
Efficacy of Radiofrequency as Therapy and Diagnostic Support in the Management of Musculoskeletal Pain: A Systematic Review and Meta-Analysis

 ,
,  ,
,  , , ,
, , , 

Abstract
1. Introduction
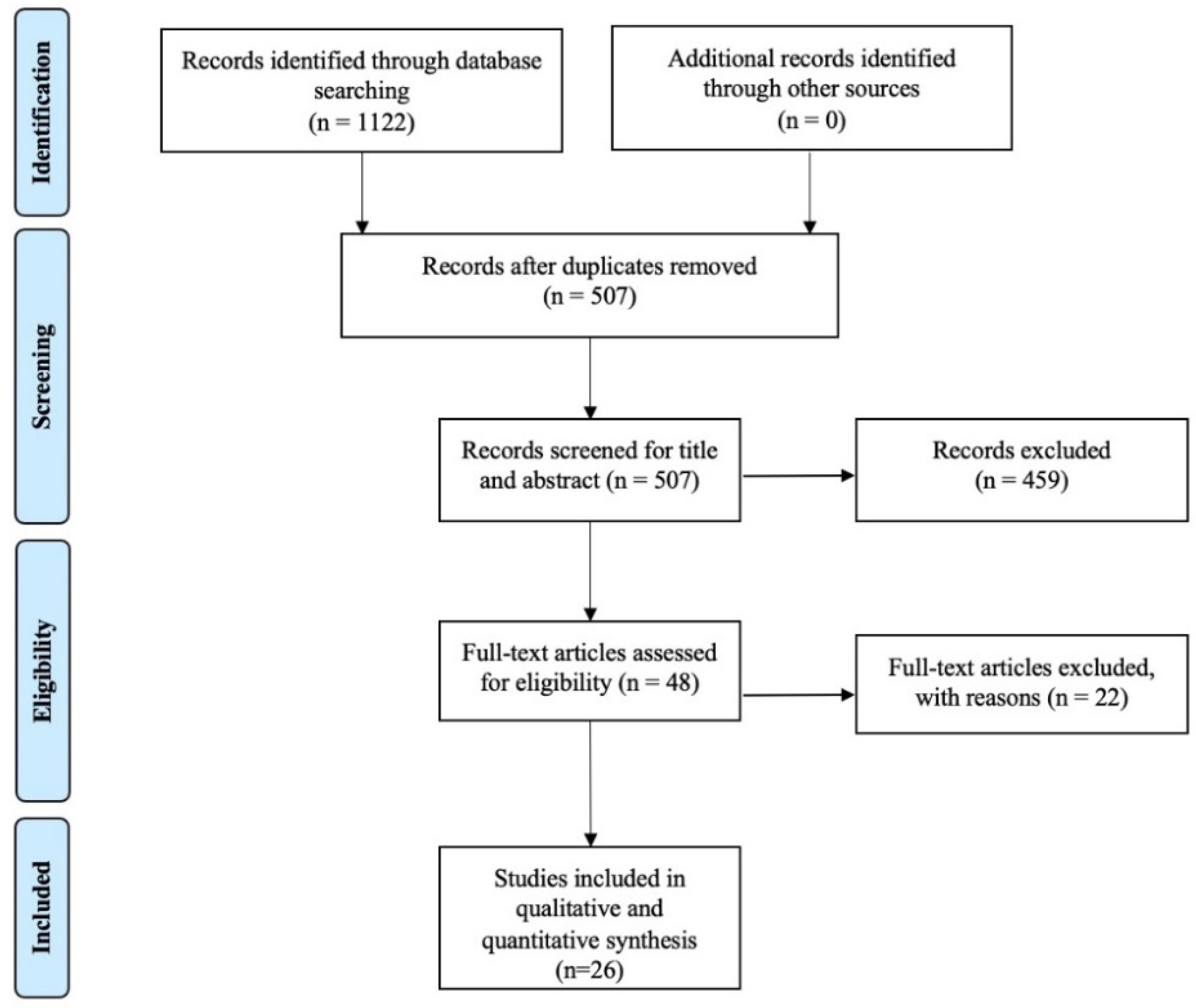
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
- -
- Participants: patients with chronic musculoskeletal pain, aged between 18 and 80;
- -
- Interventions: CRF, PRF, WCRF;
- -
- Comparison: placebo, anesthetic injection, corticosteroid injection, prolotherapy, conservative treatment (physiotherapy) and transcutaneous electrical nerve stimulation (TENS);
- -
- Outcomes: RF effects on pain and motor disability.
2.3. Data Extraction
2.4. Data Synthesis
2.5. Statistical Analysis
3. Results
- -
- To evaluate pain relief, the following scales were considered: Visual Analogical Scale (VAS) and Numeric Rating Scale (NRS);
- -
- To evaluate improvement in motor disability and articular functionality, the following scales were considered: Oswestry Disability Index (ODI); Oxford Knee score; the physical component of Short Form-36 (SF-36); Western Ontario and McMaster University (WOMAC) Osteoarthritis Index; Shoulder Pain and Disability Index (SPADI) questionnaire.
