

Blood Basophils Relevance in Chronic Rhinosinusitis with Aspirin-Exacerbated Respiratory Disease
 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
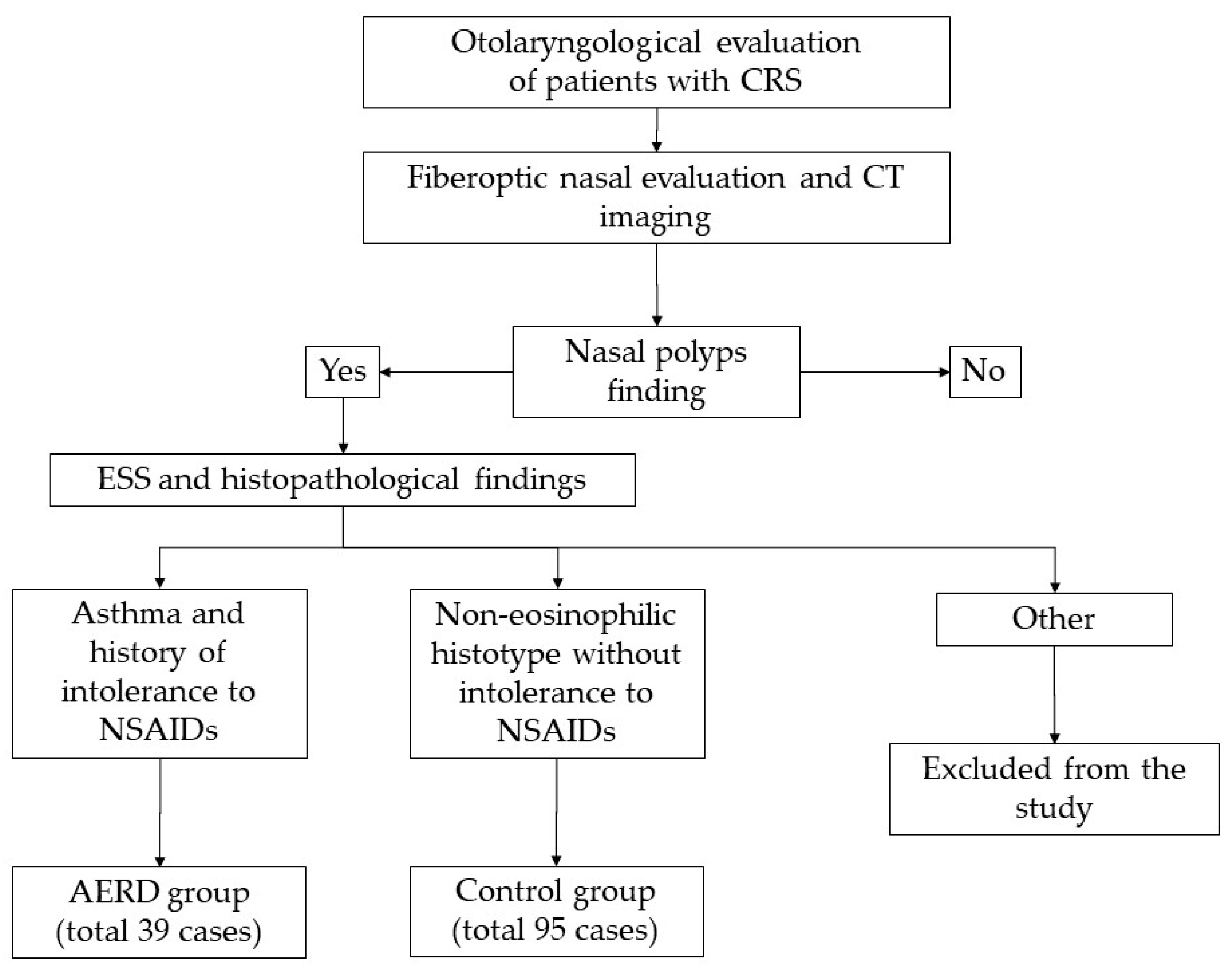
2.1. Patients
2.2. Statistical Methods
3. Results
3.1. Inter-Group Analysis (AERD Group vs. Control Group)
3.2. Intra-Group Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rajan, J.P.; Wineinger, N.E.; Stevenson, D.D.; White, A.A. Prevalence of aspirin-exacerbated respiratory disease among asthmatic patients: A meta-analysis of the literature. J. Allergy Clin. Immunol. 2015, 135, 676–681.e1. [Google Scholar] [CrossRef]
- Stevens, W.W.; Peters, A.T.; Hirsch, A.G.; Nordberg, C.M.; Schwartz, B.S.; Mercer, D.G.; Mahdavinia, M.; Grammer, L.C.; Hulse, K.E.; Kern, R.C.; et al. Clinical characteristics of patients with chronic rhinosinusitis with nasal polyps, asthma, and aspirin-exacerbated respiratory disease. J. Allergy Clin. Immunol. Pract. 2017, 5, 1061–1070.e3. [Google Scholar] [CrossRef]
- Laidlaw, T.M.; Mullol, J.; Woessner, K.M.; Amin, N.; Mannent, L.P. Chronic rhinosinusitis with nasal polyps and asthma. J. Allergy Clin. Immunol. Pract. 2021, 9, 1133–1141. [Google Scholar] [CrossRef] [PubMed]
- Walters, B.K.; Hagan, J.B.; Divekar, R.D.; Willson, T.J.; Stokken, J.K.; Pinheiro-Neto, C.D.; O’Brien, E.K.; Choby, G. Aspirin-Exacerbated Respiratory Disease and the Unified Airway: A Contemporary Review. Otolaryngol. Clin. N. Am. 2023, 56, 107–124. [Google Scholar] [CrossRef] [PubMed]
- White, A.A.; Stevenson, D.D. Aspirin-Exacerbated Respiratory Disease. N. Engl. J. Med. 2018, 379, 1060–1070. [Google Scholar] [CrossRef] [PubMed]
- Chung, K.F.; Wenzel, S.E.; Brozek, J.L.; Bush, A.; Castro, M.; Sterk, P.J.; Adcock, I.M.; Bateman, E.D.; Bel, E.H.; Bleecker, E.R.; et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur. Respir. J. 2014, 43, 343–373. [Google Scholar] [CrossRef]
- Mascia, K.; Borish, L.; Patrie, J.; Hunt, J.; Phillips, C.D.; Steinke, J.W. Chronic hyperplastic eosinophilic sinusitis as a predictor of aspirin-exacerbated respiratory disease. Ann. Allergy Asthma Immunol. 2005, 94, 652–657. [Google Scholar] [CrossRef]
