
HtrA1 in Gestational Diabetes Mellitus: A Possible Biomarker?

 , , ,
, , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Exclusion Criteria
2.2. Plasma Collection and HtrA1 ELISA
2.3. Statistical Analysis
3. Results
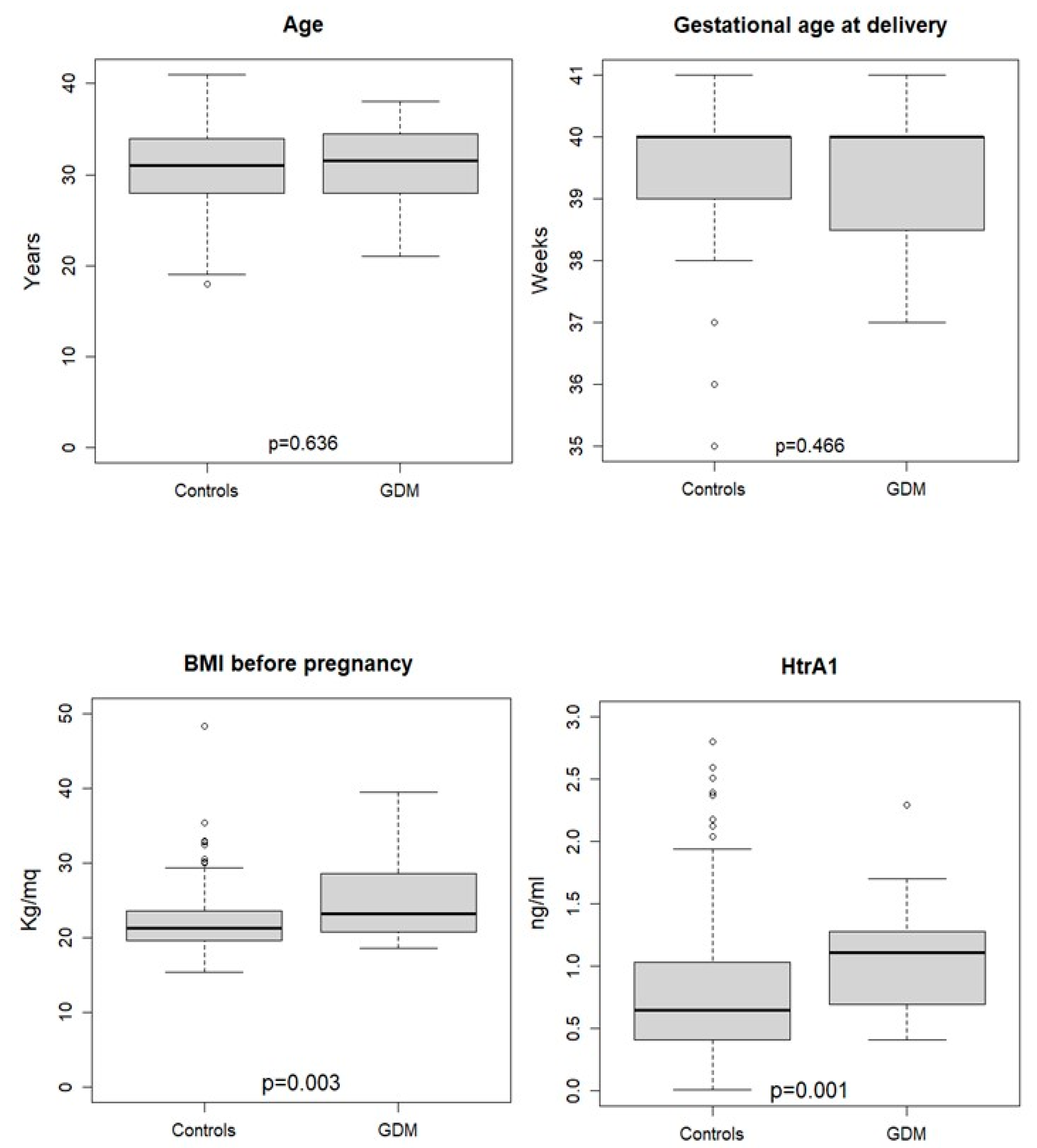
3.1. HtrA1 Plasma Concentrations Are Increased in Third Trimester of Pregnancy with GDM
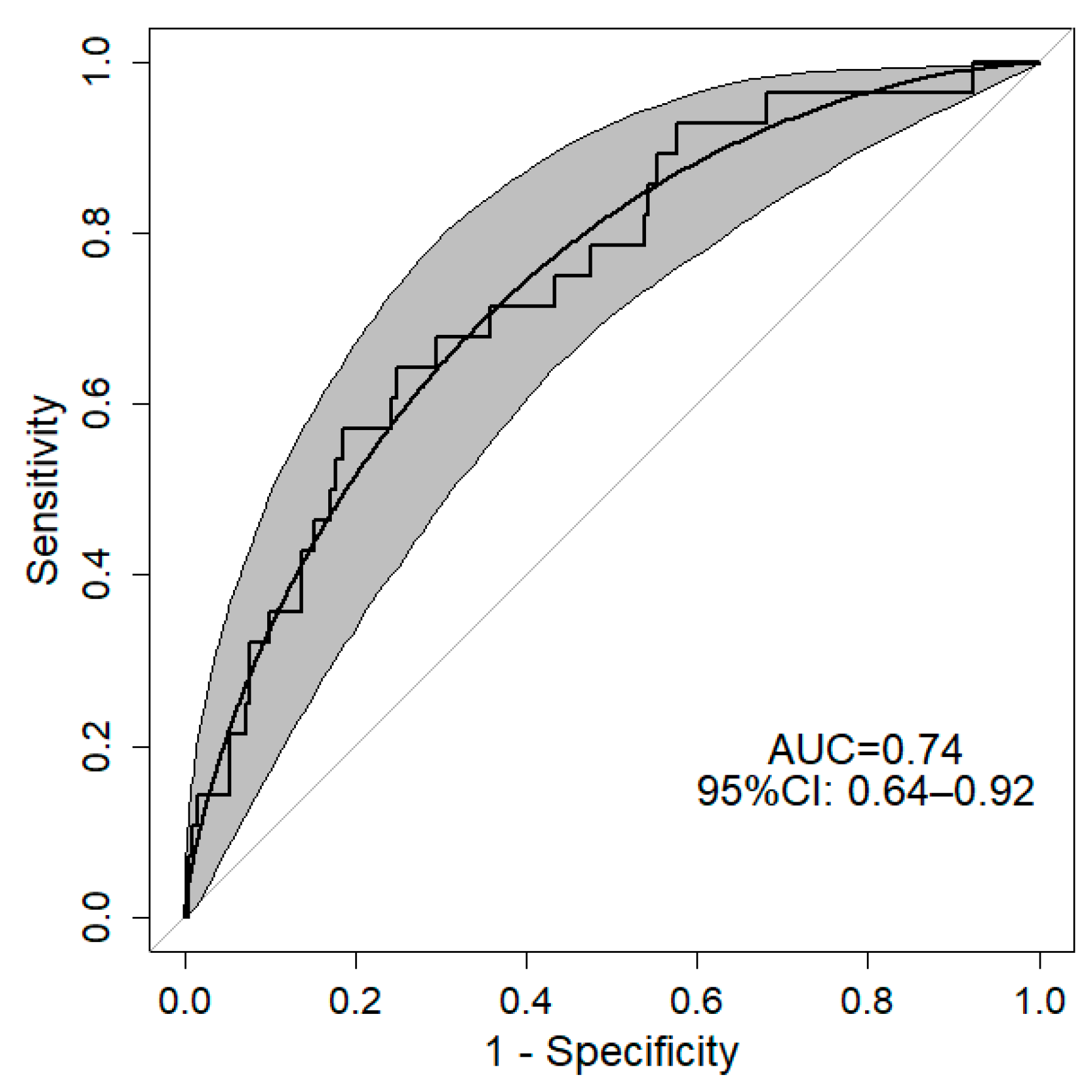
3.2. HtrA1 Could Be an Early Marker of GDM in First Trimester of Pregnancy
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Behboudi-Gandevani, S.; Amiri, M.; Bidhendi Yarandi, R.; Ramezani Tehrani, F. The impact of diagnostic criteria for gestational diabetes on its prevalence: A systematic review and meta-analysis. Diabetol. Metab. Syndr. 2019, 11, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hod, M.; Kapur, A.; Sacks, D.A.; Hadar, E.; Agarwal, M.; Di Renzo, G.C.; Roura, L.C.; McIntyre, H.D.; Morris, J.L.; Divakar, H. The International Federation of Gynecology and Obstetrics (FIGO) Initiative on gestational diabetes mellitus: A pragmatic guide for diagnosis, management, and care. Int. J. Gynaecol. Obstet. 2015, 131 (Suppl. S3), S173–S211. [Google Scholar] [CrossRef] [Green Version]
- Kapur, A.; McIntyre, H.D.; Divakar, H.; Di Renzo, G.C.; Kihara, A.B.; McAuliffe, F.; Hanson, M.; Ma, R.C.; Hod, M.; FIGO Working Group on Hyperglycemia in Pregnancy. Towards a global consensus on GDM diagnosis: Light at the end of the tunnel? Int. J. Gynaecol. Obstet. 2020, 149, 257–261. [Google Scholar] [CrossRef] [PubMed]
- Chiefari, E.; Arcidiacono, B.; Foti, D.; Brunetti, A. Gestational diabetes mellitus: An updated overview. J. Endocrinol. Investig. 2017, 40, 899–909. [Google Scholar] [CrossRef] [PubMed]
- Plows, J.F.; Stanley, J.L.; Baker, P.N.; Reynolds, C.M.; Vickers, M.H. The Pathophysiology of Gestational Diabetes Mellitus. Int. J. Mol. Sci. 2018, 19, 3342. [Google Scholar] [CrossRef] [Green Version]
- Guo, Z.; Pan, J.; Zhu, H.; Chen, Z.Y. Metabolites of Gut Microbiota and Possible Implication in Development of Diabetes Mellitus. J. Agric. Food Chem. 2022, 70, 5945–5960. [Google Scholar] [CrossRef]
- Mishra, J.; Srivastava, S.K.; Pandey, K.B. Compromised Renal and Hepatic Functions and Unsteady Cellular Redox State during Preeclampsia and Gestational Diabetes Mellitus. Arch. Med. Res. 2021, 52, 635–640. [Google Scholar] [CrossRef]
