
Influence of the Fluoroscopy Setting towards the Patient When Identifying the MPFL Insertion Point

 , , ,
, , ,
Abstract
:1. Introduction
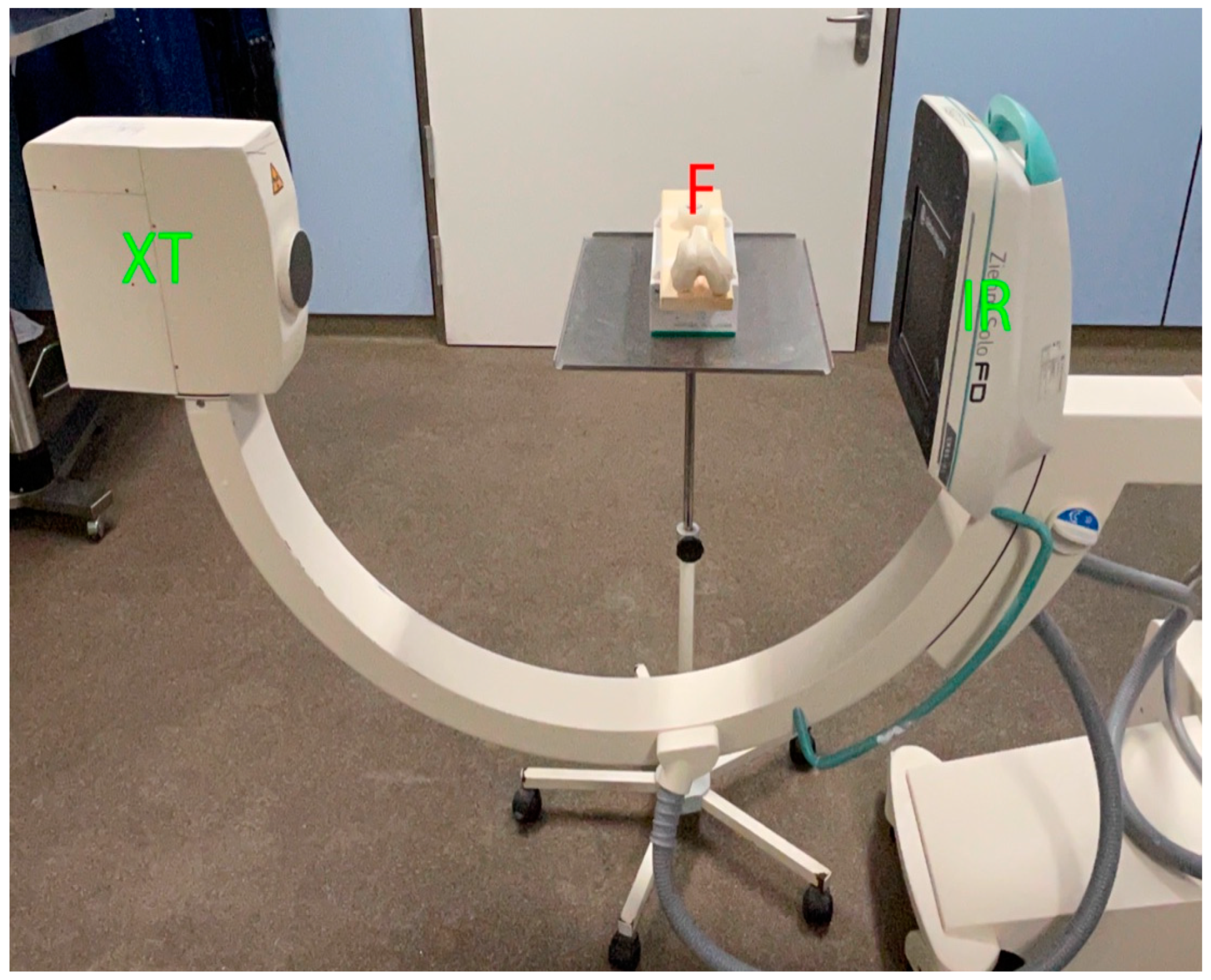
2. Materials and Methods
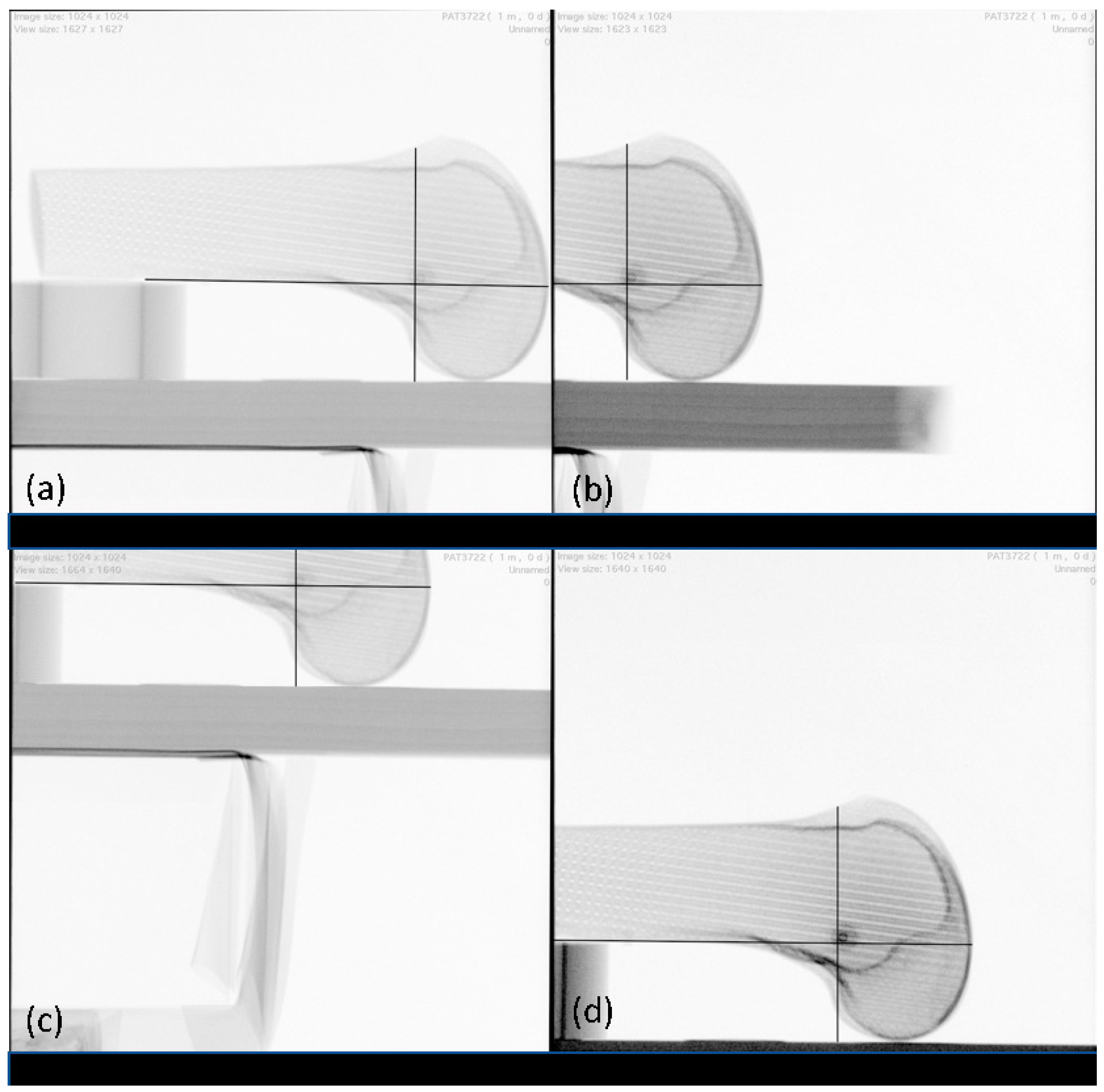
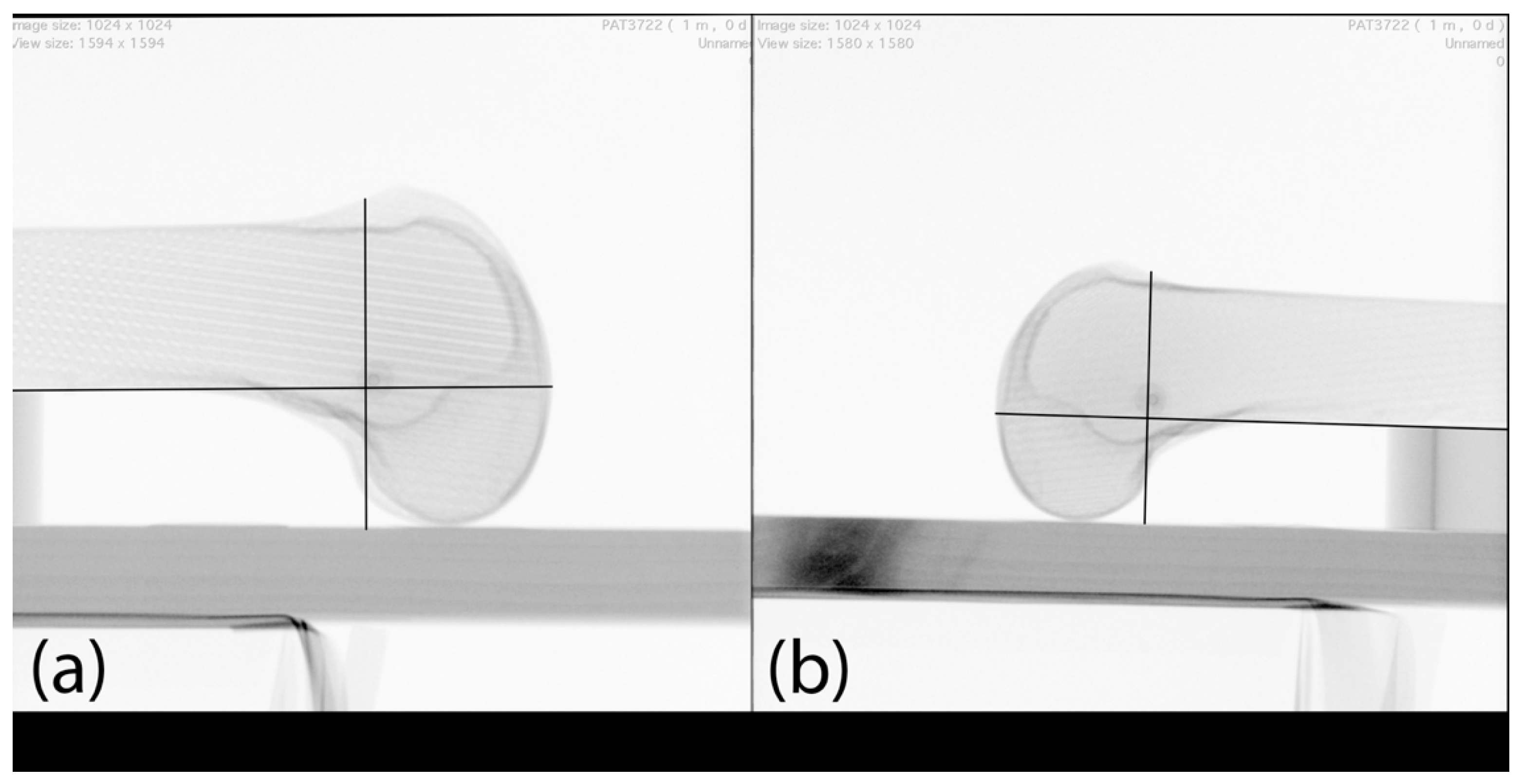
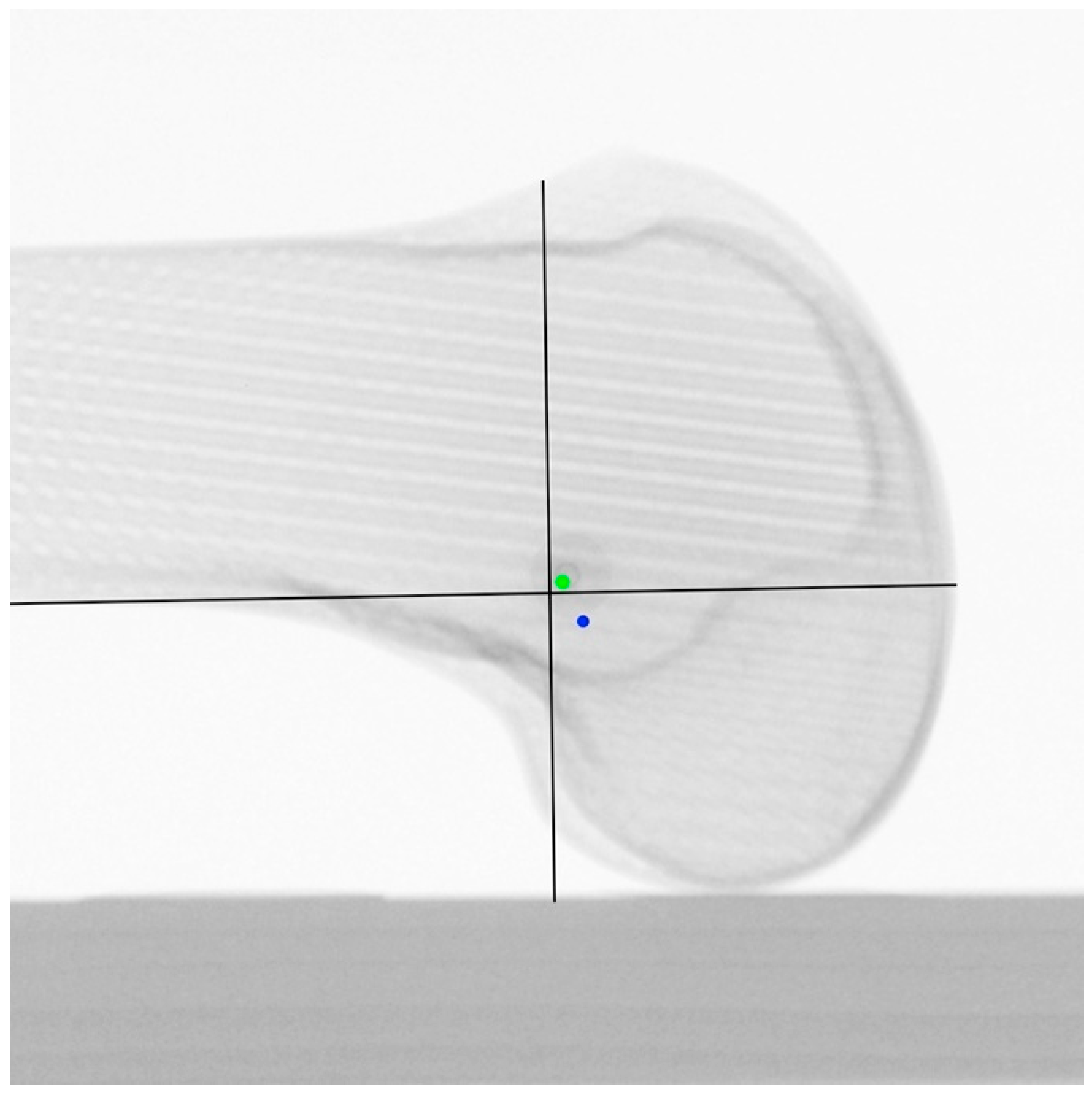
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Desio, S.M.; Burks, R.T.; Bachus, K.N. Soft Tissue Restraints to Lateral Patellar Translation in the Human Knee. Am. J. Sports Med. 1998, 26, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Frings, J.; Krause, M.; Akoto, R.; Wohlmuth, P.; Frosch, K.H. Combined Distal Femoral Osteotomy (DFO) in Genu Valgum Leads to Reliable Patellar Stabilization and an Improvement in Knee Function. Knee Surg. Sport. Traumatol. Arthrosc. 2018, 26, 3572–3581. [Google Scholar] [CrossRef] [PubMed]
- Frosch, K.H.; Schmeling, A. A New Classification System of Patellar Instability and Patellar Maltracking. Arch. Orthop. Trauma Surg. 2016, 136, 485–497. [Google Scholar] [CrossRef] [PubMed]
- Schneider, D.K.; Grawe, B.; Magnussen, R.A.; Ceasar, A.; Parikh, S.N.; Wall, E.J.; Colosimo, A.J.; Kaeding, C.C.; Myer, G.D. Outcomes after Isolated Medial Patellofemoral Ligament Reconstruction for the Treatment of Recurrent Lateral Patellar Dislocations. Am. J. Sports Med. 2016, 44, 2993–3005. [Google Scholar] [CrossRef] [Green Version]
- Shah, J.N.; Howard, J.S.; Flanigan, D.C.; Brophy, R.H.; Carey, J.L.; Lattermann, C. A Systematic Review of Complications and Failures Associated with Medial Patellofemoral Ligament Reconstruction for Recurrent Patellar Dislocation. Am. J. Sports Med. 2012, 40, 1916–1923. [Google Scholar] [CrossRef] [Green Version]