- Young, J.; Frenkiel, S.; Tewfik, M.A.; Mouadeb, D.A. Long-term outcome analysis of endoscopic sinus surgery for chronic sinusitis. Am. J. Rhinol. 2007, 21, 743–747. [Google Scholar] [CrossRef]
- Brescia, G.; Alessandrini, L.; Parrino, D.; Franz, L.; Barion, U.; Marioni, G. Emerging contribution of histopathology to our understanding of chronic rhinosinusitis endotypes: Tissue eosinophil count and aggregates. Am. J. Rhinol. Allergy 2020, 34, 122–126. [Google Scholar] [CrossRef]
- Gevaert, P.; Han, J.K.; Smith, S.G.; Sousa, A.R.; Howarth, P.H.; Yancey, S.W.; Chan, R.; Bachert, C. The roles of eosinophils and interleukin-5 in the pathophysiology of chronic rhinosinusitis with nasal polyps. Int. Forum. Allergy Rhinol. 2022, 12, 1413–1423. [Google Scholar] [CrossRef]
- Li, X.; Wang, Z.; Chang, L.; Chen, X.; Yang, L.; Lai, X.; Li, S.; Huang, J.; Huang, Z.; Wu, X.; et al. γδT cells contribute to type 2 inflammatory profiles in eosinophilic chronic rhinosinusitis with nasal polyps. Clin. Sci. (1979) 2019, 133, 2301–2315. [Google Scholar] [CrossRef]
- Zhang, F.; Xu, Z.; He, X.; Sun, Y.; Zhao, C.; Zhang, J. Increased B Cell-Activating Factor Expression Is Associated with Postoperative Recurrence of Chronic Rhinosinusitis with Nasal Polyps. Mediator. Inflamm. 2022, 2022, 7338692. [Google Scholar] [CrossRef] [PubMed]
- Brescia, G.; Sfriso, P.; Marioni, G. Role of blood inflammatory cells in chronic rhinosinusitis with nasal polyps. Acta Otolaryngol. 2019, 139, 48–51. [Google Scholar] [CrossRef] [PubMed]
- Bai, J.; Huang, J.H.; Price, C.P.E.; Schauer, J.M.; Suh, L.A.; Harmon, R.; Conley, D.B.; Welch, K.C.; Kern, R.C.; Shintani-Smith, S.; et al. Prognostic factors for polyp recurrence in chronic rhinosinusitis with nasal polyps. J. Allergy Clin. Immunol. 2022, 150, 352–361.e7. [Google Scholar] [CrossRef]
- Guo, M.; Alasousi, F.; Okpaleke, C.; Habib, A.R.; Javer, A. Prognosis of Chronic Rhinosinusitis with Nasal Polyps Using Preoperative Eosinophil/Basophil Levels and Treatment Compliance. Am. J. Rhinol. Allergy 2018, 32, 440–446. [Google Scholar] [CrossRef]
- Brescia, G.; Barion, U.; Zanotti, C.; Giacomelli, L.; Martini, A.; Marioni, G. The prognostic role of serum eosinophil and basophil levels in sinonasal polyposis. Int. Forum. Allergy Rhinol. 2017, 7, 261–267. [Google Scholar] [CrossRef]