4. Discussion
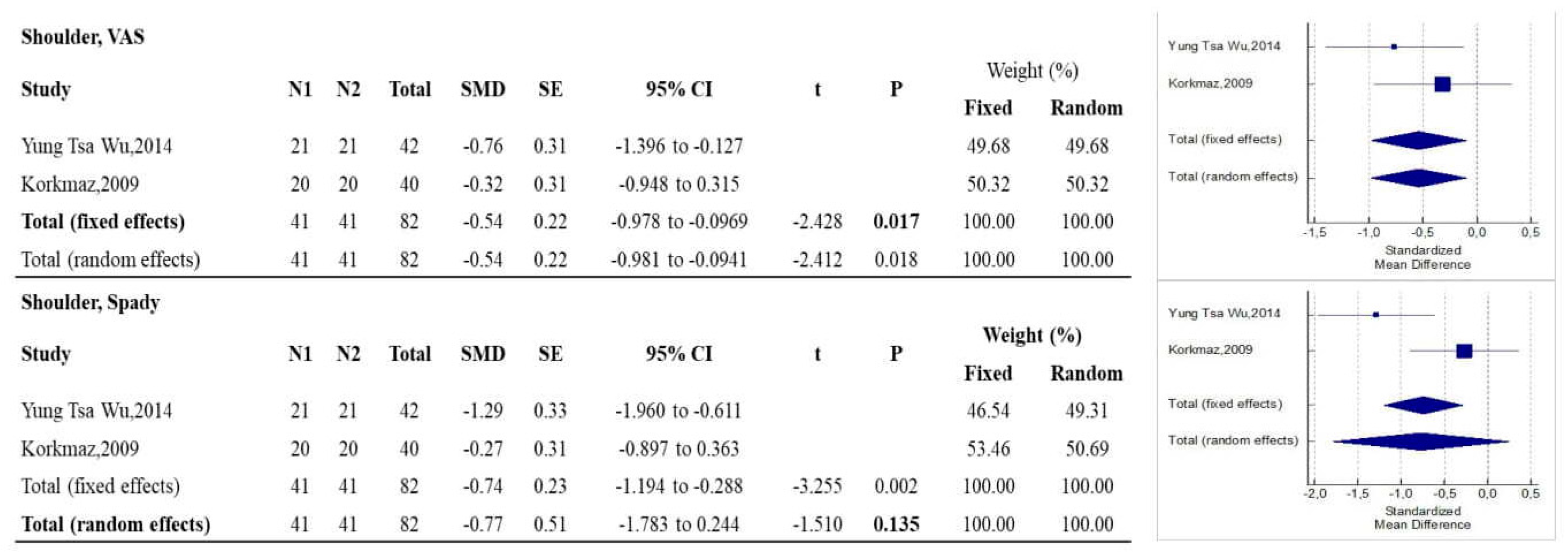
4.1. Shoulder
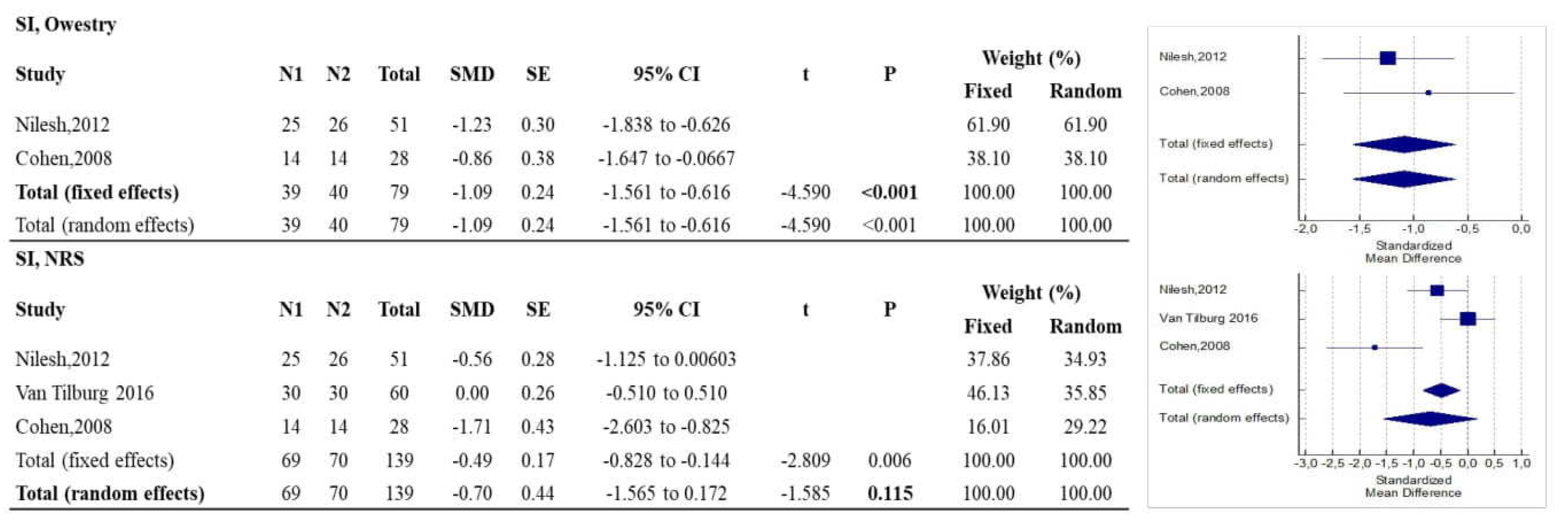
4.2. Sacroiliac Joint
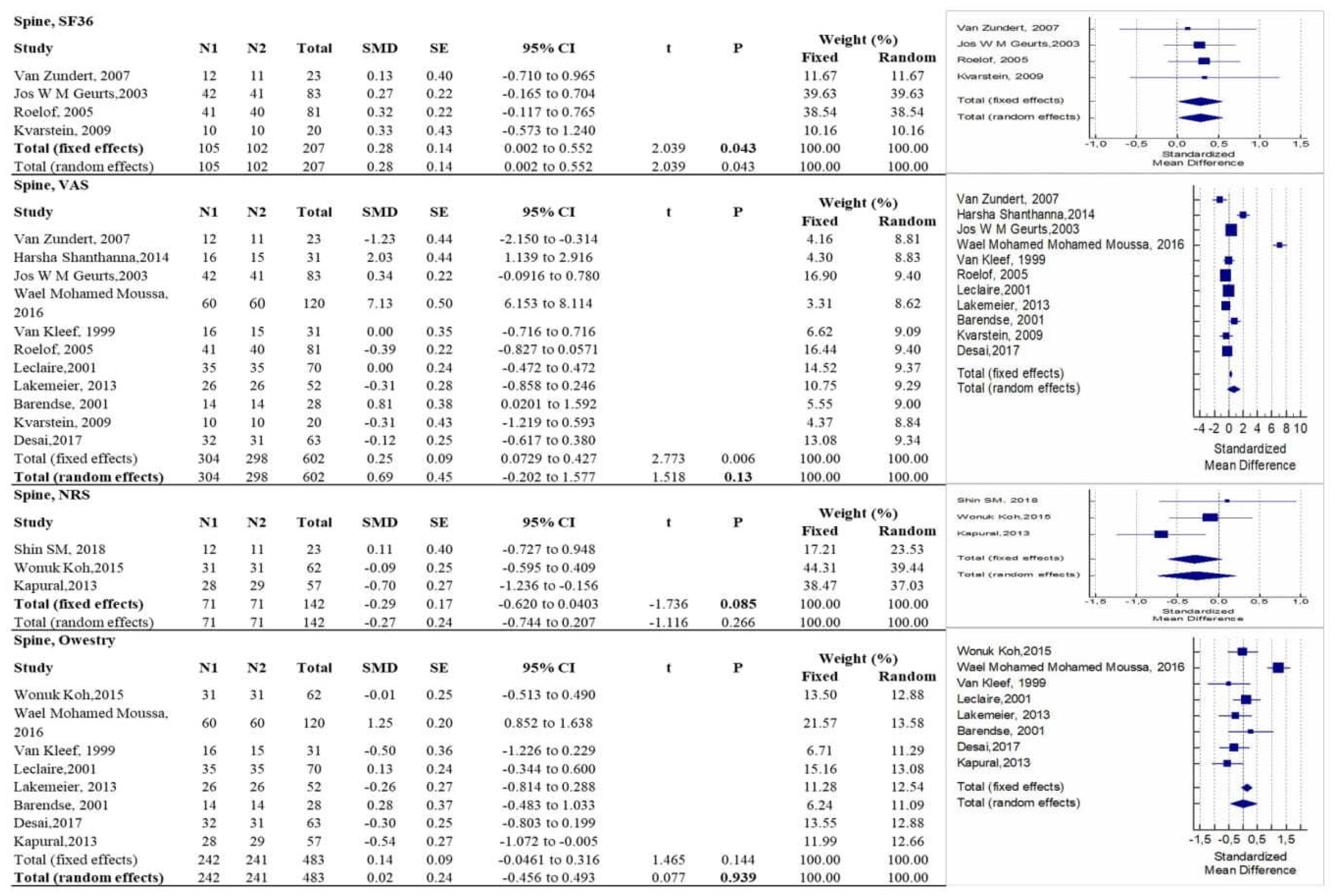
4.3. Spine
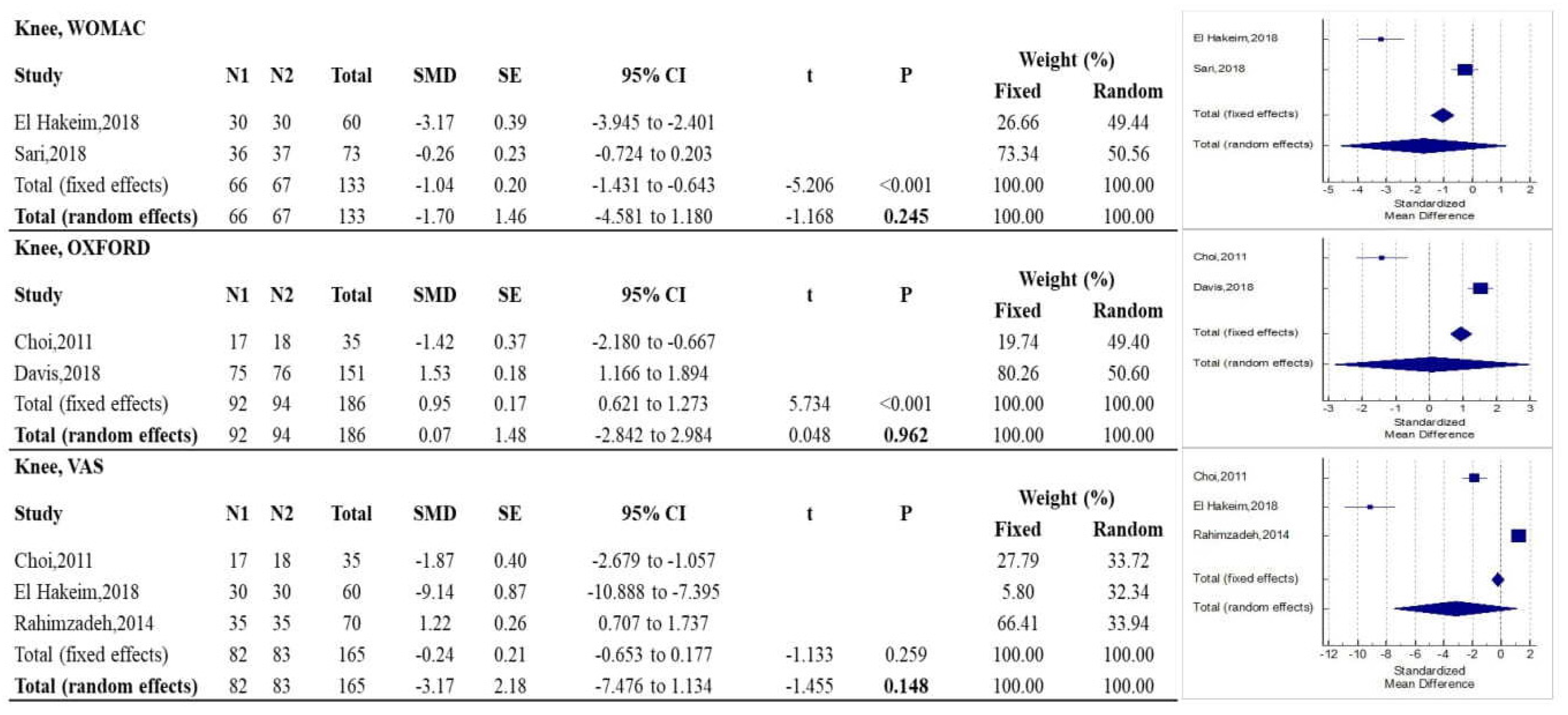
4.4. Knee
4.5. Radiofrequency: An Opportunity for Musculoskeletal Rehabilitation and Pain Medicine
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Huang, Y.; Deng, Q.; Yang, L.; Ma, J.; Wang, Z.; Huang, D.; Luo, L.; Zhou, H. Efficacy and Safety of Ultrasound-Guided Radiofrequency Treatment for Chronic Pain in Patients with Knee Osteoarthritis: A Systematic Review and Meta-Analysis. Pain Res. Manag. 2020, 2020, 2537075. [Google Scholar] [CrossRef] [PubMed]
- Mariconda, C.; Megna, M.; Farì, G.; Bianchi, F.P.; Puntillo, F.; Correggia, C.; Fiore, P. Therapeutic exercise and radiofrequency in the rehabilitation project for hip osteoarthritis pain. Eur. J. Phys. Rehabil. Med. 2020, 56, 451–458. [Google Scholar] [CrossRef] [PubMed]
- Uematsu, S.; Udvarhelyi, G.B.; Benson, D.W.; Siebens, A.A. Percutaneous radiofrequency rhizotomy. Surg. Neurol. 1974, 2, 319–325. [Google Scholar]
- Bogduk, N. ISIS Position Paper on Pulsed radiofrequency. Pain Med. 2006, 7, 396–407. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, F.M. Cooled Radiofrequency Genicular Neurotomy. Tech. Vasc. Interv. Radiol. 2020, 23, 100706. [Google Scholar] [CrossRef] [PubMed]
- de Sire, A.; Lippi, L.; Curci, C.; Calafiore, D.; Cisari, C.; Ammendolia, A.; Invernizzi, M. Effectiveness of Combined Treatment Using Physical Exercise and Ultrasound-Guided Radiofrequency Ablation of Genicular Nerves in Patients with Knee Osteoarthritis. Appl. Sci. 2021, 11, 4338. [Google Scholar] [CrossRef]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef]
- Min Shin, S.; Kwak, S.G.; Lee, D.G.; Chang, M. Clinical Effectiveness of Intra-articular Pulsed Radiofrequency Compared to Intra-articular Corticosteroid Injection for Management of Atlanto-occipital Joint Pain. A prospective Randomized Controlled Pilot Study. Spine 2018, 43, 741–747. [Google Scholar] [CrossRef]
- Zundert, J.; Patijn, J.; Kessels, A.; Lame, I. ´; Suijlekom, H.; Van Kleef, M. Pulsed radiofrequency adjacent to the cervical dorsal root ganglion in chronic cervical radicular pain: A double blind sham controlled randomized clinical trial. Pain 2007, 127, 173–182. [Google Scholar] [CrossRef]
- Roelof, M.; Van Wijk, W.R.; Geurts, W.M.J.; Wynne, H.J.; Hammink, E.; Buskens, E.; Lousberg, R.; Knape, J.T.A.; Groen, J.G. Radiofrequency Denervation of Lumbar Facet Joints in the Treatment of Chronic Low Back Pain. A Randomized, Double-Blind, Sham Lesion-Controlled Trial. Clin. J. Pain. 2005, 21, 335–344. [Google Scholar]
- Nath, S.; Nath, C.A.; Pettersson, K. Percutaneous Lumbar Zygapophysial (Facet) Joint Neurotomy Using Radiofrequency Current, in the Management of Chronic Low Back Pain. Spine 2008, 33, 1291–1297, discussion 1298. [Google Scholar] [CrossRef]
- Leclaire, R.; Fortin, L.; Lambert, R.; Bergeron, Y.M.; Rossignol, M. Radiofrequency Facet Joint Denervation in the Treatment of Low Back Pain. A Placebo-Controlled Clinical Trial to Assess Efficacy. Spine 2011, 26, 1411–1417. [Google Scholar] [CrossRef] [PubMed]
- Lakemeier, S.; Lind, M.; Schultz, W.; Fuchs-Winkelmann, S.; Timmesfeld, N.; Foelsch, C.; Peterlein, C.D. A Comparison of Intrarticular Lumbar Facet Joint Steroid Injections and Lumbar Facet Joint Radiofrequency Denervation in the Treatment of Low Back Pain: A Randomized, Controlled, Double-Blind Trial. Anesth. Analg. 2013, 117, 228–235. [Google Scholar] [CrossRef]
- Mohamed Mohamed Moussa, W.; Khedr, W. Percutaneous radiofrequency facet capsule denervation as analternative target in lumbar facet syndrom. Clin. Neurol. Neurosurg. 2016, 150, 96–104. [Google Scholar] [CrossRef] [PubMed]