- Stephen, J.M.; Lumpaopong, P.; Deehan, D.J.; Kader, D.; Amis, A.A. The Medial Patellofemoral Ligament: Location of Femoral Attachment and Length Change Patterns Resulting from Anatomic and Nonanatomic Attachments. Am. J. Sports Med. 2012, 40, 1871–1879. [Google Scholar] [CrossRef]
- Kernkamp, W.A.; Wang, C.; Li, C.; Hu, H.; van Arkel, E.R.A.; Nelissen, R.G.H.H.; LaPrade, R.F.; van de Velde, S.K.; Tsai, T.Y. The Medial Patellofemoral Ligament Is a Dynamic and Anisometric Structure: An In Vivo Study on Length Changes and Isometry. Am. J. Sports Med. 2019, 47, 1645–1653. [Google Scholar] [CrossRef]
- Stephen, J.M.; Kaider, D.; Lumpaopong, P.; Deehan, D.J.; Amis, A.A. The Effect of Femoral Tunnel Position and Graft Tension on Patellar Contact Mechanics and Kinematics after Medial Patellofemoral Ligament Reconstruction. Am. J. Sports Med. 2014, 42, 364–372. [Google Scholar] [CrossRef]
- Hopper, G.P.; Leach, W.J.; Rooney, B.P.; Walker, C.R.; Blyth, M.J. Does Degree of Trochlear Dysplasia and Position of Femoral Tunnel Influence Outcome after Medial Patellofemoral Ligament Reconstruction? Am. J. Sports Med. 2014, 42, 716–722. [Google Scholar] [CrossRef]
- Servien, E.; Fritsch, B.; Lustig, S.; Demey, G.; Debarge, R.; Lapra, C.; Neyret, P. In Vivo Positioning Analysis of Medial Patellofemoral Ligament Reconstruction. Am. J. Sports Med. 2011, 39, 134–139. [Google Scholar] [CrossRef]
- Herschel, R.; Hasler, A.; Tscholl, P.M.; Fucentese, S.F. Visual-Palpatory versus Fluoroscopic Intraoperative Determination of the Femoral Entry Point in Medial Patellofemoral Ligament Reconstruction. Knee Surg. Sport. Traumatol. Arthrosc. 2017, 25, 2545–2549. [Google Scholar] [CrossRef] [PubMed]
