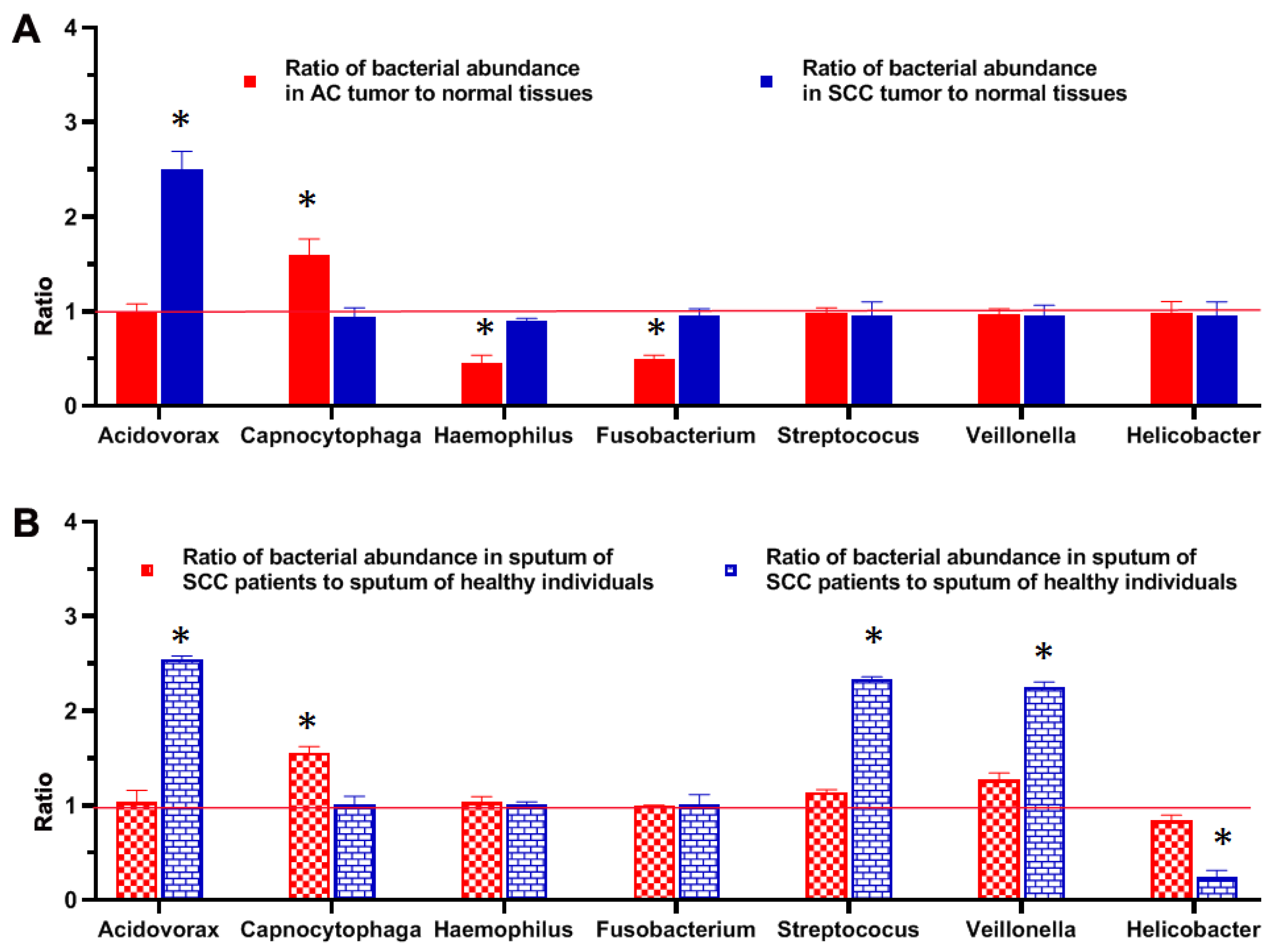
3.1. Bacterial Genera Displayed Different Abundances between Lung Tumor and Noncancerous Lung Tissues
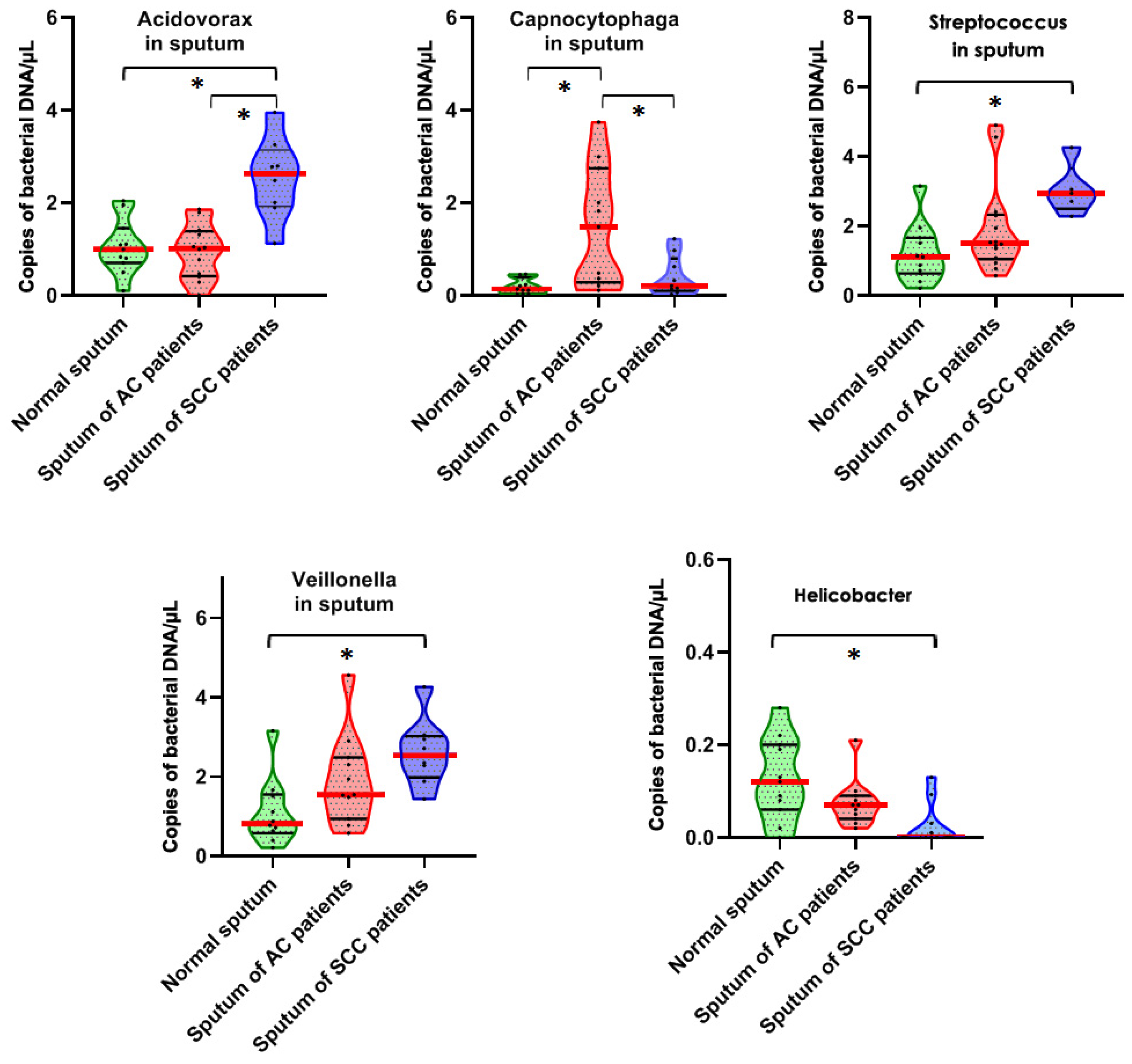
3.2. Bacterial Genera Displayed Different Abundances in Sputum of Lung Cancer Patients vs. Cancer-Free Smokers
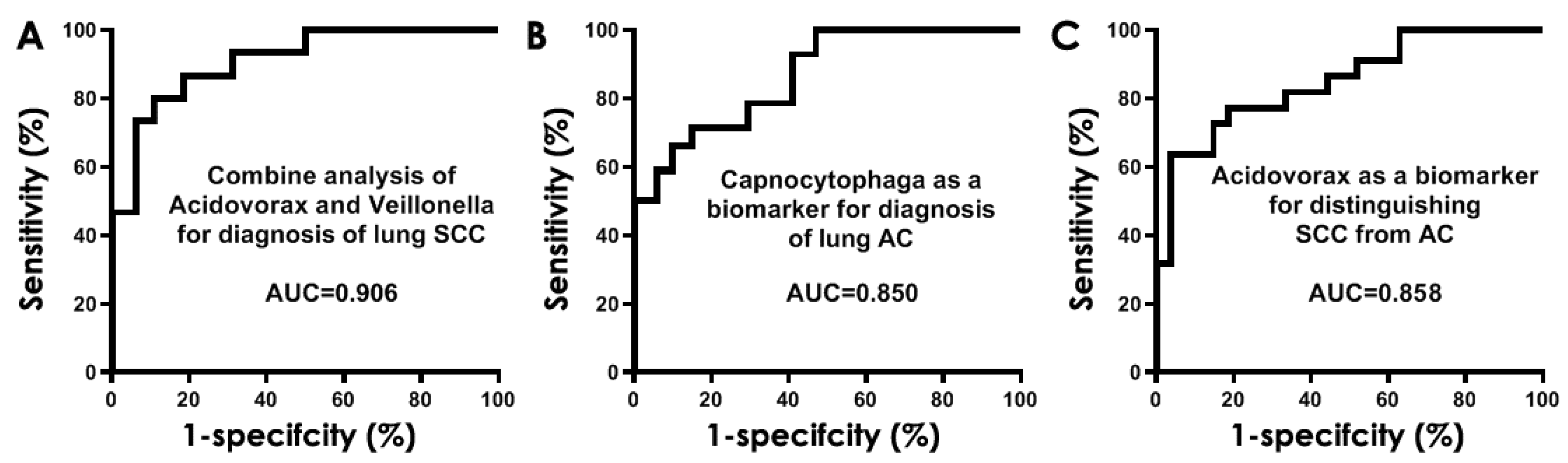
3.3. Development of Sputum Bacteria Biomarkers for NSCLC
3.4. Validating the Bacterial Biomarkers in an Independent Set of Lung Cancer Patients and Controls
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The National Lung Screening Trial Research Team. Reduced lung-cancer mortality with low-dose computed tomographic screening. N. Engl. J. Med. 2011, 365, 395–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garrett, W.S. Cancer and the microbiota. Science 2015, 348, 80–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kovaleva, O.V.; Romashin, D.; Zborovskaya, I.B.; Davydov, M.M.; Shogenov, M.S.; Gratchev, A. Human Lung Microbiome on the Way to Cancer. J. Immunol. Res. 2019, 2019, 1394191. [Google Scholar] [CrossRef]
- Mao, Q.; Jiang, F.; Yin, R.; Wang, J.; Xia, W.; Dong, G.; Ma, W.; Yang, Y.; Xu, L.; Hu, J. Interplay between the lung microbiome and lung cancer. Cancer Lett. 2018, 415, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Peters, B.A.; Hayes, R.B.; Goparaju, C.; Reid, C.; Pass, H.I.; Ahn, J. The microbiome in lung cancer tissue and recurrence-free survival. Cancer Epidemiol. Biomark. Prev. 2019, 28, 731–740. [Google Scholar] [CrossRef] [Green Version]
- Yu, G.; Gail, M.H.; Consonni, D.; Carugno, M.; Humphrys, M.; Pesatori, A.C.; Caporaso, N.E.; Goedert, J.J.; Ravel, J.; Landi, M.T. Characterizing human lung tissue microbiota and its relationship to epidemiological and clinical features. Genome Biol. 2016, 17, 163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, H.-X.; Tao, L.-L.; Zhang, J.; Zhu, Y.-G.; Zheng, Y.; Liu, D.; Zhou, M.; Ke, H.; Shi, M.-M.; Qu, J.-M. Difference of lower airway microbiome in bilateral protected specimen brush between lung cancer patients with unilateral lobar masses and control subjects. Int. J. Cancer 2018, 142, 769–778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greathouse, K.L.; White, J.R.; Vargas, A.J.; Bliskovsky, V.V.; Beck, J.A.; von Muhlinen, N.; Polley, E.C.; Bowman, E.D.; Khan, M.A.; Robles, A.I.; et al. Interaction between the microbiome and TP53 in human lung cancer. Genome Biol. 2018, 19, 123. [Google Scholar] [CrossRef]
- Apopa, P.L.; Alley, L.; Penney, R.B.; Arnaoutakis, K.; Steliga, M.A.; Jeffus, S.; Bircan, E.; Gopalan, B.; Jin, J.; Patumcharoenpol, P.; et al. PARP1 Is Up-Regulated in Non-small Cell Lung Cancer Tissues in the Presence of the Cyanobacterial Toxin Microcystin. Front. Microbiol. 2018, 9, 1757. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; O’Brien, J.L.; Ajami, N.J.; E Scheurer, M.; Amirian, E.S.; Armstrong, G.; Tsavachidis, S.; Thrift, A.P.; Jiao, L.; Wong, M.C.; et al. Lung tissue microbial profile in lung cancer is distinct from emphysema. Am. J. Cancer Res. 2018, 8, 1775–1787. [Google Scholar]