- Geurts, W.M.J.; Van Wijk, W.R.; Wynne, H.J.; Hammink, E.; Buskens, E.; Lousberg, R.; Knape, J.T.A.; Groen, G.J. Radiofrequency lesioning of dorsal root ganglia for chronic lumbosacral radicular pain: A randomised, double-blind, controlled trial. Lancet 2003, 361, 21–26. [Google Scholar] [CrossRef]
- Shanthanna, H.; Chan, P.; McChesneyJThabane, L.; Pa, J. Pulsed radiofrequency treatment of the lumbar dorsal root ganglion in patients with chronic lumbar radicular pain: A randomized, placebo-controlled pilot study. J. Pain Res. 2014, 7, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Koh, W.; Choi, S.; Karm, M.H.; Suh, J.H.; Gil Leem, J.; Do Lee, J.; Ki Kim, Y.; Shin, J. Treatment of Chronic Lumbosacral Radicular Pain Using Adjuvant Pulsed Radiofrequency: A Randomized Controlled Study. Pain Med. 2015, 16, 432–441. [Google Scholar] [CrossRef] [PubMed]
- Van Kleef, M.; Barendse, G.A.; Kessels, A.; Voets, H.M.; Weber, W.E.J.; De Lange, S. Randomized trial of radiofrequency lumbar facet denervation for chronic low back pain. Spine 1999, 1937–1942. [Google Scholar] [CrossRef]
- Kvarstein, G.; Måwea, L.; Indahl, A.; Hol, P.C.; Tennøe, B.; Digernes, R.; Stubhaug, A.; Tønnessen, T.I.; Beivik, H. A randomized double-blind controlled trial of intra-annular radiofrequency thermal disc therapy—A 12-month follow-up. Pain 2009, 145, 279–286. [Google Scholar] [CrossRef]
- Barendse, G.A.M.; Van den Berg, S.G.M.; Kessels, A.H.F.; Weber, W.E.J.; Van Kleef, M. Randomized Controlled Trial of Percutaneous Intradiscal Radiofrequency Thermocoagulation for Chronic Discogenic Back Pain. Spine 2011, 26, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Desai, M.J.; Kapural, L.; Petersohn, J.D.; Vallejo, R.; Menzies, R.; Creamer, M.; Gofeld, M. Twelve-Month Follow-up of a Randomized Clinical Trial Comparing Intradiscal Biacuplasty to Conventional Medical Management for Discogenic Lumbar Back Pain. Pain Med. 2017, 18, 751–763. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kapural, L.; Vrooman, B.; Sarwar, S.; Krizanac-Bengez, L.; Rauck, R.; Gilmore, C.; North, J.; Girgis, G.; Mekhail, N. A Randomized, Placebo-Controlled Trial of Transdiscal Radiofrequency, Biacuplasty for Treatment of Discogenic Lower Back Pain. Pain Med. 2013, 14, 362–373. [Google Scholar] [CrossRef] [PubMed]
- Choi, W.-J.; Hwang, S.; Song, J.; Leem, J.; Kang, Y.; Park, P.; Shin, J. Radiofrequency treatment relieves chronic knee osteoarthritis pain: A double-blind randomized controlled trial. Pain 2011, 152, 481–487. [Google Scholar] [CrossRef]
- El-Hakeim, E.; Elawamy, A.; Zarief Kamel, E.; Goma, S.; Gamal, R.; Ghandour, A.; Osman, A.; Morsy, K. Fluoroscopic Guided Radiofrequency of Genicular Nerves for Pain Alleviation in Chronic Knee Osteoarthritis: A Single-Blind Randomized Controlled Trial. Pain Phys. 2018, 21, 169–217. [Google Scholar]
- Sari, S.; Aydin, O.; Turan, Y.; Ozleulerden, P.; Efe, U.; Omurlu, K. Which one is more effective for the clinical treatment of chronic pain in knee osteoarthritis: Radiofrequency neurotomy of the genicular nerves or intra-articular injection? Int. J. Rheum. Dis. 2018, 21, 1772–1778. [Google Scholar] [CrossRef]
- Davis, T.; Loudermilk, E.; DePalma Corey Hunter, C.; Lindley, D.; Patel, N.; Choi, D.; Soloman, M.; Gupta, A.; Desai, M.; Buvanendran, A.; et al. Prospective, Multicenter, Randomized, Crossover Clinical Trial Comparing the Safety and Effectiveness of Cooled Radiofrequency Ablation with Corticosteroid Injection in the Management of Knee Pain from Osteoarthritis. Reg. Anesth. Pain Med. 2018, 43, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Rahimzadeh, P.; Imani, F.; Faiz, S.H.; Entezary, S.R.; Nasiri, A.A.; Ziaeefard, M. Investigation the efficacy of intra-articular prolotherapy with erythropoietin and dextrose and intra-articular pulsed radiofrequency on pain level reduction and range of motion improvement in primary osteoarthritis of knee. J. Res. Med. Sci. 2014, 19, 696–702. [Google Scholar]
