4. Discussion
Periprosthetic joint infection is the most serious complication after hip or knee replacement and may lead to repeated surgical interventions, prolonged hospitalization, and very high costs [
6]. Late, chronic, low-grade infection is mostly associated with nonspecific symptoms and remains a challenging diagnostic problem.
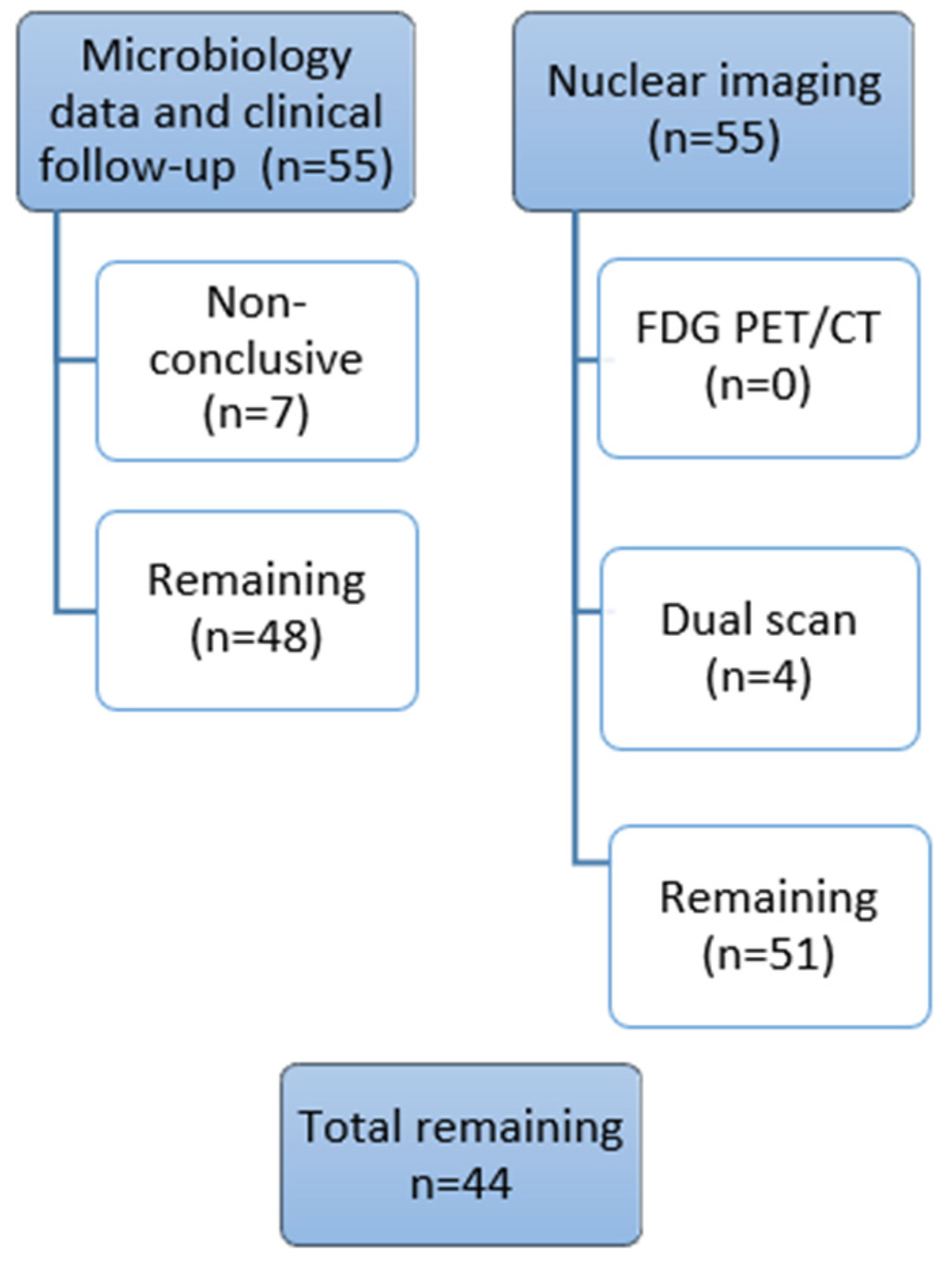
In this prospective PRIS study, 156 patients representing 163 cases of TKA or THA were recruited and assessed by the use of a multidisciplinary diagnostic algorithm including multimodal nuclear imaging (on the subgroup of 55 patients) and extended microbiological diagnostics with optimized sampling logistics, culturing methods, 16S rRNA gene polymerase chain reaction (PCR), and amplicon sequencing [
2]. To our knowledge, this is the first study of its kind [
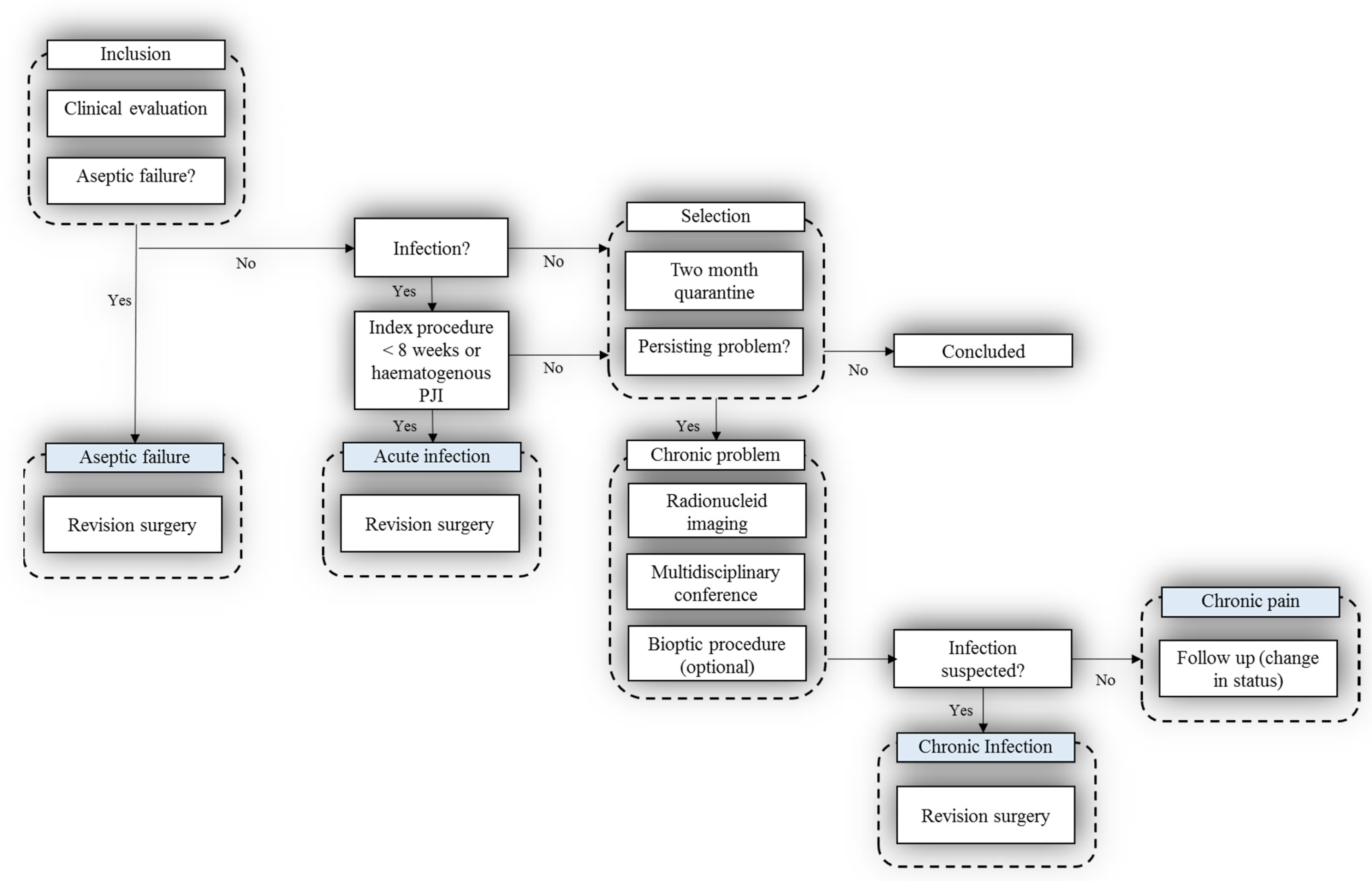
2]. The hypothesis was that diagnosis in patients experiencing post-hip or -knee replacement problems can be improved by following a structured diagnostic multidisciplinary algorithm.
The study was prospectively designed and involved a highly specialized multidisciplinary team throughout the project. It is well known that healthcare today has an increasing need for a team-based approach to care requiring interdisciplinary collaboration [
42]. Cooperation and effective communication between the entire multidisciplinary team can maximize patient outcomes. Chronic PJI can only be cured by prosthesis replacement performed as a one- or two-stage procedure with concomitant antibiotic therapy [
43] but should be applied when relevant due to the high risk of secondary infection. The results of PRIS study showed that surgical revision was obviated in approximately 20% of patients after using a strict diagnostic workup [
2]. The strength of the study was the prospective design and multidisciplinary cooperation, serving as tools in personalized patient treatment.