- Lee, S.H.; Sung, J.Y.; Yong, D.; Chun, J.; Kim, S.Y.; Song, J.H.; Chung, K.S.; Kim, E.Y.; Jung, J.Y.; Kang, Y.A.; et al. Characterization of microbiome in bronchoalveolar lavage fluid of patients with lung cancer comparing with benign mass like lesions. Lung Cancer 2016, 102, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Tsay, J.-C.J.; Wu, B.G.; Badri, M.H.; Clemente, J.C.; Shen, N.; Meyn, P.; Li, Y.; Yie, T.-A.; Lhakhang, T.; Olsen, E.; et al. Airway microbiota is associated with upregulation of the PI3K pathway in lung cancer. Am. J. Respir. Crit. Care Med. 2018, 198, 1188–1198. [Google Scholar] [CrossRef] [PubMed]
- Jin, J.; Gan, Y.; Liu, H.; Wang, Z.; Yuan, J.; Deng, T.; Zhou, Y.; Zhu, Y.; Zhu, H.; Yang, S.; et al. Diminishing microbiome richness and distinction in the lower respiratory tract of lung cancer pa-tients: A multiple comparative study design with independent validation. Lung Cancer 2019, 136, 129–135. [Google Scholar] [CrossRef]
- Yang, J.; Mu, X.; Wang, Y.; Zhu, D.; Zhang, J.; Liang, C.; Chen, B.; Wang, J.; Zhao, C.; Zuo, Z.; et al. Dysbiosis of the Salivary Microbiome Is Associated With Non-smoking Female Lung Cancer and Correlated With Immunocytochemistry Markers. Front. Oncol. 2018, 8, 520. [Google Scholar] [CrossRef] [PubMed]
- Yan, X.; Yang, M.; Liu, J.; Gao, R.; Hu, J.; Li, J.; Zhang, L.; Shi, Y.; Guo, H.; Cheng, J.; et al. Discovery and validation of potential bacterial biomarkers for lung cancer. Am. J. Cancer Res. 2015, 5, 3111–3122. [Google Scholar] [PubMed]
- Hosgood, H.D., 3rd; Sapkota, A.R.; Rothman, N.; Rohan, T.; Hu, W.; Xu, J.; Vermeulen, R.; He, X.; White, J.B.; Wu, G.; et al. The potential role of lung microbiota in lung cancer attributed to house-hold coal burning exposures. Environ. Mol. Mutagen. 2014, 55, 643–651. [Google Scholar] [CrossRef] [Green Version]
- Cameron, S.J.S.; Lewis, K.E.; Huws, S.A.; Hegarty, M.J.; Lewis, P.D.; Pachebat, J.A.; Mur, L.A.J. A pilot study using metagenomic sequencing of the sputum microbiome suggests potential bacterial biomarkers for lung cancer. PLoS ONE 2017, 12, e0177062. [Google Scholar] [CrossRef] [Green Version]
- Druzhinin, V.G.; Matskova, L.V.; Demenkov, P.S.; Baranova, E.D.; Volobaev, V.P.; Minina, V.I.; Apalko, S.V.; Churina, M.A.; Romanyuk, S.A.; Shcherbak, S.G.; et al. Taxonomic diversity of sputum microbiome in lung cancer patients and its relationship with chromosomal aberrations in blood lymphocytes. Sci. Rep. 2020, 10, 9681. [Google Scholar] [CrossRef]
- Cheng, C.; Wang, Z.; Wang, J.; Ding, C.; Sun, C.; Liu, P.; Xu, X.; Liu, Y.; Chen, B.; Gu, B. Characterization of the lung microbiome and exploration of potential bacterial biomarkers for lung cancer. Transl. Lung Cancer Res. 2020, 9, 693–704. [Google Scholar] [CrossRef]