- Van Tilburg, C.; Schuurmans, F.; Stronks, D.; Groeneweg, J.; Huygen, F. Randomized Sham-controlled Double-Blind Multicenter Clinical Trial to Ascertain the Effect of Percutaneous Radiofrequency Treatment for Sacroiliac Joint Pain. Three-month Results. Clin. J. Pain 2016, 32, 921–926. [Google Scholar] [CrossRef]
- Cohen, S.; Hurley, R.; Buckenmaier, C.; Kurihara, C.; Morlando, B.; Dragovich, A. Randomized Placebo-Controlled Study Evaluating Lateral Branch Radiofrequency Denervation for Sacroiliac Joint Pain. Anesthesiology 2008, 109, 279–288. [Google Scholar] [CrossRef]
- Patel, N.; Gross, A.; Brown, L.; Gekht, G. A Randomized, Placebo-Controlled Study to Assess the Efficacy of Lateral Branch Neurotomy for Chronic Sacroiliac Joint Pain. Pain Med. 2012, 13, 383–398. [Google Scholar] [CrossRef]
- Wu, Y.T.; Ho, C.W.; Chen, Y.L.; Li, T.Y.; Lee, K.C.; Chen, L.C. Ultrasound-guided pulsed radiofrequency stimulation of the suprascapular nerve for adhesive capsulitis: A prospective, randomized, controlled trial. Anesth. Analg. 2014, 119, 686–692. [Google Scholar] [CrossRef]
- Korkmaz, O.; Capaci, K.; Eyigor, C.; Eyigor, S. Pulsed radiofrequency versus conventional transcutaneous electrical nerve stimulation in painful shoulder: A prospective, randomized study. Clin. Rehabil. 2010, 24, 1000–1008. [Google Scholar] [CrossRef]
- Gofeld, M.; Restrepo-Garces, C.; Theodore, B.; Faclier, G. Pulsed Radiofrequency of Suprascapular Nerve for Chronic Shoulder Pain: A Randomized Double-Blind Active Placebo-Controlled Study. Pain Pract. 2012, 13, 96–103. [Google Scholar] [CrossRef]
- Bernetti, A.; Agostini, F.; de Sire, A.; Mangone, M.; Tognolo, L.; Di Cesare, A.; Ruiu, P.; Paolucci, T.; Invernizzi, M.; Paoloni, M. Neuropathic Pain and Rehabilitation: A Systematic Review of International Guidelines. Diagnostics 2021, 11, 74. [Google Scholar] [CrossRef]
- Farì, G.; Santagati, D.; Pignatelli, G.; Scacco, V.; Renna, D.; Cascarano, G.; Vendola, F.; Bianchi, F.P.; Fiore, P.; Ranieri, M.; et al. Collagen Peptides, in Association with Vitamin C, Sodium Hyaluronate, Manganese and Copper, as Part of the Rehabilitation Project in the Treatment of Chronic Low Back Pain. Endocr. Metab. Immune Disord. Drug Targets 2021, 22, 108–115. [Google Scholar] [CrossRef]
- Bernetti, A.; Mangone, M.; Alviti, F.; Paolucci, T.; Attanasi, C.; Murgia, M.; Di Sante, L.; Agostini, F.; Vitale, M.; Paoloni, M. Spa therapy and rehabilitation of musculoskeletal pathologies: A proposal for best practice in Italy. Int. J. Biometeorol. 2020, 64, 905–914. [Google Scholar] [CrossRef] [PubMed]
- Farì, G.; Fischetti, F.; Zonno, A.; Marra, F.; Maglie, A.; Bianchi, F.P.; Messina, G.; Ranieri, M.; Megna, M. Musculoskeletal Pain in Gymnasts: A Retrospective Analysis on a Cohort of Professional Athletes. Int. J. Environ. Res. Public Health 2021, 18, 5460. [Google Scholar] [CrossRef] [PubMed]
- de Sire, A.; Marotta, N.; Lippi, L.; Scaturro, D.; Farì, G.; Liccardi, A.; Moggio, L.; Letizia Mauro, G.; Ammendolia, A.; Invernizzi, M. Pharmacological Treatment for Acute Traumatic Musculoskeletal Pain in Athletes. Medicina 2021, 57, 1208. [Google Scholar] [CrossRef] [PubMed]
- Farì, G.; Santagati, D.; Macchiarola, D.; Ricci, V.; Di Paolo, S.; Caforio, L.; Invernizzi, M.; Notarnicola, A.; Megna, M.; Ranieri, M. Musculoskeletal pain related to surfing practice: Which role for sports rehabilitation strategies? A cross-sectional study. J. Back Musculoskelet. Rehabil. 2022, ahead of print. [CrossRef]
