
Biomarker Dynamics and Long-Term Treatment Outcomes in Breast Cancer Patients with Residual Cancer Burden after Neoadjuvant Therapy

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population and Follow-Up
2.2. Pathological Assessment and Breast Cancer Subtype Classification
2.3. Residual Cancer Burden Assessment
2.4. Long-Term Outcomes and Statistical Analysis
3. Results
3.1. Baseline Characteristics and Treatment Response to NAT
3.2. Residual Cancer Burden and Biomarker Dynamics after NAT
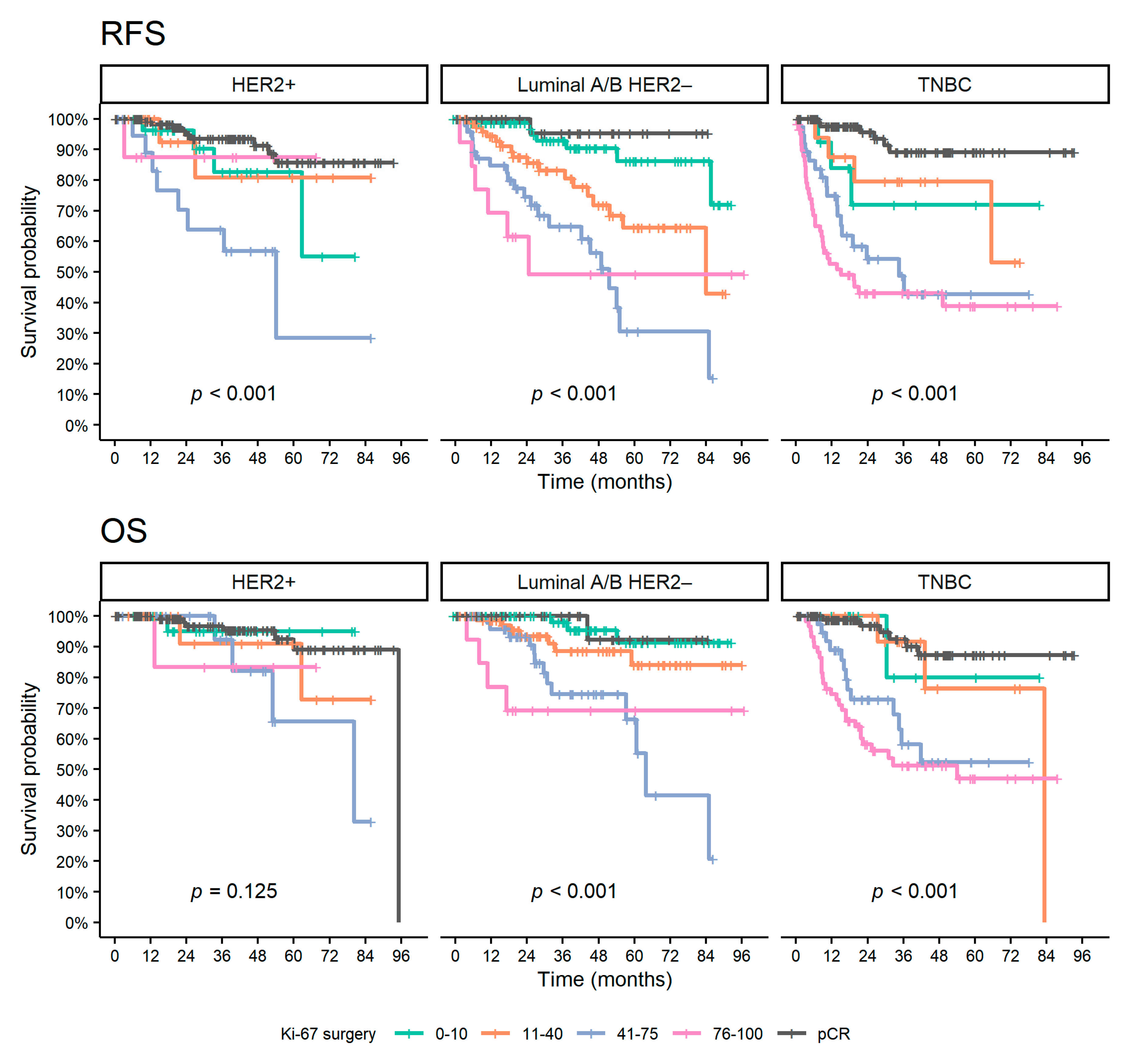
3.3. Ki-67 Expression and Long-Term Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burstein, H.; Curigliano, G.; Thürlimann, B.; Weber, W.; Poortmans, P.; Regan, M.; Senn, H.; Winer, E.; Gnant, M.; Aebi, S.; et al. Customizing local and systemic therapies for women with early breast cancer: The St. Gallen International Consensus Guidelines for treatment of early breast cancer 2021. Ann. Oncol. 2021, 32, 1216–1235. [Google Scholar] [CrossRef] [PubMed]
- Denduluri, N.; Somerfield, M.R.; Chavez-MacGregor, M.; Comander, A.H.; Dayao, Z.; Eisen, A.; Freedman, R.A.; Gopalakrishnan, R.; Graff, S.L.; Hassett, M.J.; et al. Selection of Optimal Adjuvant Chemotherapy and Targeted Therapy for Early Breast Cancer: ASCO Guideline Update. J. Clin. Oncol. 2021, 39, 685–693. [Google Scholar] [CrossRef] [PubMed]
- Korde, L.A.; Somerfield, M.R.; Carey, L.A.; Crews, J.R.; Denduluri, N.; Hwang, E.S.; Khan, S.A.; Loibl, S.; Morris, E.A.; Perez, A.; et al. Neoadjuvant Chemotherapy, Endocrine Therapy, and Targeted Therapy for Breast Cancer: ASCO Guideline. J. Clin. Oncol. 2021, 39, 1485–1505. [Google Scholar] [CrossRef]
- Cortazar, P.; Geyer, C.E. Pathological Complete Response in Neoadjuvant Treatment of Breast Cancer. Ann. Surg. Oncol. 2015, 22, 1441–1446. [Google Scholar] [CrossRef]
- Cortazar, P.; Zhang, L.; Untch, M.; Mehta, K.; Costantino, J.P.; Wolmark, N.; Bonnefoi, H.; Cameron, D.; Gianni, L.; Valagussa, P.; et al. Pathological complete response and long-term clinical benefit in breast cancer: The CTNeoBC pooled analysis. Lancet 2014, 384, 164–172. [Google Scholar] [CrossRef] [Green Version]
- Von Minckwitz, G.; Untch, M.; Blohmer, J.-U.; Costa, S.D.; Eidtmann, H.; Fasching, P.A.; Gerber, B.; Eiermann, W.; Hilfrich, J.; Huober, J.; et al. Definition and Impact of Pathologic Complete Response on Prognosis After Neoadjuvant Chemotherapy in Various Intrinsic Breast Cancer Subtypes. J. Clin. Oncol. 2012, 30, 1796–1804. [Google Scholar] [CrossRef] [Green Version]
- Liedtke, C.; Mazouni, C.; Hess, K.R.; André, F.; Tordai, A.; Mejia, J.A.; Symmans, W.F.; Gonzalez-Angulo, A.M.; Hennessy, B.; Green, M.; et al. Response to Neoadjuvant Therapy and Long-Term Survival in Patients With Triple-Negative Breast Cancer. J. Clin. Oncol. 2008, 26, 1275–1281. [Google Scholar] [CrossRef]