- Manzoor, S.S.; Doedens, A.; Burns, M.B. The promise and challenge of cancer microbiome research. Genome Biol. 2020, 21, 131. [Google Scholar] [CrossRef]
- Gupta, C.; Su, J.; Zhan, M.; Stass, S.A.; Jiang, F. Sputum long non-coding RNA biomarkers for diagnosis of lung cancer. Cancer Biomark. 2019, 26, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Su, J.; Leng, Q.; Lin, Y.; Ma, J.; Jiang, F.; Lee, C.-J.; Fang, H.; Jiang, F. Integrating Circulating Immunological and Sputum Biomarkers for the Early Detection of Lung Cancer. Biomark. Cancer 2018, 10. [Google Scholar] [CrossRef] [PubMed]
- Su, Y.; Fang, H.; Jiang, F. Integrating DNA methylation and microRNA biomarkers in sputum for lung cancer detection. Clin. Epigenet. 2016, 8, 109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, Y.; Guarnera, M.A.; Fang, H.; Jiang, F. Small non-coding RNA biomarkers in sputum for lung cancer diagnosis. Mol. Cancer 2016, 15, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, J.; Anjuman, N.; Guarnera, M.A.; Zhang, H.; Stass, S.A.; Jiang, F. Analysis of Lung Flute-collected Sputum for Lung Cancer Diagnosis. Biomark. Insights 2015, 10, 55–61. [Google Scholar] [CrossRef]
- Su, J.; Liao, J.; Gao, L.; Shen, J.; Guarnera, M.A.; Zhan, M.; Fang, H.; Stass, S.A.; Jiang, F. Analysis of small nucleolar RNAs in sputum for lung cancer diagnosis. Oncotarget 2016, 7, 5131–5142. [Google Scholar] [CrossRef] [Green Version]
- Xing, L.; Su, J.; Guarnera, M.A.; Zhang, H.; Cai, L.; Zhou, R.; Stass, S.A.; Jiang, F. Sputum microRNA biomarkers for identifying lung cancer in indeterminate solitary pul-monary nodules. Clin. Cancer Res. 2015, 21, 484–489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, L.; Shen, J.; Mannoor, K.; Guarnera, M.; Jiang, F. Identification of ENO1 as a potential sputum biomarker for early-stage lung cancer by shotgun proteomics. Clin. Lung Cancer 2014, 15, 372–378.e1. [Google Scholar] [CrossRef] [Green Version]
- Shen, J.; Liao, J.; Guarnera, M.A.; Fang, H.; Cai, L.; Stass, S.A.; Jiang, F. Analysis of MicroRNAs in sputum to improve computed tomography for lung cancer diagnosis. J. Thorac. Oncol. 2014, 9, 33–40. [Google Scholar] [CrossRef] [Green Version]
- Li, N.; Ma, J.; Guarnera, M.A.; Fang, H.; Cai, L.; Jiang, F. Digital PCR quantification of miRNAs in sputum for diagnosis of lung cancer. J. Cancer Res. Clin. Oncol. 2013, 140, 145–150. [Google Scholar] [CrossRef] [Green Version]
- Anjuman, N.; Li, N.; Guarnera, M.; A Stass, S.; Jiang, F. Evaluation of lung flute in sputum samples for molecular analysis of lung cancer. Clin. Transl. Med. 2013, 2, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, L.; Todd, N.W.; Xing, L.; Xie, Y.; Zhang, H.; Liu, Z.; Fang, H.; Zhang, J.; Katz, R.L.; Jiang, F. Early detection of lung adenocarcinoma in sputum by a panel of microRNA markers. Int. J. Cancer 2010, 127, 2870–2878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, F.; Todd, N.W.; Li, R.; Zhang, H.; Fang, H.; Stass, S.A. A Panel of Sputum-Based Genomic Marker for Early Detection of Lung Cancer. Cancer Prev. Res. 2010, 3, 1571–1578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xing, L.; Todd, N.W.; Yu, L.; Fang, H.; Jiang, F. Early detection of squamous cell lung cancer in sputum by a panel of microRNA markers. Mod. Pathol. 2010, 23, 1157–1164. [Google Scholar] [CrossRef]
