
Analysis of Nasal Foreign Bodies in South Korea: Over 10-Year Experience



Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Park, J.W.; Jung, J.H.; Kwak, Y.H.; Jung, J.Y. Epidemiology of pediatric visits to the emergency department due to foreign body injuries in South Korea: Nationwide cross-sectional study. Medicine 2019, 98, e15838. [Google Scholar] [CrossRef]
- Kiger, J.R.; Brenkert, T.E.; Losek, J.D. Nasal foreign body removal in children. Pediatr. Emerg. Care 2008, 24, 785–792. [Google Scholar] [CrossRef] [PubMed]
- Gregori, D.; Salerni, L.; Scarinzi, C.; Morra, B.; Berchialla, P.; Snidero, S.; Corradetti, R.; Passali, D. Foreign bodies in the nose causing complications and requiring hospitalization in children 0–14 age: Results from the European survey of foreign bodies injuries study. Rhinology 2008, 46, 28–33. [Google Scholar] [PubMed]
- Zavdy, O.; Viner, I.; London, N.; Menzely, T.; Hod, R.; Raveh, E.; Gilony, D. Intranasal foreign bodies: A 10-year analysis of a large cohort, in a tertiary medical center. Am. J. Emerg. Med. 2021, 50, 356–359. [Google Scholar] [CrossRef] [PubMed]
- Yan, S.; Zeng, N.; Chen, G.; Chen, Y.; Wu, Z.; Pan, H.; Teng, Y.; Ma, X.; Li, L. Presentation and management of nasal foreign bodies in a Chinese metro area. Medicine 2021, 100, e25626. [Google Scholar] [CrossRef] [PubMed]
- Pagella, F.; Pusateri, A.; Matti, E.; Riceputi, G.; Brambilla, I.; Marseglia, G.L.; Benazzo, M. Nasal foreign bodies management in children: Our experience in 106 patients. Clin. Otolaryngol. 2019, 44, 660–663. [Google Scholar] [CrossRef] [PubMed]
- Cetinkaya, E.A.; Arslan, İ.B.; Cukurova, İ. Nasal foreign bodies in children: Types, locations, complications and removal. Int. J. Pediatr. Otorhinolaryngol. 2015, 79, 1881–1885. [Google Scholar] [CrossRef]
- Sajid, T.; Shah, M.I.; Qamar Naqvi, S.R. Pattern of presentation of nasal foreign bodies, An Experience with 155 Patients. J. Ayub Med. Coll. Abbottabad 2018, 30, 548–550. [Google Scholar] [PubMed]