- Hartnell, A.; Heinemann, A.; Conroy, D.M.; Wait, R.; Sturm, G.J.; Caversaccio, M.; Jose, P.J.; Williams, T.J. Identification of selective basophil chemoattractants in human nasal polyps as insulin-like growth factor-1 and insulin-like growth factor-2. J. Immunol. 2004, 173, 6448–6457. [Google Scholar] [CrossRef]
- Brescia, G.; Pedruzzi, B.; Barion, U.; Cinetto, F.; Giacomelli, L.; Martini, A.; Marioni, G. Are neutrophil-, eosinophil-, and basophil-to-lymphocyte ratios useful markers for pinpointing patients at higher risk of recurrent sinonasal polyps? Am. J. Otolaryngol. 2016, 37, 339–345. [Google Scholar] [CrossRef]
- Brescia, G.; Barion, U.; Zanotti, C.; Cinetto, F.; Giacomelli, L.; Martini, A.; Marioni, G. Blood eosinophil-to-basophil ratio in patients with sinonasal polyps: Does it have a clinical role? Ann. Allergy Asthma Immunol. 2017, 119, 223–226. [Google Scholar] [CrossRef]
- Horak, F.; Doberer, D.; Eber, E.; Horak, E.; Pohl, W.; Riedler, J.; Szépfalusi, Z.; Wantke, F.; Zacharasiewicz, A.; Studnicka, M. Diagnosis and management of asthma-Statement on the 2015 GINA Guidelines. Wien. Klin. Wochenschr. 2016, 128, 541–554. [Google Scholar] [CrossRef]
- Brescia, G.; Contro, G.; Ruaro, A.; Barion, U.; Frigo, A.C.; Sfriso, P.; Marioni, G. Sex and age-related differences in chronic rhinosinusitis with nasal polyps electing ESS. Am. J. Otolaryngol. 2022, 43, 103342. [Google Scholar] [CrossRef]
- Miyake, K.; Ito, J.; Karasuyama, H. Role of Basophils in a Broad Spectrum of Disorders. Front. Immunol. 2022, 13, 902494. [Google Scholar] [CrossRef]
- Karasuyama, H.; Shibata, S.; Yoshikawa, S.; Miyake, K. Basophils, a neglected minority in the immune system, have come into the limelight at last. Int. Immunol. 2021, 33, 809–813. [Google Scholar] [CrossRef] [PubMed]
- Karasuyama, H.; Mukai, K.; Obata, K.; Tsujimura, Y.; Wada, T. Nonredundant roles of basophils in immunity. Annu. Rev. Immunol. 2011, 29, 45–69. [Google Scholar] [CrossRef] [PubMed]
- Dennis, S.K.; Lam, K.; Luong, A. A review of classification schemes for chronic rhinosinusitis with nasal polyposis endotypes. Laryngoscope Investig. Otolaryngol. 2016, 1, 130–134. [Google Scholar] [CrossRef]
