
Non-Invasive Assessment of Congestion by Cardiovascular and Pulmonary Ultrasound and Biomarkers in Heart Failure


Abstract
:1. Background
2. Echocardiography and Vascular Ultrasound
2.1. Left and Right Ventricular Filling Pressures
2.1.1. Left Ventricular Filling Pressures and Pulmonary Congestion
Mitral Inflow Velocities and E/A Ratio
E/e’ Ratio
Peak Tricuspid Regurgitation (TR) Velocity and Systolic Pulmonary Artery Pressure (sPAP) Estimation
Left Atrial Maximal Volume Index
LA Function
2.1.2. Right Ventricular Filling Pressure and Systemic Congestion
Inferior Vena Cava
Doppler Flow in the Hepatic Veins
Ultrasonographic Evaluation of Intrarenal Venous Flow
Ultrasonographic Evaluation of the Internal Jugular Vein
3. Imaging of Pulmonary Congestion
3.1. Chest Radiography and Computer Tomography
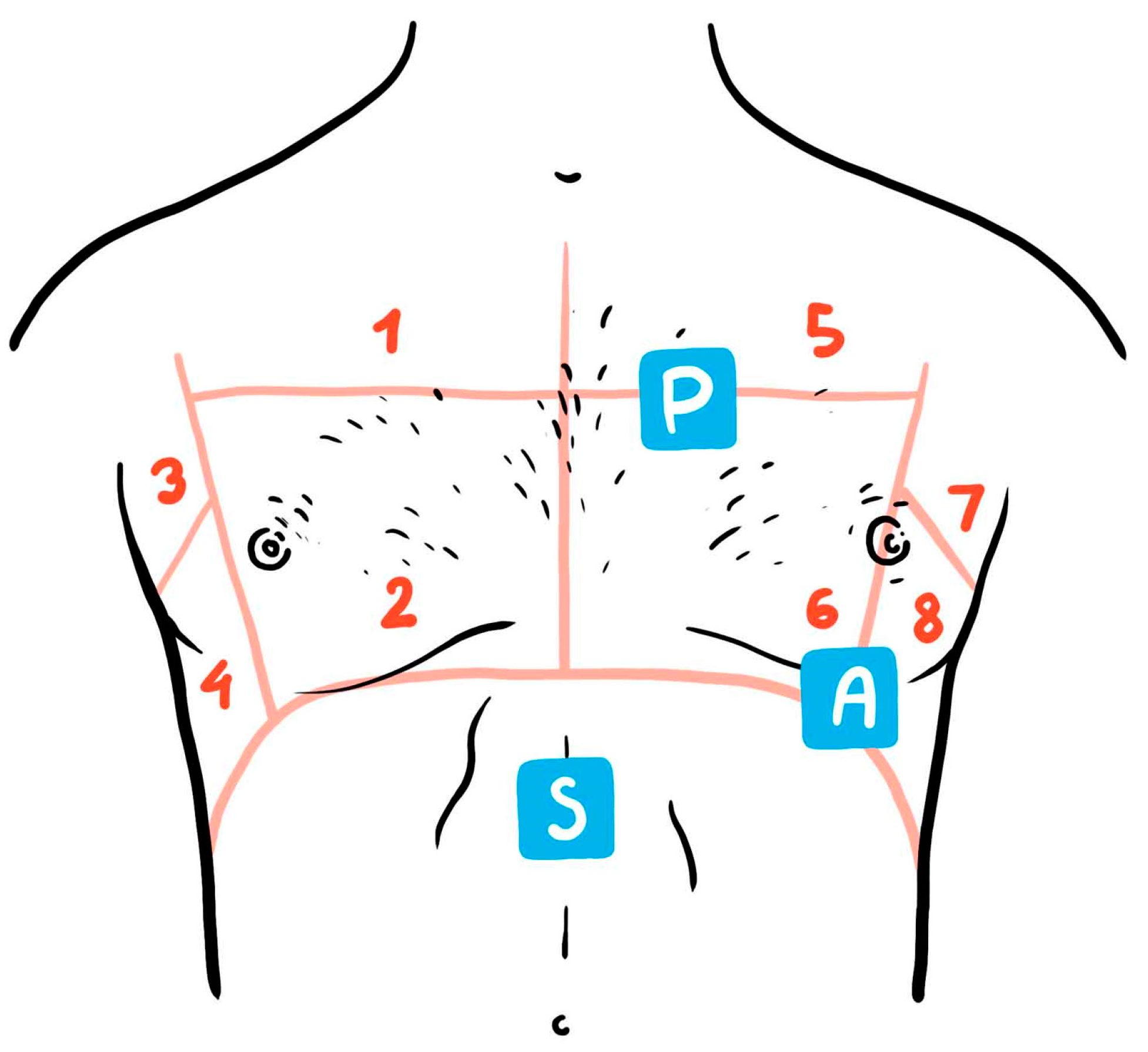
3.2. Lung Ultrasound
3.2.1. The Role in HF Diagnosis
3.2.2. The Role in Monitoring Congestion
3.2.3. The Prognostic Role
3.2.4. Limitations
4. Biomarkers
4.1. Natriuretic Peptides

{kind=link}
{kind=link}
| HF Clinical Setting | NT-ProBNP (pg/mL) | BNP (pg/mL) | MR-ProANP (pg/mL) | Comments | ||
|---|---|---|---|---|---|---|
| Rule-In | Rule-Out | Rule-In | Rule-Out | Rule-Out | ||
| Suspected acute HF (Patients with acute dyspnoea) * | Age–related <50 y >450 51–75 y >900 >75 y >1800 | <300 | >400 | <100 | <120 | Higher NP levels in HFREF vs HFPEF [13] Less data for MR-proANP |
| Suspected acute HF and eGFR < 60 mL/min | Same as in suspected Acute HF | <200 | - | No supplementary correction recommended for NT-proBNP age-adjusted cut-offs due to correspondence between renal function decline and increasing age [13] | ||
| Suspected acute HF and AF | >600 (SOCRATES trial [106]) >900 (PARAGON trial [107]) | <400 | >240 | <150 | - | Higher NP levels occasionally observed in patients with AF but no clinical data to sustain HF diagnosis [108] In HFPEF trials, the NP cut-off values as inclusion criteria were higher in patients with AF vs sinus rhythm [106,107] |
| Suspected acute HF and obesity > 30 kg/m2 | Lowering the cut-off levels by up to 50% | <50 | - | Presumed overlap between NP levels in HFPEF and obesity [109] | ||
| HF in the community (Non-acute setting) | >600 | <125 | >150 | <35 | <40 | NP serial dosing during follow-up in conjunction with symptoms and weight gain are recommended in order to recognize early decompensation [13]. |
4.2. Cardiac Troponin: Conventional and High-Sensitivity Assays
4.3. Emerging Congestion Biomarkers of Cardiac Origin
4.3.1. Soluble Suppression of Tumorigenesis-2
4.3.2. Carbohydrate Antigen 125 (CA125)
4.3.3. Soluble Melanoma Cell Adhesion Molecule (CD146)
4.3.4. Mid-Regional Pro-Adrenomedullin (MR-ProADM)
4.4. Other Biomarkers of Systemic Congestion
4.4.1. Renal Function Biomarkers
4.4.2. Liver Function Biomarkers
4.4.3. Haemoconcentration
4.5. Point of Care Testing
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Chioncel, O.; Mebazaa, A.; Harjola, V.-P.; Coats, A.J.; Piepoli, M.F.; Crespo-Leiro, M.G.; Laroche, C.; Seferovic, P.M.; Anker, S.D.; Ferrari, R.; et al. Clinical phenotypes and outcome of patients hospitalized for acute heart failure: The ESC Heart Failure Long-Term Registry. Eur. J. Heart Fail. 2017, 19, 1242–1254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ross, J.S.; Chen, J.; Lin, Z.; Bueno, H.; Curtis, J.P.; Keenan, P.S.; Normand, S.-L.T.; Schreiner, G.; Spertus, J.A.; Vidán, M.T.; et al. Recent National Trends in Readmission Rates After Heart Failure Hospitalization. Circ. Heart Fail. 2010, 3, 97–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Setoguchi, S.; Stevenson, L.W. Hospitalizations in Patients with Heart Failure: Who and Why. J. Am. Coll. Cardiol. 2009, 54, 1703–1705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verbrugge, F.H.; Guazzi, M.; Testani, J.M.; Borlaug, B.A. Altered hemodynamics and end-organ damage in heart failure: Impact on the Lung and kidney. Circulation 2020, 142, 998–1012. [Google Scholar] [CrossRef]
- Van Aelst, L.N.; Arrigo, M.; Plácido, R.; Akiyama, E.; Girerd, N.; Zannad, F.; Manivet, P.; Rossignol, P.; Badoz, M.; Sadoune, M.; et al. Acutely decompensated heart failure with preserved and reduced ejection fraction present with comparable haemodynamic congestion. Eur. J. Heart Fail. 2018, 20, 738–747. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, L.W.; Zile, M.; Bennett, T.D.; Kueffer, F.J.; Jessup, M.L.; Adamson, P.; Abraham, W.T.; Manda, V.; Bourge, R.C. Chronic Ambulatory Intracardiac Pressures and Future Heart Failure Events. Circ. Heart Fail. 2010, 3, 580–587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Girerd, N.; Seronde, M.-F.; Coiro, S.; Chouihed, T.; Bilbault, P.; Braun, F.; Kenizou, D.; Maillier, B.; Nazeyrollas, P.; Roul, G.; et al. Integrative Assessment of Congestion in Heart Failure Throughout the Patient Journey. JACC Heart Fail. 2018, 6, 273–285. [Google Scholar] [CrossRef] [PubMed]
- Metra, M.; Davison, B.; Bettari, L.; Sun, H.; Edwards, C.; Lazzarini, V.; Piovanelli, B.; Carubelli, V.; Bugatti, S.; Lombardi, C.; et al. Is worsening renal function an ominous prognostic sign in patients with acute heart failure? The role of congestion and its interaction with renal function. Circ. Heart Fail. 2012, 5, 54–62. [Google Scholar] [CrossRef] [Green Version]
- Maggioni, A.P.; Dahlström, U.; Filippatos, G.; Chioncel, O.; Crespo Leiro, M.; Drozdz, J.; Fruhwald, F.; Gullestad, L.; Logeart, D.; Fabbri, G.; et al. EURObservational Research Programme: Regional differences and 1-year follow-up results of the Heart Failure Pilot Survey (ESC-HF Pilot). Eur. J. Heart Fail. 2013, 15, 808–817. [Google Scholar] [CrossRef] [Green Version]
- Rubio-Gracia, J.; Demissei, B.G.; ter Maaten, J.M.; Cleland, J.G.; O’Connor, C.M.; Metra, M.; Ponikowski, P.; Teerlink, J.R.; Cotter, G.; Davison, B.A.; et al. Prevalence, predictors and clinical out-come of residual congestion in acute decompensated heart failure. Int. J. Cardiol. 2018, 258, 185–191. [Google Scholar] [CrossRef] [Green Version]