- Hira, İ.; Tofar, M.; Bayram, A.; Yaşar, M.; Mutlu, C.; Özcan, İ. Childhood nasal foreign bodies: Analysis of 1724 cases. Turk. Arch. Otorhinolaryngol. 2019, 57, 187–190. [Google Scholar] [CrossRef] [PubMed]
- Ocagli, H.; Azzolina, D.; Bressan, S.; Bottigliengo, D.; Settin, E.; Lorenzoni, G.; Gregori, D.; Da Dalt, L. Epidemiology and trends over time of foreign body injuries in the pediatric emergency department. Children 2021, 8, 938. [Google Scholar] [CrossRef] [PubMed]
- Abou-Elfadl, M.; Horra, A.; Abada, R.L.; Mahtar, M.; Roubal, M.; Kadiri, F. Nasal foreign bodies: Results of a study of 260 cases. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2015, 132, 343–346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peyre, H.; Hoertel, N.; Bernard, J.Y.; Rouffignac, C.; Forhan, A.; Taine, M.; Heude, B.; Ramus, F. Sex differences in psychomotor development during the preschool period: A longitudinal study of the effects of environmental factors and of emotional, behavioral, and social functioning. J. Exp. Child. Psychol. 2019, 178, 369–384. [Google Scholar] [CrossRef] [PubMed]
- Toivainen, T.; Papageorgiou, K.A.; Tosto, M.G.; Kovas, Y. Sex differences in non-verbal and verbal abilities in childhood and adolescence. Intelligence 2017, 64, 81–88. [Google Scholar] [CrossRef]
- Dann, L.; Doody, J.; Howard, R.; Blackburn, C.; Russell, J.; Barrett, M. Nasal foreign bodies in the paediatric emergency department. Ir. J. Med. Sci. 2019, 188, 1401–1405. [Google Scholar] [CrossRef] [PubMed]
- Cohen, H.A.; Goldberg, E.; Horev, Z. Removal of nasal foreign bodies in children. Clin. Pediatr. 1993, 32, 192. [Google Scholar] [CrossRef] [PubMed]
- Lou, Z.C. Analysis of nasal foreign bodies in 341 children. J. Laryngol. Otol. 2019, 133, 908–912. [Google Scholar] [CrossRef] [PubMed]