- Mamounas, E.P.; Anderson, S.J.; Dignam, J.J.; Bear, H.D.; Julian, T.B.; Geyer, C.E., Jr.; Taghian, A.; Wickerham, D.L.; Wolmark, N. Predictors of Locoregional Recurrence After Neoadjuvant Chemotherapy: Results From Combined Analysis of National Surgical Adjuvant Breast and Bowel Project B-18 and B-27. J. Clin. Oncol. 2012, 30, 3960–3966. [Google Scholar] [CrossRef]
- Yau, C.; Osdoit, M.; van der Noordaa, M.; Shad, S.; Wei, J.; de Croze, D.; Hamy, A.-S.; Laé, M.; Reyal, F.; Sonke, G.S.; et al. Residual cancer burden after neoadjuvant chemotherapy and long-term survival outcomes in breast cancer: A multicentre pooled analysis of 5161 patients. Lancet Oncol. 2022, 23, 149–160. [Google Scholar] [CrossRef]
- Hamy, A.-S.; Darrigues, L.; Laas, E.; De Croze, D.; Topciu, L.; Lam, G.-T.; Evrevin, C.; Rozette, S.; Laot, L.; Lerebours, F.; et al. Prognostic value of the Residual Cancer Burden index according to breast cancer subtype: Validation on a cohort of BC patients treated by neoadjuvant chemotherapy. PLoS ONE 2020, 15, e0234191. [Google Scholar] [CrossRef] [PubMed]
- Symmans, W.F.; Peintinger, F.; Hatzis, C.; Rajan, R.; Kuerer, H.; Valero, V.; Assad, L.; Poniecka, A.; Hennessy, B.; Green, M.; et al. Measurement of Residual Breast Cancer Burden to Predict Survival After Neoadjuvant Chemotherapy. J. Clin. Oncol. 2007, 25, 4414–4422. [Google Scholar] [CrossRef] [PubMed]
- Petrelli, F.; Coinu, A.; Lonati, V.; Cabiddu, M.; Ghilardi, M.; Borgonovo, K.; Barni, S. Neoadjuvant dose-dense chemotherapy for locally advanced breast cancer: A Meta-Analysis of Published Studies. Anti-Cancer Drugs 2016, 27, 702–708. [Google Scholar] [CrossRef]
- Kr, A. Dose dense neoadjuvant and adjuvant chemotherapy in triple-negative breast cancer patients: Survival analysis. Ann. Oncol. 2019, 30, iii37. [Google Scholar] [CrossRef]
- Wang, L.; Zhang, Y.; He, Y.; Li, J.; Wang, T.; Xie, Y.; Fan, Z.; Ouyang, T. Impact of dose-dense neoadjuvant chemotherapy on pathologic response and survival for HER2-positive breast cancer patients who receive trastuzumab. NPJ Breast Cancer 2021, 7, 75. [Google Scholar] [CrossRef]
- Gianni, L.; Pienkowski, T.; Im, Y.-H.; Roman, L.; Tseng, L.-M.; Liu, M.-C.; Lluch, A.; Staroslawska, E.; De La Haba-Rodriguez, J.; Im, S.-A.; et al. Efficacy and safety of neoadjuvant pertuzumab and trastuzumab in women with locally advanced, inflammatory, or early HER2-positive breast cancer (NeoSphere): A randomised multicentre, open-label, phase 2 trial. Lancet Oncol. 2012, 13, 25–32. [Google Scholar] [CrossRef]
- Schneeweiss, A.; Chia, S.; Hickish, T.; Harvey, V.; Eniu, A.; Hegg, R.; Tausch, C.; Seo, J.H.; Tsai, Y.-F.; Ratnayake, J.; et al. Pertuzumab plus trastuzumab in combination with standard neoadjuvant anthracycline-containing and anthracycline-free chemotherapy regimens in patients with HER2-positive early breast cancer: A randomized phase II cardiac safety study (TRYPHAENA). Ann. Oncol. 2013, 24, 2278–2284. [Google Scholar] [CrossRef]
