
Volume Changes in the Descending Aorta after Frozen Elephant Trunk and Conventional Hemi-Arch Repair after Acute Type A Aortic Dissection

 , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Surgical Replacement
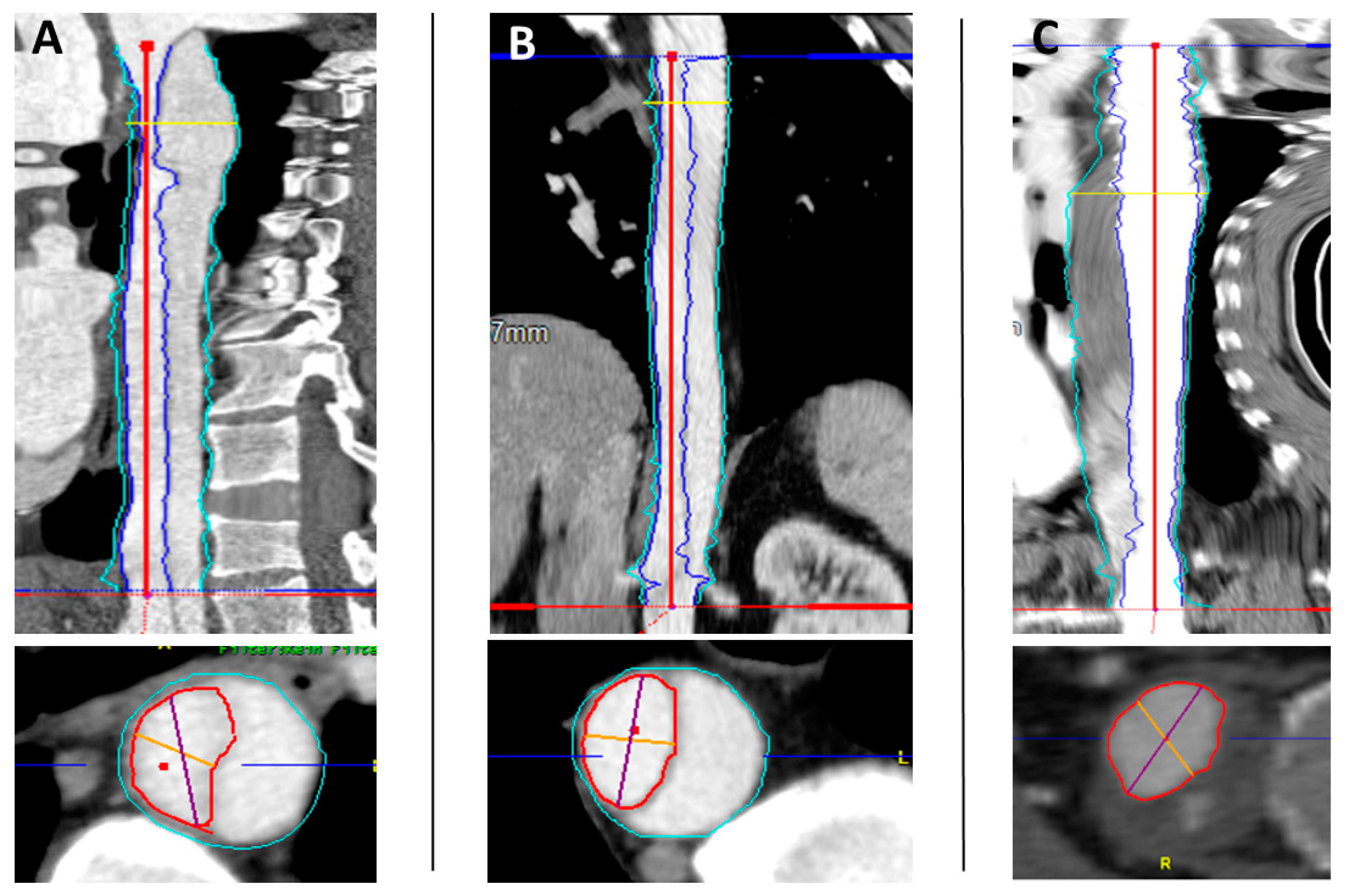
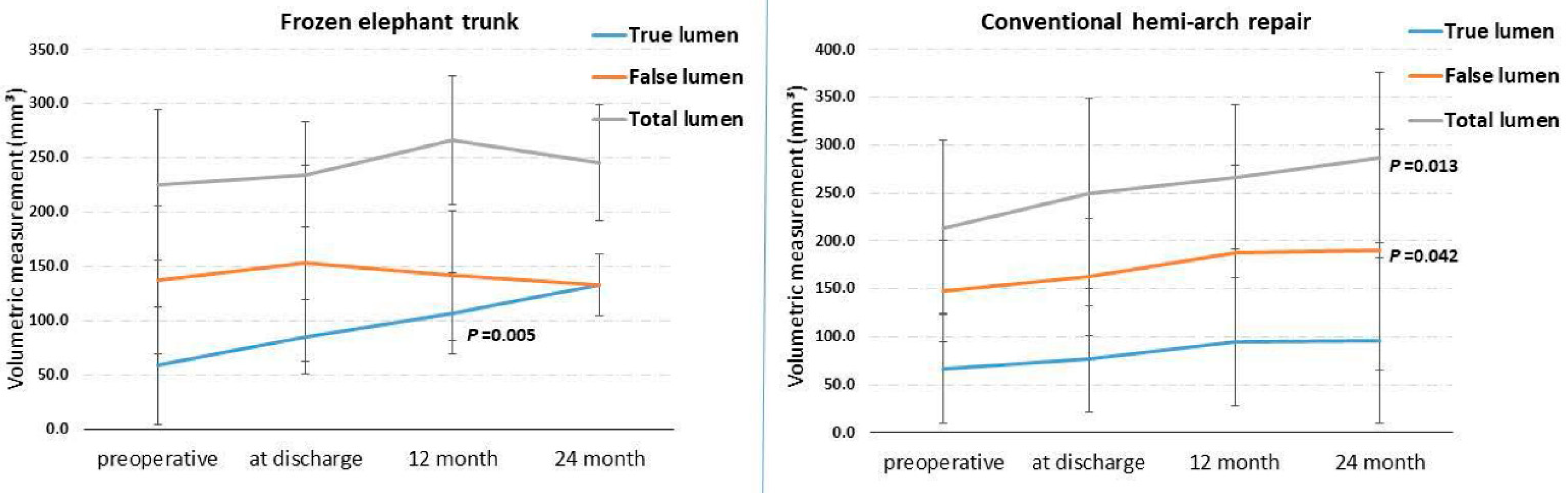
2.2. Volume Measurement
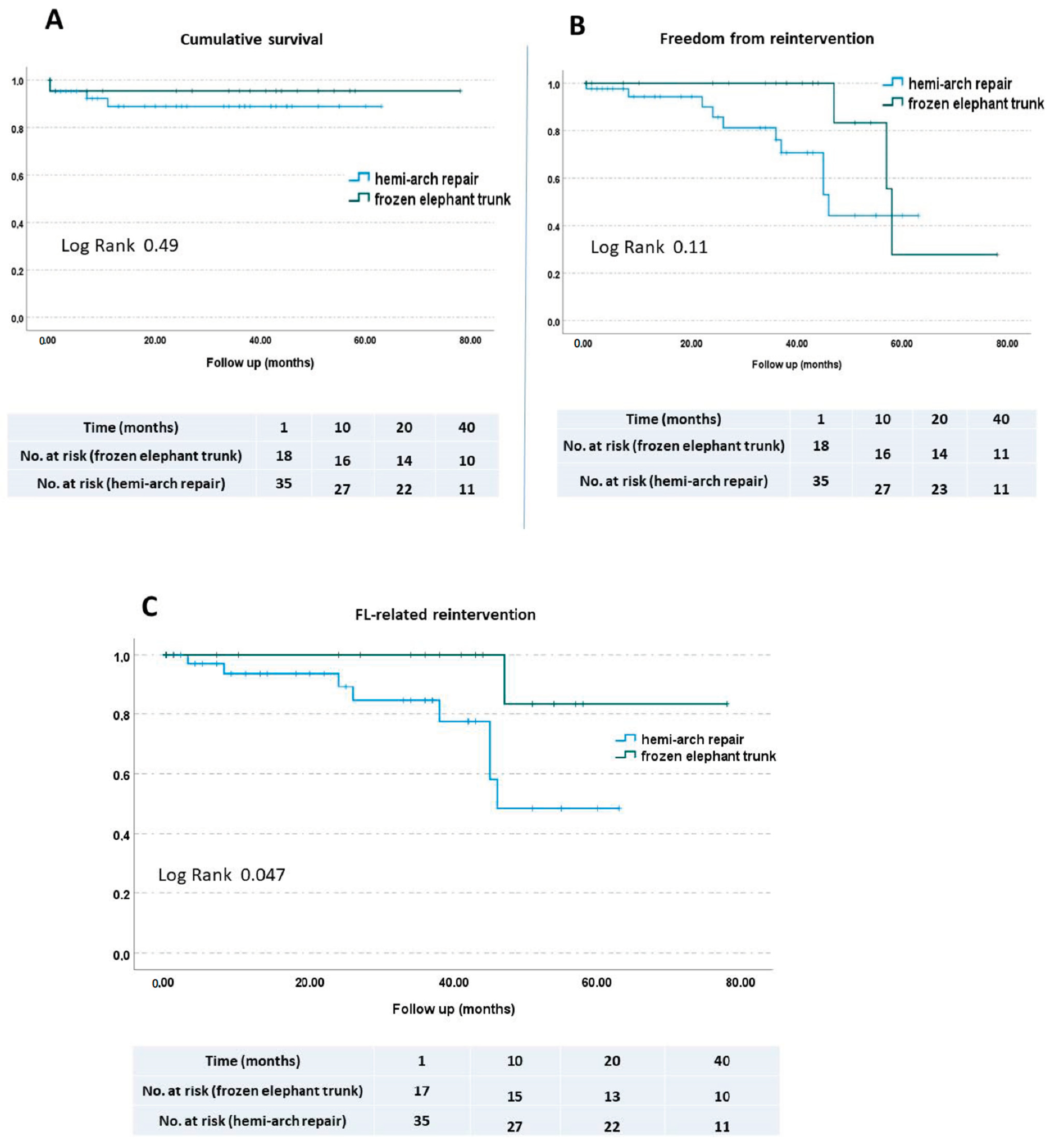
2.3. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rylski, B.; Beyersdorf, F.; Blanke, P.; Boos, A.; Hoffmann, I.; Dashkevich, A.; Siepe, M. Supracoronary ascending aortic replacement in patients with acute aortic dissection type A: What happens to the aortic root in the long run? J. Thorac. Cardiovasc. Surg. 2013, 146, 285–290. [Google Scholar] [CrossRef] [PubMed]
- Pacini, D.; Tsagakis, K.; Jakob, H.; Mestres, C.A.; Armaro, A.; Weiss, G.; Grabenwoger, M.; Borger, M.A.; Mohr, F.W.; Bonser, R.S.; et al. The frozen elephant trunk for the treatment of chronic dissection of the thoracic aorta: A multicenter experience. Ann. Thorac. Surg. 2011, 92, 1663–1670. [Google Scholar] [CrossRef] [PubMed]
- Murana, G.; Castrovinci, S.; Kloppenburg, G.; Yousif, A.; Kelder, H.; Schepens, M.; de Maat, G.; Sonker, U.; Morshuis, W.; Heijmen, R. Open thoracoabdominal aortic aneurysm repair in the modern era: Results from a 20-year single-centre experience. Eur. J. Cardiothorac. Surg. 2016, 49, 1374–1381. [Google Scholar] [CrossRef] [PubMed]
- Takagi, H.; Umemoto, T.; ALICE Group. A Meta-Analysis of Total Arch Replacement with Frozen Elephant Trunk in Acute Type A Aortic Dissection. Vasc. Endovascular. Surg. 2016, 50, 33–46. [Google Scholar] [CrossRef]
