Abstract
In the transoral endoscopic thyroidectomy vestibular approach (TOETVA), three oral vestibular incisions are used to access the thyroid. This approach leaves no scar on the body surface; however, unexpected complications may occur. Three patients (two women, one man) underwent TOETVA using the standard three-port technique. Broken cannulas of the 12 mm central port were noted in all cases. All cannulas broke on the ventral side of the distal shaft. The fracture lines were 3–4 cm in length, with some fragments scattered throughout the operative field and oral cavity. The fractures were caused by compression against the mandible while tilting the cannula during surgical manipulation. Male sex, short stature, and protruding chin may be risk factors for cannula fracture in TOETVA. Measures should be taken to prevent this complication, particularly in high-risk patients.
1. Introduction
The transoral endoscopic thyroidectomy vestibular approach (TOETVA) is a novel technique with excellent cosmetic outcomes [1]. Compared with other remote-access thyroidectomies, such as those via the axilla or breast, the vestibular approach has the shortest distance to the neck and requires lesser skin-flap dissection [2,3]. Because this technique is minimal invasive, it has been quickly adopted worldwide since Dr. Anuwong published his first case series in 2016 [1,4].
Current evidence shows comparable surgical outcomes between transoral and conventional thyroidectomy [5]. However, using three incisions in the oral vestibule to access the thyroid might cause some complications that are unique to TOETVA and unseen in the conventional approach, such as mental nerve injury and mentalis muscle laceration [6,7]. Furthermore, the trocar is placed in a small confined space above the mandible, and complete breakdown of the trocar cannula into two parts with some scattered fragments has been reported [8]. The sharp edge of the broken cannula may injure the surrounding tissue. Moreover, small dislodged fragments may be dispersed widely and difficult to find. Needless to say, retained foreign objects are a serious threat to patient safety and may trigger a medical malpractice claim [9].
Herein, we present three cases of cannula fracture during TOETVA. We summarize the fracture pattern, possible mechanisms, and predisposing factors for cannula fractures. We also propose strategies for the prevention and management of cannula breakage.
2. Case Presentation
2.1. Case 1
A 57-year-old man (height, 166 cm; weight, 82 kg) presented with a 1.7 cm left thyroid nodule that was incidentally found during a health examination. Fine-needle aspiration cytology (FNAC) suggested that the nodule was a follicular neoplasm, and the patient was referred for surgical resection for a definitive diagnosis. He had no history of head and neck surgery.
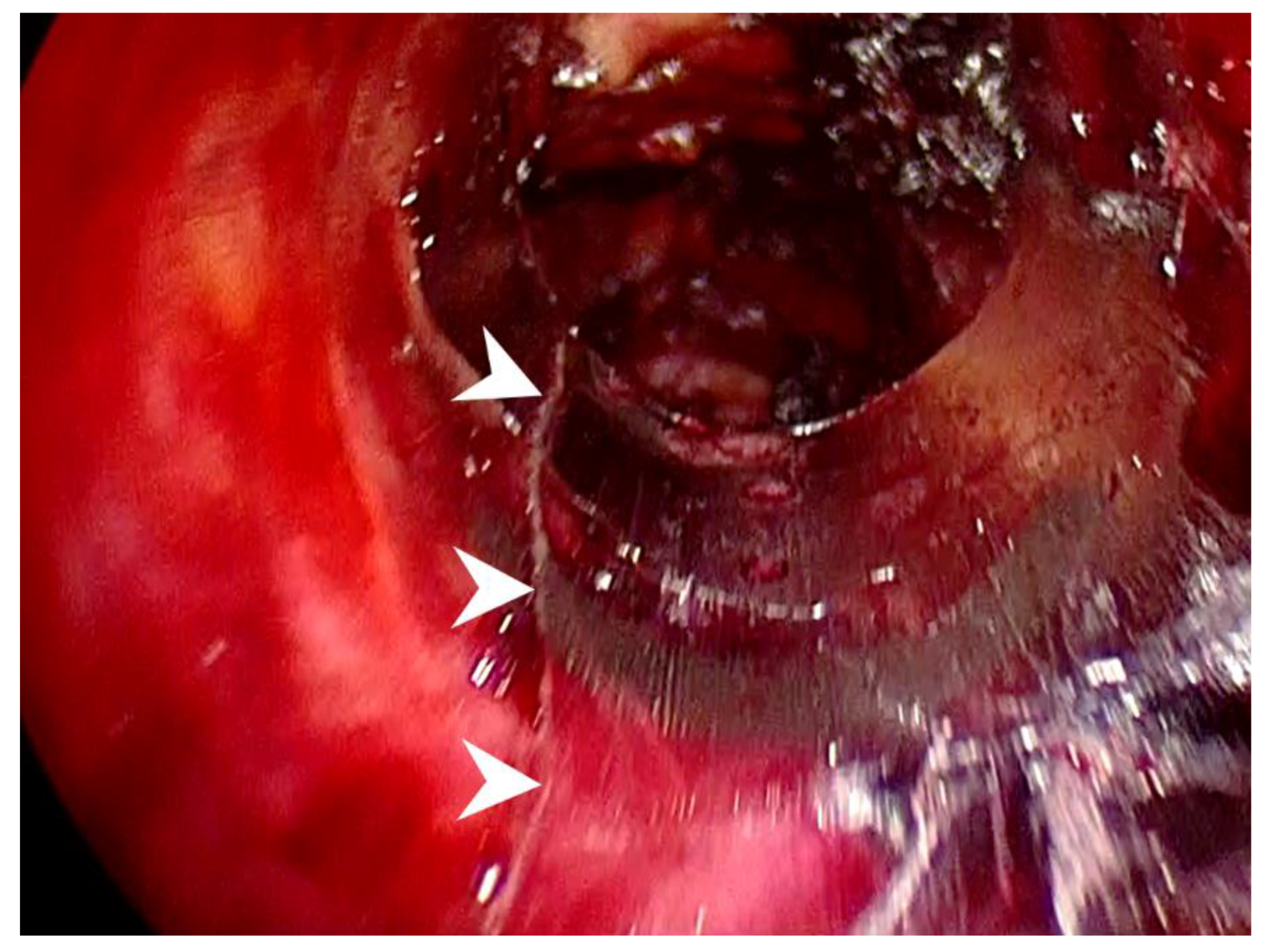
