
The Role of Left-Atrial Mechanics Assessed by Two-Dimensional Speckle-Tracking Echocardiography to Differentiate Hypertrophic Cardiomyopathy from Hypertensive Left-Ventricular Hypertrophy

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Genetic Testing
2.3. Echocardiographic Image Acquisition
2.3.1. Conventional Echocardiography Analysis
2.3.2. Left Atrial 2D Volumetric Analysis
2.3.3. LA 2D Speckle-Tracking Analysis
2.4. Reproducibility Assessment
2.5. Statistical Analysis
3. Results
3.1. Study Population and Conventional Echocardiography Parameters
3.2. Reproducibility Analysis
3.3. LA Volumetric Analysis
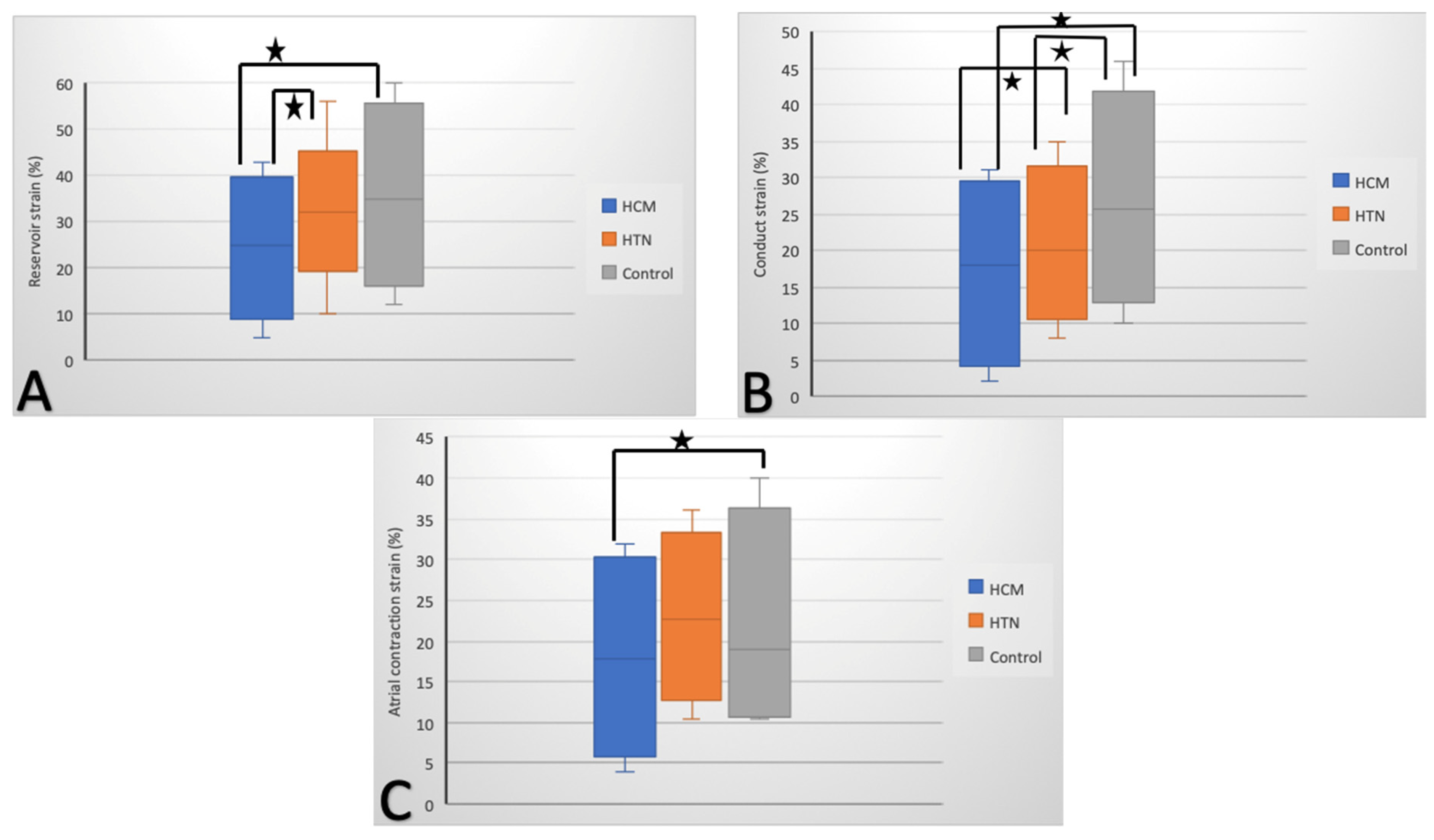
3.4. LA 2D Speckle-Tracking Analysis
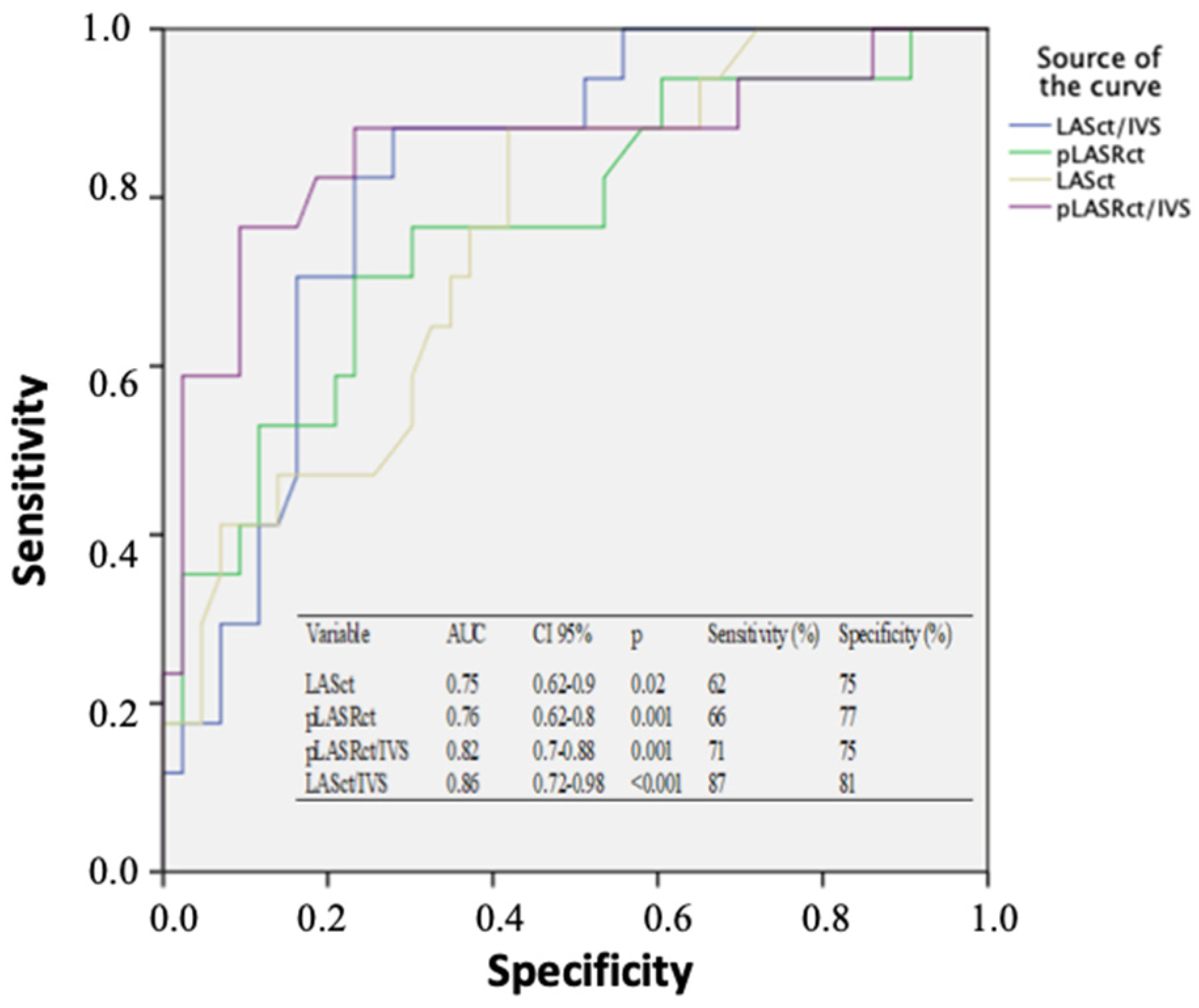
3.5. The Novel Strain-To-Thickness Ratio
3.6. LA Mechanics According to Genotype
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lopes, L.R.; Elliott, P.M. A straightforward guide to the sarcomeric basis of cardiomyopathies. Heart 2014, 100, 1916–1923. [Google Scholar] [CrossRef] [PubMed]
- Razumova, M.V.; Shaffer, J.F.; Tu, A.Y.; Flint, G.V.; Regnier, M.; Harris, S.P. Effects of the N-terminal domains of myosin binding protein-C in an in vitro motility assay: Evidence for long-lived cross-bridges. J. Biol. Chem. 2006, 281, 35846–35854. [Google Scholar] [CrossRef] [Green Version]
- Ferrazzi, P.; Spirito, P.; Binaco, I.; Zyrianov, A.; Poggio, D.; Vaccari, G.; Grillo, M.; Pezzoli, L.; Scatigno, A.; Dorobantu, L.; et al. Congenital Muscular Mitral-Aortic Discontinuity Identified in Patients With Obstructive Hypertrophic Cardiomyopathy. J. Am. Coll. Cardiol. 2020, 76, 2238–2247. [Google Scholar] [CrossRef] [PubMed]
- Kahan, T.; Bergfeldt, L. Left ventricular hypertrophy in hypertension: Its arrhythmogenic potential. Heart 2005, 91, 250–256. [Google Scholar] [CrossRef] [Green Version]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F.; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2016, 17, 1321–1360. [Google Scholar]
- Russo, C.; Jin, Z.; Homma, S.; Rundek, T.; Elkind, M.S.; Sacco, R.L.; Di Tullio, M.R. LA Phasic Volumes and Reservoir Function in the Elderly by Real-Time 3D Echocardiography: Normal Values, Prognostic Significance, and Clinical Correlates. JACC: Cardiovasc. Imaging 2017, 10, 976–985. [Google Scholar]