- Jaecker, V.; Brozat, B.; Banerjee, M.; Otchwemah, R.; Bouillon, B.; Shafizadeh, S. Fluoroscopic Control Allows for Precise Tunnel Positioning in MPFL Reconstruction. Knee Surg. Sport. Traumatol. Arthrosc. 2017, 25, 2688–2694. [Google Scholar] [CrossRef] [PubMed]
- Koenen, P.; Shafizadeh, S.; Pfeiffer, T.R.; Wafaisade, A.; Bouillon, B.; Kanakamedala, A.C.; Jaecker, V. Intraoperative Fluoroscopy during MPFL Reconstruction Improves the Accuracy of the Femoral Tunnel Position. Knee Surg. Sport. Traumatol. Arthrosc. 2018, 26, 3547–3552. [Google Scholar] [CrossRef] [PubMed]
- DeLee, J.C.; Riley, M.B.; Rockwood, C.A. Acute Posterolateral Rotatory Instability of the Knee. Am. J. Sports Med. 1983, 11, 199–207. [Google Scholar] [CrossRef] [PubMed]
- de Abreu-e-Silva, G.M.; Buarque, F.A.R.; Dias, T.S.; Lei, P.; Bueno, E.L.R.; de Andrade, M.A.P. Anatomical Femoral Tunnel Positioning in the Medial Patellofemoral Ligament Reconstruction: Is the Free-Hand Technique Accurate? Ann. Transl. Med. 2020, 8, 924. [Google Scholar] [CrossRef]
- Balcarek, P.; Walde, T.A. Accuracy of Femoral Tunnel Placement in Medial Patellofemoral Ligament Reconstruction: The Effect of a Nearly True-Lateral Fluoroscopic View. Am. J. Sports Med. 2015, 43, 2228–2232. [Google Scholar] [CrossRef]
- Barnett, A.J.; Howells, N.R.; Burston, B.J.; Ansari, A.; Clark, D.; Eldridge, J.D. Radiographic Landmarks for Tunnel Placement in Reconstruction of the Medial Patellofemoral Ligament. Knee Surg. Sport. Traumatol. Arthrosc. 2012, 20, 2380–2384. [Google Scholar] [CrossRef]