- Vigers, T.; Vinovskis, C.; Li, L.P.; Prasad, P.; Heerspink, H.; D′Alessandro, A.; Reisz, J.A.; Piani, F.; Cherney, D.Z.; van Raalte, D.H.; et al. Plasma levels of carboxylic acids are markers of early kidney dysfunction in young people with type 1 diabetes. Pediatr. Nephrol. 2022; Online ahead of print. [Google Scholar] [CrossRef]
- Piani, F.; Reinicke, T.; Borghi, C.; Tommerdahl, K.L.; Cara-Fuentes, G.; Johnson, R.J.; Bjornstad, P. Acute Kidney Injury in Pediatric Diabetic Kidney Disease. Front. Pediatr. 2021, 9, 668033. [Google Scholar] [CrossRef]
- Farahvar, S.; Walfisch, A.; Sheiner, E. Gestational diabetes risk factors and long-term consequences for both mother and offspring: A literature review. Expert Rev. Endocrinol. Metab. 2019, 14, 63–74. [Google Scholar] [CrossRef]
- Altobelli, E.; Latella, G.; Morroni, M.; Licini, C.; Tossetta, G.; Mazzucchelli, R.; Profeta, V.F.; Coletti, G.; Leocata, P.; Castellucci, M.; et al. Low HtrA1 expression in patients with longstanding ulcerative colitis and colorectal cancer. Oncol. Rep. 2017, 38, 418–426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rallis, K.S.; Corrigan, A.E.; Dadah, H.; Stanislovas, J.; Zamani, P.; Makker, S.; Szabados, B.; Sideris, M. IL-10 in cancer: An essential thermostatic regulator between homeostatic immunity and inflammation—A comprehensive review. Future Oncol. 2022, 18, 29. [Google Scholar] [CrossRef] [PubMed]
- Meehan, E.V.; Wang, K. Interleukin-17 Family Cytokines in Metabolic Disorders and Cancer. Genes 2022, 13, 1643. [Google Scholar] [CrossRef] [PubMed]
- Marinelli Busilacchi, E.; Costantini, A.; Mancini, G.; Tossetta, G.; Olivieri, J.; Poloni, A.; Viola, N.; Butini, L.; Campanati, A.; Goteri, G.; et al. Nilotinib Treatment of Patients Affected by Chronic Graft-versus-Host Disease Reduces Collagen Production and Skin Fibrosis by Downmodulating the TGF-beta and p-SMAD Pathway. Biol. Blood Marrow Transpl. 2020, 26, 823–834. [Google Scholar] [CrossRef] [PubMed]
- Alston, M.C.; Redman, L.M.; Sones, J.L. An Overview of Obesity, Cholesterol, and Systemic Inflammation in Preeclampsia. Nutrients 2022, 14, 2087. [Google Scholar] [CrossRef]