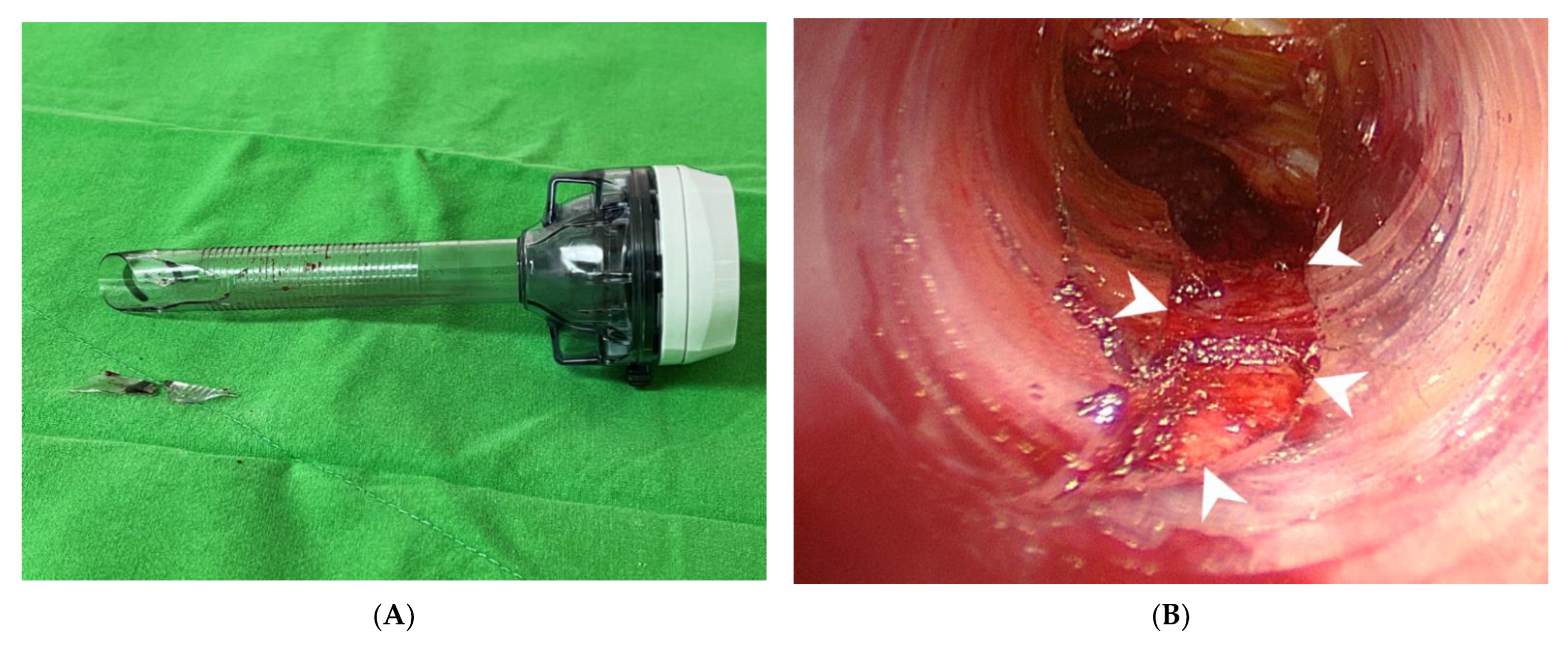
The patient underwent transoral endoscopic left thyroidectomy. The operative procedure was similar to Dr. Anuwong’s technique with some refinements, as described in our previous publication [10,11]. One 12 mm trocar (ENDOPATH XCEL Trocar, Ethicon, Cincinnati, OH, USA), and two 5 mm trocars (VersaOne Optical Trocar, Medtronic, Minneapolis, MN, USA) were placed. A 30-degree 10 mm endoscope was inserted into the central trocar for inspection. The operative procedure was uneventful. However, a linear fracture of the distal part of the central port was found at the end of the surgery (Figure 1). The fracture line was located on the ventral side of the cannula, with a slight deviation to the left. After cannula removal, no bleeding was observed at the fracture site. The patient’s postoperative course was uneventful, and the final pathologic diagnosis revealed a non-invasive follicular thyroid neoplasm with papillary-like nuclear features.
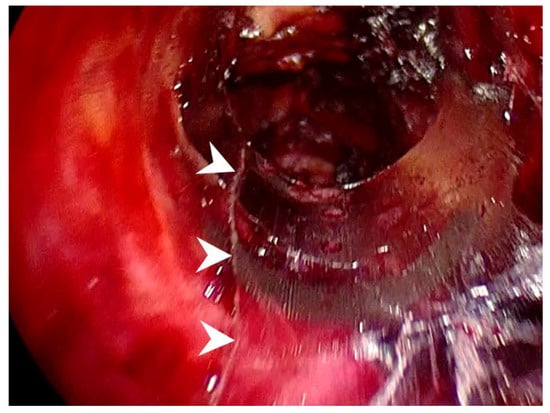
Figure 1.
Intraoperative view of Case 1 demonstrating a linear fracture on the left ventral side of the cannula (arrowheads).
2.2. Case 2
A 56-year-old woman (height, 154 cm; weight, 80 kg) was found to have a 1.9 cm left thyroid nodule during a health examination. FNAC of the lesion suggested papillary carcinoma. Preoperative computed tomography revealed no evidence of cervical lymph node metastases.