- Saijo, Y.; Van Iterson, E.; Desai, M.Y.; Lever, H.; Thamilarasan, M.; Popovic, Z.; Grimm, R.A.; Griffin, B.P.; Xu, B. Utility of left atrial strain mechanics for predicting exercise intolerance in patients with hypertrophic cardiomyopathy. J. Am. Coll. Cardiol. 2020, 75, 1659. [Google Scholar] [CrossRef]
- Todaro, M.C.; Choudhuri, I.; Belohlavek, M.; Jahangir, A.; Carerj, S.; Oreto, L.; Khandheria, B.K. New echocardiographic techniques for evaluation of left atrial mechanics. Eur. Hear. J. Cardiovasc. Imaging 2012, 13, 973–984. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoit, B.D. Left atrial size and function: Role in prognosis. J. Am. Coll. Cardiol. 2014, 63, 493–505. [Google Scholar] [CrossRef] [PubMed]
- Badran, H.M.; Faheem, N.; Elnoamany, M.F.; Kenawy, A.; Yacoub, M. Characterization of left atrial mechanics in hypertrophic cardiomyopathy and essential hypertension using vector velocity imaging. Echocardiography 2015, 32, 1527–1538. [Google Scholar] [CrossRef] [PubMed]
- Donal, E.; Galli, E.; Schnell, F. Left atrial strain: A must or a plus for routine clinical practice? Circ. Cardiovasc. Imaging 2017, 10, e007023. [Google Scholar] [CrossRef] [Green Version]
- Elliott, P.M.; Anastasakis, A.; Borger, M.A.; Borggrefe, M.; Cecchi, F.; Charron, P.; Hagege, A.A.; Lafont, A.; Limongelli, G.; Mahrholdt, H.; et al. 2014 ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy. Eur. Heart J. 2014, 35, 2733–2779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nicoleta-Monica, P.-F.; Micheu, M.M.; Onciul, S.; Zamfir, D.; Dorobanţu, M. Combined right and left ventricular mechanical dispersion enhance the arrhythmic risk stratification in hypertrophic cardiomyopathy. J. Cardiol. 2020, 76, 364–370. [Google Scholar]
- Micheu, M.M.; Nicoleta-Monica, P.-F.; Oprescu, N.; Dorobantu, M.; Ratiu, A.C.; Ecovoiu, A.A. NGS data validated by Sanger sequencing reveal a puzzling small deletion of MYBPC3 gene associated with hypertrophic cardiomyopathy. Rom. Biotechnol. Lett. 2019, 24, 91–99. [Google Scholar] [CrossRef]