In this analysis of the patient subgroup, we report the diagnostic value of advanced hybrid nuclear imaging in patients with chronic problems after total hip or knee arthroplasty. It is important to emphasize that nuclear imaging significantly impacted clinical decisions on patient management in this prospective study. Imaging data from all imaging modalities were discussed together with clinical and biochemical patient data among a multidisciplinary team before further invasive procedures were performed. The purpose of our study was to investigate the diagnostic value of advanced hybrid imaging to include the best technique in future clinical diagnostic workups for diagnosing PJI. Bone scans, including three-phase bone scintigraphy, are the most widely used screening modality for the diagnosis of PJI [
6], as they are very sensitive to any bone remodeling. This examination should be avoided in the first years after surgery [
44], as physiological bone remodeling probably takes place in the first years after joint replacement surgery and is also dependent on the type of prosthesis [
6,
45]. When performing bone scans with SPECT/CT for PJI, one should remember that the most important contribution of the modality is its very high negative predictive value (NPV) [
6,
7,
22,
23]. If a bone scan is negative, an additional WBC scan can be avoided with a sensitivity of 80% and a specificity of 99.5% [
46,
47,
48] and is considered strong evidence against the presence of an infection [
6,
16,
49]. Therefore, normal physiological tracer uptake in symptomatic patients is a good indicator for an alternative cause of pain rather than post-operative complications [
50]. In our study, the normal tracer distribution on bone SPECT/CT was demonstrated in 6 out of 55 patients, which was confirmed by following dual-isotope SPECT/CT and FDG PET/CT. The diagnosis of periprosthetic joint infection and/or AF was excluded in these patients, and they were referred to the pain clinic for further investigations and were preserved from undergoing unnecessary revision operations.
Conversely, the specificity of bone SPECT/CT alone reported in the literature is usually lower than sensitivity, especially for PJI. The evidence in the literature shows heterogeneity of data concerning the diagnostic accuracy of bone scintigraphy but demonstrates lower specificity than all other nuclear imaging modalities [