- de Sire, A. Low back pain: Old concepts and new insights. J Back Musculoskelet. Rehabil. 2021, 34, 723–724. [Google Scholar] [CrossRef] [PubMed]
- Bernetti, A.; Agostini, F.; Alviti, F.; Giordan, N.; Martella, F.; Santilli, V.; Paoloni, M.; Mangone, M. New Viscoelastic Hydrogel Hymovis MO.RE. Single Intra-articular Injection for the Treatment of Knee Osteoarthritis in Sportsmen: Safety and Efficacy Study Results. Front Pharmacol. 2021, 12, 673988. [Google Scholar] [CrossRef] [PubMed]
- Conaghan, P.G.; Cook, A.D.; Hamilton, J.A.; Tak, P.P. Therapeutic options for targeting inflammatory osteoarthritis pain. Nat. Rev. Rheumatol. 2019, 15, 355–363. [Google Scholar] [CrossRef] [PubMed]
- Ferreira-Valente, M.A.; Pais-Ribeiro, J.L.; Jensen, M.P. Associations between psychosocial factors and pain intensity, physical functioning, and psychological functioning in patients with chronic pain: A cross-cultural comparison. Clin. J. Pain 2014, 30, 713–723. [Google Scholar] [CrossRef]
- Santilli, V.; Mangone, M.; Paoloni, M.; Agostini, F.; Alviti, F.; Bernetti, A. Comment on “Early Efficacy of Intra-Articular HYADD® 4 (Hymovis®) Injections for Symptomatic Knee Osteoarthritis”. Joints 2018, 6, 131–132. [Google Scholar] [CrossRef]
- de Sire, A.; Agostini, F.; Lippi, L.; Mangone, M.; Marchese, S.; Cisari, C.; Bernetti, A.; Invernizzi, M. Oxygen-Ozone Therapy in the Rehabilitation Field: State of the Art on Mechanisms of Action, Safety and Effectiveness in Patients with Musculoskeletal Disorders. Biomolecules 2021, 11, 356. [Google Scholar] [CrossRef] [PubMed]
- de Sire, A.; Stagno, D.; Minetto, M.A.; Cisari, C.; Baricich, A.; Invernizzi, M. Long-term effects of intra-articular oxygen-ozone therapy versus hyaluronic acid in older people affected by knee osteoarthritis: A randomized single-blind extension study. J Back Musculoskelet. Rehabil. 2020, 33, 347–354. [Google Scholar] [CrossRef]
- Pushparaj, H.; Hoydonckx, Y.; Mittal, N.; Peng, P.; Cohen, S.P.; Cao, X.; Bhatia, A. A systematic review and meta-analysis of radiofrequency procedures on innervation to the shoulder joint for relieving chronic pain. Eur. J. Pain. 2021, 25, 986–1011. [Google Scholar] [CrossRef]
- Yan, J.; Zhang, X.M. A randomized controlled trial of ultrasound-guided pulsed radiofrequency for patients with frozen shoulder. Medicine 2019, 98, e13917. [Google Scholar] [CrossRef]
- Ergonenc, T.; Beyaz, S.G. Effects of ultrasound-guided suprascapular nerve pulsed radiofrequency on chronic shoulder pain. Med. Ultrason. 2018, 20, 461–466. [Google Scholar] [CrossRef]
- Chen, C.H.; Weng, P.W.; Wu, L.C.; Chiang, Y.F.; Chiang, C.J. Radiofrequency neurotomy in chronic lumbar and sacroiliac joint pain: A meta-analysis. Medicine 2019, 98, e16230. [Google Scholar] [CrossRef]
- Rashbaum, R.F.; Ohnmeiss, D.D.; Lindley, E.M.; Kitchel, S.H.; Patel, V.V. Sacroiliac Joint Pain and Its Treatment. Clin. Spine Surg. 2016, 29, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Chuang, C.W.; Hung, S.K.; Pan, P.T.; Kao, M.C. Diagnosis and interventional pain management options for sacroiliac joint pain. Tzu-Chi Med. J. 2019, 31, 207–210. [Google Scholar]
- Niemistö, L.; Kalso, E.; Malmivaara, A.; Seitsalo, S.; Hurri, H.; Cochrane Collaboration Back Review Group. Radiofrequency denervation for neck and back pain: A systematic review within the framework of the cochrane collaboration back review group. Spine 2003, 28, 1877–1888. [Google Scholar] [CrossRef]
- Lee, C.H.; Chung, C.K.; Kim, C.H. The efficacy of conventional radiofrequency denervation in patients with chronic low back pain originating from the facet joints: A meta-analysis of randomized controlled trials. Spine J. 2017, 17, 1770–1780. [Google Scholar] [CrossRef] [PubMed]
