
Differences between [18F]FLT and [18F]FDG Uptake in PET/CT Imaging in CC Depend on Vaginal Bacteriology

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
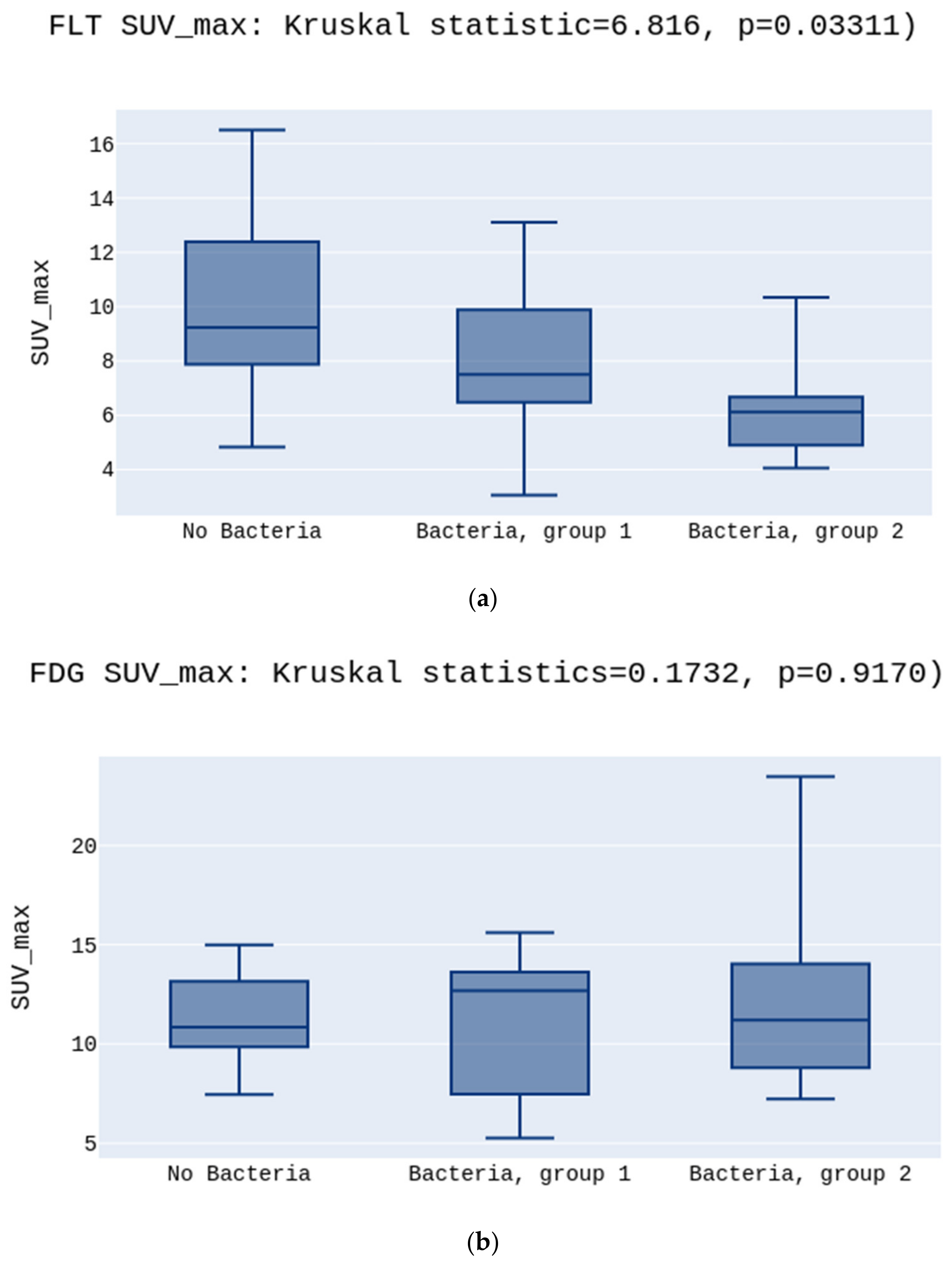
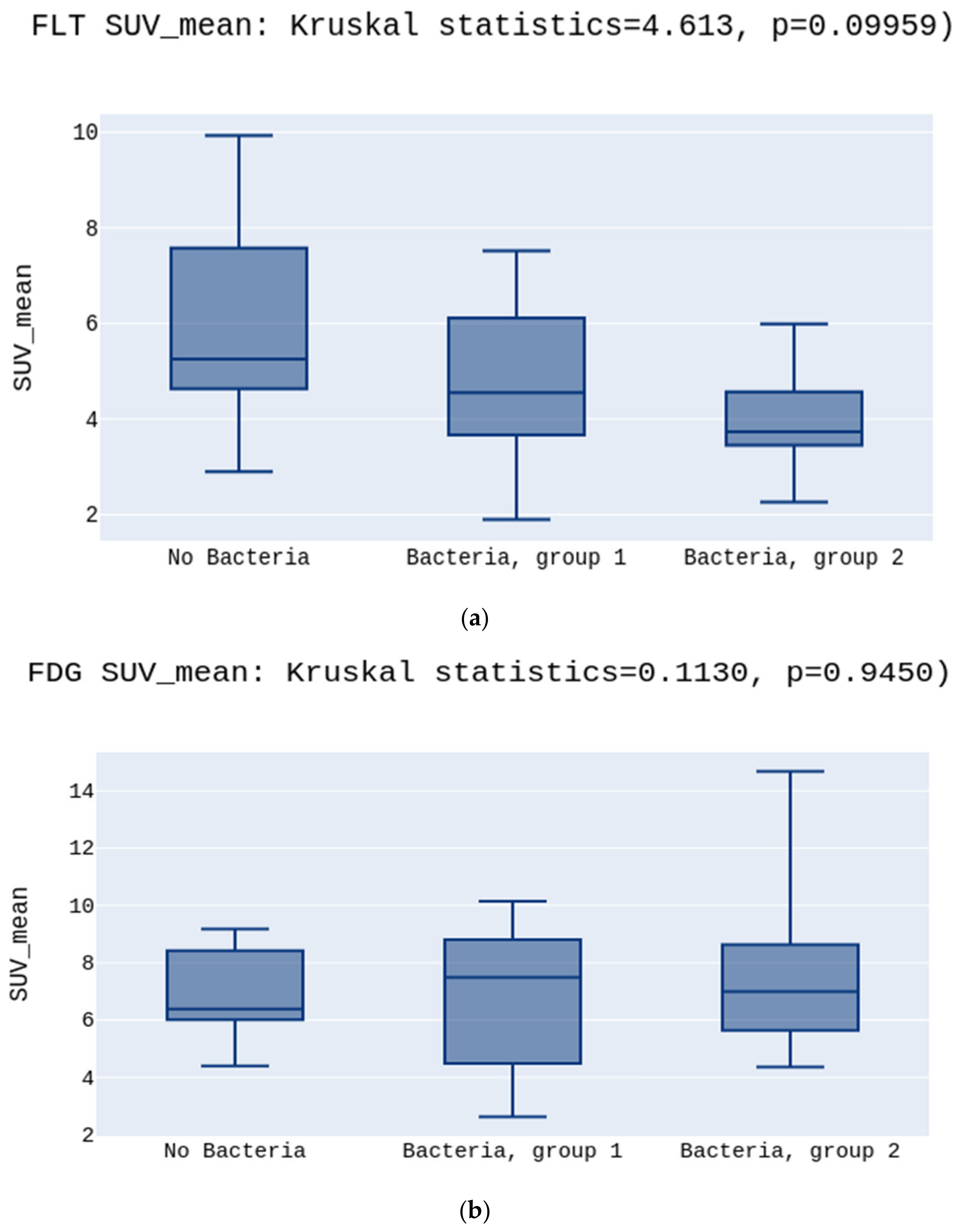
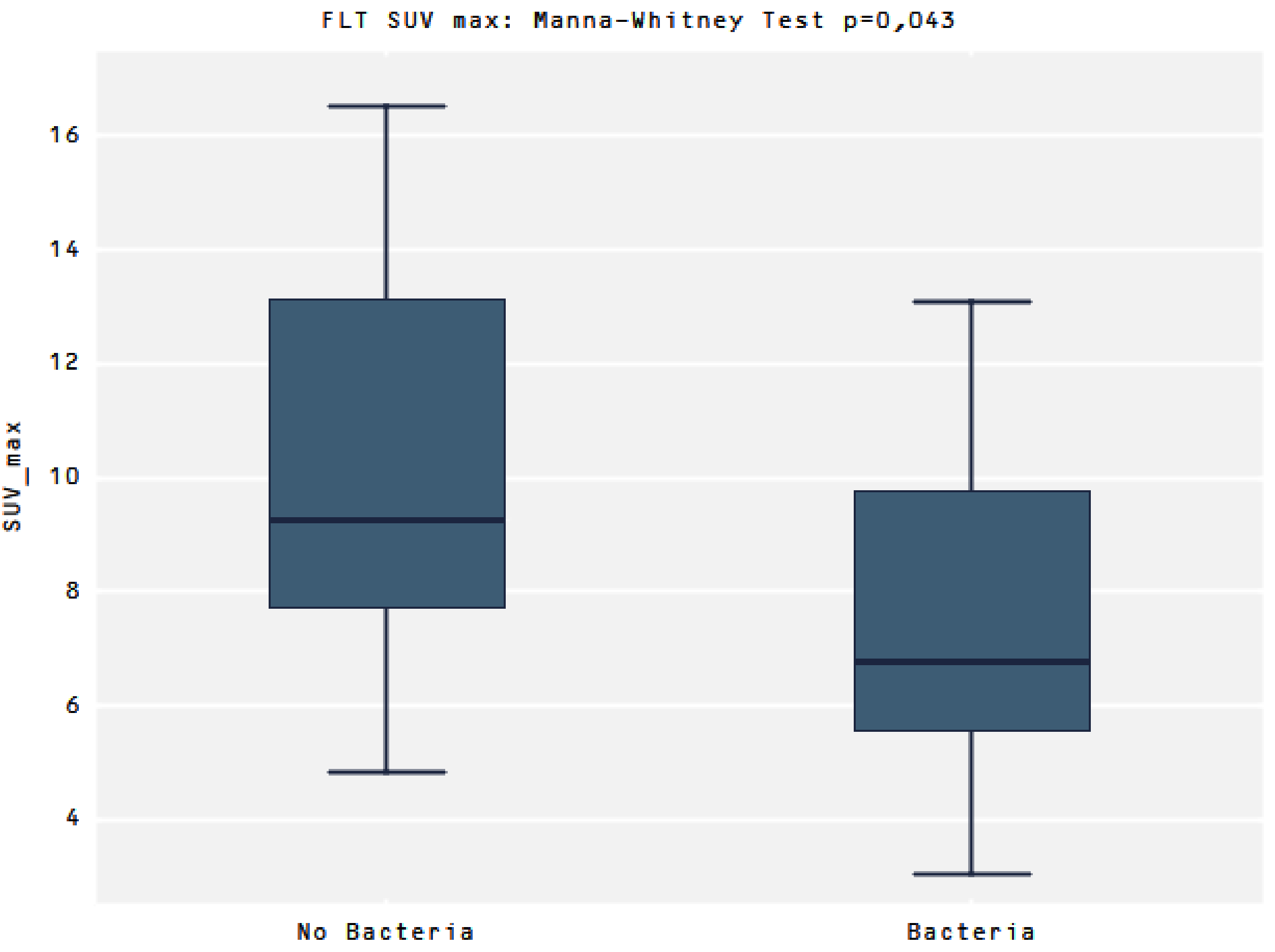
3. Results
Group Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries|Enhanced Reader. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Ravel, J.; Gajer, P.; Abdo, Z.; Schneider, G.M.; Koenig, S.S.K.; McCulle, S.L.; Karlebach, S.; Gorle, R.; Russell, J.; Tacket, C.O.; et al. Vaginal microbiome of reproductive-age women. Proc. Natl. Acad. Sci. USA 2011, 108 (Suppl. 1), 4680–4687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitra, A.; MacIntyre, D.A.; Lee, Y.S.; Smith, A.; Marchesi, J.R.; Lehne, B.; Bhatia, R.; Lyons, D.; Paraskevaidis, E.; Li, J.V.; et al. Cervical intraepithelial neoplasia disease progression is associated with increased vaginal microbiome diversity. Sci. Rep. 2015, 5, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, Y.; Chen, M.; Qin, L.; Wan, B.; Wang, H. A meta-analysis of the relationship between vaginal microecology, human papillomavirus infection and cervical intraepithelial neoplasia. Infect. Agents Cancer 2019, 29, 14. [Google Scholar]
- Tsai, C.S.; Chang, T.C.; Lai, C.H.; Tsai, C.C.; Ng, K.K.; Hsueh, S.; Yen, T.-C.; Hong, J.-H. Preliminary report of using FDG-PET to detect extrapelvic lesions in cervical cancer patients with enlarged pelvic lymph nodes on MRI/CT. Int. J. Radiat. Oncol. Biol. Phys. 2004, 58, 1506–1512. [Google Scholar] [CrossRef] [PubMed]