51]. Several meta-analyses showed a pooled specificity of 56% (95% CI, 47–64%) for bone scintigraphy [
51] or a pooled sensitivity and specificity of 80% (95% CI, 72–86%) and 69% (95% CI, 91–99%) [
9]. The reported isotope distribution patterns on bone scans are less specific for infection and a bone scan is not recommended for PJI diagnosis as a single modality. On the contrary, a recent study published by Bäcker et al. showed very high sensitivity, specificity, positive predictive value, and negative predictive value for loosening of SPECT/CT, of 93%, 97%, 90%, and 100%, respectively [
52]. The authors reported the results of MRI and dual-phase bone scan with SPECT/CT with very high accuracy of both modalities. Loosening in this study was diagnosed according to the combined SPECT/CT criteria published by Dobrindt et al. [
53].
It should be additionally mentioned that bone scintigraphy, especially in combination with CT, can help to assess other abnormalities causing chronic pain, such as heterotopic ossification, “hot patella” sign, periprosthetic fractures, wear-associated osteolysis, histiocytic reaction, or fluid collections [
52,
54].
In our institution, bone SPECT/CT remains the first nuclear imaging modality in patients with a low probability of infection in THA and TKA, which is in agreement with recently suggested diagnostic flowcharts [
6,
22]. The results of bone SPECT/CT in our study were not categorized as possible PJI, as it was beyond the scope of this study and therefore not included in the statistical analysis. The aim of performing this modality was to detect possible periprosthetic loosening as much as negative cases or other possible post-operative complications causing chronic pain and comparing findings with dual-isotope SPECT/CT and FDG PET/CT.
In the case of a positive bone scan, another nuclear imaging modality is necessary in patients suspected of having PJI. The standard of care in these cases is radiolabeled WBC scintigraphy [
9,
22,
49], with
99mTc_HMPAO or
111In-oxine, which can confirm or rule out infection with high diagnostic accuracy, especially if performed using EANM standardized criteria for the labeling procedure, acquisition, and interpretation [
9,
11,
40,