- Mahdavinia, M.; Carter, R.G.; Ocampo, C.J.; Stevens, W.; Kato, A.; Tan, B.K.; Kern, R.C.; Conley, D.B.; Chandra, R.; Hulse, K.E.; et al. Basophils are elevated in nasal polyps of patients with chronic rhinosinusitis without aspirin sensitivity. J. Allergy Clin. Immunol. 2014, 133, 1759–1763. [Google Scholar] [CrossRef]
- Peters, M.C.; Wenzel, S.E. Intersection of biology and therapeutics: Type 2 targeted therapeutics for adult asthma. Lancet 2020, 395, 371–383. [Google Scholar] [CrossRef]
- Brescia, G.; Contro, G.; Giacomelli, L.; Barion, U.; Frigo, A.C.; Marioni, G. Blood eosinophilic and basophilic trends in recurring and non-recurring eosinophilic rhinosinusitis with nasal polyps. Am. J. Rhinol. Allergy 2021, 35, 296–301. [Google Scholar] [CrossRef] [PubMed]
- Kagoya, R.; Kondo, K.; Baba, S.; Toma-Hirano, M.; Nishijima, H.; Suzukawa, K.; Kikuta, S.; Yamasoba, T. Correlation of basophil infiltration in nasal polyps with the severity of chronic rhinosinusitis. Ann. Allergy Asthma Immunol. 2015, 114, 30–35. [Google Scholar] [CrossRef]
- Li, Z.; Zeng, M.; Deng, Y.; Zhao, J.; Zhou, X.; Trudeau, J.B.; Goldschmidt, E.; Moore, J.A.; Chu, H.; Zhang, W.; et al. 15-Lipoxygenase 1 in nasal polyps promotes CCL26/eotaxin 3 expression through extracellular signal-regulated kinase activation. J. Allergy Clin. Immunol. 2019, 144, 1228–1241.e9. [Google Scholar] [CrossRef]
- Otsuka, A.; Kabashima, K. Contribution of basophils to cutaneous immune reactions and Th2-mediated allergic responses. Front. Immunol. 2015, 6, 393. [Google Scholar] [CrossRef] [PubMed]
- Das, M.; Stephen-Victor, E.; Bayry, J. Regulatory T cells do not suppress rather activate human basophils by IL-3 and STAT5-dependent mechanisms. Oncoimmunology 2020, 9, 1773193. [Google Scholar] [CrossRef] [PubMed]
- Ellis, A.K.; Tenn, M.W. Advances in rhinitis: Models and mechanisms. Ann. Allergy Asthma Immunol. 2018, 121, 61–64. [Google Scholar] [CrossRef]
- Stevens, W.W.; Schleimer, R.P. Aspirin-exacerbated respiratory disease as an endotype of chronic rhinosinusitis. Immunol. Allergy Clin. N. Am. 2016, 36, 669–680. [Google Scholar] [CrossRef] [PubMed]