- Micheu, M.M.; Popa-Fotea, N.-M.; Oprescu, N.; Bogdan, S.; Dan, M.; Deaconu, A.; Dorobantu, L.; Gheorghe-Fronea, O.; Greavu, M.; Iorgulescu, C.; et al. Yield of rare variants detected by targeted next-generation sequencing in a cohort of romanian index patients with hypertrophic cardiomyopathy. Diagnostics 2020, 10, 1061. [Google Scholar] [CrossRef] [PubMed]
- Richards, S.; Aziz, N.; Bale, S.; Bick, D.; Das, S.; Gastier-Foster, J.; Grody, W.W.; Hegde, M.; Lyon, E.; Spector, E.; et al. Standards and guidelines for the interpretation of sequence variants: A joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet. Med. 2015, 17, 405–423. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rokey, R.; Sterling, L.L.; Zoghbi, W.A.; Sartori, M.P.; Limacher, M.C.; Kuo, L.C.; Quinones, M.A. Determination of regurgitant fraction in isolated mitral or aortic regurgitation by pulsed Doppler two-dimensional echocardiography. J. Am. Coll. Cardiol. 1986, 7, 1273–1278. [Google Scholar] [CrossRef] [Green Version]
- Manning, W.J.; Katz, S.E.; Douglas, P.S.; Silverman, D.I. Atrial ejection force: A noninvasive assessment of atrial systolic function. J. Am. Coll. Cardiol. 1993, 22, 221–225. [Google Scholar] [CrossRef]
- Thomas, L.; Marwick, T.H.; Popescu, B.A.; Donal, E.; Badano, L.P. Left Atrial Structure and Function, and Left Ventricular Diastolic Dysfunction: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2019, 73, 1961–1977. [Google Scholar] [CrossRef]
- Badano, L.P.; Kolias, T.J.; Muraru, D.; Abraham, T.P.; Aurigemma, G.; Edvardsen, T.; D’Hooge, J.; Donal, E.; Fraser, A.G.; Marwick, T.; et al. Standardization of left atrial, right ventricular, and right atrial deformation imaging using two-dimensional speckle tracking echocardiography: A consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 591–600. [Google Scholar] [CrossRef] [PubMed]
- Machino-Ohtsuka, T.; Seo, Y.; Tada, H.; Ishizu, T.; Machino, T.; Yamasaki, H.; Igarashi, M.; Xu, D.; Sekiguchi, Y.; Aonuma, K. Left Atrial Stiffness Relates to Left Ventricular Diastolic Dysfunction and Recurrence After Pulmonary Vein Isolation for Atrial Fibrillation. J. Cardiovasc. Electrophysiol. 2011, 22, 999–1006. [Google Scholar] [CrossRef]