- Byrski, T.; Huzarski, T.; Dent, R.; Marczyk, E.; Jasiówka, M.; Gronwald, J.; Jakubowicz, J.; Cybulski, C.; Wisniowski, R.; Godlewski, D.; et al. Pathologic complete response to neoadjuvant cisplatin in BRCA1-positive breast cancer patients. Breast Cancer Res. Treat. 2014, 147, 401–405. [Google Scholar] [CrossRef]
- Telli, M.L.; Jensen, K.C.; Vinayak, S.; Kurian, A.W.; Lipson, J.A.; Flaherty, P.J.; Timms, K.; Abkevich, V.; Schackmann, E.A.; Wapnir, I.L.; et al. Phase II Study of Gemcitabine, Carboplatin, and Iniparib As Neoadjuvant Therapy for Triple-Negative and BRCA1/2 Mutation–Associated Breast Cancer With Assessment of a Tumor-Based Measure of Genomic Instability: PrECOG 0105. J. Clin. Oncol. 2015, 33, 1895–1901. [Google Scholar] [CrossRef] [Green Version]
- von Minckwitz, G.; Schneeweiss, A.; Loibl, S.; Salat, C.; Denkert, C.; Rezai, M.; Blohmer, J.U.; Jackisch, C.; Paepke, S.; Gerber, B.; et al. Neoadjuvant carboplatin in patients with triple-negative and HER2-positive early breast cancer (GeparSixto; GBG 66): A randomised phase 2 trial. Lancet Oncol. 2014, 15, 747–756. [Google Scholar] [CrossRef]
- Alba, E.; Chacon, J.I.; Lluch, A.; Anton, A.; Estevez, L.; Cirauqui, B.; Carrasco, E.; Calvo, L.; Segui, M.A.; Ribelles, N.; et al. A randomized phase II trial of platinum salts in basal-like breast cancer patients in the neoadjuvant setting. Results from the GEICAM/2006-03, multicenter study. Breast Cancer Res. Treat. 2012, 136, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Mayer, E.L.; Abramson, V.; Jankowitz, R.; Falkson, C.; Marcom, P.K.; Traina, T.; Carey, L.; Rimawi, M.; Specht, J.; Miller, K.; et al. TBCRC 030: A phase II study of preoperative cisplatin versus paclitaxel in triple-negative breast cancer: Evaluating the homologous recombination deficiency (HRD) biomarker. Ann. Oncol. 2020, 31, 1518–1525. [Google Scholar] [CrossRef] [PubMed]
- Schmid, P.; Cortes, J.; Pusztai, L.; McArthur, H.; Kümmel, S.; Bergh, J.; Denkert, C.; Park, Y.H.; Hui, R.; Harbeck, N.; et al. Pembrolizumab for Early Triple-Negative Breast Cancer. N. Engl. J. Med. 2020, 382, 810–821. [Google Scholar] [CrossRef]
- Nahleh, Z.A.; Sivasubramaniam, D.; Dhaliwal, S.; Sundarajan, V.; Komrokji, R. Residual Cancer Burden in Locally Advanced Breast Cancer: A Superior Tool. Curr. Oncol. 2008, 15, 271–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coiro, S.; Gasparini, E.; Falco, G.; Santandrea, G.; Foroni, M.; Besutti, G.; Iotti, V.; Di Cicilia, R.; Foroni, M.; Mele, S.; et al. Biomarkers Changes after Neoadjuvant Chemotherapy in Breast Cancer: A Seven-Year Single Institution Experience. Diagnostics 2021, 11, 2249. [Google Scholar] [CrossRef] [PubMed]
- Lokuhetty, D.; White, V.A.; Watanabe, R.; Cree, I.A.; WHO. Classification of Tumours Editorial Board; International Agency for Research on Cancer Breast Tumours: Lyon, France, 2019; ISBN 978-92-832-4500-1.