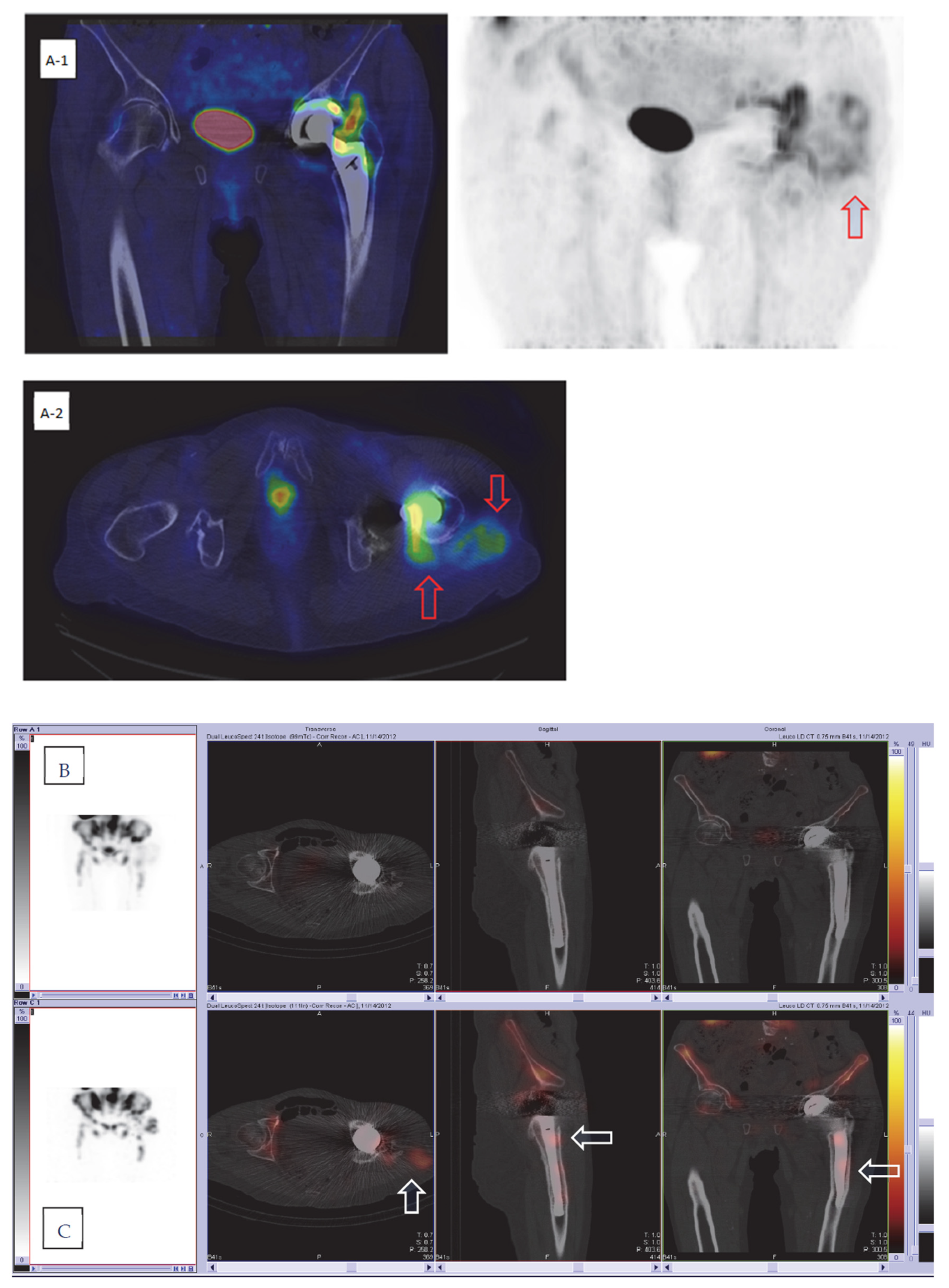
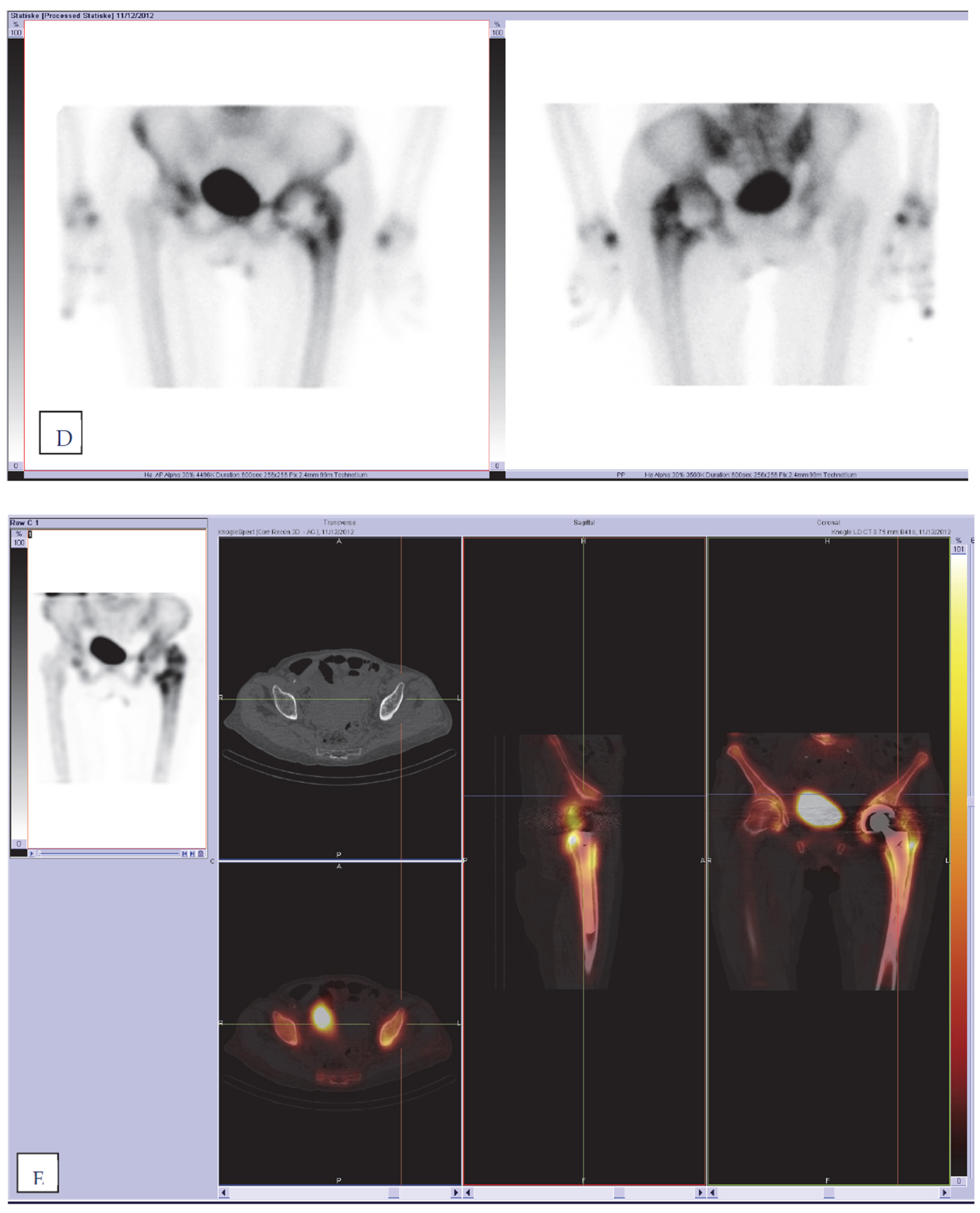
51]. Radiolabeled leucocytes accumulate not only in infections, but also physiologically in the active reticuloendothelial component of bone marrow. The distribution of bone marrow is affected by joint prostheses, making it difficult to differentiate labeled leukocyte accumulation in infection from accumulation in atypically located but otherwise normal marrow. This differentiation is accomplished by complementary bone marrow imaging with
99mTc-sulfur colloid. Leukocytes and sulfur colloids both accumulate in the reticuloendothelial cells of the bone marrow, and tracer uptake on both scan types indicates the presence of physiological uptake in atypically located bone marrow and thus allows us to reduce the number of false-positive cases in WBC scintigraphy.
In vitro leucocyte labeling with
111In-oxine has been used in humans for infection imaging for more than 50 years [
55], and since 1988 has been largely replaced by
99mTc-HMPAO [
56]. Nowadays, WBC labeling with
111In-oxine or
99mTc-HMPAO is a well-established technique in Europe [
29,
56], but the procedure requires highly specific laboratories and qualified personnel validated for the WBC labeling process and handling the blood components of the patient who could potentially be infected, and it is time consuming. WBC scans require 24 to 72 h before results are obtained. Despite these disadvantages, scintigraphy with labeled autologous WBSs is a widely used method and remains the most specific imaging technique for detecting sites of infection. The study by Palestro et al. from 1990 demonstrated high diagnostic accuracy on combined
111In-labeled leucocyte and bone marrow imaging in PJI; the results demonstrated a sensitivity, a specificity, and an accuracy of 100%, 97%, and 98%, respectively [
37]. Some later published papers reported slightly different diagnostic accuracy for combining techniques, ranging from 86% to 98% [
18]; the sensitivity, specificity, and accuracy reported by Love C et al. were 100%, 91%, and 95%, respectively [
57,
58]; those reported by El Esper et al. were 80%, 94%, and 91%, respectively [
59]; and those reported by Brammen L et al. were 60%, 97%, and 90%, respectively [