- Welch, B.M.; McNell, E.E.; Edin, M.L.; Ferguson, K.K. Inflammation and oxidative stress as mediators of the impacts of environmental exposures on human pregnancy: Evidence from oxylipins. Pharmacol. Ther. 2022, 239, 108181. [Google Scholar] [CrossRef]
- Cecati, M.; Sartini, D.; Campagna, R.; Biagini, A.; Ciavattini, A.; Emanuelli, M.; Giannubilo, S.R. Molecular analysis of endometrial inflammation in preterm birth. Cell Mol. Biol. 2017, 63, 51–57. [Google Scholar] [CrossRef]
- Tossetta, G.; Fantone, S.; Giannubilo, S.R.; Marzioni, D. The Multifaced Actions of Curcumin in Pregnancy Outcome. Antioxidants 2021, 10, 126. [Google Scholar] [CrossRef]
- Pietzner, M.; Kaul, A.; Henning, A.K.; Kastenmuller, G.; Artati, A.; Lerch, M.M.; Adamski, J.; Nauck, M.; Friedrich, N. Comprehensive metabolic profiling of chronic low-grade inflammation among generally healthy individuals. BMC Med. 2017, 15, 210. [Google Scholar] [CrossRef] [Green Version]
- Bernea, E.G.; Suica, V.I.; Uyy, E.; Cerveanu-Hogas, A.; Boteanu, R.M.; Ivan, L.; Ceausu, I.; Mihai, D.A.; Ionescu-Tirgoviste, C.; Antohe, F. Exosome Proteomics Reveals the Deregulation of Coagulation, Complement and Lipid Metabolism Proteins in Gestational Diabetes Mellitus. Molecules 2022, 27, 5502. [Google Scholar] [CrossRef]
- Fantone, S.; Giannubilo, S.R.; Marzioni, D.; Tossetta, G. HTRA family proteins in pregnancy outcome. Tissue Cell 2021, 72, 101549. [Google Scholar] [CrossRef] [PubMed]
- De Luca, A.; De Falco, M.; Fedele, V.; Cobellis, L.; Mastrogiacomo, A.; Laforgia, V.; Tuduce, I.L.; Campioni, M.; Giraldi, D.; Paggi, M.G.; et al. The serine protease HtrA1 is upregulated in the human placenta during pregnancy. J. Histochem. Cytochem. 2004, 52, 885–892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nie, G.Y.; Li, Y.; Minoura, H.; Batten, L.; Ooi, G.T.; Findlay, J.K.; Salamonsen, L.A. A novel serine protease of the mammalian HtrA family is up-regulated in mouse uterus coinciding with placentation. Mol. Hum. Reprod. 2003, 9, 279–290. [Google Scholar] [CrossRef] [Green Version]
- De Luca, A.; De Falco, M.; Severino, A.; Campioni, M.; Santini, D.; Baldi, F.; Paggi, M.G.; Baldi, A. Distribution of the serine protease HtrA1 in normal human tissues. J. Histochem. Cytochem. 2003, 51, 1279–1284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tossetta, G.; Fantone, S.; Licini, C.; Marzioni, D.; Mattioli-Belmonte, M. The multifaced role of HtrA1 in the development of joint and skeletal disorders. Bone 2022, 157, 116350. [Google Scholar] [CrossRef] [PubMed]