- Allen, L.A.; Gheorghiade, M.; Reid, K.J.; Dunlay, S.M.; Chan, P.S.; Hauptman, P.J.; Zannad, F.; Konstam, M.A.; Spertus, J.A. Identifying Patients Hospitalized with Heart Failure at Risk for Unfavorable Future Quality of Life. Circ. Cardiovasc. Qual. Outcomes 2011, 4, 389–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunlay, S.M.; Gheorghiade, M.; Reid, K.J.; Allen, L.A.; Chan, P.S.; Hauptman, P.J.; Zannad, F.; Maggioni, A.P.; Swedberg, K.; Konstam, M.A.; et al. Critical elements of clinical follow-up after hospital discharge for heart failure: Insights from the EVEREST trial. Eur. J. Heart Fail. 2010, 12, 367–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mueller, C.; McDonald, K.; de Boer, R.A.; Maisel, A.; Cleland, J.G.; Kozhuharov, N.; Coats, A.J.; Metra, M.; Mebazaa, A.; Ruschitzka, F.; et al. Heart Failure Association of the European Society of Cardiology practical guidance on the use of natriuretic peptide concentrations. Eur. J. Heart Fail. 2019, 21, 715–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cox, E.G.M.; Koster, G.; Baron, A.; Kaufmann, T.; Eck, R.J.; Veenstra, T.C.; Hiemstra, B.; Wong, A.; Kwee, T.C.; Tulleken, J.E.; et al. Should the ultrasound probe replace your stethoscope? A SICS-I sub-study comparing lung ultrasound and pulmonary auscultation in the critically ill. Crit. Care 2020, 24, 14. [Google Scholar] [CrossRef] [Green Version]
- Arts, L.; Lim, E.H.T.; Van De Ven, P.M.; Heunks, L.; Tuinman, P.R. The diagnostic accuracy of lung auscultation in adult patients with acute pulmonary pathologies: A meta-analysis. Sci. Rep. 2020, 10, 7347. [Google Scholar] [CrossRef] [PubMed]
- Ambrosy, A.P.; Cerbin, L.P.; Armstrong, P.; Butler, J.; Coles, A.; DeVore, A.D.; Dunlap, M.E.; Ezekowitz, J.; Felker, G.M.; Fudim, M.; et al. Body Weight Change During and After Hospitalization for Acute Heart Failure: Patient Characteristics, Markers of Congestion, and Outcomes: Findings from the ASCEND- HF Trial. JACC Heart Fail. 2017, 5, 1–13. [Google Scholar] [CrossRef]
- Mullens, W.; Damman, K.; Harjola, V.-P.; Mebazaa, A.; Rocca, H.-P.B.-L.; Martens, P.; Testani, J.M.; Tang, W.W.; Orso, F.; Rossignol, P.; et al. The use of diuretics in heart failure with congestion—A position statement from the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2019, 21, 137–155. [Google Scholar] [CrossRef]
- Beaubien-Souligny, W.; Rola, P.; Haycock, K.; Bouchard, J.; Lamarche, Y.; Spiegel, R.; Denault, A.Y. Quantifying systemic congestion with Point-Of-Care ultrasound: Development of the venous excess ultrasound grading system. Ultrasound J. 2020, 12, 16. [Google Scholar] [CrossRef] [Green Version]
- Narula, J.; Chandrashekhar, Y.; Braunwald, E. Time to Add a Fifth Pillar to Bedside Physical Examination: Inspection, Palpation, Percussion, Auscultation, and Insonation. JAMA Cardiol. 2018, 3, 346–350. [Google Scholar] [CrossRef]
- Smiseth, O.A.; Morris, D.A.; Cardim, N.; Cikes, M.; Delgado, V.; Donal, E.; Flachskampf, F.A.; Galderisi, M.; Gerber, B.L.; Gimelli, A.; et al. Multimodality imaging in patients with heart failure and preserved ejection fraction: An expert consensus document of the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2022, 23, e34–e61. [Google Scholar] [CrossRef]
- Kasner, M.; Westermann, D.; Steendijk, P.; Gaub, R.; Wilkenshoff, U.; Weitmann, K.; Hoffmann, W.; Poller, W.; Schultheiss, H.-P.; Pauschinger, M.; et al. Utility of Doppler echocardiography and tissue Doppler imaging in the estimation of diastolic function in heart failure with normal ejection fraction: A comparative Doppler-conductance catheterization study. Circulation 2007, 116, 637–647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F., III; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferre, R.M.; Chioncel, O.; Pang, P.S.; Lang, R.M.; Gheorghiade, M.; Collins, S.P. Acute heart failure: The role of focused emergency cardiopulmonary ultrasound in identification and early management. Eur. J. Heart Fail. 2015, 17, 1223–1227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mullens, W.; Borowski, A.G.; Curtin, R.J.; Thomas, J.D.; Tang, W.H.W. Tissue Doppler Imaging in the Estimation of Intracardiac Filling Pressure in Decompensated Patients with Advanced Systolic Heart Failure. Circulation 2009, 119, 62–70. [Google Scholar] [CrossRef]
- Balaney, B.; Medvedofsky, D.; Mediratta, A.; Singh, A.; Ciszek, B.; Kruse, E.; Shah, A.P.; Addetia, K.; Lang, R.M.; Mor-Avi, V. Invasive Validation of the Echocardiographic Assessment of Left Ventricular Filling Pressures Using the 2016 Diastolic Guidelines: Head-to-Head Comparison with the 2009 Guidelines. J. Am. Soc. Echocardiogr. 2018, 31, 79–88. [Google Scholar] [CrossRef] [Green Version]
- Lancellotti, P.; Galderisi, M.; Edvardsen, T.; Donal, E.; Goliasch, G.; Cardim, N.; Magne, J.; Laginha, S.; Hagendorff, A.; Haland, T.F.; et al. Echo-Doppler estimation of left ventricular filling pressure: Results of the multicentre EACVI Euro-Filling study. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 961–968. [Google Scholar] [CrossRef]
- Dabestani, A.; Mahan, G.; Gardin, J.M.; Takenaka, K.; Burn, C.; Allfie, A.; Henry, W.L. Evaluation of pulmonary artery pressure and resistance by pulsed Doppler echocardiography. Am. J. Cardiol. 1987, 59, 662–668. [Google Scholar] [CrossRef]
- Shah, A.M.; Claggett, B.; Sweitzer, N.K.; Shah, S.J.; Anand, I.S.; O’Meara, E.; Desai, A.S.; Heitner, J.F.; Li, G.; Fang, J.; et al. Cardiac structure and function and prognosis in heart failure with preserved ejection fraction: Findings from the echocardiographic study of the Treatment of Preserved Cardiac Function Heart Failure with an Aldosterone Antagonist (TOPCAT) Trial. Circ. Heart Fail. 2014, 7, 740–751. [Google Scholar] [CrossRef] [Green Version]