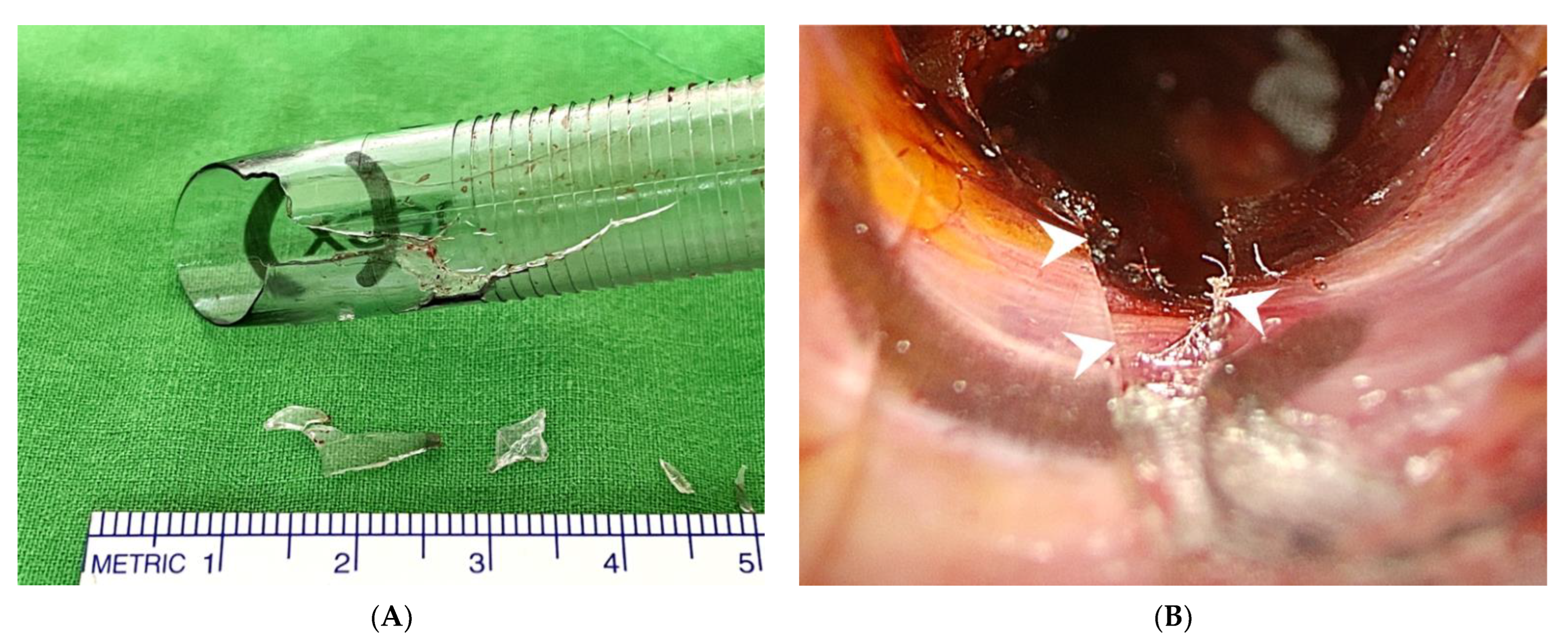
The patient underwent transoral endoscopic left thyroidectomy. After complete dissection of the thyroid gland, the central port was withdrawn to remove the surgical specimen, which was enclosed in an endo bag (Endo Pocket, UNIMAX, New Taipei, Taiwan). A broken cannula with a defect in the distal part was observed (Figure 2A). The cannula defect was on the ventral side, which was in contact with the mandible (Figure 2B). Missing fragments constituting the cannula defect were found in the operative field. Postoperatively, the patient recovered smoothly. Pathological examination revealed non-invasive follicular thyroid neoplasm with papillary-like nuclear features.
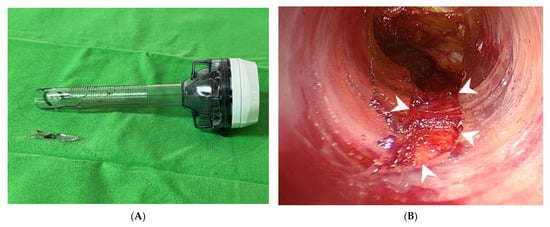
Figure 2.
The broken cannula in Case 2. (A) The fracture is in the distal end of the cannula. Two fragments were retrieved. (B) Intraoperative view shows a cannula fracture with a defect on the ventral side of the cannula (arrowheads).