- Kwak, S.G.; Lee, D.G.; Chang, M.C. Effectiveness of pulsed radiofrequency treatment on cervical radicular pain: A meta-analysis. Medicine 2018, 97, e11761. [Google Scholar] [CrossRef] [PubMed]
- Shih, C.L.; Shen, P.C.; Lu, C.C.; Liu, Z.M.; Tien, Y.C.; Huang, P.J.; Chou, S.H. A comparison of efficacy among different radiofrequency ablation techniques for the treatment of lumbar facet joint and sacroiliac joint pain: A systematic review and meta-analysis. Clin. Neurol. Neurosurg. 2020, 195, 105854. [Google Scholar] [CrossRef]
- Manchikanti, L.; Kaye, A.D.; Boswell, M.V.; Bakshi, S.; Gharibo, C.G.; Grami, V.; Grider, J.S.; Gupta, S.; Jha, S.S.; Mann, D.P.; et al. A Systematic Review and Best Evidence Synthesis of the Effectiveness of Therapeutic Facet Joint Interventions in Managing Chronic Spinal Pain. Pain Phys. 2015, 18, E535–E582. [Google Scholar] [CrossRef]
- Fonkoué, L.; Behets, C.; Kouassi, J.K.; Coyette, M.; Detrembleur, C.; Thienpont, E.; Cornu, O. Distribution of sensory nerves supplying the knee joint capsule and implications for genicular blockade and radiofrequency ablation: An anatomical study. Surg. Radiol. Anat. 2019, 41, 1461–1471. [Google Scholar] [CrossRef]
- Mittal, N.; Catapano, M.; Peng, P.W.H. Knee Ablation Approaches. Phys. Med. Rehabil. Clin. N. Am. 2021, 32, 779–790. [Google Scholar] [CrossRef]
- Ajrawat, P.; Radomski, L.; Bhatia, A.; Peng, P.; Nath, N.; Gandhi, R. Radiofrequency Procedures for the Treatment of Symptomatic Knee Osteoarthritis: A Systematic Review. Pain Med. 2020, 21, 333–348. [Google Scholar] [CrossRef]
- Chen, A.F.; Mullen, K.; Casambre, F.; Visvabharathy, V.; Brown, G.A. Thermal Nerve Radiofrequency Ablation for the Nonsurgical Treatment of Knee Osteoarthritis: A Systematic Literature Review. J. Am. Acad. Orthop. Surg. 2021, 29, 387–396. [Google Scholar] [CrossRef] [PubMed]
- Palermi, S.; Massa, B.; Vecchiato, M.; Mazza, F.; De Blasiis, P.; Romano, A.M.; Di Salvatore, M.G.; Della Valle, E.; Tarantino, D.; Ruosi, C.; et al. Indirect Structural Muscle Injuries of Lower Limb: Rehabilitation and Therapeutic Exercise. J. Funct. Morphol. Kinesiol. 2021, 6, 75. [Google Scholar] [CrossRef] [PubMed]
- Yarmolenko, P.S.; Moon, E.J.; Landon, C.; Manzoor, A.; Hochman, D.W.; Viglianti, B.L.; Dewhirst, M.W. Thresholds for thermal damage to normal tissues: An update. Int. J. Hyperther. 2011, 27, 320–343. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Year | PEDro Score | Sample Size | Anatomical Region of Musculoskeletal Pain | Type of Radiofrequency | Target | Outcome | Control Group | Radiofrequency Method |
|---|---|---|---|---|---|---|---|---|---|
| Min Shin et al. [8] | 2018 | 8 | 23 | Chronic suboccipital neck pain | Pulsed | Occipital-atlas Joint | NRS | Intra-articular Corticosteroid | 42° × 360 s |
| Zundert et al. [9] | 2007 | 9 | 23 | Neck pain | Pulsed | Medial branch of the dorsal ramus | VAS, GPE, SF-36 | Sham without RF | NS × 120 s |
| Roelof et al. [10] | 2005 | 9 | 81 | Low back pain | Pulsed | Medial branch of the dorsal ramus | VAS, SF-36 | Sham without RF | 80° × 60 s |
| Sherdil et al. [11] | 2008 | 9 | 40 | Low back pain | Pulsed | Medial branch of the dorsal ramus | VAS, ROM | Sham without RF | 85° × 60 s |
| Leclaire et al. [12] | 2001 | 7 | 70 | Low back pain | Pulsed | Medial branch of the dorsal ramus | VAS, ODI, RMDQ | Sham without RF | 80° × 90 s |
| Lakemeier et al. [13] | 2013 | 8 | 52 | Low back pain | Continue | Medial branch of the dorsal ramus | VAS, ODI, RMDQ | Intra-articular Corticosteroid | 80° × 90 s |
| Moussa and Khedr [14] | 2016 | 8 | 120 | Low back pain | Continue | Medial branch of the dorsal ramus Facet joint capsule | VAS, ODI | Sham without RF | 85° × 90 s |