- Lazzari, R.; Cecconi, A.; Jereczek-Fossa, B.A.; Travaini, L.L.; Dell’Acqua, V.; Cattani, F.; Rizzo, S.; Fodor, C.; Landoni, F.; Orecchia, R. The role of [18F]FDG-PET/CT in staging and treatment planning for volumetric modulated Rapidarc radiotherapy in cervical cancer: Experience of the European Institute of Oncology, Milan, Italy. Ecancermedicalscience 2014, 8, 409. [Google Scholar]
- Barwick, T.; Bencherif, B.; Mountz, J.M.; Avril, N. Molecular PET and PET/CT imaging of tumour cell proliferation using F-18 fluoro-L-thymidine: A comprehensive evaluation. Nucl. Med. Commun. 2009, 30, 908–917. [Google Scholar] [CrossRef] [PubMed]
- Been, L.B.; Suurmeijer, A.; Cobben, D.C.P.; Jager, P.L.; Hoekstra, H.J.; Elsinga, P.H. [18F]FLT-PET in oncology: Current status and opportunities. Eur. J. Nucl. Med. Mol. Imaging 2004, 31, 1659–1672. [Google Scholar] [CrossRef] [PubMed]
- Bussink, J.; Kaanders, J.H.A.M.; van der Graaf, W.T.A.; Oyen, W.J.G. PET–CT for radiotherapy treatment planning and response monitoring in solid tumors. Nat. Rev. Clin. Oncol. 2011, 8, 233–242. [Google Scholar] [CrossRef] [PubMed]
- Mirpour, S.; Mhlanga, J.C.; Logeswaran, P.; Russo, G.; Mercier, G.; Subramaniam, R.M. The Role of PET/CT in the Management of Cervical Cancer. Am. J. Roentgenol. 2013, 201, W192–W205. [Google Scholar] [CrossRef] [PubMed]
- Cybulski, Z.; Urbański, B.; Grabiec, A.; Talaga, Z.; Pawlak, M.; Wareńczak-Florczak, Ż.; Roszak, A. The incidence of inflammation among patients suffering from cervix cancer with positive beta haemolytic streptococci cultures from genital tract. Rep. Pract. Oncol. Radiother. 2019, 24, 428–431. [Google Scholar] [CrossRef] [PubMed]