- Sehanobish, E.; Asad, M.; Jerschow, E. New concepts for the pathogenesis and management of aspirin-exacerbated respiratory disease. Curr. Opin. Allergy Clin. Immunol. 2022, 22, 42–48. [Google Scholar] [CrossRef]
- Stevens, W.W.; Ocampo, C.J.; Berdnikovs, S.; Sakashita, M.; Mahdavinia, M.; Suh, L.; Takabayashi, T.; Norton, J.E.; Hulse, K.E.; Conley, D.B.; et al. Cytokines in Chronic Rhinosinusitis. Role in Eosinophilia and Aspirin-exacerbated Respiratory Disease. Am. J. Respir. Crit. Care Med. 2015, 192, 682–694. [Google Scholar] [CrossRef]
- Schleimer, R.P. Immunopathogenesis of Chronic Rhinosinusitis and Nasal Polyposis. Annu. Rev. Pathol. 2017, 12, 331–357. [Google Scholar] [CrossRef]
- Mitsui, C.; Kajiwara, K.; Ono, E.; Watai, K.; Hayashi, H.; Kamide, Y.; Fukutomi, Y.; Sekiya, K.; Tsuburai, T.; Yamamoto, K.; et al. Analysis of basophil activation in patients with aspirin-exacerbated respiratory disease. J. Allergy Clin. Immunol. 2017, 140, 1162–1164.e8. [Google Scholar] [CrossRef]
- Hamada, K.; Oishi, K.; Chikumoto, A.; Murakawa, K.; Ohteru, Y.; Matsuda, K.; Uehara, S.; Suetake, R.; Ohata, S.; Murata, Y.; et al. Impact of sinus surgery on type 2 airway and systemic inflammation in asthma. J. Asthma 2021, 58, 750–758. [Google Scholar] [CrossRef]
- Brescia, G.; Barion, U.; Zanotti, C.; Parrino, D.; Marioni, G. Pre-and postoperative blood neutrophil-to-lymphocyte and eosinophil-to-lymphocyte ratios in patients with sinonasal polyps: A preliminary investigation. Allergy Asthma Proc. 2017, 38, 64–69. [Google Scholar] [CrossRef]
- Otsuka, A.; Nonomura, Y.; Kabashima, K. Roles of basophils and mast cells in cutaneous inflammation. Semin. Immunopathol. 2016, 38, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Chu, H.H.; Kobayashi, Y.; Bui, D.V.; Yun, Y.; Nguyen, L.M.; Mitani, A.; Suzuki, K.; Asako, M.; Kanda, A.; Iwai, H. CCL4 Regulates Eosinophil Activation in Eosinophilic Airway Inflammation. Int. J. Mol. Sci. 2022, 23, 16149. [Google Scholar] [CrossRef] [PubMed]
- Brescia, G.; Alessandrini, L.; Zanotti, C.; Parrino, D.; Tealdo, G.; Torsello, M.; Zybine, V.; Giacomelli, L.; Barion, U.; Marioni, G. Histopathological and hematological changes in recurrent nasal polyposis. Int. Forum. Allergy Rhinol. 2019, 9, 813–820. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Recurrence | ||||