- McCarthy, M.; Ridley, T.J.; Bollier, M.; Wolf, B.; Albright, J.; Amendola, A. Femoral Tunnel Placement in Medial Patellofemoral Ligament Reconstruction. Iowa Orthop. J. 2013, 33, 58–63. [Google Scholar] [CrossRef]
- Chatterton, A.; Nielsen, T.G.; Sørensen, O.G.; Lind, M. Clinical Outcomes after Revision Surgery for Medial Patellofemoral Ligament Reconstruction. Knee Surg. Sport. Traumatol. Arthrosc. 2018, 26, 739–745. [Google Scholar] [CrossRef]
- Walker, M.; Maini, L.; Kay, J.; Siddiqui, A.; Almasri, M.; de SA, D. Femoral Tunnel Malposition Is the Most Common Indication for Revision Medial Patellofemoral Ligament Reconstruction with Promising Early Outcomes Following Revision Reconstruction: A Systematic Review. Knee Surg. Sport. Traumatol. Arthrosc. 2022, 30, 1352–1361. [Google Scholar] [CrossRef]
- Fauber, T. Radiographic Imaging and Exposure; Elsevier Inc.: Amsterdam, The Netherlands, 2016; ISBN 978-0-323-35624-4. [Google Scholar]
- Dejour, H.; Walch, G.; Nove-Josserand, L.; Guier, C. Knee Surgery Sports Traumatology I Arthroscopy Patellar Problems Factors of Patellar Instability: An Anatomic Radiographic Study. Knee Surg. Sports Traumatol. Arthrosc. 1994, 2, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Schöttle, P.B.; Schmeling, A.; Rosenstiel, N.; Weiler, A. Radiographic Landmarks for Femoral Tunnel Placement in Medial Patellofemoral Ligament Reconstruction. Am. J. Sports Med. 2007, 35, 801–804. [Google Scholar] [CrossRef] [PubMed]
- Schöttle, P.B.; Hensler, D.; Imhoff, A.B. Anatomical Double-Bundle MPFL Reconstruction with an Aperture Fixation. Knee Surg. Sport. Traumatol. Arthrosc. 2010, 18, 147–151. [Google Scholar] [CrossRef] [PubMed]