60]. Different results in reported studies can be explained by the use of different acquisition protocols and interpretations. The low sensitivity reported by Brammen et al. could be rated to 100% after reviewing imaging by one of the leading nuclear medicine specialists, demonstrating the importance of standardized image interpretation by experts [
60]. The latest reviews and meta-analysis obtained from papers with consistent combined techniques show a pooled specificity of 92% (95% CI, 84–97%) [
51] and diagnostic accuracy ranging from 83% to 98% for both hip and knee prosthesis infections [
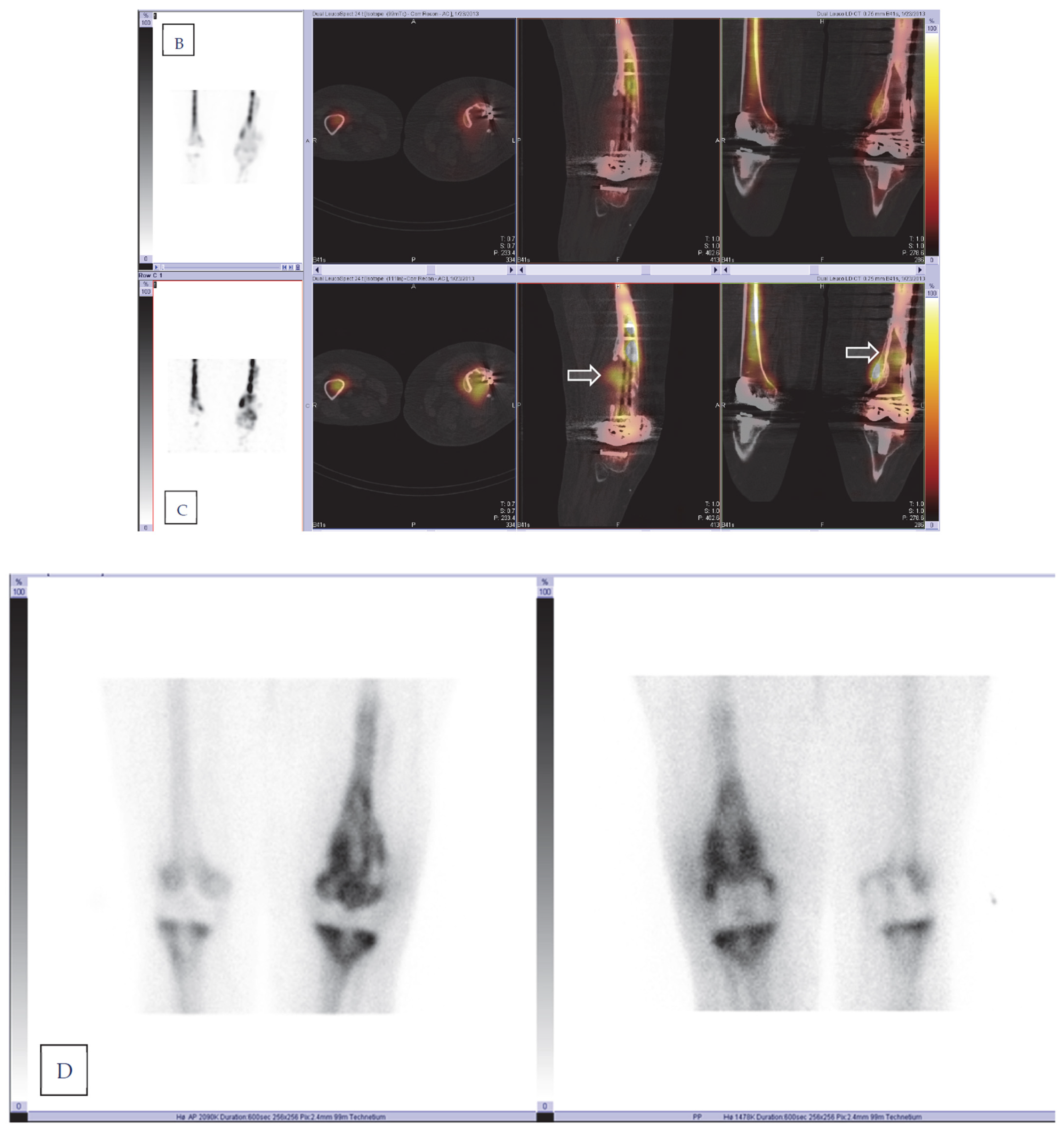
49]. In our study, we performed a combined dual-isotope
111In-labeled WBC/
99mTc-Nanocoll bone marrow scan with the SPECT/CT technique, which was standardized in accordance with the European Society of Nuclear Medicine guidelines. This advanced hybrid combination of two nuclear imaging modalities with CT has been shown to have the highest diagnostic accuracy. Adding SPECT/CT can increase the diagnostic accuracy in the case of PJI due to its better resolution and morphological information [
6,
54,
61]. The specificity for SPECT/CT compared with SPECT alone combined with different tracers can be increased by up to 38% [
6].
The results of dual-isotope imaging SPECT/CT in our study demonstrate high sensitivity, specificity, diagnostic accuracy, and NPV values, with 100%, 97%, 98%, and 100%, respectively, compared to the gold standard and comparable to the overall accuracy reported in the literature. However, there are some limitations which must be discussed. The estimates on diagnostic accuracy presented extremely high, and the confidence intervals skew to the left. When corrected to skewness in confidence intervals, the sensitivity and specificity are 88% and 92%, respectively. Another limitation of this analysis is that seven patients lacking the gold standard were excluded due to equivocal clinical follow-up results. When these inconclusive clinical results were categorized in contrast to imaging results, the sensitivity, specificity, and diagnostic accuracy were significantly lower at 76%, 88%, and 84%, respectively. Interestingly, the imaging results for all seven patients were consistent on both dual-isotope and PET/CT; therefore, the accuracy in the “worst-case” analysis may be considered underestimated.