- Shrestha, M.; Martens, A.; Kaufeld, T.; Beckmann, E.; Bertele, S.; Krueger, H.; Neuser, J.; Fleissner, F.; Ius, F.; Abd Alhadi, F.; et al. Single-centre experience with the frozen elephant trunk technique in 251 patients over 15 years. Eur. J. Cardiothorac. Surg. 2017, 52, 858–866. [Google Scholar] [CrossRef] [PubMed]
- Usai, M.V.; Ibrahim, A.; Oberhuber, A.; Dell’Aquila, A.M.; Martens, S.; Motekallemi, A.; Rukosujew, A. Quantification of volume changes in the descending aorta after frozen elephant trunk procedure using the Thoraflex hybrid prosthesis for type A aortic dissection. J. Thorac. Dis 2020, 13, 60. [Google Scholar] [CrossRef] [PubMed]
- Di Marco, L.; Pacini, D.; Leone, A.; Pantaleo, A.; Murana, G.; Di Bartolomeo, R. La tecnica del “frozen elephant trunk” nel trattamento delle lesioni complesse dell’aorta toracica [The frozen elephant trunk technique for the treatment of complex lesions of the thoracic aorta]. G. Ital. Cardiol. 2017, 18, 631–637. (In Italian) [Google Scholar]
- Shrestha, M.; Bachet, J.; Bavaria, J.; Carrel, T.P.; De Paulis, R.; Di Bartolomeo, R.; Etz, C.D.; Grabenwöger, M.; Grimm, M.; Haverich, A.; et al. Current status and recommendations for use of the frozen elephant trunk technique: A position paper by the Vascular Domain of EACTS. Eur. J. Cardiothorac. Surg. 2015, 47, 759–769. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, M.; Pichlmaier, M.; Martens, A.; Hagl, C.; Khaladj, N.; Haverich, A. Total aortic arch replacement with a novel four-branched frozen elephant trunk graft: First-in-man results. Eur. J. Cardiothorac. Surg. 2013, 43, 406–410. [Google Scholar] [CrossRef] [PubMed]