- Wolff, A.C.; Hammond, M.E.H.; Allison, K.H.; Harvey, B.E.; Mangu, P.B.; Bartlett, J.M.S.; Bilous, M.; Ellis, I.O.; Fitzgibbons, P.; Hanna, W.; et al. Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline Focused Update. Arch. Pathol. Lab. Med. 2018, 142, 1364–1382. [Google Scholar] [CrossRef] [Green Version]
- Fujii, T.; Kogawa, T.; Dong, W.; Sahin, A.A.; Moulder, S.; Litton, J.K.; Tripathy, D.; Iwamoto, T.; Hunt, K.K.; Pusztai, L.; et al. Revisiting the definition of estrogen receptor positivity in HER2-negative primary breast cancer. Ann. Oncol. 2017, 28, 2420–2428. [Google Scholar] [CrossRef]
- Bankhead, P.; Loughrey, M.B.; Fernández, J.A.; Dombrowski, Y.; McArt, D.G.; Dunne, P.D.; McQuaid, S.; Gray, R.T.; Murray, L.J.; Coleman, H.G.; et al. QuPath: Open source software for digital pathology image analysis. Sci. Rep. 2017, 7, 16878. [Google Scholar] [CrossRef] [Green Version]
- Kaplan, E.L.; Meier, P. Nonparametric Estimation from Incomplete Observations. J. Am. Stat. Assoc. 1958, 53, 457–481. [Google Scholar] [CrossRef]
- Cox, D.R. Regression Models and Life-Tables. J. R. Stat. Soc. Ser. B Methodol. 1972, 34, 187–220. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2013; ISBN 3-900051-070. Available online: http://www.R-project.org/ (accessed on 8 February 2021).
- Del Prete, S.; Caraglia, M.; Luce, A.; Montella, L.; Galizia, G.; Sperlongano, P.; Cennamo, G.; Lieto, E.; Capasso, E.; Fiorentino, O.; et al. Clinical and pathological factors predictive of response to neoadjuvant chemotherapy in breast cancer: A single center experience. Oncol. Lett. 2019, 18, 3873–3879. [Google Scholar] [CrossRef] [PubMed]
- Fasching, P.A.; Heusinger, K.; Haeberle, L.; Niklos, M.; Hein, A.; Bayer, C.M.; Rauh, C.; Schulz-Wendtland, R.; Bani, M.R.; Schrauder, M.; et al. Ki67, chemotherapy response, and prognosis in breast cancer patients receiving neoadjuvant treatment. BMC Cancer 2011, 11, 486. [Google Scholar] [CrossRef] [Green Version]
- Chen, R.; Ye, Y.; Yang, C.; Peng, Y.; Zong, B.; Qu, F.; Tang, Z.; Wang, Y.; Su, X.; Li, H.; et al. Assessment of the predictive role of pretreatment Ki-67 and Ki-67 changes in breast cancer patients receiving neoadjuvant chemotherapy according to the molecular classification: A retrospective study of 1010 patients. Breast Cancer Res. Treat. 2018, 170, 35–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loibl, S.; von Minckwitz, G.; Untch, M.; Denkert, C.; Group, C.; on behalf of the German Breast Group. Predictive Factors for Response to Neoadjuvant Therapy in Breast Cancer. Oncol. Res. Treat. 2014, 37, 563–568. [Google Scholar] [CrossRef] [PubMed]
- Sheri, A.; Smith, I.E.; Johnston, S.R.; A’Hern, R.; Nerurkar, A.; Jones, R.; Hills, M.; Detre, S.; Pinder, S.E.; Symmans, W.F.; et al. Residual proliferative cancer burden to predict long-term outcome following neoadjuvant chemotherapy. Ann. Oncol. 2014, 26, 75–80. [Google Scholar] [CrossRef]
- Nielsen, T.O.; Leung, S.C.Y.; Rimm, D.L.; Dodson, A.; Acs, B.; Badve, S.; Denkert, C.; Ellis, M.J.; Fineberg, S.; Flowers, M.; et al. Assessment of Ki67 in Breast Cancer: Updated Recommendations From the International Ki67 in Breast Cancer Working Group. J. Natl. Cancer Inst. 2020, 113, 808–819. [Google Scholar] [CrossRef]
