
Dendritic Cells Are Associated with Prognosis and Survival in Breast Cancer

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Description of Study Group
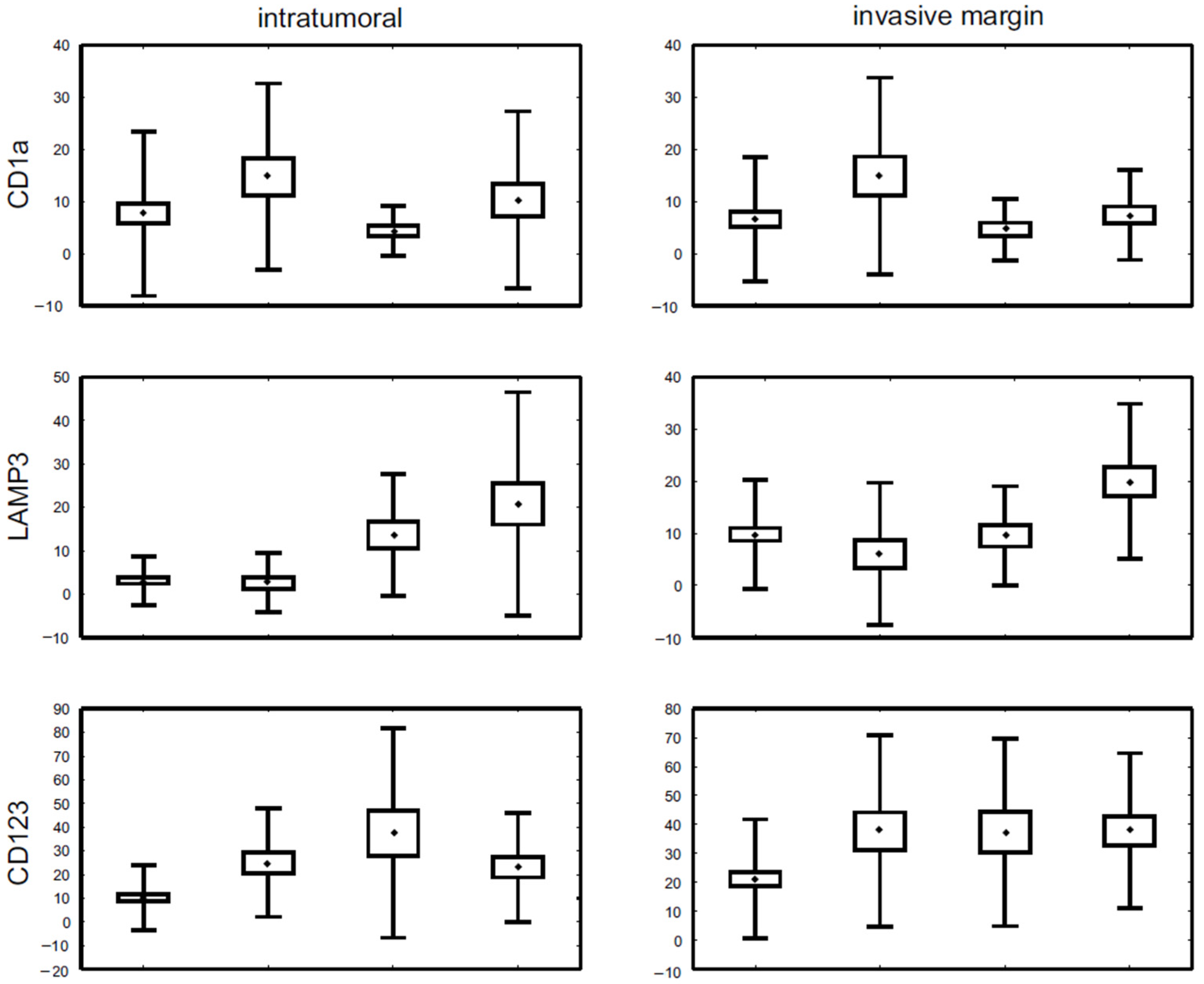
3.2. DC Subpopulations in Molecular Cancer Subtypes
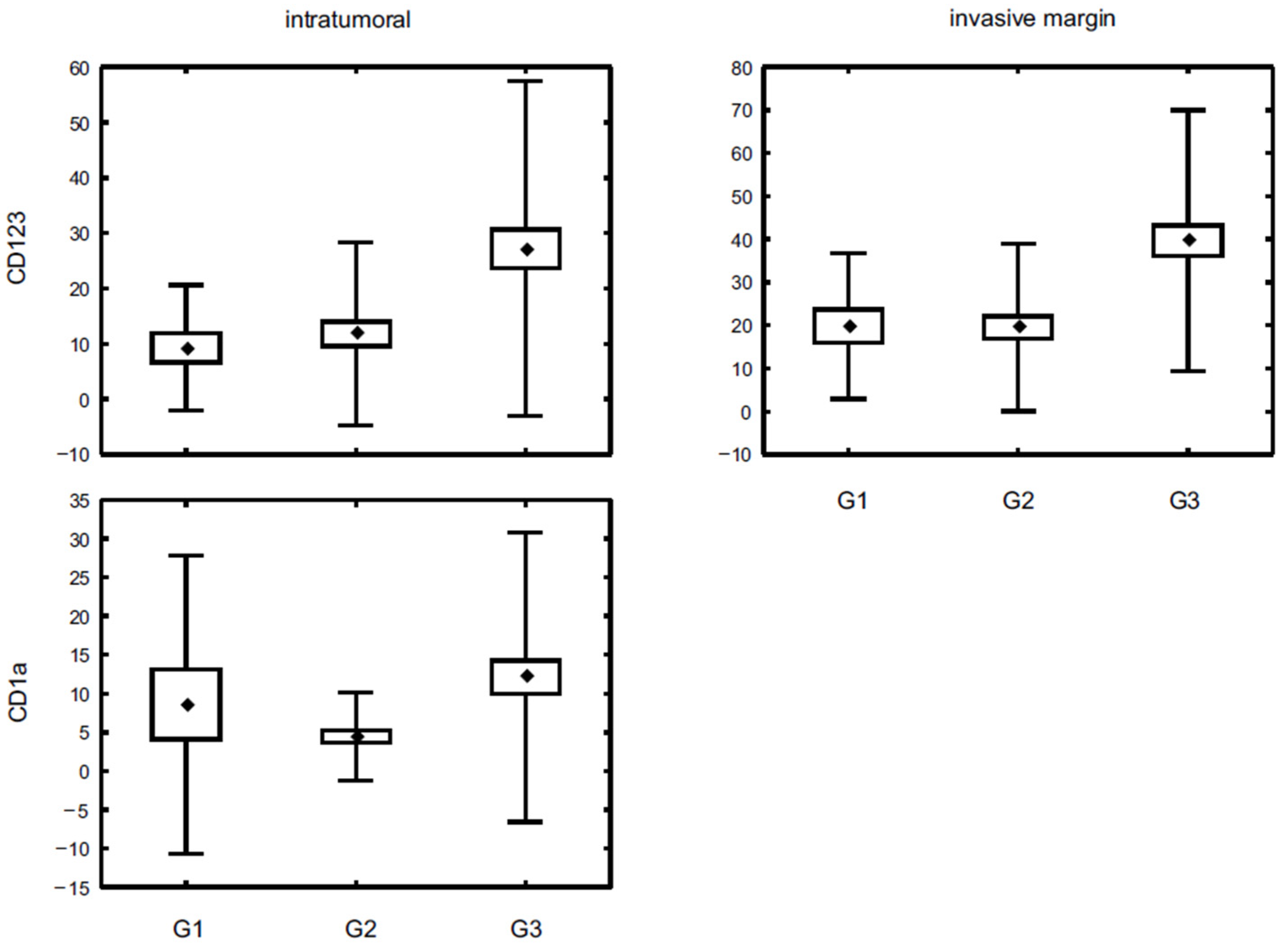
3.3. DC Subpopulations and Other Pathological Prognostic Factors
3.4. Survival Analysis
3.5. DC Subpopulation Distribution
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gelao, L.; Criscitiello, C.; Esposito, A.; De Laurentiis, M.; Fumagalli, L.; Locatelli, M.A.; Minchella, I.; Santangelo, M.; De Placido, S.; Goldhirsch, A.; et al. Dendritic cell-based vaccines: Clinical applications in breast cancer. Immunotherapy 2014, 6, 349–360. [Google Scholar] [CrossRef] [PubMed]
- Bell, D.; Chomarat, P.; Broyles, D.; Netto, G.; Harb, G.M.; Lebecque, S.; Valladeau, J.; Davoust, J.; Palucka, K.A.; Banchereau, J. In Breast Carcinoma Tissue, Immature Dendritic Cells Reside within the Tumor, Whereas Mature Dendritic Cells Are Located in Peritumoral Areas. J. Exp. Med. 1999, 190, 1417–1426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De la Cruz-Merino, L.; Barco-Sánchez, A.; Henao Carrasco, F.; Nogales Fernández, E.; Vallejo Benítez, A.; Brugal Molina, J.; Martínez Peinado, A.; Grueso López, A.; Ruiz Borrego, M.; de Villena, M.C.M.; et al. New insights into the role of the immune microenviron-ment in breast carcinoma. Clin. Dev. Immunol. 2013, 2013, 785317. [Google Scholar] [CrossRef] [PubMed]
- Talmadge, J.E.; Donkor, M.; Scholar, E. Inflammatory cell infiltration of tumors: Jekyll or Hyde. Cancer Metastasis Rev. 2007, 26, 373–400. [Google Scholar] [CrossRef] [PubMed]
- Karthaus, N.; Torensma, R.; Tel, J. Deciphering the Message Broadcast by Tumor-Infiltrating Dendritic Cells. Am. J. Pathol. 2012, 181, 733–742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reichert, T.E.; Scheuer, C.; Day, R.; Wagner, W.; Whiteside, T.L. The number of intratumoral dendritic cells and zeta-chain expression in T cells as prognostic and survival biomarkers in patients with oral carcinoma. Cancer 2001, 91, 2136–2147. [Google Scholar] [CrossRef]
- Goldman, S.A.; Baker, E.; Weyant, R.J.; Clarke, M.R.; Myers, J.N.; Lotze, M.T. Peritumoral CD1a-positive dendritic cells are associated with improved survival in patients with tongue carcinoma. Arch. Otolaryngol. Head Neck Surg. 1998, 124, 641–646. [Google Scholar] [CrossRef] [Green Version]