- Leontyev, S.; Misfeld, M.; Daviewala, P.; Borger, M.A.; Etz, C.D.; Belaev, S.; Seeburger, J.; Holzhey, D.; Bakhtiary, F.; Mohr, F.W. Early- and medium-term results after aortic arch replacement with frozen elephant trunk techniques-a single center study. Ann. Cardiothorac. Surg. 2013, 2, 606–611. [Google Scholar] [PubMed]
- Rylski, B.; Blanke, P.; Beyersdorf, F.; Desai, N.D.; Milewski, R.K.; Siepe, M.; Kari, F.A.; Czerny, M.; Carrel, T.; Schlensak, C.; et al. How does the ascending aorta geometry change when it dissects? J. Am. Coll. Cardiol. 2014, 63, 1311–1319. [Google Scholar] [CrossRef] [PubMed]
- Dohle, D.S.; Tsagakis, K.; Janosi, R.A.; Benedik, J.; Kühl, H.; Penkova, L.; Stebner, F.; Wendt, D.; Jakob, H. Aortic remodelling in aortic dissection after frozen elephant trunk. Eur. J. Cardiothorac. Surg. 2016, 49, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Katayama, A.; Uchida, N.; Katayama, K.; Arakawa, M.; Sueda, T. The frozen elephant trunk technique for acute type A aortic dissection: Results from 15 years of experience. Eur. J. Cardiothorac. Surg. 2015, 47, 355–360, discussion 360. [Google Scholar] [CrossRef]
- Fattouch, K.; Sampognaro, R.; Navarra, E.; Caruso, M.; Pisano, C.; Coppola, G.; Speziale, G.; Ruvolo, G. Long-term results after repair of type A acute aortic dissection according to false lumen patency. Ann. Thorac. Surg. 2009, 88, 1244–1250. [Google Scholar] [CrossRef]
- Pacini, D.; Murana, G.; Di Marco, L.; Di Bartolomeo, R. Aortic remodeling in acute type A aortic dissection after frozen elephant trunk implantation. Indian J. Thorac. Cardiovasc. Surg. 2019, 35 (Suppl. S2), 112–117. [Google Scholar] [CrossRef] [PubMed]
- Uchida, N.; Katayama, A.; Tamura, K.; Sutoh, M.; Kuraoka, M.; Ishihara, H. Frozen elephant trunk technique and partial remodeling for acute type A aortic dissection. Eur. J. Cardiothorac. Surg. 2011, 40, 1066–1071. [Google Scholar] [CrossRef] [PubMed]