- Xie, Y.; Todd, N.W.; Liu, Z.; Zhan, M.; Fang, H.; Peng, H.; Alattar, M.; Deepak, J.; Stass, S.A.; Jiang, F. Altered miRNA expression in sputum for diagnosis of non-small cell lung cancer. Lung Cancer 2010, 67, 170–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, F.; Todd, N.W.; Qiu, Q.; Liu, Z.; Katz, R.L.; Stass, S.A. Combined genetic analysis of sputum and computed tomography for noninvasive diagnosis of non-small-cell lung cancer. Lung Cancer 2009, 66, 58–63. [Google Scholar] [CrossRef] [Green Version]
- Qiu, Q.; Todd, N.W.; Li, R.; Peng, H.; Liu, Z.; Yfantis, H.G.; Katz, R.L.; Stass, S.A.; Jiang, F. Magnetic enrichment of bronchial epithelial cells from sputum for lung cancer diagnosis. Cancer 2008, 114, 275–283. [Google Scholar] [CrossRef]
- Li, R.; Todd, N.W.; Qiu, Q.; Fan, T.; Zhao, R.Y.; Rodgers, W.H.; Fang, H.-B.; Katz, R.L.; Stass, S.A.; Jiang, F. Genetic Deletions in Sputum as Diagnostic Markers for Early Detection of Stage I Non–Small Cell Lung Cancer. Clin. Cancer Res. 2007, 13, 482–487. [Google Scholar] [CrossRef] [Green Version]
- Liao, J.; Shen, J.; Leng, Q.; Qin, M.; Zhan, M.; Jiang, F. MicroRNA-based biomarkers for diagnosis of non-small cell lung cancer (NSCLC). Thorac. Cancer 2020, 11, 762–768. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Jiang, Z.; Leng, Q.; Bai, F.; Wang, J.; Ding, X.; Li, Y.; Zhang, X.; Fang, H.; Yfantis, H.G.; et al. A prediction model for distinguishing lung squamous cell carcinoma from adenocarcinoma. Oncotarget 2017, 8, 50704–50714. [Google Scholar] [CrossRef] [Green Version]
- Bingula, R.; Filaire, M.; Radosevic-Robin, N.; Berthon, J.Y.; Bernalier-Donadille, A.; Vasson, M.P.; Thivat, E.; Kwiatkowski, F.; Filaire, E. Characterisation of gut, lung, and upper airways microbiota in patients with non-small cell lung carcinoma: Study protocol for case-control observational trial. Medicine 2018, 97, e13676. [Google Scholar] [CrossRef] [PubMed]
- Goto, T. Airway Microbiota as a Modulator of Lung Cancer. Int. J. Mol. Sci. 2020, 21, 3044. [Google Scholar] [CrossRef] [PubMed]
- Romeo, M.S.; Sokolova, I.A.; Morrison, L.E.; Zeng, C.; Barón, A.E.; Hirsch, F.R.; Miller, Y.E.; Franklin, W.A.; Varella-Garcia, M. Chromosomal abnormalities in non-small cell lung carcinomas and in bron-chial epithelia of high-risk smokers detected by multi-target interphase fluorescence in situ hybridization. J. Mol. Diagn. 2003, 5, 103–112. [Google Scholar] [CrossRef] [Green Version]