- Schöttle, P.; Schmeling, A.; Romero, J.; Weiler, A. Anatomical Reconstruction of the Medial Patellofemoral Ligament Using a Free Gracilis Autograft. Arch. Orthop. Trauma Surg. 2009, 129, 305–309. [Google Scholar] [CrossRef] [PubMed]
- Fink, C.; Veselko, M.; Herbort, M.; Hoser, C. MPFL Reconstruction Using a Quadriceps Tendon Graft Part 2: Operative Technique and Short Term Clinical Results. Knee 2014, 21, 1175–1179. [Google Scholar] [CrossRef] [Green Version]
- Herbort, M.; Hoser, C.; Domnick, C.; Raschke, M.J.; Lenschow, S.; Weimann, A.; Kösters, C.; Fink, C. MPFL Reconstruction Using a Quadriceps Tendon Graft. Part 1: Biomechanical Properties of Quadriceps Tendon MPFL Reconstruction in Comparison to the Intact MPFL. A Human Cadaveric Study. Knee 2014, 21, 1169–1174. [Google Scholar] [CrossRef] [Green Version]
- Ellera Gomes, J.L.; Stigler Marczyk, L.R.; De César, P.C.; Jungblut, C.F. Medial Patellofemoral Ligament Reconstruction with Semitendinosus Autograft for Chronic Patellar Instability: A Follow-up Study. Arthrosc. J. Arthrosc. Relat. Surg. 2004, 20, 147–151. [Google Scholar] [CrossRef]
- Han, H.; Xia, Y.; Yun, X.; Wu, M. Anatomical Transverse Patella Double Tunnel Reconstruction of Medial Patellofemoral Ligament with a Hamstring Tendon Autograft for Recurrent Patellar Dislocation. Arch. Orthop. Trauma Surg. 2011, 131, 343–351. [Google Scholar] [CrossRef]
- Toritsuka, Y.; Amano, H.; Mae, T.; Uchida, R.; Hamada, M.; Ohzono, K.; Shino, K. Dual Tunnel Medial Patellofemoral Ligament Reconstruction for Patients with Patellar Dislocation Using a Semitendinosus Tendon Autograft. Knee 2011, 18, 214–219. [Google Scholar] [CrossRef]