- Norenhag, J.; Du, J.; Olovsson, M.; Verstraelen, H.; Engstrand, L.; Brusselaers, N. The vaginal microbiota, human papillomavirus and cervical dysplasia: A systematic review and network meta-analysis. BJOG Int. J. Obstet. Gynaecol. 2020, 127, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Gillet, E.; Meys, J.F.; Verstraelen, H.; Bosire, C.; De Sutter, P.; Temmerman, M.; Broeck, D.V. Bacterial vaginosis is associated with uterine cervical human papillomavirus infection: A meta-analysis. BMC Infect. Dis. 2011, 11, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laniewski, P.; Barnes, D.; Goulder, A.; Cui, H.; Roe, D.J.; Chase, D.M.; Herbst-Kralovetz, M.M. Linking cervicovaginal immune signatures, HPV and microbiota composition in cervical carcinogenesis in non-Hispanic and Hispanic women. Sci. Rep. 2018, 8, 7593. [Google Scholar] [CrossRef] [PubMed]
- Shields, A.F.; Lim, K.; Grierson, J.; Link, J.; Krohn, K.A. Utilization of labeled thymidine in DNA synthesis: Studies for PET. J. Nucl. Med. 1990, 31, 337–342. [Google Scholar] [PubMed]
- Shields, A.F.; Grierson, J.R.; Koxawa, S.M.; Zheng, M. Development of Labeled Thymidine Analogs for Imaging Tumor Pr&liferation. Nucl. Med. Biol. 1996, 23, 17–22. [Google Scholar] [PubMed]
- Krhili, S.; Muratet, J.-P.; Roche, S.; Pointreau, Y.; Yossi, S.; Septans, A.-L.; Denis, F. Use of Metabolic Parameters as Prognostic Factors During Concomitant Chemoradiotherapy for Locally Advanced Cervical Cancer. Am. J. Clin. Oncol. 2017, 40, 250–255. [Google Scholar] [CrossRef] [PubMed]