- Kurt, M.; Wang, J.; Torre-Amione, G.; Nagueh, S.F. Left atrial function in diastolic heart failure. Circ. Cardiovasc. Imaging 2009, 2, 10–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, N.G.; Lee, K.J.; Lee, S.; Jeong, S.-Y.; Lee, Y.S.; Choi, Y.J.; Yoon, H.S.; Kim, J.H.; Jeong, K.T.; Park, S.C.; et al. Feasibility of Two-Dimensional Global Longitudinal Strain and Strain Rate Imaging for the Assessment of Left Atrial Function: A Study in Subjects with a Low Probability of Cardiovascular Disease and Normal Exercise Capacity. Echocardiography 2009, 26, 1179–1187. [Google Scholar] [CrossRef] [PubMed]
- Sirbu, C.; Herbots, L.; D’Hooge, J.; Claus, P.; Marciniak, A.; Langeland, T.; Bijnens, B.; Rademakers, F.; Sutherland, G. Feasibility of strain and strain rate imaging for the assessment of regional left atrial deformation: A study in normal subjects. Eur. J. Echocardiogr. 2006, 7, 199–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, W.-C.; Huang, Y.-Y.; Liu, Y.-W.; Shih, J.-Y.; Lin, C.-C.; Tsai, L.-M. Changes of Left Atrial Phasic Function Assessed by Speckle Tracking Echocardiography in Untreated Hypertension. J. Med. Ultrasound 2012, 20, 220–227. [Google Scholar] [CrossRef] [Green Version]
- Hrabia, J.B.; Pogue, E.P.; Zayachkowski, A.G.; Długosz, D.; Kruszelnicka, O.; Surdacki, A.; Chyrchel, B. Left atrial compliance: An overlooked predictor of clinical outcome in patients with mitral stenosis or atrial fibrillation undergoing invasive management. Postepy w Kardiol Interwencyjnej. Adv. Interv. Cardiol. 2018, 14, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Kowallick, J.T.; Vieira, M.S.; Kutty, S.; Lotz, J.; Hasenfuss, G.; Chiribiri, A.; Schuster, A. Left atrial performance in the course of hypertrophic cardiomyopathy: Relation to left ventricular hypertrophy and fibrosis. Investig. Radiol. 2017, 52, 177–185. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Yin, G.; Jiang, Y.; Song, L.; Zhao, S.; Lu, M. Quantification of left atrial function in patients with non-obstructive hypertrophic cardiomyopathy by cardiovascular magnetic resonance feature tracking imaging: A feasibility and reproducibility study. J. Cardiovasc. Magn. Reson. 