- Varella-Garcia, M.; Kittelson, J.; Schulte, A.P.; Vu, K.O.; Wolf, H.J.; Zeng, C.; Hirsch, F.R.; Byers, T.; Kennedy, T.; Miller, Y.E.; et al. Multi-target interphase fluorescence in situ hybridization assay increases sensitivity of sputum cytology as a predictor of lung cancer. Cancer Detect. Prev. 2004, 28, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Katz, R.L.; Zaidi, T.M.; Fernandez, R.L.; Zhang, J.; He, W.; Acosta, C.; Daniely, M.; Madi, L.; A Vargas, M.; Dong, Q.; et al. Automated detection of genetic abnormalities combined with cytology in sputum is a sensitive predictor of lung cancer. Mod. Pathol. 2008, 21, 950–960. [Google Scholar] [CrossRef] [Green Version]
- Su, Y.; Bin Fang, H.; Jiang, F. An epigenetic classifier for early stage lung cancer. Clin. Epigenet. 2018, 10, 68. [Google Scholar] [CrossRef] [Green Version]
- Jiang, F.; Qiu, Q.; Khanna, A.; Todd, N.W.; Deepak, J.; Xing, L.; Wang, H.; Liu, Z.; Su, Y.; Stass, S.A.; et al. Aldehyde Dehydrogenase 1 Is a Tumor Stem Cell-Associated Marker in Lung Cancer. Mol. Cancer Res. 2009, 7, 330–338. [Google Scholar] [CrossRef] [Green Version]
- Ma, J.; Li, N.; Guarnera, M.; Jiang, F. Quantification of Plasma miRNAs by Digital PCR for Cancer Diagnosis. Biomark. Insights 2013, 8, 127–136. [Google Scholar] [CrossRef] [Green Version]
- Ma, J.; Mannoor, K.; Gao, L.; Tan, A.; Guarnera, M.A.; Zhan, M.; Shetty, A.; Stass, S.A.; Xing, L.; Jiang, F. Characterization of microRNA transcriptome in lung cancer by next-generation deep sequencing. Mol. Oncol. 2014, 8, 1208–1219. [Google Scholar] [CrossRef]
- Lin, Y.; Holden, V.; Dhilipkannah, P.; Deepak, J.; Todd, N.W.; Jiang, F. A Non-Coding RNA Landscape of Bronchial Epitheliums of Lung Cancer Patients. Biomedicines 2020, 8, 88. [Google Scholar] [CrossRef]
- Lin, Y.; Leng, Q.; Zhan, M.; Jiang, F. A Plasma Long Noncoding RNA Signature for Early Detection of Lung Cancer. Transl. Oncol. 2018, 11, 1225–1231. [Google Scholar] [CrossRef] [PubMed]
- Leng, Q.; Tsou, J.-H.; Zhan, M.; Jiang, F. Fucosylation genes as circulating biomarkers for lung cancer. J. Cancer Res. Clin. Oncol. 2018, 144, 2109–2115. [Google Scholar] [CrossRef] [PubMed]
- Sambo, F.; Finotello, F.; Lavezzo, E.; Baruzzo, G.; Masi, G.; Peta, E.; Falda, M.; Toppo, S.; Barzon, L.; Di Camillo, B. Optimizing PCR primers targeting the bacterial 16S ribosomal RNA gene. BMC Bioinform. 2018, 19, 343. [Google Scholar] [CrossRef]
- Zhi, X.Y.; Tang, S.K.; Li, W.J.; Xu, L.H.; Jiang, C.L. New genus-specific primers for the PCR identification of novel isolates of the genus Strep-tomonospora. FEMS Microbiol. Lett. 2006, 263, 48–53. [Google Scholar] [CrossRef] [Green Version]
- Zheng, Y.; Fang, Z.; Xue, Y.; Zhang, J.; Zhu, J.; Gao, R.; Yao, S.; Ye, Y.; Wang, S.; Lin, C.; et al. Specific gut microbiome signature predicts the early-stage lung cancer. Gut Microbes 2020, 11, 1030–1042. [Google Scholar] [CrossRef]