- Lawal, I.; Lengana, T.; Van Rensburg, C.J.; Reyneke, F.; Popoola, G.O.; Ankrah, A.; Sathekge, M.M. Fluorodeoxyglucose Positron Emission Tomography integrated with computed tomography in carcinoma of the cervix: Its impact on accurate staging and the predictive role of its metabolic parameters. PLoS ONE 2019, 14, e0215412. [Google Scholar] [CrossRef] [PubMed]
- Heuker, M.; Sijbesma, J.W.A.; Suárez, R.A.; de Jong, J.R.; Boersma, H.H.; Luurtsema, G.; Elsinga, P.H.; Glaudemans, A.W.J.M.; van Dam, G.M.; van Dijl, J.M.; et al. In Vitro imaging of bacteria using 18F-fluorodeoxyglucose micro positron emission tomography. Sci. Rep. 2017, 7, 4973. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n | % | Average | Median | Min. | Max. | SD | |
|---|---|---|---|---|---|---|---|
| Age (years) | 34 | 100% | 57.2 | 59 | 30 | 84 | 12.3 |
| BMI | 34 | 100% | 26.4 | 24.9 | 18.4 | 43.9 | 5.8 |
| FIGO Stage | |||||||
| IIB | 12 | 35.3% | |||||
| IIIB | 20 | 58.8% | |||||
| IV | 2 | 5.9% | |||||
| Histopathology | |||||||
| SCC | 32 | 91.2% | |||||
| AC | 1 | 2.9% | |||||
| UD | 1 | 2.9% | |||||
| Hgb mmol/L | 34 | 100% | 7.38 | 7.9 | 4.6 | 9.6 | 1.1 |
| Leu G/L | 34 | 100% | 9.2 | 8.9 | 3.8 | 21.4 | 3.2 |
| Neu G/L | 34 | 100% | 6.3 | 5.7 | 2.3 | 16.6 | 2.8 |
| Bacteriology | n | % | Group |
|---|---|---|---|
| Enterobacter cloacae | 1 | 2.9% | 2 |
| Escherichia coli | 10 | 29.4% | 2 |
| Staphylococcus aureus | 3 | 8.9% | n.a. |
| Staphylococcus lugdunensis | 1 | 2.9% | n.a. |
| Streptococcus agalactiae | 9 | 26.3% | 1 |
| Streptococcus beta haemolyticus gr C | 2 | 2.9% | 1 |
| No bacteria | 7 | 20.6% | 0 |
| n | Average | Median | Min. | Max. | SD | |
|---|---|---|---|---|---|---|
| Activity of FDG (mCi) | 34 | 9.7 | 9.7 | 5.9 | 13.4 | 1.9 |
| SUV max FDG | 34 | 11.7 | 11.8 | 5.3 | 24.7 | 4.2 |