2020, 22, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Colan, S.D.; Lipshultz, S.E.; Lowe, A.M.; Sleeper, L.A.; Messere, J.; Cox, G.F.; Lurie, P.R.; Orav, E.J.; Towbin, J.A. Epidemiology and Cause-Specific Outcome of Hypertrophic Cardiomyopathy in Children. Circulation 2007, 115, 773–781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, H.; Woo, A.; Monakier, D.; Jamorski, M.; Fedwick, K.; Wigle, E.D.; Rakowski, H. Enlarged Left Atrial Volume in Hypertrophic Cardiomyopathy: A Marker for Disease Severity. J. Am. Soc. Echocardiogr. 2005, 18, 1074–1082. [Google Scholar] [CrossRef] [PubMed]
- Marsiglia, J.D.C.; Credidio, F.L.; de Oliveira, T.G.M.; Reis, R.F.; Antunes, M.O.; de Araujo, A.Q.; Pedrosa, R.P.; Barbosa-Ferreira, J.M.B.; Mady, C.; Krieger, J.E.; et al. Screening of MYH7, MYBPC3, and TNNT2 genes in Brazilian patients with hypertrophic cardiomyopathy. Am. Heart J. 2013, 166, 775–782. [Google Scholar] [CrossRef] [PubMed]
- Badano, L.P.; Miglioranza, M.H.; Mihăilă, S.; Peluso, D.; Xhaxho, J.; Marra, M.P.; Cucchini, U.; Soriani, N.; Iliceto, S.; Muraru, D. Left atrial volumes and function by three-dimensional echocardiography: Reference Values, accuracy, reproducibility, and comparison with two-dimensional echocardiographic measurements. Circ. Cardiovasc. Imaging 2016, 9, e004229. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variable | HCM (n = 43) | HTN wit LVH (n = 43) | Control (n = 33) | p HCM vs. Control | p HTN vs. Control | p HCM vs. HTN |
|---|---|---|---|---|---|---|
| Age (years) | 50 ± 14.5 | 51.4 ± 13.1 | 47 ± 11.2 | 0.29 | 0.10 | 0.97 |
| Gender (male) (%) | 36 (78.3%) | 30 (69.6%) | 29 (80.5%) | 0.35 | 0.09 | 0.2 |
| IVS (mm) | 20.24 ± 4.32 | 16.2 ± 2.6 | 8.2 ± 1.7 | <0.001 | <0.001 | <0.001 |
| Posterior wall (mm) | 14.18 ± 3.6 | 14.2 ± 1.4 | 7.6 ± 1.6 | <0.001 | <0.001 | 0.972 |
| RWT | 0.66 ± 0.13 | 0.96 ± 0.23 | 0.35 ± 0.1 | <0.001 | <0.001 | <0.001 |
| Indexed LV Mass (g/m2) | 131.85 ± 44.7 | 92 ± 30.9 | 71 ± 19.23 | <0.001 | <0.001 | <0.001 |
| LVEDD (mm) | 40.84 ± 7.58 | 40 ± 11.6 | 38 ± 4.8 | 0.053 | 0.29 | 0.68 |
