
Prognostic Comparison between Oncotype DX® and a 23-Gene Classifier, RecurIndex®, on the Taiwan Breast Cancer Population
 , ,
, ,
Abstract
:1. Introduction
2. Methods and Materials
2.1. Study Population
2.2. RecurIndex, 23-Gene Classifier
2.3. Determination of Cut-Off Values
2.4. Clinical Performance and Concordance between Oncotype DX® and the 23-Gene Classifier
3. Results
3.1. Characteristics of the Study Population
3.2. Patient Characteristics as Determined by the 23-Gene Classifier
3.3. Patient Characteristics as Determined by the Oncotype DX®
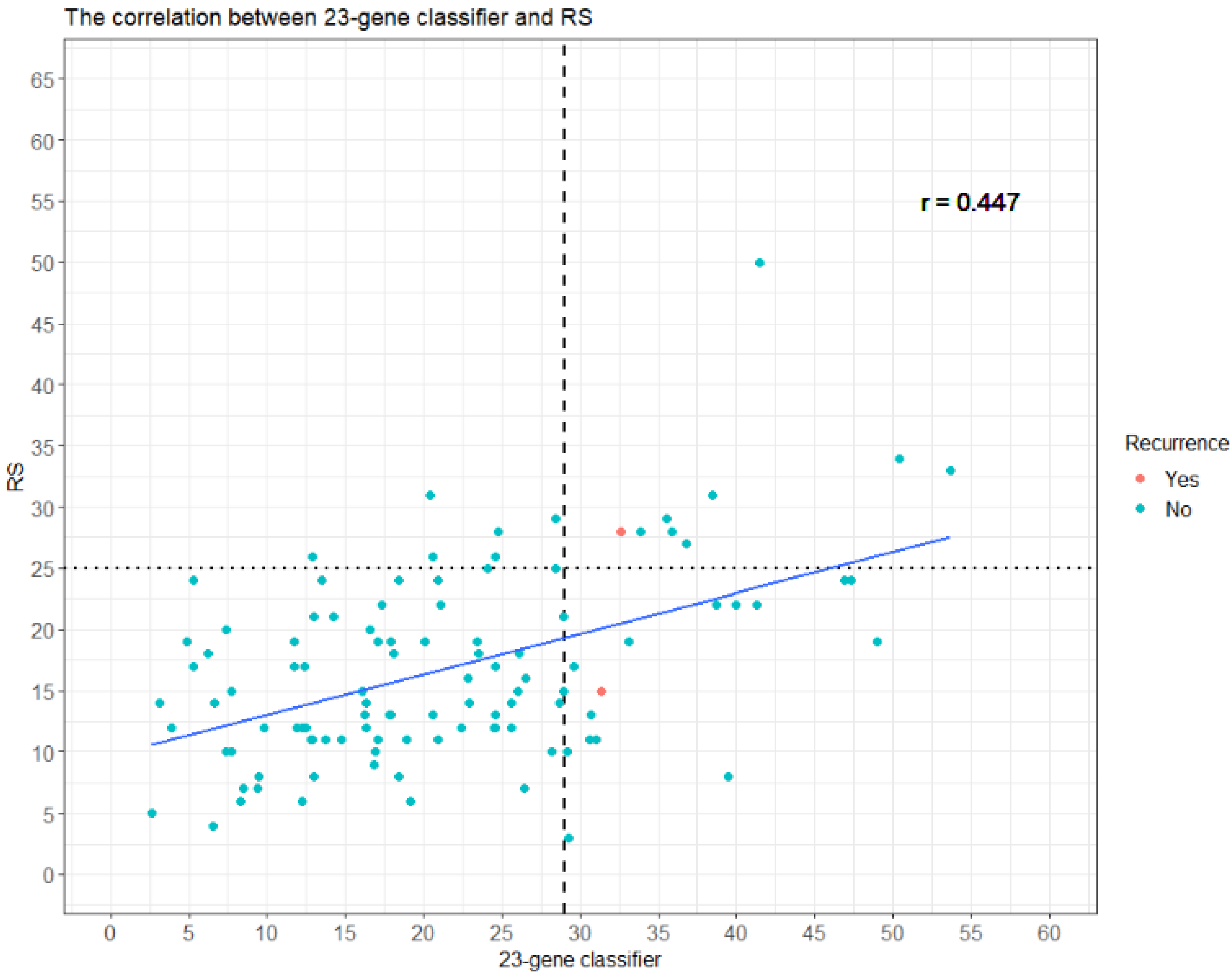
3.4. Clinical Performance of the 23-Gene Classifier RI and Oncotype DX® RS
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Brayn, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Dignam, J.J.; Dukic, V.; Anderson, S.J.; Mamounas, E.P.; Wickerham, D.L.; Wolmark, N. Hazard of recurrence and adjuvant treatment effects over time in lymph node-negative breast cancer. Breast Cancer Res. Treat. 2009, 116, 595–602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, S.H.-C.; Yu, B.-L.; Horng, C.-F.; Tsai, S.Y.; Chen, C.-M.; Chu, N.-M.; Tsou, M.H.; Lin, C.K.; Shih, L.S.; Liu, M.C. Long-term survival and stage I breast cancer subtypes. J. Cancer Res. Pract. 2016, 3, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Esserman, L.J.; Thompson, I.M.; Reid, B. Overdiagnosis and overtreatment in cancer: An opportunity for improvement. JAMA 2013, 310, 797–798. [Google Scholar] [CrossRef] [PubMed]
- Sparano, J.A.; Gray, R.J.; Makower, D.F.; Pritchard, K.I.; Albain, K.S.; Hayes, D.F.; Geyer, C.E., Jr.; Dees, E.C.; Goetz, M.P.; Olson, J.A., Jr.; et al. Adjuvant Chemotherapy Guided by a 21-Gene Expression Assay in Breast Cancer. N. Engl. J. Med. 2018, 379, 111–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, L.N.; Ismaila, N.; McShane, L.M.; Andre, F.; Collyar, D.E.; Gonzalez-Angulo, A.M.; Hammond, E.H.; Kuderer, N.M.; Liu, M.C.; Mennel, R.G.; et al. Use of biomarkers to guide decisions on adjuvant systemic therapy for women with early-stage invasive breast cancer: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2016, 34, 1134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iqbal, J.; Ginsburg, O.; Rochon, P.A.; Sun, P.; Narod, S.A. Differences in breast cancer stage at diagnosis and cancer-specific survival by race and ethnicity in the United States. JAMA 2015, 313, 165–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeo, W.; Ueno, T.; Lin, C.H.; Liu, Q.; Lee, K.H.; Leung, R.; Naito, Y.; Park, Y.H.; Im, S.A.; Li, H.; et al. Asian Breast Cancer Cooperative Group. Treating HR+/HER2- breast cancer in premenopausal Asian women: Asian Breast Cancer Cooperative Group 2019 Consensus and position on ovarian suppression. Breast Cancer Res. Treat. 2019, 177, 549–559. [Google Scholar] [CrossRef] [PubMed]