- Nagueh, S.F.; Appleton, C.P.; Gillebert, T.; Marino, P.; Oh, J.K.; Smiseth, O.A.; Waggoner, A.D.; Flachskampf, F.A.; Pellikka, P.A.; Evangelisa, A. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography. Eur. J. Echocardiogr. 2009, 10, 165–193. [Google Scholar] [CrossRef] [Green Version]
- Andersen, O.S.; Smiseth, O.A.; Dokainish, H.; Abudiab, M.M.; Schutt, R.C.; Kumar, A.; Sato, K.; Harb, S.; Gude, E.; Remme, E.W.; et al. Estimating Left Ventricular Filling Pressure by Echocardiography. J. Am. Coll. Cardiol. 2017, 69, 1937–1948. [Google Scholar] [CrossRef]
- Inoue, K.; Khan, F.H.; Remme, E.W.; Ohte, N.; García-Izquierdo, E.; Chetrit, M.; Moñivas-Palomero, V.; Mingo-Santos, S.; Andersen, S.; Gude, E.; et al. Determinants of left atrial reservoir and pump strain and use of atrial strain for evaluation of left ventricular filling pressure. Eur. Heart J. Cardiovasc. Imaging 2021, 23, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Milan, A.; Magnino, C.; Veglio, F. Echocardiographic indexes for the non-invasive evaluation of pulmonary hemodynamics. Am. Soc. Echocardiogr. 2010, 23, 225–239. [Google Scholar] [CrossRef] [PubMed]
- Brennan, J.M.; Blair, J.E.; Goonewardena, S.; Ronan, A.; Shah, D.; Vasaiwala, S.; Brooks, E.; Levy, A.; Kirkpatrick, J.N.; Spencer, K.T. A Comparison by Medicine Residents of Physical Examination Versus Hand-Carried Ultrasound for Estimation of Right Atrial Pressure. Am. J. Cardiol. 2007, 99, 1614–1616. [Google Scholar] [CrossRef] [PubMed]
- Blair, J.E.; Brennan, J.M.; Goonewardena, S.N.; Shah, D.; Vasaiwala, S.; Spencer, K.T. Usefulness of Hand-Carried Ultrasound to Predict Elevated Left Ventricular Filling Pressure. Am. J. Cardiol. 2009, 103, 246–247. [Google Scholar] [CrossRef] [PubMed]
- Dokainish, H.; Nguyen, J.S.; Bobek, J.; Goswami, R.; Lakkis, N.M. Assessment of the American Society of Echocardiography-European Association of Echocardiography guidelines for diastolic function in patients with depressed ejection fraction: An echocardiographic and invasive haemodynamic study. Eur. J. Echocardiogr. 2011, 12, 857–864. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miglioranza, M.H.; Gargani, L.; Sant’Anna, R.T.; Rover, M.M.; Martins, V.M.; Mantovani, A.; Weber, C.; Moraes, M.A.; Feldman, C.J.; Kalil, R.A.K.; et al. Lung ultrasound for the evaluation of pulmonary congestion in outpatients: A comparison with clinical assessment, natriuretic peptides, and echocardiography. JACC Cardiovasc. Imaging 2013, 6, 1141–1151. [Google Scholar] [CrossRef] [Green Version]
- Öhman, J.; Harjola, V.-P.; Karjalainen, P.; Lassus, J. Focused echocardiography and lung ultrasound protocol for guiding treatment in acute heart failure. ESC Heart Fail. 2018, 5, 120–128. [Google Scholar] [CrossRef]
- Burnett, J.C., Jr.; Knox, F.G. Renal interstitial pressure and sodium excretion during renal vein constriction. Am. J. Physiol. Renal Physiol. 1980, 238, F279–F282. [Google Scholar] [CrossRef]
- Tang, W.H.; Kitai, T. Intrarenal Venous Flow: A Window into the Congestive Kidney Failure Phenotype of Heart Failure? JACC Heart Fail. 2016, 4, 683–686. [Google Scholar] [CrossRef]
- Nijst, P.; Martens, P.; Dupont, M.; Tang, W.W.; Mullens, W. Intrarenal Flow Alterations During Transition from Euvolemia to Intravascular Volume Expansion in Heart Failure Patients. JACC Heart Fail. 2017, 5, 672–681. [Google Scholar] [CrossRef]
- Ter Maaten, J.M.; Dauw, J.; Martens, P.; Somers, F.; Damman, K.; Metalidis, C.; Nijst, P.; Dupont, M.; Mullens, W. The Effect of Decongestion on Intrarenal Venous Flow Patterns in Patients with Acute Heart Failure. J. Card. Fail. 2021, 27, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, M.; Seo, Y.; Iida, N.; Ishizu, T.; Yamada, Y.; Nakatsukasa, T.; Nakagawa, D.; Kawamatsu, N.; Sato, K.; Machino-Ohtsuka, T.; et al. Prognostic Impact of Changes in Intrarenal Venous Flow Pattern in Patients with Heart Failure. J. Card. Fail. 2021, 27, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Bateman, G.A.; Cuganesan, R. Renal Vein Doppler Sonography of Obstructive Uropathy. AJR. Am. J. Roentgenol. 2002, 178, 921–925. [Google Scholar] [CrossRef] [PubMed]
- Pellicori, P.; Kallvikbacka-Bennett, A.; Zhang, J.; Khaleva, O.; Warden, J.; Clark, A.L.; Cleland, J.G. Revisiting a classical clinical sign: Jugular venous ultrasound. Int. J. Cardiol. 2014, 170, 364–370. [Google Scholar] [CrossRef]
- Pellicori, P.; Kallvikbacka-Bennett, A.; Dierckx, R.; Zhang, J.; Putzu, P.; Cuthbert, J.; Boyalla, V.; Shoaib, A.; Clark, A.L.; Cleland, J.G.F. Prognostic significance of ultrasound-assessed jugular vein distensibility in heart failure. Heart 2015, 101, 1149–1158. [Google Scholar] [CrossRef]
- Simon, M.A.; Kliner, D.E.; Girod, J.P.; Moguillansky, D.; Villanueva, F.S.; Pacella, J.J. Detection of elevated right atrial pressure using a simple bedside ultrasound measure. Am. Heart J. 2010, 159, 421–427. [Google Scholar] [CrossRef]
- Simon, M.A.; Schnatz, R.G.; Romeo, J.D.; Pacella, J.J. Bedside Ultrasound Assessment of Jugular Venous Compliance as a Potential Point-of-Care Method to Predict Acute Decompensated Heart Failure 30-Day Readmission. J. Am. Heart Assoc. 2018, 7, e008184. [Google Scholar] [CrossRef] [Green Version]
- Picano, E.; Scali, M.C. The lung water cascade in heart failure. Echocardiography 2017, 34, 1503–1507. [Google Scholar] [CrossRef]
- Picano, E.; Scali, M.C.; Ciampi, Q.; Lichtenstein, D. Lung Ultrasound for the Cardiologist. JACC Cardiovasc. Imaging 2018, 11, 1692–1705. [Google Scholar] [CrossRef]
- Gargani, L.; Pang, P.S.; Frassi, F.; Miglioranza, M.H.; Dini, F.L.; Landi, P.; Picano, E. Persistent pulmonary congestion before discharge predicts rehospitalization in heart failure: A lung ultrasound study. Cardiovasc. Ultrasound 2015, 13, 40. [Google Scholar] [CrossRef] [Green Version]
- Price, S.; Platz, E.; Cullen, L.; Tavazzi, G.; Christ, M.; Cowie, M.R.; Maisel, A.S.; Masip, J.; Miro, O.; McMurray, J.J.; et al. Acute Heart Failure Study Group of the European Society of Cardiology Acute Cardiovascular Care Association. Expert consensus document: Echocardiography and lung ultrasonography for the assessment and management of acute heart failure. Nat. Rev. Cardiol. 2017, 14, 427–440. [Google Scholar] [CrossRef] [PubMed]