|---|---|---|---|---|
| No (N = 100) | Yes (N = 34) | p-Value | HR (95% CI) | |
| Group | ||||
| N missing | 0 | 0 | <0.0001 | |
| Control group | 81 (81.0%) | 14 (41.2%) | 1 | |
| AERD group | 19 (19.0%) | 20 (58.8%) | 5.473 (2.753; 10.881) | |
| Group | |||
|---|---|---|---|
| AERD (N = 39) | Control (N = 95) | p-Value | |
| Gender | |||
| N missing | 0 | 0 | 0.2976 |
| Male | 20 (51.3%) | 58 (61.1%) | |
| Female | 19 (48.7%) | 37 (38.9%) | |
| Age | |||
| N missing | 0 | 0 | |
| Median (range) | 50.0 (26.0–81.0) | 52.0 (24.0–80.0) | 0.6842 |
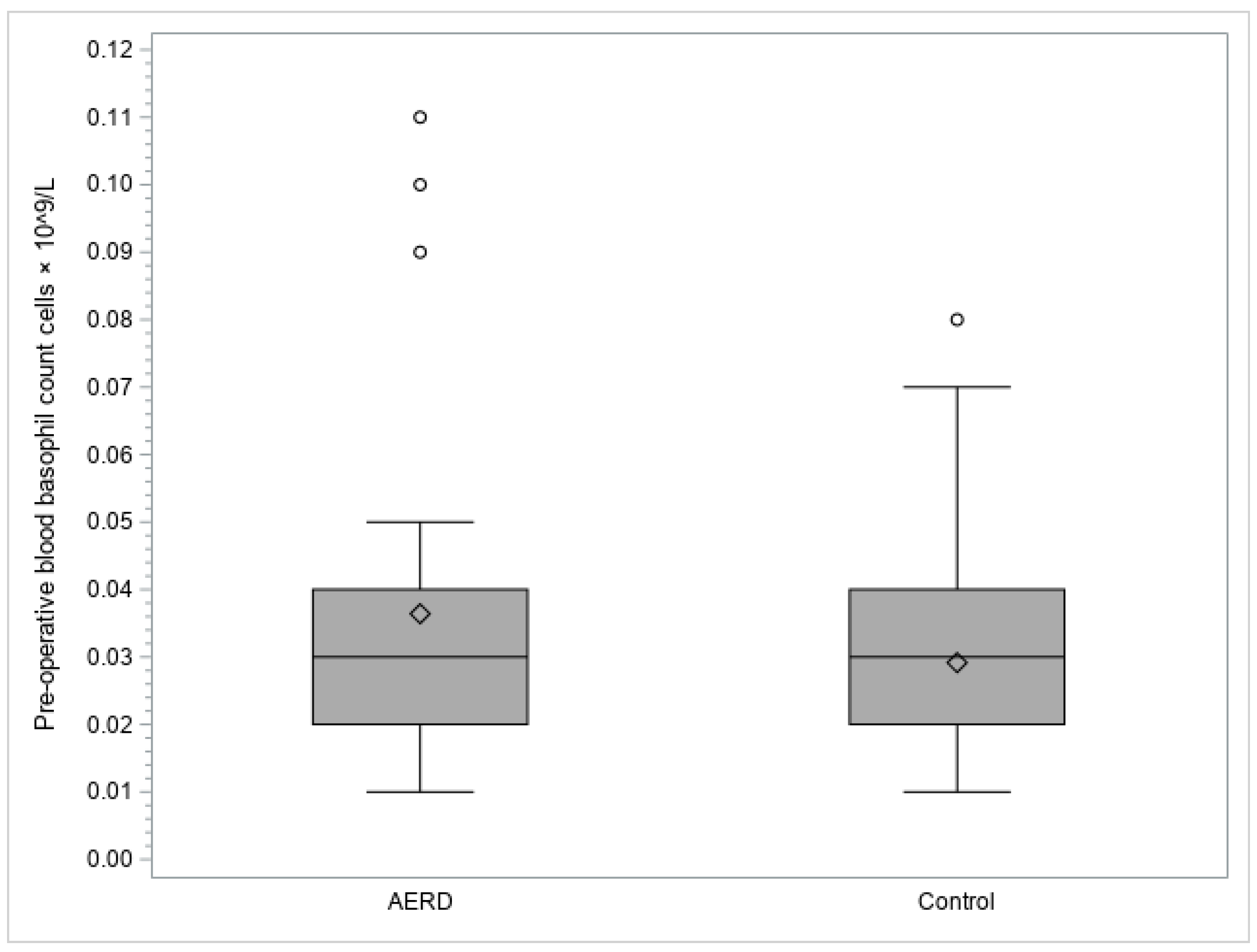
| Pre-operative blood basophil count (cells × 109/L) | |||
| N missing | 0 | 0 | |
| Median (range) | 0.03 (0.01–0.11) | 0.03 (0.01–0.08) | 0.0364 |
| Pre-operative blood basophils rate | |||
| N missing | 0 | 0 | |
| Median (range) | 0.50 (0.10–1.90) | 0.40 (0.10–1.50) | 0.0640 |
| Pre-operative basophils/lymphocytes ratio | |||
| N missing | 3 | 20 | |
| Median (range) | 0.02 (0.00–0.10) | 0.01 (0.00–0.07) | 0.1322 |
| Post-operative blood basophil count (cells × 109/L) | |||
| N missing | 15 | 0 | |
| Median (range) | 0.03 (0.00–0.40) | 0.03 (0.00–0.11) | 0.4931 |
| Post-operative blood basophils rate | |||
| N missing | 15 | 0 | |
| Median (range) | 0.40 (0.00–6.50) | 0.40 (0.00–1.90) | 0.4301 |
| Post-operative basophils/lymphocytes ratio | |||
| N missing | 19 | 20 | |
| Median (range) | 0.01 (0.01–0.39) | 0.01 (0.00–0.07) | 0.4061 |
| Pre-operative eosinophils/basophils ratio | |||
| N missing | 0 | 0 | |
| Median (range) | 11.75 (0.00–49.00) | 7.00 (0.57–29.00) | 0.0006 |
| Post-operative eosinophils/basophils ratio | |||
| N missing | 16 | 1 | |
| Median (range) | 8.20 (0.00–28.00) | 7.00 (0.50–316.67) | 0.6607 |
| Recurrence | ||||
|---|---|---|---|---|
| No (N = 19) | Yes (N = 20) | p-Value | HR (95% CI) | |
| Gender | ||||
| N missing | 00 (00.0%) | 00 (00.0%) | ||
| Male | 11 (57.9%) | 09 (45.0%) | 0.5093 | 1 |
| Female | 08 (42.1%) | 11 (55.0%) | 1.346 (0.557; 3.251) | |
| Age | ||||
| N missing | 0 | 0 | ||
| 0.2768 | 0.982 (0.950; 1.015) | |||
| Median (range) | 52.00 (39.00–81.00) | 47.50 (26.00–75.00) | ||