- Rathore, K.S. Distal Aortic Remodeling after Type A Dissection Repair: An Ongoing Mirage. J. Chest. Surg. 2021, 54, 439–448. [Google Scholar] [CrossRef] [PubMed]
- Manenti, A.; Roncati, L.; Manco, G. Inside Pathophysiology of Thoracic Aorta Grafts. Ann. Thorac. Surg. 2022, 114, 1098. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Overall (66) | FET (n = 22) | CAR (n = 44) | Significance | |
|---|---|---|---|---|
| Demographic characteristics | ||||
| Age (years), mean ± SD | 61.25 ± 10.79 | 56.95 ± 9.4 | 63.65 ± 11 | 0.063 |
| Female gender, n (%) | 18 (7.2) | 2 (9) | 16 (36.3) | 0.038 |
| Body mass index (kg/m2), | 26.45 ± 5.36 | 25.5 ± 3.95 | 28 ± 5.9 | 0.287 |
| Medical history, n (%) | ||||
| Hypertension | 50 (75.7) | 15 (68.1) | 35 (79.5) | 0.367 |
| Previous stroke/TIA | 7 (10.6) | 3 (13.6) | 4 (9) | 0.678 |
| COPD | 5 (7.5) | 1 (4.5) | 4 (9) | 0.658 |
| NYHA III or NYHA IV | 7 (10.6) | 0 (0) | 7 (15.9) | 0.086 |
| Current/previous smoker | 21 (31.8) | 6 (27.2) | 15 (34) | 0.078 |
| Atrial fibrillation | 10 (15.1) | 2 (9) | 8 (18.1) | 0.476 |
| previous cardiac surgery | 4 (6) | 0 (0) | 4 (9) | 0.293 |
| Overall | FET | CET | Significance | |
|---|---|---|---|---|
| True lumen in cm3, median (IQR) | ||||
| Preoperative | 63.8 (29–732) | 58.5 (29.5–732) | 66.5 (29–226) | 0.908 |
| At discharge | 78.1 (30–268) | 85 (39.9–181) | 76 (30–268) | 0.416 |
| 12 months | 102 (27–283) | 107 (51–179) | 94.9 (27–283) | 0.422 |
| 24 months | 100 (27–319) | 133 (93.4–168) | 96 (27–319) | 0.268 |
| False lumen in cm3, median (IQR) | ||||