- La Rocca, G.; Anzalone, R.; Corrao, S.; Magno, F.; Rappa, F.; Marasà, S.; Czarnecka, A.M.; Marasà, L.; Sergi, C.; Zummo, G.; et al. CD1a down-regulation in primary invasive ductal breast carcinoma may predict regional lymph node invasion and patient outcome. Histopathology 2007, 52, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Hillenbrand, E.E.; Neville, A.M.; Coventry, B.J. Immunohistochemical localization of CD1a-positive putative dendritic cells in human breast tumours. Br. J. Cancer 1999, 79, 940–944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Treilleux, I.; Blay, J.-Y.; Bendriss-Vermare, N.; Ray-Coquard, I.; Bachelot, T.; Guastalla, J.-P.; Bremond, A.; Goddard, S.; Pin, J.-J.; Barthelemy-Dubois, C.; et al. Dendritic Cell Infiltration and Prognosis of Early Stage Breast Cancer. Clin. Cancer Res. 2004, 10, 7466–7474. [Google Scholar] [CrossRef] [Green Version]
- Sisirak, V.; Faget, J.; Gobert, M.; Goutagny, N.; Vey, N.; Treilleux, I.; Renaudineau, S.; Poyet, G.; Labidi-Galy, I.; Goddard-Leon, S.; et al. Impaired IFN-α production by plasmacytoid dendritic cells favors regulatory T-cell ex-pansion that may contribute to breast cancer progression. Cancer Res. 2012, 72, 5188–5197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takagi, S.; Miyagawa, S.; Ichikawa, E.; Soeda, J.; Miwa, S.; Miyagawa, Y.; Iijima, S.; Noike, T.; Kobayashi, A.; Kawasaki, S. Dendritic cells, T-cell infiltration, and Grp94 expression in cholangiocellular car-cinoma. Hum. Pathol. 2004, 35, 881–886. [Google Scholar] [CrossRef]
- Miyagawa, S.; Soeda, J.; Takagi, S.; Miwa, S.; Ichikawa, E.; Noike, T. Prognostic significance of mature dendritic cells and factors associated with their accumulation in metastatic liver tumors from colorectal cancer. Hum. Pathol. 2004, 35, 1392–1396. [Google Scholar] [CrossRef] [PubMed]
- La Torre, D.; Lernmark, A. Immunology of beta-cell destruction. Adv. Exp. Med. Biol. 2010, 654, 537–583. [Google Scholar]
- Coventry, B.; Heinzel, S. CD1a in human cancers: A new role for an old molecule. Trends Immunol. 2004, 25, 242–248. [Google Scholar] [CrossRef]
- Palucka, K.; Banchereau, J. Cancer immunotherapy via dendritic cells. Nat. Rev. Cancer. 2012, 12, 265–277. [Google Scholar] [CrossRef] [PubMed]