| Pre-operative blood basophil count (cells × 109/L) | ||||
| N missing | 19 (0) | 0 | ||
| 0.6817 | 39.568 (0.000; 1.7004 × 109) | |||
| Median (range) | 0.03 (0.01–0.10) | 0.04 (0.01–0.11) | ||
| Pre-operative blood basophils rate | ||||
| N missing | 0 | 0 | ||
| 0.6398 | 1.259 (0.480; 3.304) | |||
| Median (range) | 0.50 (0.10–1.50) | 0.55 (0.20–1.90) | ||
| Pre-operative basophils/lymphocytes ratio | ||||
| N missing | 2 | 1 | ||
| 0.6469 | 55.564 (0.000; 1.6246 × 109) | |||
| Median (range) | 0.02 (0.00–0.03) | 0.02 (0.00–0.10) | ||
| Post-operative blood basophil count (cells × 109/L) | ||||
| N missing | 7 | 8 | ||
| 0.8425 | 0.575 (0.002; 135.804) | |||
| Median (range) | 0.03 (0.00–0.20) | 0.03 (0.01–0.40) | ||
| Post-operative blood basophils rate | ||||
| N missing | 7 | 8 | ||
| 0.4250 | 1.137 (0.829; 1.561) | |||
| Median (range) | 0.45 (0.00–0.90) | 0.40 (0.10–6.50) | ||
| Post-operative basophils/lymphocytes ratio | ||||
| N missing | 10 | 9 | ||
| 0.9205 | 1.299 (0.008; 221.911) | |||
| Median (range) | 0.01 (0.01–0.03) | 0.02 (0.01–0.39) | ||
| Pre-operative eosinophils/basophils ratio | ||||
| N missing | 0 | 0 | ||
| 0.8419 | 0.996 (0.953; 1.040) | |||
| Median (range) | 12.75 (2.40–32.50) | 10.78 (0.00–49.00) | ||
| Post-operative eosinophils/basophils ratio | ||||
| N missing | 8 | 8 | ||
| 0.3505 | 0.967 (0.900; 1.038) | |||
| Median (range) | 8.20 (0.20–28.00) | 8.75 (0.00–18.00) | ||
| Recurrence | ||||
|---|---|---|---|---|
| No (N = 81) | Yes (N = 14) | p-Value | HR (95% CI) | |
| Gender | ||||
| N missing | 0 | 0 | ||
| Male | 47 (58.0%) | 11 (78.6%) | 1 | |
| Female | 34 (42.0%) | 03 (21.4%) | 0.1161 | 0.353 (0.097; 1.293) |
| Age | ||||
| N missing | 0 | 0 | ||
| 0.1445 | 0.973 (0.939; 1.009) | |||
| Median (range) | 55.00 (25.00–80.00) | 43.50 (24.00–75.00) | ||
| Pre-operative blood basophil count (cells × 109/L) | ||||
| N missing | 0 | 0 | ||
| 0.7505 | 84.067 (0.000; 6.133 × 1013) | |||
| Median (range) | 0.03 (0.01–0.08) | 0.02 (0.01–0.07) | ||
| Pre-operative blood basophils rate | ||||
| N missing | 0 | 0 | ||
| 0.8598 | 1.172 (0.201; 6.850) | |||
| Median (range) | 0.40 (0.10–1.50) | 0.30 (0.10–1.30) | ||