In our institution, dual-isotope WBC/bone marrow imaging performed with the SPECT/CT technique is included in the diagnostic imaging algorithm in daily clinical practice for THA and TKA chronic periprosthetic problems if bone scans cannot rule out PJI. The labeling in our institution is performed with
111In-oxine. When comparing imaging with
99mTc-HMPAO to
111In-oxine-labeled WBC, there are some advantages and disadvantages. The main advantage of
111In-oxine over
99mTc-HMPAO is the higher labeling efficiency (LE) and less efflux of radioactivity from the labeled WBC. The most important disadvantage, however, is the radiation exposure of labeled cells, critical organs (spleen), and the whole body to
111In-oxine, which is substantially higher than that from
99mTc-HMPAO. Planar images obtained with
111In-labeled WBC are of substantially lower quality than those obtained with
99mTc-labeled WBC. SPECT images of
111In-labeled WBC are of very low quality as well, unless the acquisition time is largely increased. On the other hand, the use of
111In-oxine-labeled WBC does not interfere with imaging of
99mTc-nanocolloids, because different energy windows can be used to detect
99mTc and
111In simultaneously [
29,
56]. Fluorine-18 fluorodeoxyglucose positron emission tomography (
18F-FDG-PET), which is primarily used for the localization of malignancy, has also demonstrated utility for the detection of infection or inflammation. FDG is a glucose analog that is primarily taken up by high-glucose-consuming cells, including inflammatory cells such as neutrophils and monocytes [
62]. The nonspecific mechanism of
18F-FDG uptake has been shown to be beneficial in terms of its high sensitivity and high negative predictive value but has a limitation of low specificity for imaging inflammation and infection. The diagnostic performance of
18F-FDG PET/CT in detecting PJI in hip and knee replacements has been increasingly proven in the literature to not be inferior to labeled leukocyte scintigraphy [
1,
5,
9,
49,
51]. The joint EANM/SNMMI guidelines for the use of FDG in inflammation and infection reported an overall sensitivity of 96% for FDG PET and a specificity of 98% for knee and hip PJI [
32]. A recent meta-analysis of the diagnostic performance of FDG PET/CT reported a poled sensitivity of 86% (95% CI, 80–90%) and a pooled specificity of 93% (95% CI, 90–95%) for hip prostheses for FDG PET/CT [
9]. Another meta-analysis of the diagnostic performance of FDG PET/CT reported a pooled sensitivity of 70% (95% CI, 56–81%) and a pooled specificity of 84% (95% CI, 76–90%) for knee prostheses [
51]. Results from a recently published meta-analysis by Kim showed a pooled sensitivity of 0.88 (95% CI; 0.80–0.93) and a pooled specificity of 0.89 (95% CI; 2 0.83–0.93) for the detection of PPI of lower limb arthroplasty of the 19 included studies [
63].
There are few published papers that directly compare FDG PET/CT and WBC scintigraphy in prosthetic infections, and the tested interpretation criteria are different [
6]. The results from these studies are heterogeneous [
5], but all papers confirm the lower specificity of FDG PET/CT compared with WBC scintigraphy in PJI [
57,
58,
64,
65,
66]. In our study, the overall accuracy was significantly lower for FDG PET/CT (79%) than for dual-isotope WBC/bone marrow scintigraphy (98%). In the case of the “worst-case scenario”, the diagnostic accuracy for FDG PET/CT was lower compared with dual-isotope WBC/bone marrow scintigraphy. The results from our study are comparable to the accuracy reported in the literature, but the heterogeneity of the reported diagnostic performance of FDG PET/CT in PJI in the literature should be mentioned. Even though the diagnostic accuracy of FDG PETC/CT in pooled data in meta-analysis was high, the ranges for both sensitivity and specificity in individual studies were quite large (sensitivity 28–91% and specificity 34–97%) [
6]. As reported by Signore et al., this is largely attributable to the differences in study design and interpretation criteria [
6]. Therefore, standardization of acquisition protocols, diagnostic criteria, and reference standards is required for further validation of the method [
5,
67]. Furthermore,
18F-FDG PET/CT has been increasingly used in evaluating not only in oncological cases, but also patients with different infectious and inflammatory diseases, fever of unknown origin, as well as spondylodiscitis [