- Katayama, Y.; Yamada, T.; Shimamoto, T.; Iwasaku, M.; Kaneko, Y.; Uchino, J.; Takayama, K. The role of the gut microbiome on the efficacy of immune checkpoint inhibitors in Japanese responder patients with advanced non-small cell lung cancer. Transl. Lung Cancer Res. 2019, 8, 847–853. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.; Su, X.; Yuan, M.; Zhang, S.; He, J.; Deng, Q.; Qiu, W.; Dong, H.; Cai, S. The characterization of lung microbiome in lung cancer patients with different clinicopathology. Am. J. Cancer Res. 2019, 9, 2047–2063. [Google Scholar] [PubMed]
- Bingula, R.; Filaire, E.; Molnar, I.; Delmas, E.; Berthon, J.-Y.; Vasson, M.-P.; Bernalier-Donadille, A.; Filaire, M. Characterisation of microbiota in saliva, bronchoalveolar lavage fluid, non-malignant, peritumoural and tumour tissue in non-small cell lung cancer patients: A cross-sectional clinical trial. Respir. Res. 2020, 21, 129. [Google Scholar] [CrossRef] [PubMed]
- Demirci, M.; Tokman, H.; Uysal, H.; Demiryas, S.; Karakullukcu, A.; Saribas, S.; Cokugras, H.; Kocazeybek, B. Reduced Akkermansia muciniphila and Faecalibacterium prausnitzii levels in the gut microbiota of children with allergic asthma. Allergol. Immunopathol. 2019, 47, 365–371. [Google Scholar] [CrossRef]
- Abed, J.; Maalouf, N.; Parhi, L.; Chaushu, S.; Mandelboim, O.; Bachrach, G. Tumor Targeting by Fusobacterium nucleatum: A Pilot Study and Future Perspectives. Front. Cell. Infect. Microbiol. 2017, 7, 295. [Google Scholar] [CrossRef] [Green Version]
- Wypych, T.P.; Wickramasinghe, L.C.; Marsland, B.J. The influence of the microbiome on respiratory health. Nat. Immunol. 2019, 20, 1279–1290. [Google Scholar] [CrossRef]
- Mounika, P. Helicobacter pylori Infection and Risk of Lung Cancer: A Meta-Analysis. Lung Cancer Int. 2013, 2013, 131869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ding, L.; Yang, Z.; Lu, J.; Ma, L.; Liu, Y.; Wu, X.; Yao, W.; Zhang, X.; Zhu, K. Characterization of Phenotypic and Genotypic Traits of Klebsiella pneumoniae from Lung Cancer Patients with Respiratory Infection. Infect. Drug Resist. 2020, 13, 237–245. [Google Scholar] [CrossRef] [Green Version]
- Jin, C.; Lagoudas, G.K.; Zhao, C.; Bullman, S.; Bhutkar, A.; Hu, B.; Ameh, S.; Sandel, D.; Liang, X.S.; Mazzilli, S.; et al. Commensal Microbiota Promote Lung Cancer Development via gammadelta T Cells. Cell 2019, 176, 998–1013.e16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tamura, A.; Hebisawa, A.; Kusaka, K.; Hirose, T.; Suzuki, J.; Yamane, A.; Nagai, H.; Fukami, T.; Ohta, K.; Takahashi, F. Relationship Between Lung Cancer and Mycobacterium Avium Complex Isolated Using Bronchoscopy. Open Respir. Med. J. 2016, 10, 20–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García-Núñez, M.; Millares, L.; Pomares, X.; Ferrari, R.; Pérez-Brocal, V.; Gallego, M.; Espasa, M.; Moya, A.; Monsó, E. Severity-related changes of bronchial microbiome in chronic obstructive pulmonary disease. J. Clin. Microbiol. 2014, 52, 4217–4223. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Z.; Fei, K.; Bai, H.; Wang, Z.; Duan, J.; Wang, J. Metagenome association study of the gut microbiome revealed biomarkers linked to chemo-therapy outcomes in locally advanced and advanced lung cancer. Thorac. Cancer 2021, 12, 66–78. [Google Scholar] [CrossRef] [PubMed]