- Li, X.; Wang, M.; Wang, M.; Yu, X.; Guo, J.; Sun, T.; Yao, L.; Zhang, Q.; Xu, Y. Predictive and Prognostic Roles of Pathological Indicators for Patients with Breast Cancer on Neoadjuvant Chemotherapy. J. Breast Cancer 2019, 22, 497–521. [Google Scholar] [CrossRef]
- Hirata, T.; Shimizu, C.; Yonemori, K.; Hirakawa, A.; Kouno, T.; Tamura, K.; Ando, M.; Katsumata, N.; Fujiwara, Y. Change in the hormone receptor status following administration of neoadjuvant chemotherapy and its impact on the long-term outcome in patients with primary breast cancer. Br. J. Cancer 2009, 101, 1529–1536. [Google Scholar] [CrossRef] [Green Version]
- Jin, X.; Jiang, Y.-Z.; Chen, S.; Yu, K.-D.; Shao, Z.-M.; Di, G.-H. Prognostic value of receptor conversion after neoadjuvant chemotherapy in breast cancer patients: A prospective observational study. Oncotarget 2015, 6, 9600–9611. [Google Scholar] [CrossRef] [Green Version]
- Matsubara, N.; Mukai, H.; Masumoto, M.; Sasaki, M.; Naito, Y.; Fujii, S.; Wada, N. Survival outcome and reduction rate of Ki-67 between pre- and post-neoadjuvant chemotherapy in breast cancer patients with non-pCR. Breast Cancer Res. Treat. 2014, 147, 95–102. [Google Scholar] [CrossRef]
- Focke, C.M.; Bürger, H.; van Diest, P.J.; Finsterbusch, K.; Gläser, D.; Korsching, E.; Decker, T.; Anders, M.; Bollmann, R.; Eiting, F.; et al. Interlaboratory variability of Ki67 staining in breast cancer. Eur. J. Cancer 2017, 84, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Polley, M.-Y.C.; Leung, S.C.Y.; McShane, L.M.; Gao, D.; Hugh, J.C.; Mastropasqua, M.G.; Viale, G.; Zabaglo, L.A.; Penault-Llorca, F.; Bartlett, J.M.; et al. An International Ki67 Reproducibility Study. J. Natl. Cancer Inst. 2013, 105, 1897–1906. [Google Scholar] [CrossRef] [PubMed]
- Pistelli, M.; Merloni, F.; Crocetti, S.; Scortichini, L.; Tassone, L.; Cantini, L.; Agostinelli, V.; Bastianelli, L.; Savini, A.; Berardi, R. Prognostic Impact of Ki-67 Change in Locally Advanced and Early Breast Cancer after Neoadjuvant Chemotherapy: A Single Institution Experience. J. Oncol. 2021, 2021, e5548252. [Google Scholar] [CrossRef] [PubMed]
- Montagna, E.; Bagnardi, V.; Viale, G.; Rotmensz, N.; Sporchia, A.; Cancello, G.; Balduzzi, A.; Galimberti, V.; Veronesi, P.; Luini, A.; et al. Changes in PgR and Ki-67 in residual tumour and outcome of breast cancer patients treated with neoadjuvant chemotherapy. Ann. Oncol. 2014, 26, 307–313. [Google Scholar] [CrossRef]
- Cabrera-Galeana, P.; Muñoz-Montaño, W.; Lara-Medina, F.; Alvarado-Miranda, A.; Pérez-Sánchez, V.; Villarreal-Garza, C.; Quintero, R.M.; Porras-Reyes, F.; Bargallo-Rocha, E.; Del Carmen, I.; et al. Ki67 Changes Identify Worse Outcomes in Residual Breast Cancer Tumors After Neoadjuvant Chemotherapy. Oncologist 2018, 23, 670–678. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Group (n = 767) | aRCB Group (n = 468) | |||||
|---|---|---|---|---|---|---|
| Variables | HER2+ n = 238 | Luminal A/B HER2– n = 286 | TNBC n = 243 | HER2+ n = 94 | Luminal A/B HER2– n = 240 | TNBC n = 134 |
| Age (years) | ||||||