| Preoperative | 144.5 (37–336) | 137 (53–336) | 147 (37–300) | 0.772 |
| At discharge | 158 (34–459) | 153 (34–459) | 162 (43–326) | 0.522 |
| 12 months | 169 (42–392) | 142 (49–261) | 187 (42–392) | 0.222 |
| 24 months | 162 (93.4–495) | 133 (93.4–168) | 190 (95.5–495) | 0.020 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ibrahim, A.; Motekallemi, A.; Yahia, A.; Oberhuber, A.; Eierhoff, T.; Martens, S.; Marchiori, E.; Rukosujew, A. Volume Changes in the Descending Aorta after Frozen Elephant Trunk and Conventional Hemi-Arch Repair after Acute Type A Aortic Dissection. Diagnostics 2022, 12, 2524. https://doi.org/10.3390/diagnostics12102524
Ibrahim A, Motekallemi A, Yahia A, Oberhuber A, Eierhoff T, Martens S, Marchiori E, Rukosujew A. Volume Changes in the Descending Aorta after Frozen Elephant Trunk and Conventional Hemi-Arch Repair after Acute Type A Aortic Dissection. Diagnostics. 2022; 12(10):2524. https://doi.org/10.3390/diagnostics12102524
Chicago/Turabian StyleIbrahim, Abdulhakim, Arash Motekallemi, Ahmed Yahia, Alexander Oberhuber, Thorsten Eierhoff, Sven Martens, Elena Marchiori, and Andreas Rukosujew. 2022. "Volume Changes in the Descending Aorta after Frozen Elephant Trunk and Conventional Hemi-Arch Repair after Acute Type A Aortic Dissection" Diagnostics 12, no. 10: 2524. https://doi.org/10.3390/diagnostics12102524
APA StyleIbrahim, A., Motekallemi, A., Yahia, A., Oberhuber, A., Eierhoff, T., Martens, S., Marchiori, E., & Rukosujew, A. (2022). Volume Changes in the Descending Aorta after Frozen Elephant Trunk and Conventional Hemi-Arch Repair after Acute Type A Aortic Dissection. Diagnostics, 12(10), 2524. https://doi.org/10.3390/diagnostics12102524