- Siebold, R.; Chikale, S.; Sartory, N.; Hariri, N.; Feil, S.; Pässler, H.H. Hamstring Graft Fixation in MPFL Reconstruction at the Patella Using a Transosseous Suture Technique. Knee Surg. Sport. Traumatol. Arthrosc. 2010, 18, 1542–1544. [Google Scholar] [CrossRef]
- Deie, M.; Ochi, M.; Adachi, N.; Shibuya, H.; Nakamae, A. Medial Patellofemoral Ligament Reconstruction Fixed with a Cylindrical Bone Plug and a Grafted Semitendinosus Tendon at the Original Femoral Site for Recurrent Patellar Dislocation. Am. J. Sports Med. 2011, 39, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Christiansen, S.E.; Jacobsen, B.W.; Lund, B.; Lind, M. Reconstruction of the Medial Patellofemoral Ligament with Gracilis Tendon Autograft in Transverse Patellar Drill Holes. Arthrosc. J. Arthrosc. Relat. Surg. 2008, 24, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, C.G.; Fulkerson, J.P.; Edgar, C. Radiographic Reference Points Are Inaccurate with and Without a True Lateral Radiograph. Am. J. Sports Med. 2016, 44, 133–142. [Google Scholar] [CrossRef] [PubMed]
- Berard, J.B.; Magnussen, R.A.; Bonjean, G.; Ozcan, S.; Lustig, S.; Neyret, P.; Servien, E. Femoral Tunnel Enlargement after Medial Patellofemoral Ligament Reconstruction: Prevalence, Risk Factors, and Clinical Effect. Am. J. Sports Med. 2014, 42, 297–301. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, F.; Börtlein, J.; Milinkovic, D.D.; Balcarek, P. Patient-Reported Outcomes After Revision Surgery for Failed Medial Patellofemoral Ligament Reconstruction: A Matched-Pair Analysis Including Correction of Predisposing Factors. Am. J. Sports Med. 2020, 48, 3566–3572. [Google Scholar] [CrossRef] [PubMed]