- Cardinale, L.; Priola, A.M.; Moretti, F.; Volpicelli, G. Effectiveness of chest radiography, lung ultrasound and thoracic computed tomography in the diagnosis of congestive heart failure. World J. Radiol. 2014, 6, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Martindale, J.L.; Wakai, A.; Collins, S.P.; Levy, P.D.; Diercks, D.B.; Hiestand, B.C.; Fermann, G.J.; Desouza, I.; Sinert, R. Diagnosing Acute Heart Failure in the Emergency Department: A Systematic Review and Meta-analysis. Acad. Emerg. Med. 2016, 23, 223–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shochat, M.K.; Fudim, M.; Kapustin, D.; Kazatsker, M.; Kleiner, I.; Weinstein, J.M.; Panjrath, G.; Rozen, G.; Roguin, A.; Meisel, S.R. Early Impedance-Guided Intervention Improves Long-Term Outcome in Patients with Heart Failure. J. Am. Coll. Cardiol. 2021, 78, 1751–1752. [Google Scholar] [CrossRef] [PubMed]
- Domenichini, G.; Rahneva, T.; Diab, I.G.; Dhillon, O.S.; Campbell, N.G.; Finlay, M.C.; Baker, V.; Hunter, R.J.; Earley, M.J.; Schilling, R.J. The lung impedance monitoring in treatment of chronic heart failure (the LIMIT-CHF study). Europace 2016, 18, 428–435. [Google Scholar] [CrossRef]
- Picano, E.; Pellikka, P.A. Ultrasound of extravascular lung water: A new standard for pulmonary congestion. Eur. Heart J. 2016, 37, 2097–2104. [Google Scholar] [CrossRef] [Green Version]
- Gargani, L. Lung ultrasound: A new tool for the cardiologist. Cardiovasc. Ultrasound 2011, 9, 6. [Google Scholar] [CrossRef] [Green Version]
- Neskovic, A.N.; Skinner, H.; Price, S.; Via, G.; De Hert, S.; Stankovic, I.; Galderisi, M.; Donal, E.; Muraru, D.; Sloth, E.; et al. Focus cardiac ultrasound core curriculum and core syllabus of the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 475–481. [Google Scholar] [CrossRef]
- Neskovic, A.N.; Hagendorff, A.; Lancellotti, P.; Guarracino, F.; Varga, A.; Cosyns, B.; Flachskampf, F.A.; Popescu, B.A.; Gargani, L.; Zamorano, J.L.; et al. Emergency echocardiography: The European Asso-ciation of Cardiovascular Imaging recommendations. Eur. Heart J. Cardiovasc. Imaging 2013, 14, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Marini, T.J.; Rubens, D.J.; Zhao, Y.T.; Weis, J.; O’Connor, T.P.; Novak, W.H.; Kaproth-Joslin, K.A. Lung Ultrasound: The Essentials. Radiol. Cardiothorac. Imaging 2021, 3, e200564. [Google Scholar] [CrossRef]
- Volpicelli, G. Lung Sonography. J. Ultrasound Med. 2013, 32, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Gargani, L. Ultrasound of the Lungs: More than a Room with a View. Heart Fail. Clin. 2019, 15, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Pivetta, E.; Goffi, A.; Nazerian, P.; Castagno, D.; Tozzetti, C.; Tizzani, P.; Tizzani, M.; Porrino, G.; Ferreri, E.; Busso, V.; et al. Lung ultrasound integrated with clinical assessment for the diagnosis of acute decompensated heart failure in the emergency department: A randomized controlled trial. Eur. J. Heart Fail. 2019, 21, 754–766. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maw, A.M.; Hassanin, A.; Ho, P.M.; McInnes, M.D.F.; Moss, A.; Juarez-Colunga, E.; Soni, N.J.; Miglioranza, M.H.; Platz, E.; DeSanto, K.; et al. Diagnostic Accuracy of Point-of-Care Lung Ultrasonography and Chest Radiography in Adults with Symptoms Suggestive of Acute Decompensated Heart Failure: A Systematic Review and Meta-analysis. JAMA Netw. Open 2019, 2, e190703. [Google Scholar] [CrossRef]
- Al Deeb, M.; Barbic, S.; Featherstone, R.; Dankoff, J.; Barbic, D. Point-of-care Ultrasonography for the Diagnosis of Acute Cardiogenic Pulmonary Edema in Patients Presenting with Acute Dyspnea: A Systematic Review and Meta-analysis. Acad. Emerg. Med. 2014, 21, 843–852. [Google Scholar] [CrossRef]
- Pirrotta, F.; Mazza, B.; Gennari, L.; Palazzuoli, A. Pulmonary Congestion Assessment in Heart Failure: Traditional and New Tools. Diagnostics 2021, 11, 1306. [Google Scholar] [CrossRef]
- Scali, M.C.; Cortigiani, L.; Simionuc, A.; Gregori, D.; Marzilli, M.; Picano, E. Exercise-induced B-lines identify worse functional and prognostic stage in heart failure patients with depressed left ventricular ejection fraction. Eur. J. Heart Fail. 2017, 19, 1468–1478. [Google Scholar] [CrossRef] [Green Version]
- Scali, M.C.; Zagatina, A.; Ciampi, Q.; Cortigiani, L.; D’Andrea, A.; Daros, C.B.; Zhuravskaya, N.; Kasprzak, J.D.; Wierzbowska-Drabik, K.; Luis de Castro, E.S.P.J.; et al. Lung Ultrasound and Pulmonary Congestion During Stress Echocardiography. JACC Cardiovasc. Imaging 2020, 13, 2085–2095. [Google Scholar] [CrossRef]
- Agricola, E.; Picano, E.; Oppizzi, M.; Pisani, M.; Meris, A.; Fragasso, G.; Margonato, A. Assessment of Stress-induced Pulmonary Interstitial Edema by Chest Ultrasound During Exercise Echocardiography and its Correlation with Left Ventricular Function. J. Am. Soc. Echocardiogr. 2006, 19, 457–463. [Google Scholar] [CrossRef]
- Mozzini, C.; Perna, M.D.D.; Pesce, G.; Garbin, U.; Pasini, A.M.F.; Ticinesi, A.; Nouvenne, A.; Meschi, T.; Casadei, A.; Soresi, M.; et al. Lung ultrasound in internal medicine efficiently drives the management of patients with heart failure and speeds up the discharge time. Intern. Emerg. Med. 2018, 13, 27–33. [Google Scholar] [CrossRef]
- Araiza-Garaygordobil, D.; Gopar-Nieto, R.; Martinez-Amezcua, P.; Cabello-López, A.; Alanis-Estrada, G.; Luna-Herbert, A.; González-Pacheco, H.; Paredes-Paucar, C.P.; Sierra-Lara, M.D.; Briseño-De la Cruz, J.L.; et al. A randomized controlled trial of lung ultrasound-guided therapy in heart failure (CLUSTER-HF study). Am. Heart J. 2020, 227, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Pang, P.S.; Russell, F.M.; Ehrman, R.; Ferre, R.; Gargani, L.; Levy, P.D.; Noble, V.; Lane, K.A.; Li, X.; Collins, S.P. Lung Ultrasound–Guided Emergency Department Management of Acute Heart Failure (BLUSHED-AHF): A Randomized Controlled Pilot Trial. JACC Heart Fail. 2021, 9, 638. [Google Scholar] [CrossRef] [PubMed]