- Geijtenbeek, T.B.; Engering, A.; Van Kooyk, Y. DC-SIGN, a C-type lectin on dendritic cells that unveils many aspects of den-dritic cell biology. J. Leukoc. Biol. 2002, 71, 921–931. [Google Scholar] [PubMed]
- Byrd, D.R.; Carducci, M.A.; Compton, C.C.; Fritz, A.G.; Greene, F.L. AJCC Cancer Staging Manual, 8th ed.; Springer: Cham, Switzerland, 2017. [Google Scholar]
- Glajcar, A.; Szpor, J.; Pacek, A.; Tyrak, K.E.; Chan, F.; Streb, J.; Hodorowicz-Zaniewska, D.; Okoń, K. The relationship between breast cancer molecular subtypes and mast cell populations in tumor microenvironment. Virchows Archiv. 2017, 470, 505–515. [Google Scholar] [CrossRef] [Green Version]
- Wolff, A.C.; Hammond, M.E.H.; Hicks, D.G.; Dowsett, M.; McShane, L.M.; Allison, K.H.; Allred, D.C.; Bartlett, J.M.S.; Bilous, M.; Fitzgibbons, P.; et al. Recommendations for Human Epidermal Growth Factor Receptor 2 Test-ing in Breast Cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline Update. J. Clin. Oncol. 2013, 31, 3997–4013. [Google Scholar] [CrossRef]
- Goldhirsch, A.; Winer, E.P.; Coates, A.S.; Gelber, R.D.; Piccart-Gebhart, M.; Thürlimann, B.; Senn, H.-J.; Albain, K.S.; André, F.; Bergh, J.; et al. Personalizing the treatment of women with early breast cancer: Highlights of the St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2013. Ann. Oncol. 2013, 24, 2206–2223. [Google Scholar] [CrossRef]
- Gnant, M.; Thomssen, C.; Harbeck, N. St. Gallen/Vienna 2015: A Brief Summary of the Consensus Discussion. Breast Care 2015, 10, 124–130. [Google Scholar] [CrossRef] [Green Version]
- Wculek, S.K.; Cueto, F.J.; Mujal, A.M.; Melero, I.; Krummel, M.F.; Sancho, D. Dendritic cells in cancer immunology and immunotherapy. Nat. Rev. Immunol. 2020, 20, 7–24. [Google Scholar] [CrossRef]
- Coventry, B.J.; Morton, J. CD1a-positive infiltrating-dendritic cell density and 5-year survival from human breast cancer. Br. J. Cancer 2003, 89, 533–538. [Google Scholar] [CrossRef] [Green Version]
- Tsujitani, S.; Furukawa, T.; Tamada, R.; Okamura, T.; Yasumoto, K.; Sugimachi, K. Langerhans cells and prognosis in patients with gastric carcinoma. Cancer 1987, 59, 501–505. [Google Scholar] [CrossRef]
- Ambe, K.; Mori, M.; Enjoji, M. S-100 protein-positive dendritic cells in colorectal adenocarcinomas: Distribution and relation to clinical progress. Cancer 1989, 63, 496–503. [Google Scholar] [CrossRef]