| Geurts et al. [15] | 2003 | 10 | 83 | Low back pain | Continue | Dorsal root ganglion | VAS, DAS, SF-36, MRI findings, NARS | Sham without RF | 67° × 90 s |
| Shanthanna et al. [16] | 2014 | 10 | 31 | Low back pain | Pulsed | Dorsal root ganglion | VAS, ODI | Sham without RF | 42° × 120 s |
| Koh et al. [17] | 2015 | 10 | 62 | Low back pain | Pulsed | Dorsal root ganglion | NRS, ODI, MQS, GPE | Epidural | 42° × 120 s |
| Van Kleef et al. [18] | 1999 | 10 | 31 | Low back pain | Continue | Medial branch of the dorsal ramus | VAS, ODI, CWQS | Sham without RF | 80° × 60 s |
| Kvarstein et al. [19] | 2009 | 10 | 20 | Low back pain | Continue | Intradiscal space | NRS, ODI, SF-36 | Sham without RF | 65° × 10 min |
| Barendse et al. [20] | 2011 | 9 | 28 | Low back pain | Continue | Intradiscal space | VAS, ODI, CWQS | Sham without RF | 70° × 90 s |
| Desai et al. [21] | 2017 | 7 | 63 | Low back pain | Cooled | Intradiscal space | VAS, ODI, SF-36, EQ5D-VAS, EQ5D-HI, PGIC, BDI | Kinesitherapy | NS |
| Kapural et al. [22] | 2013 | 9 | 57 | Low back pain | Cooled | Intradiscal space | NRS, ODI, SF-36 | Sham without RF | 45 °C bipolar for 15 min, then 50 °C in bipolar for 15 min, then 60 °C monopolar for 2.5 min |
| Choi et al. [23] | 2011 | 9 | 35 | Knee osteoarthritic pain | Continue | Geniculate nerves | VAS, OKS, GPE | Sham without RF | 70° × 90 s |
| El-Hakeim et al. [24] | 2018 | 7 | 60 | Knee osteoarthritic pain | Continue | Geniculate nerves | VAS, WOMAC-OI | Paracetamol and diclofenac per os | 80° × 90 s 3 cycles |
| Sari et al. [25] | 2018 | 7 | 73 | Knee osteoarthritic pain | Continue | Geniculate nerves | VAS, WOMAC-OI | Infiltration with betamethasone and morphine | 80° × 90 s |
| Davis et al. [26] | 2018 | 6 | 151 | Knee osteoarthritic pain | Cooled | Geniculate nerves | NRS, OKS | Corticosteroid infiltration | 60° × 150 s |
| Rahimzadeh et al. [27] | 2014 | 9 | 70 | Knee osteoarthritic pain | Pulsed | Geniculate nerves | VAS, Knee ROM, GPE | Erythropoietin infiltration | 42° × 15 min 2 cycles |
| Van Tilburg et al. [28] | 2016 | 9 | 60 | Chronic sacroiliac pain | Cooled | Lateral branch of the dorsal ramus | NRS, GPE | Sham without RF | 85° × 90 s |
| Cohen et al. [29] | 2008 | 8 | 28 | Chronic sacroiliac Pain | Cooled | Lateral branch of the dorsal ramus | NRS, GPE, ODI | Sham without RF | 80° × 90 s |
| Patel et al. [30] | 2012 | 9 | 51 | Chronic sacroiliac pain | Cooled | Lateral branch of the dorsal ramus | NRS, SF-36, ODI, AQoL | Sham without RF | 60° × 150 s |
| Wu et al. [31] | 2014 | 7 | 42 | Shoulder adhesive capsulitis | Pulsed | Suprascapular nerve | SPADI, ROM, VAS | Kinesitherapy | 42° × 180 s |
| Korkmaz et al. [32] | 2009 | 7 | 40 | Shoulder adhesive capsulitis | Pulsed | Suprascapular nerve | VAS, ROM, SF-36, SPADI | TENS | 42° × 360 s |
| Gofeld et al. [33] | 2012 | 8 | 22 | Shoulder adhesive capsulitis | Pulsed | Suprascapular nerve | NRS, SPADI, CMS | Sham without RF | 42° × 120 s |
| Body Region | Outcome | Study (First Author, Year) | Intervention Group | Control Group | ||||
|---|---|---|---|---|---|---|---|---|
| N | Mean | SD | N | Mean | SD | |||
| Knee | OXFORD KNEE SCORE | Choi, 2011 | 17 | 27.4 | 10.2 | 18 | 38.9 | 4.8 |
| Davis, 2018 | 75 | 35.7 | 8.8 | 76 | 22.4 | 8.5 | ||
| VAS | Choi, 2011 | 17 | 4.2 | 2.5 | 18 | 7.8 | 1.0 | |
| El Hakeim, 2018 | 30 | 3.1 | 0.3 | 30 | 5.7 | 0.3 | ||
| Sari, 2018 | 36 | 4.0 | - | 37 | 5.5 | - | ||
| Davis, 2018 | 75 | 2.5 | - | 76 | 6.0 | - | ||
| Rahimzadeh, 2014 | 35 | 5.5 | 1.9 | 35 | 3.5 | 1.2 | ||
| WOMAC | El Hakeim, 2018 | 30 | 33.1 | 4.1 | 30 | 43.5 | 2.0 | |
| Sari, 2018 | 36 | 39.7 | 8.9 | 37 | 42.3 | 11.0 | ||
| Sacroiliac | NRS | Nilesh, 2012 | 25 | 3.6 | 2.6 | 26 | 5.0 | 2.4 |
| Van Tilburg 2016 | 30 | 5.4 | 1.7 | 30 | 5.4 | 1.9 | ||