- Elias, J.J.; Cosgarea, A.J. Technical Errors during Medial Patellofemoral Ligament Reconstruction Could Overload Medial Patellofemoral Cartilage: A Computational Analysis. Am. J. Sports Med. 2006, 34, 1478–1485. [Google Scholar] [CrossRef]
- Sanchis-Alfonso, V.; Ramirez-Fuentes, C.; Montesinos-Berry, E.; Aparisi-Rodriguez, F.; Martí-Bonmatí, L. Does Radiographic Location Ensure Precise Anatomic Location of the Femoral Fixation Site in Medial Patellofemoral Ligament Surgery? Knee Surg. Sport. Traumatol. Arthrosc. 2016, 24, 2838–2844. [Google Scholar] [CrossRef]
- Tanaka, M.J.; Chahla, J.; Farr, J.; LaPrade, R.F.; Arendt, E.A.; Sanchis-Alfonso, V.; Post, W.R.; Fulkerson, J.P. Recognition of Evolving Medial Patellofemoral Anatomy Provides Insight for Reconstruction. Knee Surg. Sport. Traumatol. Arthrosc. 2019, 27, 2537–2550. [Google Scholar] [CrossRef]
- Zhang, X.; Xie, G.; Zhang, C.; Fang, Z.; Zhao, J.; Huangfu, X. Comparation and Evaluation of the Accuracy of the Sulcus Localization Method to Establish the Medial Patellofemoral Ligament Femoral Tunnel: A Cadaveric and Clinical Study. BMC Musculoskelet. Disord. 2019, 20, 53. [Google Scholar] [CrossRef] [Green Version]
- Cheng, R.; Alexandridi, N.A.; Smith, R.M.; Shen, A.; Gandler, W.; McCreedy, E.; McAuliffe, M.J.; Sheehan, F.T. Fully Automated Patellofemoral MRI Segmentation Using Holistically Nested Networks: Implications for Evaluating Patellofemoral Osteoarthritis, Pain, Injury, Pathology, and Adolescent Development. Magn. Reson. Med. 2020, 83, 139–153. [Google Scholar] [CrossRef]