- Gallo, O.; Bianchi, S.; Giannini, A.; Gallina, E.; Libonati, G.A.; Fini-Storchi, O. Correlations Between Histopathological and Biological Findings in Nasopharyngeal Carcinoma and Its Prognostic Significance. Laryngoscope 1991, 101, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Zeid, N.A.; Muller, H.K. S-100 positive dendritic cells in human lung tumours associated with cell differentiation and enhanced survival. Pathology 1993, 25, 338–343. [Google Scholar] [CrossRef] [PubMed]
- Iwamoto, M.; Shinohara, H.; Miyamoto, A.; Okuzawa, M.; Mabuchi, H.; Nohara, T.; Gon, G.; Toyoda, M.; Tanigawa, N. Prognostic value of tumor-infiltrating dendritic cells expressing CD83 in human breast carcinomas. Int. J. Cancer 2003, 104, 92–97. [Google Scholar] [CrossRef] [PubMed]
- Perou, C.M.; Sørlie, T.; Eisen, M.B.; Van De Rijn, M.; Jeffrey, S.S.; Rees, C.A.; Pollack, J.R.; Ross, D.T.; Johnsen, H.; Akslen, L.A.; et al. Molecular portraits of human breast tumours. Nature 2000, 406, 747–752. [Google Scholar] [CrossRef]
- Rakha, E.A.; El-Sayed, M.E.; Green, A.R.; Lee, A.H.S.; Robertson, J.F.; Ellis, I.O. Prognostic markers in triple-negative breast cancer. Cancer 2006, 109, 25–32. [Google Scholar] [CrossRef]
- Rakha, E.A.; Elsheikh, S.E.; Aleskandarany, M.A.; Habashi, H.O.; Green, A.R.; Powe, D.G.; El-Sayed, M.E.; Benhasouna, A.; Brunet, J.-S.; Akslen, L.A.; et al. Triple-Negative Breast Cancer: Distinguishing between Basal and Nonbasal Subtypes. Clin. Cancer Res. 2009, 15, 2302–2310. [Google Scholar] [CrossRef] [Green Version]
- Gadalla, R.; Hassan, H.; Ibrahim, S.A.; Abdullah, M.S.; Gaballah, A.; Greve, B.; El-Deeb, S.; El-Shinawi, M.; Mohamed, M.M. Tumor microenvironmental plasmacytoid dendritic cells contribute to breast cancer lymph node metastasis via CXCR4/SDF-1 axis. Breast Cancer Res. Treat. 2019, 174, 679–691. [Google Scholar] [CrossRef] [PubMed]
- Nagelkerke, A.; Sieuwerts, A.; Bussink, J.; Sweep, F.; Look, M.; Foekens, J.; Martens, J.; Span, P. LAMP3 is involved in tamoxifen resistance in breast cancer cells through the modulation of autophagy. Endocr. Relat. Cancer 2014, 21, 101–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Le Mercier, I.; Poujol, D.; Sanlaville, A.; Sisirak, V.; Gobert, M.; Durand, I.; Dubois, B.; Treilleux, I.; Marvel, J.; Vlach, J.; et al. Tumor Promotion by Intratumoral Plasmacytoid Dendritic Cells Is Reversed by TLR7 Ligand Treatment. Cancer Res. 2013, 73, 4629–4640. [Google Scholar] [CrossRef] [Green Version]