| SUV mean FDG | 34 | 6.9 | 7.3 | 2.6 | 14.7 | 2.6 |
| SUVmin FDG | 34 | 5.1 | 5.1 | 2.3 | 10.6 | 1.8 |
| AUC-CSH FDG | 34 | 0.6 | 0.6 | 0.5 | 0.7 | 0.0 |
| SUV max FLT | 34 | 7.7 | 7.46 | 3.1 | 16.5 | 10.7 |
| SUV mean FLT | 34 | 4.8 | 4.4 | 1.9 | 9.9 | 6.8 |
| SUVmin FLT | 34 | 3.2 | 3.5 | 1.3 | 8.9 | 4.6 |
| AUC-CSH FLT | 34 | 0.6 | 0.6 | 0.5 | 0.7 | 0.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burchardt, E.; Warenczak-Florczak, Z.; Cegła, P.; Piotrowski, A.; Cybulski, Z.; Burchardt, W.; Roszak, A.; Cholewiński, W. Differences between [18F]FLT and [18F]FDG Uptake in PET/CT Imaging in CC Depend on Vaginal Bacteriology. Diagnostics 2022, 12, 70. https://doi.org/10.3390/diagnostics12010070
Burchardt E, Warenczak-Florczak Z, Cegła P, Piotrowski A, Cybulski Z, Burchardt W, Roszak A, Cholewiński W. Differences between [18F]FLT and [18F]FDG Uptake in PET/CT Imaging in CC Depend on Vaginal Bacteriology. Diagnostics. 2022; 12(1):70. https://doi.org/10.3390/diagnostics12010070
Chicago/Turabian StyleBurchardt, Ewa, Zaneta Warenczak-Florczak, Paulina Cegła, Adam Piotrowski, Zefiryn Cybulski, Wojciech Burchardt, Andrzej Roszak, and Witold Cholewiński. 2022. "Differences between [18F]FLT and [18F]FDG Uptake in PET/CT Imaging in CC Depend on Vaginal Bacteriology" Diagnostics 12, no. 1: 70. https://doi.org/10.3390/diagnostics12010070
APA StyleBurchardt, E., Warenczak-Florczak, Z., Cegła, P., Piotrowski, A., Cybulski, Z., Burchardt, W., Roszak, A., & Cholewiński, W. (2022). Differences between [18F]FLT and [18F]FDG Uptake in PET/CT Imaging in CC Depend on Vaginal Bacteriology. Diagnostics, 12(1), 70. https://doi.org/10.3390/diagnostics12010070