- Rivas-Lasarte, M.; Alvarez-Garcia, J.; Fernández-Martínez, J.; Maestro, A.; López-López, L.; Solé-González, E.; Pirla, M.J.; Mesado, N.; Mirabet, S.; Fluvià, P.; et al. Lung ultrasound-guided treatment in ambulatory patients with heart failure: A randomized controlled clinical trial (LUS-HF study). Eur. J. Heart Fail. 2019, 21, 1605–1613. [Google Scholar] [CrossRef]
- Troughton, R.W.; Frampton, C.M.; Yandle, T.; Espine, E.A.; Nicholls, M.G.; Richards, A.M. Treatment of heart failure guided by plasma aminoterminal brain natriuretic peptide (N-BNP) concentrations. Lancet 2000, 355, 1126–1130. [Google Scholar] [CrossRef]
- Bajaj, N.S.; Patel, N.; Prabhu, S.D.; Arora, G.; Wang, T.J.; Arora, P. Effect of NT-proBNP–Guided Therapy on All-Cause Mortality in Chronic Heart Failure with Reduced Ejection Fraction. J. Am. Coll. Cardiol. 2018, 71, 951–952. [Google Scholar] [CrossRef] [PubMed]
- Givertz, M.M.; Stevenson, L.W.; Costanzo, M.R.; Bourge, R.C.; Bauman, J.G.; Ginn, G.; Abraham, W.T.; CHAMPION Trial Investigators. Pulmonary Artery Pressure-Guided Management of Patients with Heart Failure and Reduced Ejection Fraction. J. Am. Coll. Cardiol. 2017, 70, 1875–1886. [Google Scholar] [CrossRef] [PubMed]
- Gargani, L.; Pugliese, N.R.; Frassi, F.; Frumento, P.; Poggianti, E.; Mazzola, M.; De Biase, N.; Landi, P.; Masi, S.; Taddei, S.; et al. Prognostic value of lung ultrasound in patients hospitalized for heart disease irrespective of symptoms and ejection fraction. ESC Heart Fail. 2021, 8, 2660–2669. [Google Scholar] [CrossRef]
- Ambrosy, A.P.; Pang, P.S.; Khan, S.; Konstam, M.A.; Fonarow, G.C.; Traver, B.; Maggioni, A.P.; Cook, T.; Swedberg, K.; Burnett, J.C.; et al. Clinical course and predictive value of congestion during hospitalization in patients admitted for worsening signs and symptoms of heart failure with reduced ejection fraction: Findings from the EVEREST trial. Eur. Heart J. 2013, 34, 835–843. [Google Scholar] [CrossRef] [Green Version]
- Coiro, S.; Porot, G.; Rossignol, P.; Ambrosio, G.; Carluccio, E.; Tritto, I.; Huttin, O.; Lemoine, S.; Sadoul, N.; Donal, E.; et al. Prognostic value of pulmonary congestion assessed by lung ultrasound imaging during heart failure hospitalisation: A two-centre cohort study. Sci. Rep. 2016, 6, 39426, Erratum in Sci. Rep. 2017, 7, 43972. [Google Scholar] [CrossRef] [Green Version]
- Coiro, S.; Rossignol, P.; Ambrosio, G.; Carluccio, E.; Alunni, G.; Murrone, A.; Tritto, I.; Zannad, F.; Girerd, N. Prognostic value of residual pulmonary congestion at discharge assessed by lung ultrasound imaging in heart failure. Eur. J. Heart Fail. 2015, 17, 1172–1181. [Google Scholar] [CrossRef]
- Cogliati, C.; Casazza, G.; Ceriani, E.; Torzillo, D.; Furlotti, S.; Bossi, I.; Vago, T.; Costantino, G.; Montano, N. Lung ultrasound and short-term prognosis in heart failure patients. Int. J. Cardiol. 2016, 218, 104–108. [Google Scholar] [CrossRef]
- Platz, E.; Lewis, E.F.; Uno, H.; Peck, J.; Pivetta, E.; Merz, A.; Hempel, D.; Wilson, C.; Frasure, S.E.; Jhund, P.; et al. Detection and prognostic value of pulmonary congestion by lung ultrasound in ambulatory heart failure patients. Eur. Heart J. 2016, 37, 1244–1251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vitturi, N.; Dugo, M.; Soattin, M.; Simoni, F.; Maresca, L.; Zagatti, R.; Maresca, M.C. Lung ultrasound during hemodialysis: The role in the assessment of volume status. Int. Urol. Nephrol. 2013, 46, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Zoccali, C.; Torino, C.; Tripepi, R.; Tripepi, G.; D’Arrigo, G.; Postorino, M.; Gargani, L.; Sicari, R.; Picano, E.; Mallamaci, F.; et al. Pulmonary Congestion Predicts Cardiac Events and Mortality in ESRD. J. Am. Soc. Nephrol. 2013, 24, 639–646. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Volpicelli, G.; Gargani, L.; Perlini, S.; Spinelli, S.; Barbieri, G.; Lanotte, A.; Casasola, G.G.; Nogué-Bou, R.; Lamorte, A.; Agricola, E.; et al. Lung ultrasound for the early diagnosis of COVID-19 pneumonia: An international multicenter study. Intensive Care Med. 2021, 47, 444–454. [Google Scholar] [CrossRef]
- Lichtenstein, D.; Goldstein, I.; Mourgeon, E.; Cluzel, P.; Grenier, P.; Rouby, J.-J. Comparative Diagnostic Performances of Auscultation, Chest Radiography, and Lung Ultrasonography in Acute Respiratory Distress Syndrome. Anesthesiology 2004, 100, 9–15. [Google Scholar] [CrossRef]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Drazner, M.H.; Fonarow, G.C.; Geraci, S.A.; Horwich, T.; Januzzi, J.L.; et al. 2013 ACCF/AHA guideline for the management of heart failure: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2013, 62, e147–e239. [Google Scholar] [CrossRef] [Green Version]
- Flachskampf, F.A.; Biering-Sørensen, T.; Solomon, S.D.; Duvernoy, O.; Bjerner, T.; Smiseth, O.A. Cardiac Imaging to Evaluate Left Ventricular Diastolic Function. JACC Cardiovasc. Imaging 2015, 8, 1071–1093. [Google Scholar] [CrossRef] [Green Version]
- Goonewardena, S.N.; Spencer, K.T. Handcarried Echocardiography to Assess Hemodynamics in Acute Decompensated Heart Failure. Curr. Heart Fail. Rep. 2010, 7, 219–227. [Google Scholar] [CrossRef]
- Nagueh, S.F.; Kopelen, H.A.; Zoghbi, W.A. Relation of Mean Right Atrial Pressure to Echocardiographic and Doppler Parameters of Right Atrial and Right Ventricular Function. Circulation 1996, 93, 1160–1169. [Google Scholar] [CrossRef]
- Singh, S.; Koratala, A. Utility of Doppler ultrasound derived hepatic and portal venous waveforms in the management of heart failure exacerbation. Clin. Case Rep. 2020, 8, 1489–1493. [Google Scholar] [CrossRef] [PubMed]
- FDA-NIH Biomarker Working Group. BEST (Biomarkers, EndpointS, and Other Tools) Resource; FDA: Silver Spring, MD, USA, 2016. Available online: http://www.ncbi.nlm.nih.gov/books/NBK326791/ (accessed on 26 December 2021).