| Pre-operative basophils/lymphocytes ratio | ||||
| N missing | 19 | 1 | ||
| 0.7319 | 1620.023 (0.000; 3.696 × 1021) | |||
| Median (range) | 0.01 (0.00–0.07) | 0.02 (0.01–0.04) | ||
| Post-operative blood basophil count | ||||
| N missing | 0 | 0 | ||
| 0.6936 | 0.005 (0.000; 1.867 × 109) | |||
| Median (range) | 0.03 (0.00–0.11) | 0.03 (0.01–0.06) | ||
| Post-operative blood basophils rate (cells × 109/L) | ||||
| N missing | 0 | 0 | ||
| 0.6521 | 0.672 (0.119; 3.785) | |||
| Median (range) | 0.40 (0.00–1.90) | 0.40 (0.20–0.80) | ||
| Post-operative basophils/lymphocytes ratio | ||||
| N missing | 19 | 1 | ||
| 0.7757 | 0.002 (0.000; 1.229 × 1016) | |||
| Median (range) | 0.01 (0.00–0.07) | 0.02 (0.01–0.03) | ||
| Pre-operative eosinophils/basophils ratio | ||||
| N missing | 0 | 0 | ||
| 0.6218 | 1.021 (0.940; 1.108) | |||
| Median (range) | 7.00 (0.57–29.00) | 7.11 (1.00–23.00) | ||
| Post-operative eosinophils/basophils ratio | ||||
| N missing | 1 | 0 | ||
| 0.9939 | 1.000 (0.977; 1.023) | |||
| Median (range) | 6.71 (0.50–316.67) | 11.00 (0.50–21.50) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brescia, G.; Fabbris, C.; Calvanese, L.; Bandolin, L.; Pedruzzi, B.; Di Pasquale Fiasca, V.M.; Marciani, S.; Mularoni, F.; Degli Esposti Pallotti, F.; Negrisolo, M.; et al. Blood Basophils Relevance in Chronic Rhinosinusitis with Aspirin-Exacerbated Respiratory Disease. Diagnostics 2023, 13, 1920. https://doi.org/10.3390/diagnostics13111920
Brescia G, Fabbris C, Calvanese L, Bandolin L, Pedruzzi B, Di Pasquale Fiasca VM, Marciani S, Mularoni F, Degli Esposti Pallotti F, Negrisolo M, et al. Blood Basophils Relevance in Chronic Rhinosinusitis with Aspirin-Exacerbated Respiratory Disease. Diagnostics. 2023; 13(11):1920. https://doi.org/10.3390/diagnostics13111920
Chicago/Turabian StyleBrescia, Giuseppe, Cristoforo Fabbris, Leonardo Calvanese, Luigia Bandolin, Barbara Pedruzzi, Valerio Maria Di Pasquale Fiasca, Silvia Marciani, Francesca Mularoni, Fabio Degli Esposti Pallotti, Michael Negrisolo, and et al. 2023. "Blood Basophils Relevance in Chronic Rhinosinusitis with Aspirin-Exacerbated Respiratory Disease" Diagnostics 13, no. 11: 1920. https://doi.org/10.3390/diagnostics13111920