| Median (IQR) | 52 (41, 62) | 48 (40, 60) | 46 (37, 58) | 53 (40, 63) | 48 (39, 60) | 49 (37, 60) |
| Range | 24, 85 | 20, 78 | 17, 78 | 25, 85 | 20, 78 | 23, 78 |
| Menopausal status | ||||||
| Pre | 113 (47%) | 151 (53%) | 132 (54%) | 42 (45%) | 125 (52%) | 68 (51%) |
| Peri/post | 125 (53%) | 135 (47%) | 111 (46%) | 52 (55%) | 115 (48%) | 66 (49%) |
| BRCA1/2 | ||||||
| Not tested | 142 (60%) | 160 (56%) | 55 (23%) | 52 (55%) | 136 (57%) | 37 (28%) |
| Wild type | 90 (38%) | 86 (30%) | 114 (47%) | 40 (43%) | 79 (33%) | 65 (49%) |
| Mutated | 6 (2.5%) | 40 (14%) | 74 (30%) | 2 (2.1%) | 25 (10%) | 32 (24%) |
| cT | ||||||
| is | 2 (0.8%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| 1 | 26 (11%) | 38 (13%) | 26 (11%) | 7 (7.4%) | 29 (12%) | 11 (8.2%) |
| 2 | 125 (53%) | 164 (57%) | 157 (65%) | 47 (50%) | 134 (56%) | 80 (60%) |
| 3 | 27 (11%) | 48 (17%) | 37 (15%) | 13 (14%) | 44 (18%) | 27 (20%) |
| 4 | 36 (15%) | 21 (7.3%) | 12 (4.9%) | 19 (20%) | 20 (8.3%) | 8 (6.0%) |
| 4d | 22 (9.2%) | 15 (5.2%) | 11 (4.5%) | 8 (8.5%) | 13 (5.4%) | 8 (6.0%) |
| cN | ||||||
| 0 | 69 (29%) | 82 (29%) | 98 (40%) | 27 (29%) | 64 (27%) | 55 (41%) |
| 1 | 147 (62%) | 172 (61%) | 124 (51%) | 58 (62%) | 146 (61%) | 67 (50%) |
| 2 | 15 (6.3%) | 22 (7.7%) | 18 (7.4%) | 6 (6.4%) | 20 (8.4%) | 10 (7.5%) |
| 3 | 7 (2.9%) | 8 (2.8%) | 3 (1.2%) | 3 (3.2%) | 8 (3.4%) | 2 (1.5%) |
| Unknown | 0 | 2 | 0 | 0 | 2 | 0 |
| Histology | ||||||
| NST | 228 (96%) | 269 (94%) | 233 (96%) | 89 (95%) | 225 (94%) | 131 (98%) |
| Other # | 10 (4.2%) | 17 (5.9%) | 10 (4.1%) | 5 (5.3%) | 15 (6.2%) | 3 (2.2%) |
| Grade | ||||||
| 1 | 1 (0.4%) | 10 (3.6%) | 1 (0.4%) | 1 (1.1%) | 10 (4.3%) | 1 (0.8%) |
| 2 | 74 (32%) | 116 (42%) | 21 (8.9%) | 33 (36%) | 106 (45%) | 11 (8.5%) |
| 2–3 | 24 (10%) | 25 (9.0%) | 12 (5.1%) | 11 (12%) | 23 (9.9%) | 7 (5.4%) |
| 3 | 135 (58%) | 127 (46%) | 201 (86%) | 47 (51%) | 94 (40%) | 111 (85%) |
| NS | 4 | 8 | 8 | 2 | 7 | 4 |
| NAT regimens * | ||||||
| A | 0 (0%) | 20 (7.0%) | 9 (3.7%) | 0 (0%) | 17 (7.1%) | 7 (5.2%) |
| A→cDDP | 0 (0%) | 8 (2.8%) | 21 (8.6%) | 0 (0%) | 5 (2.1%) | 9 (6.7%) |
| A→T | 229 (96%) | 241 (84%) | 160 (66%) | 88 (94%) | 207 (86%) | 89 (66%) |
| A→T + CBDCA | 0 (0%) | 16 (5.6%) | 53 (22%) | 0 (0%) | 10 (4.2%) | 29 (22%) |
| T | 9 (3.8%) | 1 (0.3%) | 0 (0%) | 6 (6.4%) | 1 (0.4%) | 0 (0%) |
| Dose dense | 2 (0.8%) | 5 (1.7%) | 41 (17%) | 0 (0%) | 3 (1.3%) | 18 (13%) |
| Variable | HER2+ n = 94 | Luminal A/B HER2– n = 240 | TNBC n = 134 | |||
|---|---|---|---|---|---|---|
| Biopsy Specimen | Surgical Specimen | Biopsy Specimen | Surgical Specimen | Biopsy Specimen | Surgical Specimen | |
| pT | ||||||
| 0, is | 3 (3.2%) | 19 (7.9%) | 6 (4.5%) | |||
| 1mi, 1 | 73 (78%) | 138 (58%) | 75 (56%) | |||
| 2–4 | 18 (19%) | 82 (34%) | 52 (39%) | |||
| NS | 0 | 1 | 1 | |||
| pN | ||||||
| 0, itc | 49 (52%) | 72 (30%) | 75 (56%) | |||
| 1mi, 1 | 35 (37%) | 94 (40%) | 34 (26%) | |||
| 2–3 | 10 (11%) | 71 (30%) | 24 (18%) | |||
| NS | 0 | 3 | 1 | |||
| HER2 | ||||||
| Negative | 0 (0%) | 10 (17%) | 240 (100%) | 114 (95%) | 134 (100%) | 75 (95%) |
| Positive | 94 (100%) | 49 (83%) | 0 (0%) | 6 (5.0%) | 0 (0%) | 4 (5.1%) |
| Not tested | 35 | 120 | 55 | |||