- Yaroko, A.A.; Baharudin, A. Patterns of nasal foreign body in northeast Malaysia: A five-year experience. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2015, 132, 257–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thabet, M.H.; Basha, W.M.; Askar, S. Button battery foreign bodies in children: Hazards, management, and recommendations. Biomed. Res. Int. 2013, 2013, 846091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guidera, A.K.; Stegehuis, H.R. Button batteries: The worst case scenario in nasal foreign bodies. N. Z. Med. J. 2010, 123, 68–73. [Google Scholar]
- Mackle, T.; Conlon, B. Foreign bodies of the nose and ears in children. Should these be managed in the accident and emergency setting? Int. J. Pediatr. Otorhinolaryngol. 2006, 70, 425–428. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Types of Foreign Bodies | Number (Percentage) |
|---|---|
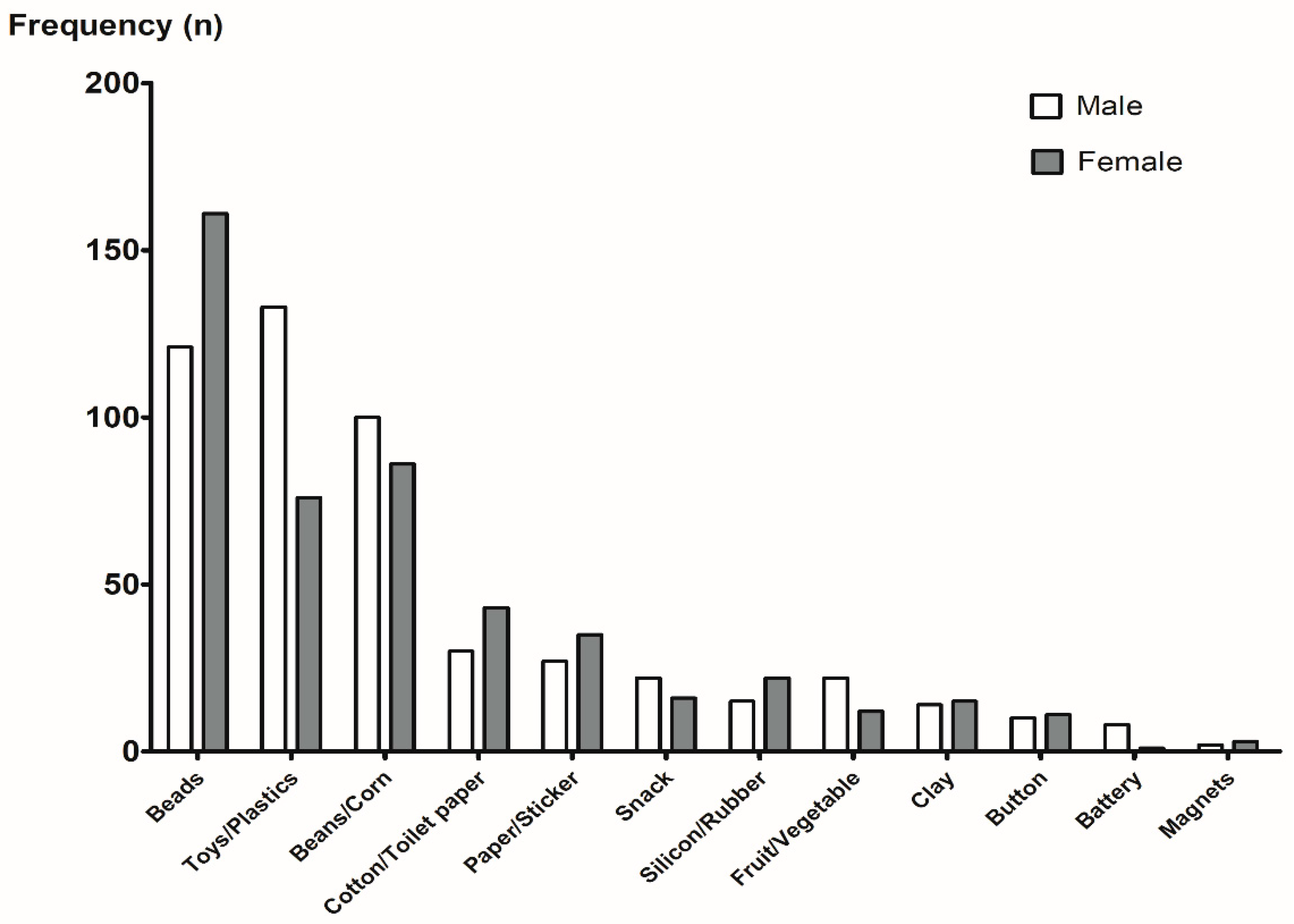
| Beads | 282 (24.0) |
| Toys/Plastics | 209 (17.8) |
| Beans/Corn | 186 (15.8) |
| Cotton/Toilet paper | 73 (6.2) |
| Paper/Sticker | 62 (5.3) |
| Snack | 38 (3.2) |
| Silicon/Rubber | 37 (3.1) |
| Fruit/Vegetable | 34 (2.9) |
| Clay | 29 (2.5) |
| Button | 21 (1.8) |
| Battery | 9 (0.8) |
| Magnets | 5 (0.4) |
| Others | 171 (14.5) |
| Age Groups | Top 5 Types of Foreign Bodies (Percentage) |
|---|---|
| 1–2 years | Beans/Corn (34.0%), Beads (17.5%), Toys/Plastics (11.3%), Cotton/Toilet paper (9.3%), Fruit/Vegetable (8.2%) |
| 2–3 years | Beans/Corn (24.5%), Beads (21.6%), Toys/Plastics (16.4%), Cotton/Toilet paper (8.6%), Paper/Sticker (7.5%) |
| 3–4 years | Beads (28.0%), Toys/Plastics (26.2%), Beans/Corn (16.8%), Paper/Sticker (6.1%), Silicon/Rubber (5.0%) |
| 4–5 years | Beads (45.0%), Toys/Plastics (25.5%), Beans/Corn (7.4%), Cotton/Toilet paper (6.0%), Paper/Sticker, Seeds (3.4%) |
| 5–6 years | Beads (42.1%), Toys/Plastics (24.6%), Cotton/Toilet paper (12.3%), Beans/Corn, Paper/Sticker (3.5%) |
| 6–7 years | Beads (30.8%), Toys/Plastics (26.9%), Beans/Corn, Cotton/Toilet paper, Paper/Sticker (3.5%) |
| 7–12 years | Beads (35.0%), Toys/Plastics (25.0%), Cotton/Toilet paper (15.0%), Paper/Sticker, Clay (10.0%) |