- Cowie, M.R.; Jourdain, P.; Maisel, A.; Dahlstrom, U.; Follath, F.; Isnard, R.; Luchner, A.; McDonagh, T.; Mair, J.; Nieminen, M.; et al. Clinical applications of B-type natriuretic peptide (BNP) testing. Eur. Heart J. 2003, 24, 1710–1718. [Google Scholar] [CrossRef]
- Cui, K.; Huang, W.; Fan, J.; Lei, H. Midregional pro-atrial natriuretic peptide is a superior biomarker to N-terminal pro-B-type natriuretic peptide in the diagnosis of heart failure patients with preserved ejection fraction. Medicine 2018, 97, e12277. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Packer, M. Should B-Type Natriuretic Peptide Be Measured Routinely to Guide the Diagnosis and Management of Chronic Heart Failure? Circulation 2003, 108, 2950–2953. [Google Scholar] [CrossRef] [Green Version]
- Law, C.; Glover, C.; Benson, K.; Guglin, M. Extremely High Brain Natriuretic Peptide Does Not Reflect the Severity of Heart Failure. Congest. Heart Fail. 2010, 16, 221–225. [Google Scholar] [CrossRef]
- Cediel, G.; Codina, P.; Spitaleri, G.; Domingo, M.; Santiago-Vacas, E.; Lupón, J.; Bayes-Genis, A. Gender-Related Differences in Heart Failure Biomarkers. Front. Cardiovasc. Med. 2021, 7, 617705. [Google Scholar] [CrossRef]
- Davidovski, F.S.; Goetze, J.P. ProANP and proBNP in plasma as biomarkers of heart failure. Biomark. Med. 2019, 13, 1129–1135. [Google Scholar] [CrossRef]
- Maisel, A.; Mueller, C.; Nowak, R.; Peacock, W.F.; Landsberg, J.W.; Ponikowski, P.; Mockel, M.; Hogan, C.; Wu, A.H.; Richards, M.; et al. Mid-region pro-hormone markers for diagnosis and prognosis in acute dyspnea: Results from the BACH (Biomarkers in Acute Heart Failure) trial. J. Am. Coll. Cardiol. 2010, 55, 2062–2076. [Google Scholar] [CrossRef] [Green Version]
- Odermatt, J.; Hersberger, L.; Bolliger, R.; Graedel, L.; Christ-Crain, M.; Briel, M.; Bucher, H.C.; Mueller, B.; Schuetz, P. The natriuretic peptide MR-proANP predicts all-cause mortality and adverse outcome in community patients: A 10-year follow-up study. Clin. Chem. Lab. Med. 2017, 55, 1407–1416. [Google Scholar] [CrossRef] [Green Version]
- Pacho, C.; Domingo, M.; Núñez, R.; Lupón, J.; Moliner, P.; de Antonio, M.; González, B.; Santesmases, J.; Vela, E.; Tor, J.; et al. Early Postdischarge STOP-HF-Clinic Reduces 30-day Readmissions in Old and Frail Patients with Heart Failure. Rev. Española Cardiol. 2017, 70, 631–638. [Google Scholar] [CrossRef]
- Gheorghiade, M.; Follath, F.; Ponikowski, P.; Barsuk, J.H.; Blair, J.E.; Cleland, J.G.; Dickstein, K.; Drazner, M.H.; Fonarow, G.C.; Jaarsma, T.; et al. Assessing and grading congestion in acute heart failure: A scientific statement from the acute heart failure committee of the heart failure association of the European Society of Cardiology and endorsed by the European Society of Intensive Care Medicine. Eur. J. Heart Fail. 2010, 12, 423–433. [Google Scholar] [CrossRef] [PubMed]
- Cohen-Solal, A.; Logeart, D.; Huang, B.; Cai, D.; Nieminen, M.S.; Mebazaa, A. Lowered B-Type Natriuretic Peptide in Response to Levosimendan or Dobutamine Treatment Is Associated with Improved Survival in Patients with Severe Acutely Decompensated Heart Failure. J. Am. Coll. Cardiol. 2009, 53, 2343–2348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishii, M.; Inomata, T.; Takehana, H.; Naruke, T.; Yanagisawa, T.; Moriguchi, M.; Takeda, S.; Izumi, T. Prognostic Utility of B-Type Natriuretic Peptide Assessment in Stable Low-Risk Outpatients with Nonischemic Cardiomyopathy After Decompensated Heart Failure. J. Am. Coll. Cardiol. 2008, 51, 2329–2335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solomon, S.D.; Rizkala, A.R.; Gong, J.; Wang, W.; Anand, I.; Ge, J.; Lam, C.S.; Maggioni, A.P.; Martinez, F.; Packer, M.; et al. Angi-otensin Receptor Neprilysin Inhibition in Heart Failure with Preserved Ejection Fraction: Rationale and Design of the PARAGON-HF Trial. JACC Heart Fail. 2017, 5, 471–482. [Google Scholar] [CrossRef]
- Morello, A.; Lloyd-Jones, D.M.; Chae, C.U.; van Kimmenade, R.R.; Chen, A.C.; Baggish, A.L.; O’Donoghue, M.; Lee-Lewandrowski, E.; Januzzi, J.L., Jr. Association of atrial fibrillation and amino-terminal pro–brain natriuretic peptide concentrations in dyspneic subjects with and without acute heart failure: Results from the ProBNP Investigation of Dyspnea in the Emergency Department (PRIDE) study. Am. Heart J. 2007, 153, 90–97. [Google Scholar] [CrossRef]
- Pieske, B.; Butler, J.; Filippatos, G.; Lam, C.; Maggioni, A.P.; Ponikowski, P.; Shah, S.; Solomon, S.; Kraigher-Krainer, E.; Samano, E.T.; et al. Rationale and design of the SOluble guanylate Cyclase stimulatoR in heArT failurE Studies (SOCRATES). Eur. J. Heart Fail. 2014, 16, 1026–1038. [Google Scholar] [CrossRef]
- Reddy, Y.N.V.; Carter, R.E.; Obokata, M.; Redfield, M.M.; Borlaug, B.A. A Simple, Evidence-Based Approach to Help Guide Diagnosis of Heart Failure with Preserved Ejection Fraction. Circulation 2018, 138, 861–870. [Google Scholar] [CrossRef]
- Thygesen, K.; Mair, J.; Mueller, C.; Huber, K.; Weber, M.; Plebani, M.; Hasin, Y.; Biasucci, L.M.; Giannitsis, E.; Lindahl, B.; et al. Recommendations for the use of natriuretic peptides in acute cardiac care: A position statement from the Study Group on Biomarkers in Cardiology of the ESC Working Group on Acute Cardiac Care. Eur. Heart J. 2012, 33, 2001–2006. [Google Scholar] [CrossRef] [Green Version]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D.; Executive Group on behalf of the Joint European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF) Task Force for the Universal Definition of Myocardial Infarction. Fourth Universal Definition of Myocardial Infarction (2018). J. Am. Coll. Cardiol. 2018, 72, 2231–2264. [Google Scholar] [CrossRef]
- Wettersten, N.; Maisel, A. Role of Cardiac Troponin Levels in Acute Heart Failure. Card. Fail. Rev. 2015, 1, 102–106. [Google Scholar] [CrossRef] [PubMed]
- Negi, S.; Sawano, M.; Kohsaka, S.; Inohara, T.; Shiraishi, Y.; Kohno, T.; Maekawa, Y.; Sano, M.; Yoshikawa, T.; Fukuda, K. Prognostic Implication of Physical Signs of Congestion in Acute Heart Failure Patients and Its Association with Steady-State Biomarker Levels. PLoS ONE 2014, 9, e96325. [Google Scholar] [CrossRef] [PubMed]
- Wettersten, N. Biomarkers in Acute Heart Failure: Diagnosis, Prognosis, and Treatment. Int. J. Heart Fail. 2021, 3, 81–105. [Google Scholar] [CrossRef]
- You, J.J.; Austin, P.; Alter, D.A.; Ko, D.; Tu, J.V. Relation between cardiac troponin I and mortality in acute decompensated heart failure. Am. Heart J. 2007, 153, 462–470. [Google Scholar] [CrossRef] [PubMed]
- Grodin, J.L.; Butler, J.; Metra, M.; Felker, G.M.; Voors, A.A.; Mcmurray, J.J.; Armstrong, P.W.; Hernandez, A.F.; O’Connor, C.; Starling, R.C.; et al. Circulating Cardiac Troponin I Levels Measured by a Novel Highly Sensitive Assay in Acute Decompensated Heart Failure: Insights from the ASCEND-HF Trial. J. Card. Fail. 2018, 24, 512–519. [Google Scholar] [CrossRef] [Green Version]