| LVESD (mm) | 24.51 ± 8.2 | 25.8 ± 4.7 | 27 ± 6 | 0.11 | 0.33 | 0.36 |
| LVEDV (mL) | 90.2 ± 15 | 85 ± 9 | 86 ± 10 | 0.18 | 0.65 | 0.055 |
| LVESV (mL) | 40 ± 15.6 | 37 ± 9 | 38 ± 11.3 | 0.53 | 0.67 | 0.28 |
| LVEF (%) | 53.2 ± 11.87 | 55 ± 9.2 | 56 ± 7 | 0.19 | 0.58 | 0.42 |
| HR (bpm) | 70 ± 12 | 72 ± 9 | 75 ± 10 | 0.057 | 0.17 | 0.38 |
| Cardiac output (L/min) | 5.7 ± 0.6 | 5.9 ± 0.2 | 6 ± 0.8 | 0.066 | 0.43 | 0.051 |
| Cardiac index (L/min/m2) | 3.2 ± 0.38 | 3.3 ± 0.42 | 3.5 ± 0.5 | 0.004 | 0.062 | 0.25 |
| LA diameter (mm) | 42.77 ± 8.91 | 40 ± 6.1 | 37.1 ± 6 | 0.001 | 0.04 | 0.097 |
| E (cm/s) | 95.4 ± 4.31 | 86 ± 9.1 | 90 ± 5.2 | <0.001 | 0.018 | <0.001 |
| A (cm/s) | 74.4 ± 3.21 | 81 ± 5.2 | 75 ± 2 | 0.96 | <0.001 | <0.001 |
| E/A (cm/s) | 1.23 ± 0.55 | 1 ± 3.4 | 1.1 ± 1.7 | 0.67 | 0.87 | 0.66 |
| e’s (cm/s) | 6.2 ± 2.4 | 10 ± 4.5 | 10 ± 3.2 | <0.001 | 0.98 | <0.001 |
| e’l (cm/s) | 8.6 ± 4 | 9 ± 4 | 11 ± 3.2 | <0.001 | 0.02 | 0.64 |
| e’m (cm/s) | 7.4 ± 3.1 | 8 ± 4.1 | 10.5 ± 1.8 | <0.001 | 0.001 | 0.45 |
| E/e’s | 18.65 ± 15.5 | 10.7 ± 5 | 9 ± 1.5 | <0.001 | 0.06 | <0.001 |
| E/e’l | 12.93 ± 8.6 | 8 ± 2.5 | 7 ± 2.2 | <0.001 | 0.07 | <0.001 |
| E/e’m | 15.8 ± 7.6 | 9 ± 3.4 | 8 ± 1.4 | <0.001 | 0.08 | <0.001 |
| Variable | HCM (n = 43) | HTN (n = 43) | Control (n = 33) | p HCM vs. Control | p HTN vs. Control | p HCM vs. HTN |
|---|---|---|---|---|---|---|
| Volumetric Variables and LAEF | ||||||
| LAVmax (mL/m2) | 32.8 ± 24.3 | 29.89 ± 17.3 | 25 ± 10.9 | <0.001 | 0.16 | 0.526 |
| LAVmin (mL/m2) | 18 ± 6.5 | 16 ± 5 | 14 ± 8.2 | 0.025 | 0.22 | 0.114 |
| LAVpre-A (mL/ m2) | 24 ± 7 | 21 ± 1.4 | 19.7 ± 2.6 | <0.001 | 0.01 | 0.008 |
| LATEF (%) | 55 ± 9.2 | 61 ± 8.9 | 60 ± 10.3 | 0.03 | 0.66 | 0.003 |
| LAEI (%) | 168 ± 50.5 | 191 ± 89 | 200 ± 87.2 | 0.048 | 0.66 | 0.144 |
| LAPEF (%) | 25 ± 10.5 | 26 ± 9.1 | 31 ± 11.2 | 0.019 | 0.035 | 0.64 |
| LAAEF (%) | 44 ± 6.9 | 47 ± 7.8 | 47 ± 15.6 | 0.31 | 0.98 | 0.062 |
| LAEF (kdyne) | 12 ± 3.4 | 13 ± 1.2 | 14 ± 6.2 | 0.077 | 0.3 | 0.073 |
| Deformation Variables | ||||||
| Reservoir Function | ||||||
| LASr (%) | 24 ± 5.8 | 32 ± 9.7 | 35 ± 7.2 | <0.001 | 0.14 | <0.001 |