- Miserocchi, G.; Mercatali, L.; Liverani, C.; De Vita, A.; Spadazzi, C.; Pieri, F.; Bongiovanni, A.; Recine, F.; Amadori, D.; Ibrahim, T. Management and potentialities of primary cancer cultures in preclinical and translational studies. J. Transl. Med. 2017, 15, 229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hudson, E.A.; Fox, L.H.; Luckett, J.C.A.; Manson, M.M. Ex vivo cancer chemoprevention research possibilities. Environ. Toxi-col. Pharmacol. 2006, 21, 204–214. [Google Scholar] [CrossRef] [PubMed]
- Satthaporn, S.; Robins, A.; Vassanasiri, W.; El-Sheemy, M.; Jibril, J.; Clark, D.; Valerio, D.; Eremin, O. Dendritic cells are dysfunctional in patients with operable breast cancer. Cancer Immunol. Immunother. 2004, 53, 510–518. [Google Scholar] [CrossRef]
- Steinman, R.M. Decisions about Dendritic Cells: Past, Present, and Future. Annu. Rev. Immunol. 2012, 30, 1–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheever, M.A.; Higano, C.S. PROVENGE (Sipuleucel-T) in prostate cancer: The first FDA-approved therapeutic cancer vaccine. Clin. Cancer Res. 2011, 1, 3520–3526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bates, J.; Derakhshandeh, R.; Jones, L.; Webb, T.J. Mechanisms of immune evasion in breast cancer. BMC Cancer 2018, 18, 556. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Primary Antibody | Clone | Dilution | Antigen Retrieval | Incubation Time | Producer |
|---|---|---|---|---|---|
| CD1a | MTB1 | 1:10 | Citrate | Overnight | Novocastra (Leica Biosystems, Nußloch, Germany) |
| CD123 | BR4MS | 1:100 | Ethylenediaminetetraacetic Acid Disodium (EDTA) | 30 min | Novocastra (Leica Biosystems, Nußloch, Germany) |
| CD83 | 1H4b | 1:50 | Citrate | 30 min | Abcam, Cambridge, UK |
| DC-LAMP3 | Rabbit polyclonal | 1:50 | EDTA | 60 min | Abcam, Cambridge, UK |
| DC-SIGN | 5D7 | 1:50 | EDTA | 30 min | Abcam, Cambridge, UK |
| Estrogen receptor | 6F11 | 1:25 | Citrate | 60 min | Novocastra (Leica Biosystems, Nußloch, Germany) |
| Progesterone receptor | PgR636 | 1:50 | Citrate | 60 min | Dako, Santa Clara, CA, USA |
| Ki67 | MIB-1 | 1:100 | EDTA | 60 min | Dako, Santa Clara, CA, USA |
| Characteristic | Number of Cases | % |
|---|---|---|
| Age Mean: 54.9 Range: 29–87 | ||
| Stage | ||
| I | 51 | 33.5 |
| II | 58 | 38.2 |
| III | 40 | 26.3 |
| IV | 1 | 0.7 |
| Unknown | 2 | 1.3 |
| Tumour size | ||
| pT1 | 77 | 50.7 |
| pT2 | 70 | 46.0 |
| pT3 | 5 | 3.3 |