- Gomes, S.; Cavadas, B.; Ferreira, J.C.; Marques, P.I.; Monteiro, C.; Sucena, M.; Sousa, C.; Rodrigues, L.V.; Teixeira, G.; Pinto, P.; et al. Profiling of lung microbiota discloses differences in adenocarcinoma and squamous cell carcinoma. Sci. Rep. 2019, 9, 12838. [Google Scholar] [CrossRef] [Green Version]
- Liu, N.-N.; Ma, Q.; Ge, Y.; Yi, C.-X.; Wei, L.-Q.; Tan, J.-C.; Chu, Q.; Li, J.-Q.; Zhang, P.; Wang, H. Microbiome dysbiosis in lung cancer: From composition to therapy. NPJ Precis. Oncol. 2020, 4, 33. [Google Scholar] [CrossRef] [PubMed]
- Mansour, B.; Monyók, Á.; Makra, N.; Gajdács, M.; Vadnay, I.; Ligeti, B.; Juhász, J.; Szabó, D.; Ostorházi, E. Bladder cancer-related microbiota: Examining differences in urine and tissue sam-ples. Sci. Rep. 2020, 10, 11042. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| NSCLC Cases (n = 17) | Controls (n = 10) | p-Value | |
|---|---|---|---|
| Age | 66.37 (SD 9.05) | 61.27 (SD 9.46) | 0.36 |
| Sex | 0.43 | ||
| Female | 7 | 4 | |
| Male | 10 | 6 | |
| Race | 0.39 | ||
| African Americans | 5 | 3 | |
| White American | 12 | 7 | |
| Smoking pack-years (median) | 32.17 | 28.38 | 0.26 |
| Stage | |||
| Stage I | 5 | ||
| Stage II | 5 | ||
| Stage III-VI | 7 | ||
| Histological type | |||
| Adenocarcinoma | 10 | ||
| Squamous cell carcinoma | 7 | ||
| Location of primary lung tumors | |||
| Peripheral location | 10 | ||
| Central location | 7 |
| NSCLC Cases (n = 69) | Controls (n = 79) | p-Value | |
|---|---|---|---|
| Age | 64.18 (SD 6.25) | 63.29 (SD 6.24) | 0.32 |
| Sex | 0.35 | ||
| Female | 26 | 30 | |
| Male | 43 | 49 | |
| Smoking pack-years (median) | 35.25 | 33.29 | 0.41 |
| Stage | |||
| Stage I | 22 | ||
| Stage II | 24 | ||
| Stage III–VI | 23 | ||
| Histological type | |||
| Adenocarcinoma | 36 | ||
| Squamous cell carcinoma | 33 | ||
| Location of primary lung tumors | |||
| Peripheral location | 36 | ||
| Central location | 33 |
| Name | Target Region (Accession #) | Forward (5′-3′) | Reward (5′-3′) | References |
|---|---|---|---|---|
| Acidovorax | NZ_LJGO01000014.1 | GTCATCCTCCACCAACCAATAC | GTCTATACCGGACCAACAACAA | [8] |
| Akkermansia | NZ_AP021898.1 | CAGCACGTGAAGGTGGGGAC | CCTTGCGGTTGGCTTCAGAT | [55] |
| Bacteroides | NZ_VKLY01000054.1 | GACCGCATGGTCTTGTTATT | CGTAGGAGTTTGGACCGTGT | [56] |
| Bifidobacterium | NZ_AKCA01000001.1 | CCACATGATCGCATGTGATTG | CCGAAGGCTTGCTCCCAAA | [56] |
| Bilophila | NZ_KE150238.1 | CGTGTGAATAATGCGAGGG | TCTCCGGTACTCAAGCGTG | [57] |
| Blautia | NZ_NQOF01000001.1 | GTGAAGGAAGAAGTATCTCGG | TTGGTAAGGTTCTTCGCGTT | [58] |
| Bradyrhizobium | NZ_VSSR01000023.1 | ATCGACGTGCTGCCAATAA | GCCGATAACAAGACGGAAATAAC | [13] |
| Capnocytophaga | NZ_BLBC01000010.1 | TGGWCAATGGTCGGAAGACTG | CCGCTACACTACACATTCCA | [9] |
| Curvibacter | NZ_CP022389.1 | GAGCCTTTACCTCACCAACTAC | CGTAGCGAAAGCTACGCTAATA | [59] |