- Hoskins, K.F.; Danciu, O.C.; Ko, N.Y.; Calip, G.S. Association of Race/Ethnicity and the 21-Gene Recurrence Score with Breast Cancer-Specific Mortality Among US Women. JAMA Oncol. 2021, 7, 370–378. [Google Scholar] [CrossRef] [PubMed]
- Cheng, S.H.; Horng, C.F.; West, M.; Huang, E.; Pittman, J.; Tsou, M.H.; Dressman, H.; Chen, C.M.; Tsai, S.Y.; Jian, J.J.; et al. Genomic prediction of locoregional recurrence after mastectomy in breast cancer. J. Clin. Oncol. 2006, 24, 4594–4602. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.H.; Chiu, J.Y.; Shih, K.H. A 23-gene prognostic classifier for prediction of recurrence and survival for Asian breast cancer patients. Biosci. Rep. 2020, 40, BSR20202794. [Google Scholar] [CrossRef] [PubMed]
- Cheng, S.H.; Huang, T.T.; Cheng, Y.H.; Tan, T.B.K.; Horng, C.F.; Wang, Y.A.; Brian, N.S.; Shih, L.S.; Yu, B.L. Validation of the 18-gene classifier as a prognostic biomarker of distant metastasis in breast cancer. PLoS ONE 2017, 12, e0184372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, P.S.; Lee, Y.H.; Chung, C.F.; Chang, Y.C.; Wang, M.Y.; Lo, C.; Tsai, L.W.; Shih, K.H.; Lei, J.; Yu, B.L.; et al. A preliminary report of head-to-head comparison of 18-gene-based clinical-genomic model and oncotype DX 21-gene assay for predicting recurrence of early-stage breast cancer. Jpn. J. Clin. Oncol. 2019, 49, 1029–1036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagalla, S.; Chou, J.W.; Willingham, M.C.; Ruiz, J.; Vaughn, J.P.; Dubey, P.; Lash, T.L.; Hamilton-Dutoit, S.J.; Bergh, J.; Sotiriou, C.; et al. Interactions between immunity, proliferation and molecular subtype in breast cancer prognosis. Genome Biol. 2013, 14, R34. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Variable | Patient Number |
|---|---|
| Age, mean (SD) | 51.79 (11.05) |
| Nodal stage | |
| N0 | 84 (76.36%) |
| N1 | 26 (23.64%) |
| Grade | |
| I | 20 (18.18%) |
| II | 82 (74.55%) |
| III | 8 (7.27%) |
| Tumor stage | |
| T1 | 63 (57.27%) |
| T2 | 46 (41.82%) |
| T3 | 1 (0.91%) |
| Recurrence | |
| Yes | 2 (1.82%) |
| No | 108 (98.18%) |
| Follow-up interval, median (IQR) | 26.98 (14.16, 45.21) |
| Characteristic | 23-Gene Classifier ≥ 29 n = 24 | 23-Gene Classifier < 29 n = 86 | p-Value |
|---|---|---|---|
| Age (SD) | 49.71 (11.96) | 52.37 (10.79) | 0.3 |
| Nodal stage | 0.3 | ||
| N0 | 16 (66.67%) | 68 (79.07%) | |
| N1 | 8 (33.33%) | 18 (20.93%) | |
| Grade | 0.068 | ||
| I | 2 (8.33%) | 18 (20.93%) | |
| II | 18 (75.00%) | 64 (74.42%) | |