- Lester, J.D.; Hsu, S.; Ahmad, C.S. Occupational Hazards Facing Orthopedic Surgeons. Am. J. Orthop. 2012, 41, 132–139. [Google Scholar] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Position | Displacement, Mean ± SD, mm | p-Value |
|---|---|---|
| LM25 | ||
| Distal | 0.9 ± 0.6 | 0.008 |
| Proximal | 1.9 ± 1.1 | 0.005 |
| Superior | 1.6 ± 0.8 | 0.005 |
| Inferior | 1.5 ± 0.8 | 0.005 |
| ML5 | 5.3 ± 1.2 | 0.005 |
| ML5 | ||
| Distal | 1.7 ± 1.3 | 0.008 |
| Proximal | 1.6 ± 1.2 | 0.005 |
| Superior | 1.3 ± 0.6 | 0.005 |
| Inferior | 1.6 ± 1.1 | 0.005 |
| LM25 | 4.8 ± 2.2 | 0.005 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Korthaus, A.; Dust, T.; Berninger, M.; Frings, J.; Krause, M.; Frosch, K.-H.; Thürig, G. Influence of the Fluoroscopy Setting towards the Patient When Identifying the MPFL Insertion Point. Diagnostics 2022, 12, 1427. https://doi.org/10.3390/diagnostics12061427
Korthaus A, Dust T, Berninger M, Frings J, Krause M, Frosch K-H, Thürig G. Influence of the Fluoroscopy Setting towards the Patient When Identifying the MPFL Insertion Point. Diagnostics. 2022; 12(6):1427. https://doi.org/10.3390/diagnostics12061427
Chicago/Turabian StyleKorthaus, Alexander, Tobias Dust, Markus Berninger, Jannik Frings, Matthias Krause, Karl-Heinz Frosch, and Grégoire Thürig. 2022. "Influence of the Fluoroscopy Setting towards the Patient When Identifying the MPFL Insertion Point" Diagnostics 12, no. 6: 1427. https://doi.org/10.3390/diagnostics12061427
APA StyleKorthaus, A., Dust, T., Berninger, M., Frings, J., Krause, M., Frosch, K.-H., & Thürig, G. (2022). Influence of the Fluoroscopy Setting towards the Patient When Identifying the MPFL Insertion Point. Diagnostics, 12(6), 1427. https://doi.org/10.3390/diagnostics12061427