2.3. Case 3
A 45-year-old woman (height, 154 cm; weight, 45 kg) presented with progressive enlargement of a right thyroid goiter up to 4.4 cm, which caused tracheal deviation and compression. The patient underwent transoral endoscopic right thyroidectomy for symptom relief. Similar to Case 2, a broken cannula with a defect at the distal end was found when we extracted the 12 mm port to gain access for specimen retrieval (Figure 3A). The fracture lines were located on the ventral side of the cannula (Figure 3B). Three of the four dislodged fragments were retrieved from the operative field using a Maryland dissector. The last missing piece was found in the oral cavity. It lay on the gauze, which was placed in the mouth to absorb excessive saliva.
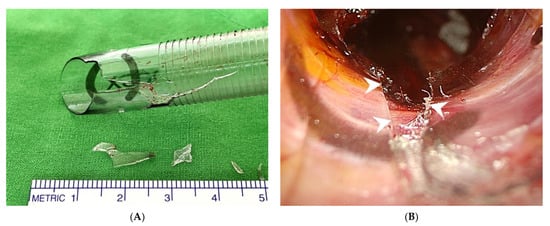
Figure 3.
The broken cannula in Case 3. (A) The fractured part is at the distal end of cannula. Four fragments were retrieved. (B) Intraoperative view shows a cannula fracture with a defect on the ventral side of the cannula (arrowheads).
Patient characteristics and patterns of cannula fracture in all three cases are summarized in Table 1 and Table 2, respectively.

Table 1.
Patient characteristics.
Table 2.
Patterns of cannula fracture.
3. Discussion
To the best of our knowledge, this is the first case series focusing on the breakage of trocar cannulas during TOETVA. In our series, all cannulas broke at the distal end with similar fracture lengths (3–4 cm), and all fractures occurred on the ventral side where the cannulas were in direct contact with the mandible. The breakages only differed in the severity, from a single linear fracture to multiple fractures with two to four displaced fragments (Table 2). Hong et al. reported complete cannula rupture into two parts, which represents the most severe damage [8]. The similar characteristics of the broken cannulas imply that all ruptures were caused by the same mechanism.
We speculate that the cannulas fractured due to compression against the mandible (Figure 4). During the operation, the observation port must be tilted down to inspect the operative field. This action applies a force against the mandible that results in an equal counterforce to the cannula. Because the cannula is confined to the small and tight premandibular space with a limited range of motion, the accumulated compression pressure leads to cannula breakage. This theory can explain why all fractures occurred on the ventral side and in the distal shaft of the cannula, which is the fulcrum of the cannula on the mandible.

Figure 4.
Proposed mechanism for cannula fracture. During the surgery, the observation port (black cylinder) is tilted down (black arrow) to inspect the operative field. This action applies a force against the mandible, which results in an equal counterforce (white arrow) to the cannula that leads to cannula breakage.
Because men tend to have prominent jaws and dense premandibular soft tissue, the cannula is encased more tightly, making it more susceptible to breakage during surgical manipulation, as in case 1 (Table 2) [12]. Patients 2 and 3 were relatively short (both women were 154 cm in height), which translated into proportionally smaller oral vestibules and chins. It is more difficult for a small chin to accommodate a standard 12 mm port; thus, a small chin may be a predisposing factor for cannula fracture. In addition, Case 3 had a protruding chin and the distance between the jaw and neck (length of jaw) was greater, even with the neck extended (Figure 4) [13]. Greater force had to be applied to tilt the central cannula, which introduced the endoscope, downwards to visualize the operative field properly. This excessive pressure increased the risk of cannula fractures. This may also explain why patients with a prominent mandibular jawline have more postoperative swelling and perceive more pain after TOETVA [13].
Table 3 summarizes the proposed strategies for preventing cannula fractures. Trocars with smaller diameters (e.g., 5 mm or 11 mm) can be used in patients with small chins to decrease passive compression caused by the surrounding tissue and mandible. Cohen et al. suggest using a 5 mm central trocar to replace the 12 mm one in pediatric patients [14]. Indeed, the premandibular space can be dilated to relieve compression, facilitate trocar movement, and remove specimens. However, routine space dilatation is not recommended because it may injure the surrounding mental nerve, which provides sensory innervation to the lower lip and chin, and/or the mentalis muscle, which elevates the lower lip and allows it to pout [7,11].
Table 3.
Strategies for preventing cannula fracture.