| ≥19 years | Cotton/Toilet paper (30.0%), Beads (10.0%), Rubber (10.0%), Fruits/Vegetable (10.0%), Paper/Sticker (10.0%) |
| Shape | Organic | Inorganic | Total |
|---|---|---|---|
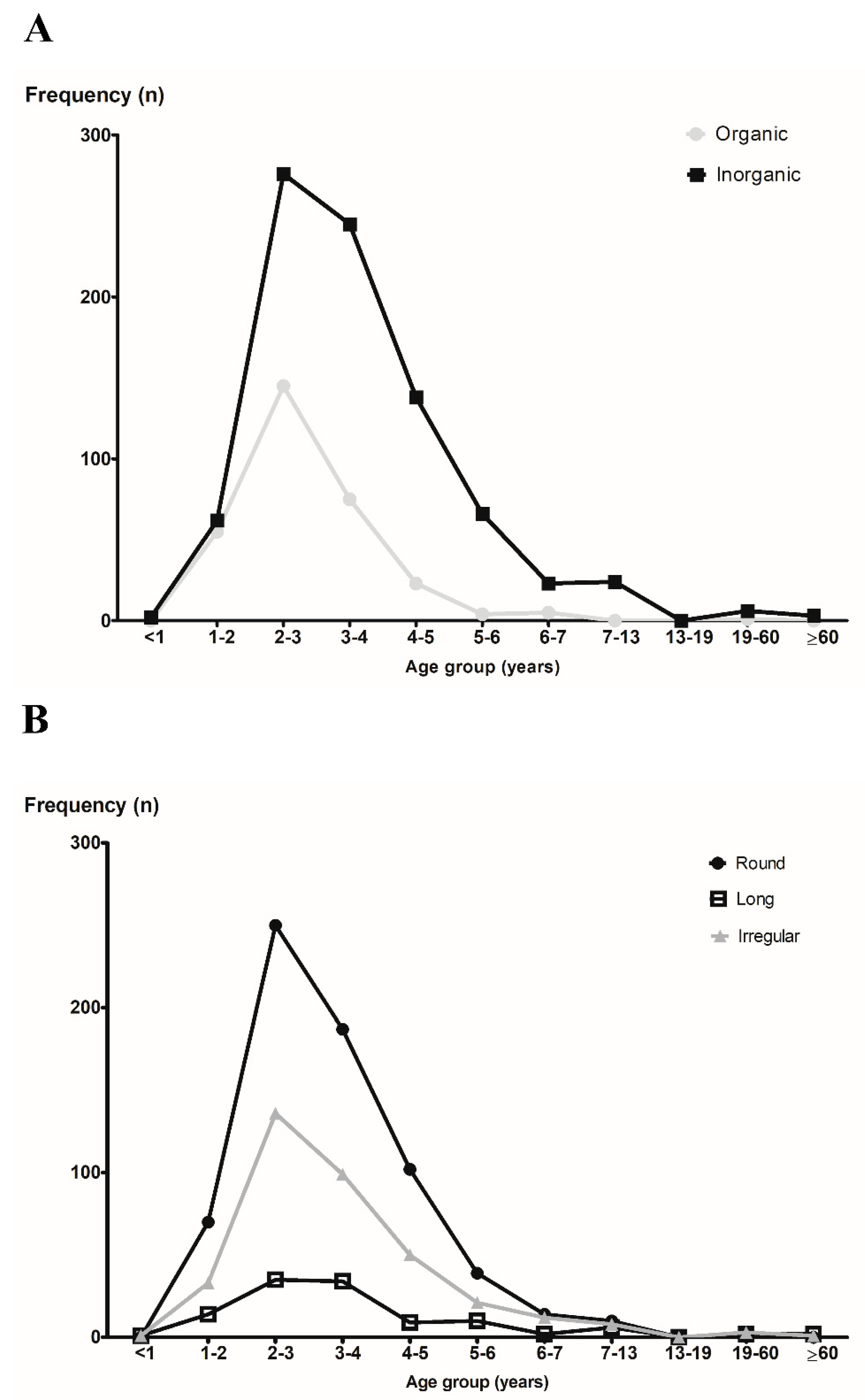
| Round | 276 | 398 | 674 (58.5%) |
| Long | 13 | 102 | 115 (10.0%) |
| Irregular | 19 | 345 | 364 (31.5%) |
| Total | 308 (26.7%) | 845 (73.3%) | 1153 |
| Symptoms | Onset (Days), Number (Percentage) | |||
|---|---|---|---|---|
| 0 | 1 | ≥2 | Total | |
| No symptoms | 1010 (98.6) | 13 (1.3) | 1 (0.1) | 1024 (83.4) |
| Foreign body sense | 25 (89.3) | 2 (7.1) | 1 (3.6) | 28 (2.3) |
| Pain | 24 (92.3) | 1 (3.8) | 1 (3.8) | 26 (2.1) |
| Epistaxis | 21 (91.3) | 0 (0.0) | 2 (8.7) | 23 (1.9) |
| Rhinorrhea | 12 (66.7) | 4 (22.2) | 2 (11.1) | 18 (1.5) |
| Cough | 10 (90.9) | 0 (0.0) | 1 (9.1) | 11 (0.9) |
| Nasal obstruction | 7 (70.0) | 1 (10.0) | 2 (20.0) | 10 (0.8) |
| Hoarseness | 1 (100.0) | 0 (0.0) | 0 (0.0) | 1 (0.1) |
| Foul odor | 0 (0.0) | 1 (100.0) | 0 (0.0) | 1 (0.1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, H.J.; Kim, S.W.; Lee, J.S.; Choi, H.G.; Wee, J.H. Analysis of Nasal Foreign Bodies in South Korea: Over 10-Year Experience. Diagnostics 2022, 12, 1810. https://doi.org/10.3390/diagnostics12081810
Jung HJ, Kim SW, Lee JS, Choi HG, Wee JH. Analysis of Nasal Foreign Bodies in South Korea: Over 10-Year Experience. Diagnostics. 2022; 12(8):1810. https://doi.org/10.3390/diagnostics12081810
Chicago/Turabian StyleJung, Hahn Jin, Sun Wook Kim, Joong Seob Lee, Hyo Geun Choi, and Jee Hye Wee. 2022. "Analysis of Nasal Foreign Bodies in South Korea: Over 10-Year Experience" Diagnostics 12, no. 8: 1810. https://doi.org/10.3390/diagnostics12081810
APA StyleJung, H. J., Kim, S. W., Lee, J. S., Choi, H. G., & Wee, J. H. (2022). Analysis of Nasal Foreign Bodies in South Korea: Over 10-Year Experience. Diagnostics, 12(8), 1810. https://doi.org/10.3390/diagnostics12081810