| Enterococcus | NZ_CP023011.2 | GGCATATTTATCCAGCACTAG | TAGCGTACGAAAAGGCATCC | [17] |
| Escherichia | NC_000913.3 | CATGCCGCGTGTATGAAGAA | CGGGTAACGTCAATGAGCAAA | [17] |
| Faecalibacterium | NZ_CP030777.1 | GGAGGAAGAAGGTCTTCGG | AATTCCGCCTACCTCTGCACT | [60] |
| Fusobacterium | NZ_LT608325.1 | AAGCGCGTCTAGGTGGTTATGT | TGTAGTTCCGCTTACCTCTCCAG | [61] |
| Haemophilus | NZ_LS483458.1 | AGCGGCTTGTAGTTCCTCTAACA | CAACAGAGTATCCGCCAAAAGTT | [62] |
| Helicobacter | NC_017379.1 | GCGCATGTCTTCGGTTAAAAA | TTCCATAGGCTATAATGTGATCCAAA | [63] |
| Klebsiella | NZ_CP023478.1 | CGGGCGTAGCGCGTAA | GATACCCGCATTCACATTAAACAG | [64] |
| Lactobacillus | NZ_MWIK01000038.1 | CGCCACTGGTGTTCYTCCATATA | AGCAGTAGGGAATCTTCCA | [65] |
| Mycobacterium | NZ_UATA01000019.1 | CAAGCGGTGGAGCATGTG | CTAAGATGTCAAACGCTGGTAAGG | [66] |
| Neisseria | NZ_UGRT01000005.1 | CTGTTGGGCARCWTGAYTGC | GATCGGTTTTRTGAGATTGG | [7] |
| Prevotella | NZ_BAKG01000039.1 | CCTACGATGGATAGGGGTT | CACGCTACTTGGCTGGTTCAG | [5] |
| Pseudomonas | NZ_BMDE01000022.1 | CAGCCATGCCGCGTGTGTGA | GTTGGTAACGTCAAAACAGCAAGG | [67] |
| Ruminococcus | NZ_QRIH01000002.1 | GCTTAGATTCTTCGGATGAAGAGGA | AGTTTTTACCCCCGCACCA | [68] |
| Selenomonas | NZ_JH376859.1 | ACRCGTAGRCAACCTGCCG | CGATCCGAAGACCTTCTTCAC | [15] |
| Streptococcus | NZ_UYIP01000002.1 | ACGCAATCTAGCAGATGAAGCA | TCGTGCGTTTTAATTCCAGC | [7,16] |
| Veillonella | NZ_AUAN01000022.1 | CGGGTGAGTAACGCGTAATCA | CCAACTAGCTGATGGGACGC | [15] |
| Genera | p Value of Ac Patients vs. Controls | p Value of Scc Patients vs. Controls | AUC of AC Patients vs. Controls | AUC of SCC Patients vs. Controls |
|---|---|---|---|---|
| Acidovorax | 0.7090 | 0.0015 | 0.5636 | 0.8814 |
| Capnocytophaga | 0.0455 | 0.3194 | 0.8502 | 0.6833 |
| Helicobacter | 0.0705 | 0.0175 | 0.7273 | 0.8070 |
| Streptococcus | 0.2775 | 0.0042 | 0.6753 | 0.8117 |
| Veillonella | 0.1086 | 0.0098 | 0.7062 | 0.8286 |
| Cohort 1 of 17 NSCLC Patients and 10 Cancer-Free Controls | Cohort 2 of 69 NSCLC Patients and 79 Cancer-Free Controls | |||
|---|---|---|---|---|
| Sensitivity | Specificity | Sensitivity | Specificity | |
| Combined Acidovorax and Veillonella for SCC | 80.79% | 89.08% | 75.76% | 88.61% |
| Capnocytophaga for AC | 72.70% | 85.28% | 69.44% | 84.42% |
| Acidovorax for distinguishing SCC from AC | 63.64% | 96.30% | 66.67% | 89.86% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leng, Q.; Holden, V.K.; Deepak, J.; Todd, N.W.; Jiang, F. Microbiota Biomarkers for Lung Cancer. Diagnostics 2021, 11, 407. https://doi.org/10.3390/diagnostics11030407
Leng Q, Holden VK, Deepak J, Todd NW, Jiang F. Microbiota Biomarkers for Lung Cancer. Diagnostics. 2021; 11(3):407. https://doi.org/10.3390/diagnostics11030407
Chicago/Turabian StyleLeng, Qixin, Van K. Holden, Janaki Deepak, Nevins W. Todd, and Feng Jiang. 2021. "Microbiota Biomarkers for Lung Cancer" Diagnostics 11, no. 3: 407. https://doi.org/10.3390/diagnostics11030407