| SR | ||||||
| Negative | 27 (29%) | 14 (24%) | 0 (0%) | 12 (8.5%) | 133 (100%) | 71 (91%) |
| Positive | 66 (71%) | 45 (76%) | 240 (100%) | 130 (92%) | 0 (0%) | 7 (9.0%) |
| Not tested | 1 | 35 | 0 | 98 | 1 | 56 |
| ER (%) | ||||||
| Median (IQR) | 80 (5, 100) | 90 (0, 100) | 100 (90, 100) | 100 (95, 100) | 0 (0, 0) | 0 (0, 0) |
| Range | 0, 100 | 0, 100 | 0, 100 | 0, 100 | 0, 10 | 0, 50 |
| 0–10 | 29 (31%) | 19 (30%) | 10 (4.2%) | 14 (9.9%) | 134 (100%) | 84 (93%) |
| >10 | 64 (69%) | 45 (70%) | 230 (96%) | 128 (90%) | 0 (0%) | 6 (6.7%) |
| Not tested | 1 | 30 | 0 | 98 | 0 | 44 |
| PR (%) | ||||||
| Median (IQR) | 15 (0, 80) | 0 (0, 45) | 58 (14, 90) | 20 (0, 80) | 0 (0, 0) | 0 (0, 0) |
| Range | 0, 100 | 0, 100 | 0, 100 | 0, 100 | 0, 10 | 0, 15 |
| 0–10 | 46 (49%) | 33 (67%) | 59 (25%) | 65 (49%) | 133 (100%) | 76 (99%) |
| >10 | 47 (51%) | 16 (33%) | 181 (75%) | 67 (51%) | 0 (0%) | 1 (1.3%) |
| Not tested | 1 | 45 | 0 | 108 | 1 | 57 |
| Ki-67 (%) | ||||||
| Median (IQR) | 50 (35, 67) | 18 (6, 48) | 40 (30, 60) | 18 (7, 44) | 74 (60, 90) | 72 (41, 90) |
| Range | 5, 90 | 1, 100 | 5, 97 | 0, 99 | 15, 98 | 2, 100 |
| 0–10 | 1 (1.1%) | 30 (37%) | 7 (3.0%) | 80 (36%) | 0 (0%) | 14 (11%) |
| 11–40 | 27 (31%) | 23 (28%) | 114 (48%) | 79 (36%) | 11 (8.7%) | 18 (14%) |
| 41–75 | 52 (59%) | 20 (25%) | 94 (40%) | 50 (23%) | 54 (43%) | 38 (29%) |
| 76–100 | 8 (9.1%) | 8 (9.9%) | 22 (9.3%) | 11 (5.0%) | 62 (49%) | 59 (46%) |
| NS | 6 | 13 | 3 | 20 | 7 | 5 |
| LVI | ||||||
| No | 80 (85%) | 154 (66%) | 101 (76%) | |||
| Yes | 14 (15%) | 80 (34%) | 32 (24%) | |||
| NS | 0 | 6 | 1 | |||
| ER (Biopsy/Surgery) | PR (Biopsy/Surgery) | |||||||
|---|---|---|---|---|---|---|---|---|
| ≤10/≤10 | >10/>10 | ≤10/>10 | >10/≤10 | ≤10/≤10 | >10/>10 | ≤10/>10 | >10/≤10 | |
| HER2+ (n) | 17 (27%) | 40 (63%) | 4 (6%) | 2 (3%) | 24 (50%) | 13 (27%) | 2 (4%) | 9 (19%) |
| Concordance | 90.5% | 77.1% | ||||||
| Cohen’s kappa (95% CI) | 0.78 (0.61, 0.95) | 0.53 (0.29, 0.76) | ||||||
| Luminal A/B HER2—(n) | 6 (4%) | 127 (89%) | 1 (1%) | 8 (6%) | 33 (25%) | 60 (45%) | 7 (5%) | 32 (24%) |
| Concordance | 93.7% | 70.5% | ||||||
| Cohen’s kappa (95% CI) | 0.54 (0.28, 0.8) | 0.41 (0.26, 0.55) | ||||||
| TNBC (n) | 84 (93%) | 0 | 6 (7%) | 0 | 75 (99%) | 0 | 1 (1%) | 0 |
| Concordance | 93.3% | 98.7% | ||||||
| Cohen’s kappa (95% CI) | NS | NS | ||||||
| RFS | OS | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HER2+ | Luminal A/B HER2– | TNBC | HER2+ | Luminal A/B HER2– | TNBC | ||||||||
| HR | p-Value | HR | p-Value | HR | p-Value | HR | p-Value | HR | p-Value | HR | p-Value | ||
| Age | 10-years | 1.30 | 0.106 | 1.24 | 0.061 | 0.87 | 0.173 | 1.75 | 0.016 | 1.59 | 0.002 | 0.97 | 0.759 |
| Menopausal status | Pre | REF | 0.025 | REF | 0.133 | REF | 0.286 | REF | <0.001 | REF | 0.008 | REF | 0.773 |
| Peri/post | 3.22 | 1.51 | 0.75 | NS | 2.80 | 0.92 | |||||||
| cT | 1–2 | REF | 0.391 | REF | 0.035 | REF | 0.107 | REF | 0.058 | REF | 0.086 | REF | 0.141 |
| 3,4,4d | 1.50 | 1.79 | 1.57 | 3.86 | 1.90 | 1.58 | |||||||
| cN | 0 | REF | 0.633 | REF | 0.001 | REF | 0.007 | REF | 0.063 | REF | 0.003 | REF | 0.039 |
| 1–3 | 1.28 | 3.08 | 2.21 | 5.10 | 4.62 | 2.03 | |||||||