The movement of the endoscope should be gentle so that the cannula is not forcibly compressed against the mandible. Using a smaller 5 mm endoscope is another option to mitigate compression [15]. Further, the cannula can be retracted back to the lower edge of the chin [16]. Thus, the distal cannula would not compress against the mandible when the endoscope is tilted down to inspect the operative field. This adjustment of port position also enhances the endoscopic view of the superior thyroid pole [16]. Finally, we could replace the plastic trocar with a metal trocar, which is more fracture-resistant and reusable [8].
Using robotic systems with flexible scopes may be another solution for this problem [17]. Compared to the standard rigid endoscope, a flexible scope can navigate the entire operative field because the direction of the scope tip can be adjusted; therefore, the main scope shaft does not need to compress the mandible to gain access for better visualization [17]. For example, the da Vinci single port robotic surgery system (Intuitive Surgical, Sunnyvale, CA, USA) has been used in TOETVA procedures with some promising results [18]. Moreover, newer surgical robots are equipped with force sensor and force control algorithms to provide haptic feedback based on the stiffness of the tissue being manipulated [19]. This can prevent the application of excessive force and further improve patient safety.
Nevertheless, if the cannula breaks, a thorough inspection of the operative field should be performed to check for lacerations in the region of fracture and to collect all dislodged fragments. The oral cavity is another potential space where fragments may be deposited and should be checked. The fragments should be retrieved one by one and no missing pieces should be left in the patient’s body.
In our institute, the incidence rate of cannula fracture during TOETVA is 2.3% (3/132), which is comparable to 3.7% (3/82) reported by Hong et al. [8]. By following the prevention strategies in Table 3, the incidence rate might decline in future.
4. Conclusions
In summary, we reported three cases of broken cannulas during TOETVA. All breakages occurred on the ventral side of the distal cannula and were associated with mandibular compression. Male sex, short stature, or a protruding chin may be risk factors for cannula fracture. Using a smaller, break-resistant cannula, gentle manipulation, and pulling the cannula back to the lower edge of the chin might reduce the risk of breakage. Once a cannula breaks, thorough inspection of the operative field to retrieve all fragments is of utmost importance.
Author Contributions
Conceptualization, T.-J.L. and S.-I.L.; data curation, T.-J.L.; writing—original draft preparation, T.-J.L.; writing—review and editing, I.-S.C. and S.-I.L.; visualization, I.-S.C.; supervision, S.-I.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
All data generated or analyzed during this study are included in this published article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Anuwong, A. Transoral endoscopic thyroidectomy vestibular approach: A series of the first 60 human cases. World J. Surg. 2016, 40, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Liang, T.J.; Wang, N.Y.; Tsai, C.Y.; Liu, S.I.; Chen, I.S. Outcome comparison between endoscopic transoral and bilateral axillo-breast approach thyroidectomy performed by a single surgeon. World J. Surg. 2021, 45, 1779–1784. [Google Scholar] [CrossRef] [PubMed]
- Russell, J.O.; Razavi, C.R.; Garstka, M.E.; Chen, L.W.; Vasiliou, E.; Kang, S.W.; Tufano, R.P.; Kandil, E. Remote-access thyroidectomy: A multi-institutional North American experience with transaxillary, robotic facelift, and transoral endoscopic vestibular approaches. J. Am. Coll. Surg. 2019, 228, 516–522. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Park, D.; Sun, H.; Anuwong, A.; Tufano, R.; Kim, H.Y.; Dionigi, G. Indications, benefits and risks of transoral thyroidectomy. Best Pract. Res. Clin. Endocrinol. Metab. 2019, 33, 101280. [Google Scholar] [CrossRef] [PubMed]