- Felker, G.M.; Mentz, R.J.; Teerlink, J.R.; Voors, A.A.; Pang, P.; Ponikowski, P.; Greenberg, B.H.; Filippatos, G.; Davison, B.A.; Cotter, G.; et al. Serial high sensitivity cardiac troponin T measurement in acute heart failure: Insights from the RELAX-AHF study. Eur. J. Heart Fail. 2015, 17, 1262–1270. [Google Scholar] [CrossRef]
- Horwich, T.B.; Patel, J.; MacLellan, W.R.; Fonarow, G.C. Cardiac Troponin I Is Associated with Impaired Hemodynamics, Progressive Left Ventricular Dysfunction, and Increased Mortality Rates in Advanced Heart Failure. Circulation 2003, 108, 833–838. [Google Scholar] [CrossRef] [Green Version]
- Packer, M.; McMurray, J.J.; Desai, A.S.; Gong, J.; Lefkowitz, M.P.; Rizkala, A.R.; Rouleau, J.L.; Shi, V.C.; Solomon, S.D.; Swedberg, K.; et al. Angiotensin Receptor Neprilysin Inhibition Compared with Enalapril on the Risk of Clinical Progression in Surviving Patients with Heart Failure. Circulation 2015, 131, 54–61. [Google Scholar] [CrossRef] [Green Version]
- Moura, B.; Aimo, A.; Al-Mohammad, A.; Flammer, A.; Barberis, V.; Bayes-Genis, A.; Rocca, H.B.; Fontes-Carvalho, R.; Grapsa, J.; Huelsmann, M.; et al. Integration of imaging and circulating biomarkers in heart failure: A consensus document by the Biomarkers and Imaging Study Groups of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2021, 23, 1577–1596. [Google Scholar] [CrossRef]
- Braunwald, E. Biomarkers in heart failure. N. Engl. J. Med. 2008, 358, 2148–2159. [Google Scholar] [CrossRef] [Green Version]
- Pascual-Figal, D.A.; Januzzi, J.L. The Biology of ST2: The International ST2 Consensus Panel. Am. J. Cardiol. 2015, 115 (Suppl. S7), 3B–7B. [Google Scholar] [CrossRef] [PubMed]
- Figal, D.A.P.; Pérez-Martínez, M.T.; Asensio-Lopez, M.C.; Sanchez-Más, J.; García-García, M.E.; Martinez, C.M.; Lencina, M.; Jara, R.; Januzzi, J.L.; Lax, A.M. Pulmonary Production of Soluble ST2 in Heart Failure. Circ. Heart Fail. 2018, 11, e005488. [Google Scholar] [CrossRef] [PubMed]
- Aimo, A.; Januzzi, J.L.; Bayes-Genis, A.; Vergaro, G.; Sciarrone, P.; Passino, C.; Emdin, M. Clinical and Prognostic Significance of sST2 in Heart Failure: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2019, 74, 2193–2203. [Google Scholar] [CrossRef]
- Kuroiwa, K.; Arai, T.; Okazaki, H.; Minota, S.; Tominaga, S.-I. Identification of Human ST2 Protein in the Sera of Patients with Autoimmune Diseases. Biochem. Biophys. Res. Commun. 2001, 284, 1104–1108. [Google Scholar] [CrossRef]
- Brunner, M.; Krenn, C.; Roth, G.; Moser, B.; Dworschak, M.; Jensen-Jarolim, E.; Spittler, A.; Sautner, T.; Bonaros, N.; Wolner, E.; et al. Increased levels of soluble ST2 protein and IgG1 production in patients with sepsis and trauma. Intensive Care Med. 2004, 30, 1468–1473. [Google Scholar] [CrossRef]
- Aurora, L.; Peterson, E.; Gui, H.; Zeld, N.; McCord, J.; Pinto, Y.; Cook, B.; Sabbah, H.N.; Williams, L.K.; Snider, J.; et al. Suppression tumorigenicity 2 (ST2) turbidimetric immunoassay compared to enzyme-linked immunosorbent assay in predicting survival in heart failure patients with reduced ejection fraction. Clin. Chim. Acta 2020, 510, 767–771. [Google Scholar] [CrossRef]
- Núñez, J.; Miñana, G.; Núñez, E.; Chorro, F.J.; Bodí, V.; Sanchis, J. Clinical utility of antigen carbohydrate 125 in heart failure. Heart Fail. Rev. 2014, 19, 575–584. [Google Scholar] [CrossRef]
- Kubena, P.; Arrigo, M.; Parenica, J.; Gayat, E.; Sadoune, M.; Ganovska, E.; Pavlusova, M.; Littnerova, S.; Spinar, J.; Mebazaa, A.; et al. Plasma Levels of Soluble CD146 Reflect the Severity of Pulmonary Congestion Better Than Brain Natriuretic Peptide in Acute Coronary Syndrome. Ann. Lab. Med. 2016, 36, 300–330. [Google Scholar] [CrossRef] [Green Version]
- Gayat, E.; Caillard, A.; Laribi, S.; Mueller, C.; Sadoune, M.; Seronde, M.-F.; Maisel, A.; Bartunek, J.; Vanderheyden, M.; Desutter, J.; et al. Soluble CD146, a new endothelial biomarker of acutely decompensated heart failure. Int. J. Cardiol. 2015, 199, 241–247. [Google Scholar] [CrossRef]
- Peacock, W.F. Novel biomarkers in acute heart failure: MR-pro-adrenomedullin. Clin. Chem. Lab. Med. 2014, 52, 1433–1435. [Google Scholar] [CrossRef]
- Willenbrock, R.; Langenickel, T.; Knecht, M.; Pagel, I.; Höhnel, K.; Philipp, S.; Dietz, R. Regulation of cardiac adrenomedullin-mRNA in different stages of experimental heart failure. Life Sci. 1999, 65, 2241–2249. [Google Scholar] [CrossRef]
- Laribi, S.; Mebazaa, A. Cardiohepatic Syndrome: Liver Injury in Decompensated Heart Failure. Curr. Heart Fail. Rep. 2014, 11, 236–240. [Google Scholar] [CrossRef] [PubMed]
- Brisco, M.A.; Coca, S.G.; Chen, J.; Owens, A.T.; McCauley, B.D.; Kimmel, S.E.; Testani, J.M. Blood Urea Nitrogen/Creatinine Ratio Identifies a High-Risk but Potentially Reversible Form of Renal Dysfunction in Patients with Decompensated Heart Failure. Circ. Heart Fail. 2013, 6, 233–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rangaswami, J.; Bhalla, V.; Blair, J.E.; Chang, T.I.; Costa, S.; Lentine, K.L.; Lerma, E.V.; Mezue, K.; Molitch, M.; Mullens, W.; et al. Cardiorenal Syndrome: Classification, Pathophysiology, Diagnosis, and Treatment Strategies: A Scientific Statement from the American Heart Association. Circulation 2019, 139, e840–e878. [Google Scholar] [CrossRef] [PubMed]
- Hanberg, J.S.; Tang, W.W.; Wilson, F.P.; Coca, S.G.; Ahmad, T.; Brisco, M.A.; Testani, J.M. An exploratory analysis of the competing effects of aggressive decongestion and high-dose loop diuretic therapy in the DOSE trial. Int. J. Cardiol. 2017, 241, 277–282. [Google Scholar] [CrossRef]
- Damman, K.; Solomon, S.D.; Pfeffer, M.A.; Swedberg, K.; Yusuf, S.; Young, J.B.; Rouleau, J.L.; Granger, C.B.; Mcmurray, J. Worsening renal function and outcome in heart failure patients with reduced and preserved ejection fraction and the impact of angiotensin receptor blocker treatment: Data from the CHARM-study programme. Eur. J. Heart Fail. 2016, 18, 1508–1517. [Google Scholar] [CrossRef] [Green Version]
- Shinagawa, H.; Inomata, T.; Koitabashi, T.; Nakano, H.; Takeuchi, I.; Naruke, T.; Ohsaka, T.; Nishii, M.; Takehana, H.; Izumi, T. Prognostic Significance of Increased Serum Bilirubin Levels Coincident with Cardiac Decompensation in Chronic Heart Failure. Circ. J. 2008, 72, 364–369. [Google Scholar] [CrossRef] [Green Version]
- Samsky, M.D.; Patel, C.B.; DeWald, T.A.; Smith, A.D.; Felker, G.M.; Rogers, J.G.; Hernandez, A.F. Cardiohepatic Interactions in Heart Failure: An overview and clinical implications. J. Am. Coll. Cardiol. 2013, 61, 2397–2405. [Google Scholar] [CrossRef] [Green Version]