| pT | 0,is,1,1mi | REF | 0.268 | REF | 0.024 | REF | <0.001 | REF | 0.242 | REF | 0.056 | REF | 0.002 |
| 2–4 | 0.47 | 1.89 | 2.77 | 0.34 | 2.05 | 2.68 | |||||||
| pN | 0,itc | REF | 0.076 | REF | <0.001 | REF | <0.001 | REF | 0.509 | REF | 0.063 | REF | <0.001 |
| 1mi,1 | 2.36 | 2.14 | 2.13 | 1.53 | 1.23 | 2.05 | |||||||
| 2–3 | 5.66 | 6.14 | 2.67 | 5.60 | |||||||||
| Ki-67 biopsy(%) | 10% * | 1.08 | 0.531 | 1.16 | 0.016 | 1.05 | 0.466 | 1.37 | 0.076 | 1.24 | 0.010 | 1.03 | 0.708 |
| 0–10 | REF | 0.378 | REF | 0.087 | REF | 0.385 | REF | 0.132 | REF | 0.156 | REF | 0.723 | |
| 11–40 | |||||||||||||
| 41–75 | 1.62 | 1.89 | 0.71 | 3.83 | 1.66 | 0.71 | |||||||
| 76–100 | 1.46 | 1.06 | 2.82 | 0.91 | |||||||||
| Ki-67 surgery(%) | 10% * | 1.07 | 0.418 | 1.24 | <0.001 | 1.14 | 0.005 | 1.14 | 0.279 | 1.33 | <0.001 | 1.17 | 0.004 |
| 0–10 | REF | 0.134 | REF | <0.001 | REF | 0.003 | REF | 0.382 | REF | <0.001 | REF | 0.004 | |
| 11–40 | 0.66 | 2.83 | 1.88 | 2.54 | |||||||||
| 41–75 | 2.37 | 6.32 | 2.78 | 3.65 | 8.05 | 3.86 | |||||||
| 76–100 | 5.45 | 3.70 | 10.9 | 5.08 | |||||||||
| Difference in Ki-67 # | 10% * | 1.02 | 0.853 | 1.13 | 0.009 | 1.10 | 0.044 | 0.96 | 0.741 | 1.16 | 0.024 | 1.15 | 0.017 |
| LVI | No | REF | 0.906 | REF | 0.003 | REF | <0.001 | REF | 0.966 | REF | 0.067 | REF | 0.001 |
| Yes | 1.08 | 2.29 | 3.76 | 0.97 | 1.98 | 2.83 | |||||||
| RFS | OS | ||||||
|---|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | ||
| HER2+ | |||||||
| Ki-67 biopsy | 10% * | 1.12 | 0.83, 1.52 | 0.462 | 1.55 | 0.94, 2.58 | 0.067 |
| Ki-67 surgery | 10% * | 1.05 | 0.87, 1.27 | 0.594 | 0.98 | 0.70, 1.37 | 0.914 |
| Luminal A/B HER2– | |||||||
| Ki-67 biopsy | 10% * | 1.27 | 1.09, 1.49 | 0.002 | 1.27 | 1.03, 1.57 | 0.025 |
| Ki-67 surgery | 10% * | 1.30 | 1.17, 1.44 | <0.001 | 1.34 | 1.16, 1.55 | <0.001 |
| TNBC | |||||||
| Ki-67 biopsy | 10% * | 1.05 | 0.89, 1.24 | 0.585 | 0.95 | 0.78, 1.16 | 0.600 |
| Ki-67 surgery | 10% * | 1.10 | 0.99, 1.23 | 0.066 | 1.16 | 1.01, 1.34 | 0.030 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Holanek, M.; Selingerova, I.; Fabian, P.; Coufal, O.; Zapletal, O.; Petrakova, K.; Kazda, T.; Hrstka, R.; Poprach, A.; Zvarikova, M.; et al. Biomarker Dynamics and Long-Term Treatment Outcomes in Breast Cancer Patients with Residual Cancer Burden after Neoadjuvant Therapy. Diagnostics 2022, 12, 1740. https://doi.org/10.3390/diagnostics12071740
Holanek M, Selingerova I, Fabian P, Coufal O, Zapletal O, Petrakova K, Kazda T, Hrstka R, Poprach A, Zvarikova M, et al. Biomarker Dynamics and Long-Term Treatment Outcomes in Breast Cancer Patients with Residual Cancer Burden after Neoadjuvant Therapy. Diagnostics. 2022; 12(7):1740. https://doi.org/10.3390/diagnostics12071740
Chicago/Turabian StyleHolanek, Milos, Iveta Selingerova, Pavel Fabian, Oldrich Coufal, Ondrej Zapletal, Katarina Petrakova, Tomas Kazda, Roman Hrstka, Alexandr Poprach, Maria Zvarikova, and et al. 2022. "Biomarker Dynamics and Long-Term Treatment Outcomes in Breast Cancer Patients with Residual Cancer Burden after Neoadjuvant Therapy" Diagnostics 12, no. 7: 1740. https://doi.org/10.3390/diagnostics12071740