| Lymph node status | ||
| pN0 | 69 | 45.4 |
| pN1 | 41 | 27.0 |
| pN2 | 21 | 13.8 |
| pN3 | 18 | 11.8 |
| Unknown | 3 | 2.0 |
| Histological type | ||
| Invasive carcinoma of no special type | 133 | 87.5 |
| Invasive lobular carcinoma | 17 | 11.2 |
| Other | 2 | 1.3 |
| Nottingham Histologic Grade | ||
| G1 | 19 | 12.5 |
| G2 | 57 | 37.5 |
| G3 | 76 | 50.0 |
| Molecular subtypes | ||
| Luminal/HER2− | 72 | 47.4 |
| Luminal B/HER2+ | 27 | 17.8 |
| Non-luminal HER2+ | 21 | 13.8 |
| Triple negative breast cancer | 30 | 19.7 |
| Unclassified | 2 | 1.3 |
| CD1a | LAMP3 | CD123 | CD83 | DC-SIGN | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| intratumoural | invasive margin | intratumoural | invasive margin | intratumoural | invasive margin | intratumoural | invasive margin | intratumoural | invasive margin | |||||||||||
| mean (SD) | p | mean (SD) | p | mean (SD) | p | mean (SD) | p | mean (SD) | p | mean (SD) | p | mean (SD) | p | mean (SD) | p | mean (SD) | p | mean (SD) | p | |
| Molecular subtype | ||||||||||||||||||||
| Luminal/HER2− | 7.55 (15.78) | <0.001 | 6.52 (12.07) | <0.001 | 3.21 (5.65) | <0.001 | 10.08 (10.54) | <0.001 | 10.35 (13.82) | <0.001 | 21.44 (20.83) | <0.009 | 2.69 (4.79) | <0.004 | 3.99 (5.59) | <0.05 | 4.02 (6.23) | NS | 11.76 (11.28) | NS |
| Luminal B/HER2+ | 14.84 (17.84) | 14.92 (18.88) | 2.62 (6.81) | 6.04 (13.67) | 24.92 (22.85) | 37.77 (33.03) | 0.19 (0.57) | 2.85 (10.52) | 8.24 (15.21) | 11.96 (14.69) | ||||||||||
| HER2+ non-luminal | 4.43 (4.80) | 4.67 (5.89) | 13.62 (14.00) | 9.52 (9.54) | 37.48 (44.16) | 37.33 (32.41) | 1.00 (2.36) | 2.65 (3.77) | 9.15 (19.43) | 14.45 (12.66) | ||||||||||
| Triple negative | 10.0 (16.84) | 7.33 (8.51) | 20.10 (25.52) | 19.30 (15.05) | 22.30 (23.09) | 37.10 (26.64) | 0.33 (1.32) | 1.77 (2.90) | 3.63 (6.51) | 14.06 (19.70) | ||||||||||
| CD1a | LAMP3 | CD123 | CD83 | DC-SIGN | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| intratumoural | invasive margin | intratumoural | invasive margin | intratumoural | invasive margin | intratumoural | invasive margin | intratumoural | invasive margin | |||||||||||
| mean (SD) | p | mean (SD) | p | mean (SD) | p | mean (SD) | p | mean (SD) | p | mean (SD) | p | mean (SD) | p | mean (SD) | p | mean (SD) | p | mean (SD) | p | |
| ER expression | ||||||||||||||||||||