- Tossetta, G.; Avellini, C.; Licini, C.; Giannubilo, S.R.; Castellucci, M.; Marzioni, D. High temperature requirement A1 and fibronectin: Two possible players in placental tissue remodelling. Eur. J. Histochem. 2016, 60, 2724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goteri, G.; Altobelli, E.; Tossetta, G.; Zizzi, A.; Avellini, C.; Licini, C.; Lorenzi, T.; Castellucci, M.; Ciavattini, A.; Marzioni, D. High temperature requirement A1, transforming growth factor beta1, phosphoSmad2 and Ki67 in eutopic and ectopic endometrium of women with endometriosis. Eur. J. Histochem. 2015, 59, 2570. [Google Scholar] [CrossRef] [Green Version]
- Carrasco-Wong, I.; Moller, A.; Giachini, F.R.; Lima, V.V.; Toledo, F.; Stojanova, J.; Sobrevia, L.; San Martin, S. Placental structure in gestational diabetes mellitus. Biochim. Biophys. Acta. Mol. Basis Dis. 2020, 1866, 165535. [Google Scholar] [CrossRef]
- Gesuita, R.; Licini, C.; Picchiassi, E.; Tarquini, F.; Coata, G.; Fantone, S.; Tossetta, G.; Ciavattini, A.; Castellucci, M.; Di Renzo, G.C.; et al. Association between first trimester plasma htra1 level and subsequent preeclampsia: A possible early marker? Pregnancy Hypertens 2019, 18, 58–62. [Google Scholar] [CrossRef]
- Giannubilo, S.R.; Licini, C.; Picchiassi, E.; Tarquini, F.; Coata, G.; Fantone, S.; Tossetta, G.; Ciavattini, A.; Castellucci, M.; Giardina, I.; et al. First trimester HtrA1 maternal plasma level and spontaneous preterm birth. J. Matern Fetal Neonatal. Med. 2022, 35, 780–784. [Google Scholar] [CrossRef]
- Marzioni, D.; Quaranta, A.; Lorenzi, T.; Morroni, M.; Crescimanno, C.; De Nictolis, M.; Toti, P.; Muzzonigro, G.; Baldi, A.; De Luca, A.; et al. Expression pattern alterations of the serine protease HtrA1 in normal human placental tissues and in gestational trophoblastic diseases. Histol. Histopathol. 2009, 24, 1213–1222. [Google Scholar] [CrossRef] [PubMed]