- Van Deursen, V.M.; Damman, K.; Hillege, H.L.; van Beek, A.P.; Van Veldhuisen, D.J.; Voors, A.A. Abnormal Liver Function in Relation to Hemodynamic Profile in Heart Failure Patients. J. Card. Fail. 2010, 16, 84–90. [Google Scholar] [CrossRef]
- Nikolaou, M.; Parissis, J.; Yilmaz, M.B.; Seronde, M.-F.; Kivikko, M.; Laribi, S.; Paugam-Burtz, C.; Cai, D.; Pohjanjousi, P.; Laterre, P.-F.; et al. Liver function abnormalities, clinical profile, and outcome in acute decompensated heart failure. Eur. Heart J. 2013, 34, 742–749. [Google Scholar] [CrossRef]
- Duarte, K.; Monnez, J.-M.; Albuisson, E.; Pitt, B.; Zannad, F.; Rossignol, P. Prognostic Value of Estimated Plasma Volume in Heart Failure. JACC Heart Fail. 2015, 3, 886–893. [Google Scholar] [CrossRef] [PubMed]
- Mentz, R.J.; Kjeldsen, K.; Rossi, G.P.; Voors, A.A.; Cleland, J.G.; Anker, S.D.; Gheorghiade, M.; Fiuzat, M.; Rossignol, P.; Zannad, F.; et al. Decongestion in acute heart failure. Eur. J. Heart Fail. 2014, 16, 471–482. [Google Scholar] [CrossRef] [PubMed]
- Tripoliti, E.E.; Ioannidou, P.; Toumpaniaris, P.; Rammos, A.; Pacitto, D.; Lourme, J.-C.; Goletsis, Y.; Naka, K.K.; Errachid, A.; Fotiadis, D.I.I. Point-of-Care Testing Devices for Heart Failure Analyzing Blood and Saliva Samples. IEEE Rev. Biomed. Eng. 2020, 13, 17–31. [Google Scholar] [CrossRef] [PubMed]
- King, K.R.; Grazette, L.P.; Paltoo, D.N.; McDevitt, J.T.; Sia, S.K.; Barrett, P.M.; Apple, F.S.; Gurbel, P.A.; Weissleder, R.; Leeds, H.; et al. Point-of-Care Technologies for Precision Cardiovascular Care and Clinical Research: National Heart, Lung, and Blood Institute Working Group. JACC Basic Transl. Sci. 2016, 1, 73–86. [Google Scholar] [CrossRef] [Green Version]
- Alan, H.B.W. Recent Advances in Point-of-Care Diagnostics for Cardiac Markers. EJIFCC 2014, 25, 170–177. [Google Scholar]
- Cullen, L.; Collinson, P.O.; Giannitsis, E. Point-of-care testing with high-sensitivity cardiac troponin assays: The challenges and opportunities. Emerg. Med. J. 2022; Epub ahead of print. [Google Scholar] [CrossRef]
- Mueller, C.; Laule-Kilian, K.; Schindler, C.; Klima, T.; Frana, B.; Rodriguez, D.; Scholer, A.; Christ, M.; Perruchoud, A.P. Cost-effectiveness of B-Type Natriuretic Peptide Testing in Patients with Acute Dyspnea. Arch. Intern. Med. 2006, 166, 1081–1087. [Google Scholar] [CrossRef] [Green Version]
- Rehman, S.A.; Khurshid, Z.; Niazi, F.H.; Naseem, M.; Al Waddani, H.; Sahibzada, H.A.; Khan, R.S. Role of Salivary Biomarkers in Detection of Cardiovascular Diseases (CVD). Proteomes 2017, 5, 21. [Google Scholar] [CrossRef]
- Quinn, A.D.; Dixon, D.; Meenan, B.J. Barriers to hospital-based clinical adoption of point-of-care testing (POCT): A systematic narrative review. Crit. Rev. Clin. Lab. Sci. 2016, 53, 1–12. [Google Scholar] [CrossRef]
- Wiencek, J.; Nichols, J. Issues in the practical implementation of POCT: Overcoming challenges. Expert Rev. Mol. Diagn. 2016, 16, 415–422. [Google Scholar] [CrossRef]
- Züsli, S.; Bierreth, F.; Boesing, M.; Haas, P.; Abig, K.; Maier, S.; Corridori, G.; Leuppi, J.D.; Dieterle, T. Point of care with serial NT-proBNP measurement in patients with acute decompensated heart failure as a therapy-monitoring during hospitalization (POC–HF): Study protocol of a prospective, unblinded, randomized, controlled pilot trial. Contemp. Clin. Trials Commun. 2021, 23, 100825. [Google Scholar] [CrossRef] [PubMed]
- Sergi, C.M. Point of care with serial N-terminal pro-B-type natriuretic peptide (NT-proBNP) for heart failure in patients with acute decompensation. An invited commentary. Contemp. Clin. Trials Commun. 2022, 26, 100889. [Google Scholar] [CrossRef]

| Clinical Scores/US Parameter | Interpretation | Comments | |
|---|---|---|---|
| Clinical examination (Symptoms and signs) | EVEREST * Composite Congestion Score [78] (CCS) | Discharge from HF hospitalization: target CCS ≤ 2 | CCS ≥ 3: 10% increase in all-cause death at 6 months |
| Lucas Score # [87] | Severity of congestion at 4–6 weeks after discharge from HF hospitalization | The 2 years mortality: score 0: 13% score 1–2: 33% score 3–5: 59% | |
| Ultrasound | |||
| Lung US | Presence of B-lines (on 8 chest zones) | ≥3 B-lines in ≥2 zones/hemithorax identifies acute HF patients (high sensitivity and specificity) [63] Target at discharge <30 B lines [80] | ≤15 B lines at discharge: low risk of rehospitalization for HF [50] |
| Cardiovascular US | |||
| Cardiac | Left atrium Other morphological data | LAVI > 34 mL/m2 | Reflects long term increase in filling pressures [14,15] In AF or significant MV disease the LA is dilated despite normal LV diastolic function [16] |
| Doppler measurements (Algorithm based on the level of EF) | Restrictive mitral filling pattern with the E-wave deceleration time <140 ms | Consistent with increased LV filling pressures in patients with reduced EF [88] | |
| E/e’ > 15 (and septal e’ < 7 cm/s) | Moderate correlation with invasively measured LV filling pressures in patients with dilated ventricles and reduced EF [24] | ||
| TR jet peak velocity > 2.8 m/s with sPAP > 35 mm Hg | Strongly indicative of elevated filling pressures in the absence of pulmonary disease [22] | ||
| Vascular | Inferior vena cava dimension and collapsibility | Max Diam >2.1 cm with Collapsibility index <50% = sustained elevation of RAP | Target at discharge: Max Diam <2.1 cm with Collapsibility index <50% [89] |
| Doppler hepatic venous flow pattern | S < D and increased atrial flow reversal = increased RAP [90] | Reversal with effective decongestive therapy [91] | |
| Doppler intrarenal venous flow pattern | Discontinuous (pulsatile, biphasic or monophasic) = high RAP [39] | Early index of systemic congestion [42] | |
| Ratio of internal JVDiam during Valsalva manoeuvre | JVDiam ratio <4 in congestion [44] | JVDiam ratio <2 in severe congestion [44] | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ilieșiu, A.M.; Hodorogea, A.S.; Balahura, A.-M.; Bădilă, E. Non-Invasive Assessment of Congestion by Cardiovascular and Pulmonary Ultrasound and Biomarkers in Heart Failure. Diagnostics 2022, 12, 962. https://doi.org/10.3390/diagnostics12040962
Ilieșiu AM, Hodorogea AS, Balahura A-M, Bădilă E. Non-Invasive Assessment of Congestion by Cardiovascular and Pulmonary Ultrasound and Biomarkers in Heart Failure. Diagnostics. 2022; 12(4):962. https://doi.org/10.3390/diagnostics12040962
Chicago/Turabian StyleIlieșiu, Adriana Mihaela, Andreea Simona Hodorogea, Ana-Maria Balahura, and Elisabeta Bădilă. 2022. "Non-Invasive Assessment of Congestion by Cardiovascular and Pulmonary Ultrasound and Biomarkers in Heart Failure" Diagnostics 12, no. 4: 962. https://doi.org/10.3390/diagnostics12040962
APA StyleIlieșiu, A. M., Hodorogea, A. S., Balahura, A. -M., & Bădilă, E. (2022). Non-Invasive Assessment of Congestion by Cardiovascular and Pulmonary Ultrasound and Biomarkers in Heart Failure. Diagnostics, 12(4), 962. https://doi.org/10.3390/diagnostics12040962