| positive | 10.04 (17.75) | NS | 8.95 (14.02) | NS | 4.98 (14.19) | <0.001 | 9.37 (12.07) | 0.001 | 15.19 (19.89) | <0.001 | 27.84 (26.91) | NS | 1.98 (4.17) | NS | 3.62 (6.92) | NS | 5.33 (9.47) | NS | 12.39 (12.41) | NS |
| negative | 5.83 (6.50) | 5.32 (7.46) | 16.00 (15.01) | 15.80 (13.32) | 29.46 (34.09) | 34.68 (27.62) | 0.35 (1.07) | 1.87 (3.30) | 5.55 (14.38) | 13.32 (17.87) | ||||||||||
| PR expression | ||||||||||||||||||||
| positive | 10.30 (18.05) | NS | 8.83 (14.24) | NS | 5.42 (14.63) | <0.001 | 9.91 (12.27) | <0.03 | 15.0 (19.16) | <0.002 | 27.03 (25.97) | NS | 1.97 (4.20) | NS | 3.57 (7.01) | NS | 4.87 (8.02) | NS | 12.34 (11.88) | NS |
| negative | 5.60 (6.23) | 5.73 (7.50) | 14.04 (14.94) | 14.11 (13.40) | 28.35 (33.92) | 35.91 (29.17) | 0.56 (1.66) | 2.16 (3.47) | 6.57 (15.88) | 13.36 (18.27) | ||||||||||
| Ki67 expression | ||||||||||||||||||||
| low | 6.51 (14.75) | <0.002 | 6.50 (12.54) | <0.02 | 5.64 (9.96) | NS | 9.75 (9.98) | NS | 11.35 (14.54) | <0.001 | 19.98 (19.74) | <0.001 | 2.35(4.74) | <0.04 | 3.64 (5.71) | NS | 5.76 (13.49) | NS | 12.29 (12.83) | NS |
| high | 10.74 (15.98) | 8.95 (12.61) | 9.97 (18.12) | 12.29 (14.45) | 25.30 (30.03) | 37.37 (29.78) | 0.89 (2.35) | 2.75 (6.52) | 5.11 (8.74) | 12.92 (15.03) | ||||||||||
| HER2 status | ||||||||||||||||||||
| normal | 8.29 (16.06) | <0.03 | 6.77 (11.07) | <0.04 | 8.33 (16.61) | NS | 12.92 (12.75) | <0.006 | 13.87 (17.82) | <0.001 | 26.09 (23.69) | NS | 1.99 (4.23) | NS | 3.32 (5.02) | NS | 3.91 (6.29) | NS | 12.46 (14.32) | NS |
| overexpressed | 10.09 (14.41) | 10.24 (15.24) | 7.53 (11.88) | 7.60 (12.01) | 30.53 (34.23) | 37.57 (32.40) | 0.54 (1.64) | 2.76 (8.21) | 8.64 (17.01) | 13.07 (13.73) | ||||||||||
| CD1a | LAMP3 | CD123 | CD83 | DC-SIGN | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| intratumoural | invasive margin | intratumoural | invasive margin | intratumoural | invasive margin | intratumoural | invasive margin | intratumoural | invasive margin | |||||||||||
| mean (SD) | p | mean (SD) | p | mean (SD) | p | mean (SD) | p | mean (SD) | p | mean (SD) | p | mean (SD) | p | mean (SD) | p | mean (SD) | p | mean (SD) | p | |
| Grade | ||||||||||||||||||||
| 1 | 8.61 (19.25) | <0.009 | 6.77 (9.14) | NS | 6.15 (9.38) | NS | 10.16 (7.17) | NS | 9.26 (11.37) | <0.001 | 19.84 (16.93) | <0.001 | 2.26 (4.36) | NS | 3.37 (5.05) | NS | 1.87 (3.48) | NS | 9.19 (6.52) | NS |