| Cohen, 2008 | 14 | 2.4 | 2.0 | 14 | 6.3 | 2.4 | ||
| OSWESTRY | Nilesh, 2012 | 25 | 24.0 | 16.0 | 26 | 39.0 | 6.0 | |
| Cohen, 2008 | 14 | 33.3 | 10.6 | 14 | 42.1 | 9.3 | ||
| Shoulder | SPADI DISABILITY | Yung Tsa Wu, 2014 | 21 | 15.0 | 12.3 | 21 | 35.2 | 18.0 |
| Korkmaz, 2009 | 20 | 9.9 | 7.9 | 20 | 12.4 | 10.3 | ||
| Gofeld, 2012 | 11 | 35.2 | - | 11 | 45.5 | - | ||
| VAS | Yung Tsa Wu, 2014 | 21 | 1.7 | 1.5 | 21 | 3.3 | 2.5 | |
| Korkmaz, 2009 | 20 | 1.8 | 0.9 | 20 | 2.1 | 1.0 | ||
| Spine | NRS | Shin SM, 2018 | 12 | 2.8 | 1.7 | 11 | 2.6 | 1.8 |
| Wonuk Koh, 2015 | 31 | 5.7 | 4.9 | 31 | 6.2 | 5.5 | ||
| Kapural, 2013 | 28 | 4.9 | 2.4 | 29 | 6.5 | 2.1 | ||
| OSWESTRY | Wonuk Koh, 2015 | 31 | 37.6 | 32.7 | 31 | 38.0 | 32.5 | |
| Harsha Shanthanna, 2014 | 16 | 40.2 | 0.2 | 15 | 4.9 | 0.1 | ||
| Wael Mohamed Moussa, 2016 | 60 | 33.9 | 31.6 | 60 | 5.9 | 0.9 | ||
| Van Kleef, 1999 | 16 | 31.0 | 14.2 | 15 | 38.0 | 13.1 | ||
| Leclaire, 2001 | 35 | 38.3 | 14.7 | 35 | 36.4 | 14.6 | ||
| Lakemeier, 2013 | 26 | 28.0 | 20.0 | 26 | 33.0 | 17.4 | ||
| Barendse, 2001 | 14 | 43.7 | 11.6 | 14 | 40.7 | 9.5 | ||
| Desai, 2017 | 32 | 22.0 | 28.0 | 31 | 29.0 | 16.0 | ||
| Kapural, 2013 | 28 | 32.9 | 16.1 | 29 | 41.2 | 13.9 | ||
| SF36 | Van Zundert, 2007 | 12 | 9.0 | 16.6 | 11 | 6.9 | 15.0 | |
| Jos W M Geurts, 2003 | 42 | 40.0 | 15.7 | 41 | 36.0 | 13.6 | ||
| Roelof, 2005 | 41 | 47.6 | 16.9 | 40 | 41.6 | 19.7 | ||
| Kvarstein, 2009 | 10 | 65.0 | 21.7 | 10 | 57.5 | 21.4 | ||
| VAS | Van Zundert, 2007 | 12 | 5.6 | 1.7 | 11 | 7.6 | 1.4 | |
| Harsha Shanthanna, 2014 | 16 | 6.8 | 3.2 | 15 | 1.5 | 1.6 | ||
| Jos W M Geurts, 2003 | 42 | 5.2 | 2.2 | 41 | 4.4 | 2.4 | ||
| Wael Mohamed Moussa, 2016 | 60 | 6.0 | 1.0 | 60 | 0.7 | 0.3 | ||
| Van Kleef, 1999 | 16 | 5.2 | 1.7 | 15 | 5.2 | 1.6 | ||
| Roelof, 2005 | 41 | 5.8 | 1.8 | 40 | 6.5 | 1.8 | ||
| Leclaire, 2001 | 35 | 5.2 | 26.7 | 35 | 5.2 | 20.8 | ||
| Lakemeier, 2013 | 26 | 4.7 | 2.4 | 26 | 5.4 | 2.1 | ||
| Nath, 2008 | 20 | 3.9 | - | 20 | 3.7 | - | ||
| Barendse, 2001 | 14 | 6.5 | 1.3 | 14 | 5.5 | 1.1 | ||
| Kvarstein, 2009 | 10 | 3.6 | 2.6 | 10 | 4.5 | 2.9 | ||
| Desai, 2017 | 32 | 4.4 | 2.9 | 31 | 4.7 | 2.0 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Farì, G.; de Sire, A.; Fallea, C.; Albano, M.; Grossi, G.; Bettoni, E.; Di Paolo, S.; Agostini, F.; Bernetti, A.; Puntillo, F.; et al. Efficacy of Radiofrequency as Therapy and Diagnostic Support in the Management of Musculoskeletal Pain: A Systematic Review and Meta-Analysis. Diagnostics 2022, 12, 600. https://doi.org/10.3390/diagnostics12030600
Farì G, de Sire A, Fallea C, Albano M, Grossi G, Bettoni E, Di Paolo S, Agostini F, Bernetti A, Puntillo F, et al. Efficacy of Radiofrequency as Therapy and Diagnostic Support in the Management of Musculoskeletal Pain: A Systematic Review and Meta-Analysis. Diagnostics. 2022; 12(3):600. https://doi.org/10.3390/diagnostics12030600
Chicago/Turabian StyleFarì, Giacomo, Alessandro de Sire, Cettina Fallea, Mariantonia Albano, Gianluca Grossi, Elisa Bettoni, Stefano Di Paolo, Francesco Agostini, Andrea Bernetti, Filomena Puntillo, and et al. 2022. "Efficacy of Radiofrequency as Therapy and Diagnostic Support in the Management of Musculoskeletal Pain: A Systematic Review and Meta-Analysis" Diagnostics 12, no. 3: 600. https://doi.org/10.3390/diagnostics12030600
APA StyleFarì, G., de Sire, A., Fallea, C., Albano, M., Grossi, G., Bettoni, E., Di Paolo, S., Agostini, F., Bernetti, A., Puntillo, F., & Mariconda, C. (2022). Efficacy of Radiofrequency as Therapy and Diagnostic Support in the Management of Musculoskeletal Pain: A Systematic Review and Meta-Analysis. Diagnostics, 12(3), 600. https://doi.org/10.3390/diagnostics12030600