| III | 4 (16.67%) | 4 (4.65%) | |
| Tumor stage | 0.6 | ||
| T1 | 12 (50.00%) | 51 (59.30%) | |
| T2 | 12 (50.00%) | 34 (39.53%) | |
| T3 | 0 (0.00%) | 1 (1.16%) | |
| Relapse | 0.046 | ||
| Yes | 2 (8.33%) | 0 (0.00%) | |
| No | 22 (91.67%) | 86 (100.0%) | |
| Follow-up interval (IQR) | 26.82 (17.68, 47.86) | 26.98 (12.86, 44.30) | 0.339 |
| Characteristic | Oncotype ≥ 25, n = 16 | Oncotype < 25, n = 94 | p-Value |
|---|---|---|---|
| Age (SD) | 53.12 (7.19) | 51.56 (11.60) | 0.5 |
| Nodal stage | >0.9 | ||
| N0 | 12 (75.00%) | 72 (76.60%) | |
| N1 | 4 (25.00%) | 22 (23.40%) | |
| Grade | 0.012 | ||
| I | 1 (6.25%) | 19 (20.21%) | |
| II | 11 (68.75%) | 71 (75.53%) | |
| III | 4 (25.00%) | 4 (4.26%) | |
| Tumor stage | 0.6 | ||
| T1 | 8 (50.00%) | 55 (58.51%) | |
| T2 | 8 (50.00%) | 38 (40.43%) | |
| T3 | 0 (0.00%) | 1 (1.06%) | |
| Relapse | 0.3 | ||
| Yes | 1 (6.25%) | 1 (1.06%) | |
| No | 15 (93.75%) | 93 (98.94%) | |
| Follow-up interval (IQR) | 28.34 [13.91, 54.78] | 26.98 [14.24, 44.30] | 0.593 |
| 23-Gene Classifier RI | Recurrence | Total | |
|---|---|---|---|
| Yes | No | ||
| high-risk | 2 (1.8%) | 22 (20%) | 24 (22%) |
| low-risk | 0 (0%) | 86 (78%) | 86 (78%) |
| Total | 2 (1.8%) | 108 (98%) | 110 (100%) |
| Oncotype Dx | Recurrence | Total | |
|---|---|---|---|
| Yes | No | ||
| high-risk | 1 (0.9%) | 15 (14%) | 16 (15%) |
| low-risk | 1 (0.9%) | 93 (84%) | 94 (85%) |
| Total | 2 (1.8%) | 108 (98%) | 110 (100%) |
| 23-Gene Classifier RI | Oncotype DX® RS | Total | |
|---|---|---|---|
| High-Risk | Non-High-Risk | ||
| high-risk | 9 (8.2%) | 15 (14%) | 24 (22%) |
| low-risk | 7 (6.4%) | 79 (72%) | 86 (78%) |
| Total | 16 (15%) | 94 (85%) | 110 (100%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, C.-H.; Yang, P.-S.; Hsieh, C.-M.; Chen, T.-H.; Cheng, S.H.-C.; Yang, C.-E.; Huang, C.-S. Prognostic Comparison between Oncotype DX® and a 23-Gene Classifier, RecurIndex®, on the Taiwan Breast Cancer Population. Diagnostics 2022, 12, 2850. https://doi.org/10.3390/diagnostics12112850
Chang C-H, Yang P-S, Hsieh C-M, Chen T-H, Cheng SH-C, Yang C-E, Huang C-S. Prognostic Comparison between Oncotype DX® and a 23-Gene Classifier, RecurIndex®, on the Taiwan Breast Cancer Population. Diagnostics. 2022; 12(11):2850. https://doi.org/10.3390/diagnostics12112850
Chicago/Turabian StyleChang, Chuan-Hsun, Po-Sheng Yang, Chia-Ming Hsieh, Ting-Hao Chen, Skye Hung-Chun Cheng, Cheng-En Yang, and Chiun-Sheng Huang. 2022. "Prognostic Comparison between Oncotype DX® and a 23-Gene Classifier, RecurIndex®, on the Taiwan Breast Cancer Population" Diagnostics 12, no. 11: 2850. https://doi.org/10.3390/diagnostics12112850