- Hasan, M.Z.; Ikawati, M.; Tocharus, J.; Kawaichi, M.; Oka, C. Abnormal development of placenta in HtrA1-deficient mice. Dev. Biol. 2015, 397, 89–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chi, C.; Loy, S.L.; Chan, S.Y.; Choong, C.; Cai, S.; Soh, S.E.; Tan, K.H.; Yap, F.; Gluckman, P.D.; Godfrey, K.M.; et al. Impact of adopting the 2013 World Health Organization criteria for diagnosis of gestational diabetes in a multi-ethnic Asian cohort: A prospective study. BMC Pregnancy Childbirth 2018, 18, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esakoff, T.F.; Guillet, A.; Caughey, A.B. Does small for gestational age worsen outcomes in gestational diabetics? J. Matern. Fetal Neonatal Med. 2017, 30, 890–893. [Google Scholar] [CrossRef]
- Marzioni, D.; Lorenzi, T.; Altobelli, E.; Giannubilo, S.R.; Paolinelli, F.; Tersigni, C.; Crescimanno, C.; Monsurro, V.; Tranquilli, A.L.; Di Simone, N.; et al. Alterations of maternal plasma HTRA1 level in preeclampsia complicated by IUGR. Placenta 2012, 33, 1036–1038. [Google Scholar] [CrossRef]
- Sahin, M.; Oguz, A.; Tuzun, D.; Isiktas, O.; Isiktas, S.; Ulgen, C.; Sahin, H.; Gul, K. A new marker predicting gestational diabetes mellitus: First trimester neutrophil/lymphocyte ratio. Medicine 2022, 101, e30514. [Google Scholar] [CrossRef]
- Hromadnikova, I.; Kotlabova, K.; Krofta, L. Cardiovascular Disease-Associated MicroRNAs as Novel Biomarkers of First-Trimester Screening for Gestational Diabetes Mellitus in the Absence of Other Pregnancy-Related Complications. Int. J. Mol. Sci. 2022, 23, 10635. [Google Scholar] [CrossRef]
- Sharma, A.K.; Singh, S.; Singh, H.; Mahajan, D.; Kolli, P.; Mandadapu, G.; Kumar, B.; Kumar, D.; Kumar, S.; Jena, M.K. Deep Insight of the Pathophysiology of Gestational Diabetes Mellitus. Cells 2022, 11, 2672. [Google Scholar] [CrossRef]
- Gu, J.; Geng, K.; Guo, M.; Huang, W.; Zhao, T.; Li, X.; Xu, Y.H.; Xu, Y. Targeting Pyroptosis: New Insights into the Treatment of Diabetic Microvascular Complications. Evid. Based Complement Altern. Med. 2022, 2022, 5277673. [Google Scholar] [CrossRef]
- Tenenbaum-Gavish, K.; Sharabi-Nov, A.; Binyamin, D.; Moller, H.J.; Danon, D.; Rothman, L.; Hadar, E.; Idelson, A.; Vogel, I.; Koren, O.; et al. First trimester biomarkers for prediction of gestational diabetes mellitus. Placenta 2020, 101, 80–89. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Healthy Pregnancies (n = 20) | Pregnancies with GDM (n = 20) | p | |