7], in which interpretation of periprosthetic FDG uptake can be necessary due to the increasing number of joint replacements in the population. Thus, validated uptake interpretation criteria are necessary.
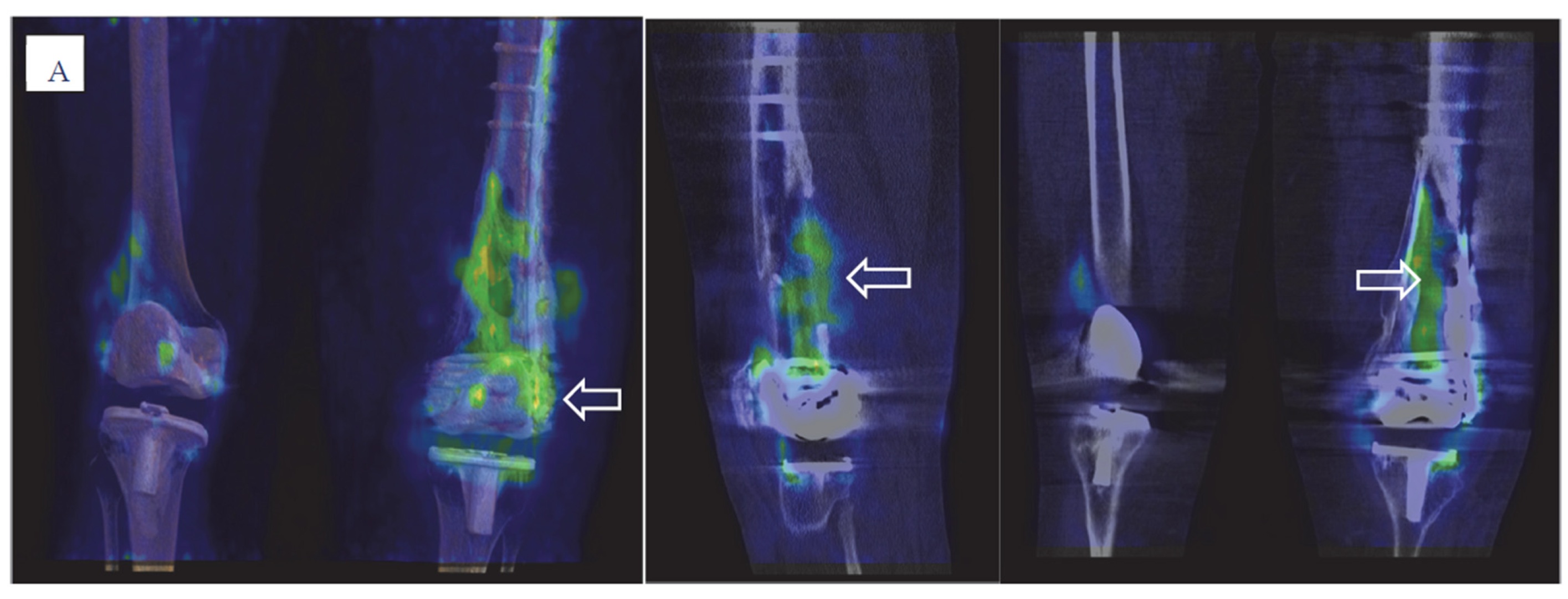
In our study, FDG PET/CT imaging was reported as suspected for PJI in 27 patients, where 10 cases (21%) (six knee and four hip prostheses) reported false positivity compared to the gold standard. In this false-positive group, three patients did not undergo dual-isotope scans due to technical issues, but seven patients underwent either revision (six) or joint aspiration with negative microbiological culturing results. In this group, uptake on FDG PET/CT was suspected due to more intense uptake in either periarticular soft tissue and/or the bone–prosthesis interface. In one case (TKA), both dual-isotope and FDG PET/CT were reported as suspected for PJI, where increased FDG and leucocyte uptake was reported in periarticular soft tissue and capsule and most likely represented tissue-reactive changes and/or synovitis. The limitations of the study should be discussed. One of the limitations of the study was that bioptic procedures and microbiological culturing were not feasible for a sizable portion of the patients. Therefore, both microbiological culturing and clinical follow-up results served as the gold standard in our study. Joint aspiration was discouraged in the initial evaluation due to possible interference with nuclear imaging. After imaging, joint aspiration or biopsies were discouraged for 38% of the patients due to negative imaging results. Joint aspiration itself involves a risk of infection, and its sensitivity is highly variable [
6]. False-negative cultures are reported in the literature in approximately 20% of PJIs [
7]. In our study, in five patients (11%), the invasive procedures were not performed despite both dual-isotope and
18F-FDG PET/CT imaging being suspected for PJI and the procedures were recommended. These patients did not undergo surgery due to severe comorbidities, mild symptoms, and other factors. To overcome this limitation, all patients were clinically followed up with and ultimately evaluated at the clinical follow-up and post hoc MDT. A further limitation is previously mentioned few equivocal imaging studies in which consensus between the readers could not be achieved and the results were discussed at the post-imaging MDT together with clinical data. The study was prospectively designed, addressed the daily clinical situation, and, in some cases, imaging results can be best interpreted and used in conjunction with the patient’s specific presentation [
68]. The rest of the imaging results were not changed after the multidisciplinary team conferences.
A further limitation of the study was that seven patients were excluded from the final statistical analysis due to inconclusive final clinical MDT decisions. Interestingly, the results for both dual-isotope WBC/bone marrow scintigraphy and
18F-FDG PET/CT were consistent in all seven patients (
Table 3), but no consensus could be reached from the clinical point of view at the time of the study. This limitation was fulfilled by additional statistical analysis, which we previously discussed.
One of the major limitations of the study is the small sample size. Post hoc power analysis [
69,
70] with the shown sensitivity and specificity in our study and CI 0.1 showed extremely high sample sizes for both imaging modalities (around 13,000 for knee PJI and 3500 for hip) calculated for the incidence of PJI in the cohort [
71]. Therefore, the superiority of one imaging modality should be determined with caution.
Exposure to ionizing radiation is additionally an important issue. The level of radiation exposure of nuclear medicine examinations is similar to that of CT scans, ranging from 2 to 15 milliSieverts (mSv), with the highest radiation exposure for tumor imaging with FDG PET/CT [
10]. In our study, an individual risk assessment was performed prior to every examination, with patients’ acceptance. However, three different nuclear medicine imaging modalities are not recommended in a daily routinely clinical practice for PJI in THA and TKA, as both WBC/bone marrow scan and FDG PET/CT show high diagnostic accuracy and can be selected according to local rules, expertise, and technical availabilities. Diagnostic strategies, though, differ between countries and nuclear imaging can be less important and less used than clinical examination and aspiration for further decision making.


 ,
, 

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}