| LASr/IVS | 1.1 ± 0.2 | 1.9 ± 0.7 | 5 ± 2.6 | <0.001 | <0.001 | <0.001 |
| pLASRr (s−1) | 1 ± 0.89 | 1.9 ± 0.4 | 2 ± 0.87 | <0.001 | 0.54 | <0.001 |
| pLASRr/IVS | 0.1 ± 0.09 | 0.15 ± 0.1 | 0.3 ± 0.08 | <0.001 | <0.001 | 0.017 |
| LASI | 1.7 ± 0.5 | 0.35 ± 0.2 | 0.24 ± 0.1 | <0.001 | 0.005 | <0.001 |
| Conduit Function | ||||||
| LAScd (%) | 18 ± 7.1 | 22 ± 1.3 | 25 ± 4.6 | <0.001 | <0.001 | <0.001 |
| LAScd/IVS | 1.1 ± 0.7 | 1.5 ± 0.2 | 3.6 ± 1.8 | <0.001 | <0.001 | 0.001 |
| pLASRcd (s−1) | −0.5 ± 0.1 | −1.2 ± 1.3 | −1.8 ± 0.95 | <0.001 | 0.029 | <0.001 |
| pLASRcd/IVS | −0.03 ± 0.1 | −0.07 ± 0.03 | −0.16 ± 0.1 | <0.001 | <0.001 | 0.014 |
| Contractile Function | ||||||
| LASct (%) | 11 ± 2.1 | 12 ± 2.5 | 13 ± 2.7 | 0.001 | 0.1 | 0.05 |
| LASct/IVS | 0.5 ± 0.1 | 0.8 ± 0.2 | 1.87 ± 0.9 | <0.001 | <0.001 | <0.001 |
| pLASRct (s−1) | −1.4 ± 0.3 | −1.5 ± 1.3 | −1.61 ± 0.35 | 0.006 | 0.62 | 0.62 |
| pLASRct/IVS | −0.05 ± 0.1 | −0.1 ± 0.09 | −0.2 ± 0.1 | <0.001 | 0.001 | 0.017 |
| Variable | G+ HCM (n = 12) | G- HCM (n = 31) | HTN (n = 43) | p G+ vs. G− | p G+ vs. HTN | p G− vs. HTN |
|---|---|---|---|---|---|---|
| Age (years) | 41 ± 11.45 | 54.3 ± 15.2 | 51.4 ± 13.1 | 0.009 | 0.015 | 0.38 |
| Gender (male) (%) | 12 (100%) | 21 (67.7%) | 30 (69.6%) | 0.04 | 0.056 | 0.4 |
| IVS (mm) | 19.17 ± 5.13 | 20.45 ± 4.33 | 16.2 ± 2.6 | 0.24 | 0.008 | <0.001 |
| Posterior wall (mm) | 13.27 ± 3.38 | 15.03 ± 3.73 | 14.2 ± 1.4 | 0.18 | 0.15 | 0.18 |
| Indexed LV mass (g/m2) | 163 ± 45.35 | 140.42 ± 43.35 | 92 ± 30.9 | 0.14 | <0.001 | <0.001 |
| LVEF (%) | 55 ± 14.46 | 55.1 ± 10.85 | 55 ± 9.2 | 0.14 | 0.98 | 0.96 |
| LA diameter (mm) | 43.2 ± 2.31 | 41.9 ± 7.16 | 40 ± 6.1 | 0.33 | 0.08 | 0.22 |
| Volumetric Variables | ||||||
| LAVmax (mL/m2) | 33.16 ± 3.07 | 32.84 ± 3 | 29.89 ± 17.3 | 0.11 | 0.52 | 0.35 |
| LAVmin (mL/m2) | 15.16 ± 1.46 | 14.64 ± 1.64 | 16 ± 5 | 0.32 | 0.57 | 0.15 |
| LAVpre-A (mL/m2) | 23 ± 2.4 | 25 ± 1.2 | 21 ± 1.4 | 0.001 | 0.001 | <0.001 |
| LATEF (%) | 54.7 ± 15.3 | 56 ± 17.2 | 61 ± 8.9 | 0.82 | 0.07 | 0.10 |
| LAEI (%) | 167 ± 18.11 | 169 ± 25 | 191 ± 89 | 0.8 | 0.36 | 0.18 |
| LAPEF (%) | 26.2 ± 2.65 | 24.22 ± 5.74 | 26 ± 9.1 | 0.45 | 0.94 | 0.34 |