|---|---|---|---|
| Maternal age (years) | 32 (30;36) | 36 (35;39) | 0.006 |
| BMI (Kg/m2) | 24 (22;25) | 21 (21;25) | 0.229 |
| Gestational age at delivery (Weeks) | 40 (38;41) | 39 (39;40) | 0.107 |
| Gestational Age at sampling (Weeks) | 34 (31;36) | 36 (32;37) | 0.124 |
| HtrA1 (ng/mL) | 1.9 (0.8;4.0) | 4.3 (3.4;6.0) | 0.004 |
| Birth weight (Kg) | 3.5 (3.3;3.6) | 3.2 (2.8;3.4) | 0.041 |
| Healthy Pregnancies (n = 210) | Pregnancies with GDM (n = 28) | p | |
|---|---|---|---|
| Smoking (yes) | 55 (26.2%) | 7 (25.0%) | 0.999 |
| Low/poor nutrition | 137 (65.2%) | 14 (50.0%) | 0.173 |
| Physical activity (yes) | 140 (66.7%) | 19 (67.9%) | 0.999 |
| OR | 95% CI | p | |
|---|---|---|---|
| HtrA1 (ng/mL) | 2.50 | 1.2; 5.16 | 0.013 |
| Maternal age (years) | 1.02 | 0.93; 1.13 | 0.628 |
| BMI before pregnancy (kg/m2) | 1.14 | 1.05; 1.25 | 0.002 |
| Gestational age (weeks) | 0.90 | 0.63; 1.29 | 0.540 |
| Nutrition (good vs. poor/low) | 0.57 | 0.34; 0.95 | 0.036 |
| Smoke (yes vs. no) | 0.91 | 0.33; 2.29 | 0.849 |
| Physical activity (yes vs. no) | 1.42 | 0.58; 3.75 | 0.457 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tossetta, G.; Fantone, S.; Gesuita, R.; Di Renzo, G.C.; Meyyazhagan, A.; Tersigni, C.; Scambia, G.; Di Simone, N.; Marzioni, D. HtrA1 in Gestational Diabetes Mellitus: A Possible Biomarker? Diagnostics 2022, 12, 2705. https://doi.org/10.3390/diagnostics12112705
Tossetta G, Fantone S, Gesuita R, Di Renzo GC, Meyyazhagan A, Tersigni C, Scambia G, Di Simone N, Marzioni D. HtrA1 in Gestational Diabetes Mellitus: A Possible Biomarker? Diagnostics. 2022; 12(11):2705. https://doi.org/10.3390/diagnostics12112705
Chicago/Turabian StyleTossetta, Giovanni, Sonia Fantone, Rosaria Gesuita, Gian Carlo Di Renzo, Arun Meyyazhagan, Chiara Tersigni, Giovanni Scambia, Nicoletta Di Simone, and Daniela Marzioni. 2022. "HtrA1 in Gestational Diabetes Mellitus: A Possible Biomarker?" Diagnostics 12, no. 11: 2705. https://doi.org/10.3390/diagnostics12112705
APA StyleTossetta, G., Fantone, S., Gesuita, R., Di Renzo, G. C., Meyyazhagan, A., Tersigni, C., Scambia, G., Di Simone, N., & Marzioni, D. (2022). HtrA1 in Gestational Diabetes Mellitus: A Possible Biomarker? Diagnostics, 12(11), 2705. https://doi.org/10.3390/diagnostics12112705