| 2 | 4.49 (5.69) | 6.30 (7.21) | 4.18 (7.39) | 10.74 (12.21) | 11.79 (16.56) | 19.53 (19.49) | 1.91 (4.06) | 3.64 (5.58) | 3.82 (5.39) | 11.92 (11.72) | ||||||||||
| 3 | 12.10 (18.69) | 9.15 (15.98) | 11.29 (19.27) | 11.91 (14.06) | 27.20 (30.27) | 39.71 (30.29) | 1.03 (3.06) | 2.63 (6.82) | 7.66 (14.67) | 14.62 (18.01) | ||||||||||
| CD1a | LAMP3 | CD123 | CD83 | DC-SIGN | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| intratumoural | invasive margin | intratumoural | invasive margin | intratumoural | invasive margin | intratumoural | invasive margin | intratumoural | invasive margin | |||||||||||
| mean (SD) | p | mean (SD) | p | mean (SD) | p | mean (SD) | p | mean (SD) | p | mean (SD) | p | mean (SD) | p | mean (SD) | p | mean (SD) | p | mean (SD) | p | |
| Histologic type | ||||||||||||||||||||
| NOS | 9.53 (16.18) | <0.015 | 8.57 (13.11) | <0.002 | 8.83 (15.91) | NS | 12.08 (13.14) | NS | 20.87 (26.12) | <0.001 | 30.51 (26.27) | <0.001 | 1.24 (3.08) | NS | 2.94 (6.12) | NS | 5.77 (11.82) | NS | 13.32 (15.58) | NS |
| Lobular | 3.06 (6.53) | 2.18 (4.20) | 2.41 (4.09) | 6.00 (6.94) | 4.12 (5.25) | 13.35 (24.74) | 3.71 (6.33) | 4.65 (6.63) | 4.18 (4.93) | 10.29 (9.56) | ||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szpor, J.; Streb, J.; Glajcar, A.; Frączek, P.; Winiarska, A.; Tyrak, K.E.; Basta, P.; Okoń, K.; Jach, R.; Hodorowicz-Zaniewska, D. Dendritic Cells Are Associated with Prognosis and Survival in Breast Cancer. Diagnostics 2021, 11, 702. https://doi.org/10.3390/diagnostics11040702
Szpor J, Streb J, Glajcar A, Frączek P, Winiarska A, Tyrak KE, Basta P, Okoń K, Jach R, Hodorowicz-Zaniewska D. Dendritic Cells Are Associated with Prognosis and Survival in Breast Cancer. Diagnostics. 2021; 11(4):702. https://doi.org/10.3390/diagnostics11040702
Chicago/Turabian StyleSzpor, Joanna, Joanna Streb, Anna Glajcar, Paulina Frączek, Aleksandra Winiarska, Katarzyna E. Tyrak, Paweł Basta, Krzysztof Okoń, Robert Jach, and Diana Hodorowicz-Zaniewska. 2021. "Dendritic Cells Are Associated with Prognosis and Survival in Breast Cancer" Diagnostics 11, no. 4: 702. https://doi.org/10.3390/diagnostics11040702
APA StyleSzpor, J., Streb, J., Glajcar, A., Frączek, P., Winiarska, A., Tyrak, K. E., Basta, P., Okoń, K., Jach, R., & Hodorowicz-Zaniewska, D. (2021). Dendritic Cells Are Associated with Prognosis and Survival in Breast Cancer. Diagnostics, 11(4), 702. https://doi.org/10.3390/diagnostics11040702