| LAAEF (%) | 44 ± 3.55 | 43.29 ± 1.98 | 47 ± 7.8 | 0.41 | 0.2 | 0.051 |
| LAEF (kdyne) | 11.1 ± 4.4 | 14 ± 3.1 | 13 ± 1.2 | 0.053 | 0.17 | 0.096 |
| Deformation Variables | ||||||
| Reservoir Function | ||||||
| LASr (%) | 24.7 ± 1.92 | 25 ± 2.7 | 32 ± 9.7 | 0.47 | <0.001 | <0.001 |
| pLASRr (s−1) | 0.93 ± 0.25 | 1.11 ± 0.28 | 1.9 ± 0.4 | 0.059 | <0.001 | <0.001 |
| LASI | 1.7 ± 0.2 | 1.8 ± 0.5 | 0.35 ± 0.2 | 0.22 | <0.001 | <0.001 |
| Conduit Function | ||||||
| LAScd (%) | 17.82 ± 1.98 | 18.4 ± 2.91 | 22 ± 1.3 | 0.17 | <0.001 | <0.001 |
| pLASRcd (s−1) | −0.42 ± 0.44 | −0.7 ± 1.2 | −1.2 ± 1.3 | 0.056 | <0.001 | <0.001 |
| Contractile Function | ||||||
| LASct (%) | 10.3 ± 1.9 | 11.4 ± 2.37 | 12 ± 2.5 | 0.003 | 0.034 | 0.3 |
| pLASRct (s−1) | −1.15 ± 0.4 | −1.5 ± 0.23 | −1.5 ± 1.3 | <0.001 | 0.02 | 0.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Popa-Fotea, N.-M.; Micheu, M.M.; Oprescu, N.; Alexandrescu, A.; Greavu, M.; Onciul, S.; Onut, R.; Petre, I.; Scarlatescu, A.; Stoian, M.; et al. The Role of Left-Atrial Mechanics Assessed by Two-Dimensional Speckle-Tracking Echocardiography to Differentiate Hypertrophic Cardiomyopathy from Hypertensive Left-Ventricular Hypertrophy. Diagnostics 2021, 11, 814. https://doi.org/10.3390/diagnostics11050814
Popa-Fotea N-M, Micheu MM, Oprescu N, Alexandrescu A, Greavu M, Onciul S, Onut R, Petre I, Scarlatescu A, Stoian M, et al. The Role of Left-Atrial Mechanics Assessed by Two-Dimensional Speckle-Tracking Echocardiography to Differentiate Hypertrophic Cardiomyopathy from Hypertensive Left-Ventricular Hypertrophy. Diagnostics. 2021; 11(5):814. https://doi.org/10.3390/diagnostics11050814
Chicago/Turabian StylePopa-Fotea, Nicoleta-Monica, Miruna Mihaela Micheu, Nicoleta Oprescu, Adriana Alexandrescu, Maria Greavu, Sebastian Onciul, Roxana Onut, Ioana Petre, Alina Scarlatescu, Monica Stoian, and et al. 2021. "The Role of Left-Atrial Mechanics Assessed by Two-Dimensional Speckle-Tracking Echocardiography to Differentiate Hypertrophic Cardiomyopathy from Hypertensive Left-Ventricular Hypertrophy" Diagnostics 11, no. 5: 814. https://doi.org/10.3390/diagnostics11050814