- Anuwong, A.; Ketwong, K.; Jitpratoom, P.; Sasanakietkul, T.; Duh, Q.Y. Safety and outcomes of the transoral endoscopic thyroidectomy vestibular approach. JAMA Surg. 2018, 153, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Tae, K. Complications of transoral thyroidectomy: Overview and update. Clin. Exp. Otorhinolaryngol. 2021, 14, 169–178. [Google Scholar] [CrossRef] [PubMed]
- Zheng, G.; Wang, X.; Wu, G.; Sun, H.; Ma, C.; Zheng, H.; Song, X. The sensorimotor changes of the lower lip and chin after transoral endoscopic thyroidectomy vestibular approach. Updates Surg. 2021, 73, 2283–2291. [Google Scholar] [CrossRef] [PubMed]
- Hong, Y.T.; Ahn, J.H.; Kim, J.H.; Yi, J.W.; Hong, K.H. Bi-institutional experience of transoral endoscopic thyroidectomy: Challenges and outcomes. Head Neck 2020, 42, 2115–2122. [Google Scholar] [CrossRef] [PubMed]
- Stawicki, S.P.; Evans, D.C.; Cipolla, J.; Seamon, M.J.; Lukaszczyk, J.J.; Prosciak, M.P.; Torigian, D.A.; Doraiswamy, V.A.; Yazzie, N.P.; Gunter, O.L., Jr.; et al. Retained surgical foreign bodies: A comprehensive review of risks and preventive strategies. Scand. J. Surg. 2009, 98, 8–17. [Google Scholar] [CrossRef] [PubMed]
- Anuwong, A.; Sasanakietkul, T.; Jitpratoom, P.; Ketwong, K.; Kim, H.Y.; Dionigi, G.; Richmon, J.D. Transoral endoscopic thyroidectomy vestibular approach (TOETVA): Indications, techniques and results. Surg. Endosc. 2018, 32, 456–465. [Google Scholar] [CrossRef] [PubMed]
- Liang, T.J.; Chen, I.S.; Liu, S.I. Working space creation in transoral thyroidectomy: Pearls and pitfalls. Cancers 2022, 14, 1031. [Google Scholar] [CrossRef] [PubMed]
- Fama, F.; Zhang, D.; Pontin, A.; Makay, Ö.; Tufano, R.P.; Kim, H.Y.; Sun, H.; Dionigi, G. Patient and surgeon candidacy for transoral endoscopic thyroid surgery. Turk. Arch. Otorhinolaryngol. 2019, 57, 105–108. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Jiang, Y.; Li, Y.; He, Q.; Pan, L.; Zhu, P.; Wang, Y.; Wang, P. Comparison of different mandibular jawlines classifications on transoral endoscopic thyroidectomy for papillary thyroid carcinoma: Experiences of 690 cases. Front. Endocrinol. 2022, 13, 842148. [Google Scholar] [CrossRef] [PubMed]
- Cohen, O.; Tufano, R.P.; Anuwong, A.; Russell, J.O.; Assadi, N.; Dionigi, G.; Kim, H.Y.; Bertelli, A.; Khafif, A. Trans-oral endoscopic thyroidectomy vestibular approach (TOETVA) for the pediatric population: A multicenter, large case series. Surg. Endosc. 2021, 36, 2507–2513. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Deng, L.; Gong, Z.; Zhu, X. The advantages of applying a 5-mm endoscope in the transoral endoscopic thyroidectomy vestibular approach. Surg. Laparosc. Endosc. Percutaneous Tech. 2022, 32, 357–361. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Wang, T.; Kim, H.Y.; Wang, P.; Dionigi, G.; Pino, A.; Sun, H. Strategies for superior thyroid pole dissection in transoral thyroidectomy: A video operative guide. Surg. Endosc. 2020, 34, 3711–3721. [Google Scholar] [CrossRef] [PubMed]
- Olds, K.; Hillel, A.T.; Cha, E.; Curry, M.; Akst, L.M.; Taylor, R.H.; Richmon, J.D. Robotic endolaryngeal flexible (Robo-ELF) scope: A preclinical feasibility study. Laryngoscope 2011, 121, 2371–2374. [Google Scholar] [CrossRef] [PubMed]
- Shaear, M.; Russell, J.O.; Steck, S.; Liu, R.H.; Chen, L.W.; Razavi, C.R.; Tufano, R.P. The intuitive da Vinci single port surgical system and feasibility of transoral thyroidectomy vestibular approach. Ann. Thyroid. 2020, 5, 20. [Google Scholar] [CrossRef]
- Haidegger, T.; Benyó, B.; Kovács, L.; Benyó, Z. Force sensing and force control for surgical robots. IFAC Proc. Vol. 2009, 42, 401–406. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).