
Artificial Intelligence Applications in Cardiovascular Magnetic Resonance Imaging: Are We on the Path to Avoiding the Administration of Contrast Media?

 , ,
, ,  ,
, 

Abstract
:1. Introduction
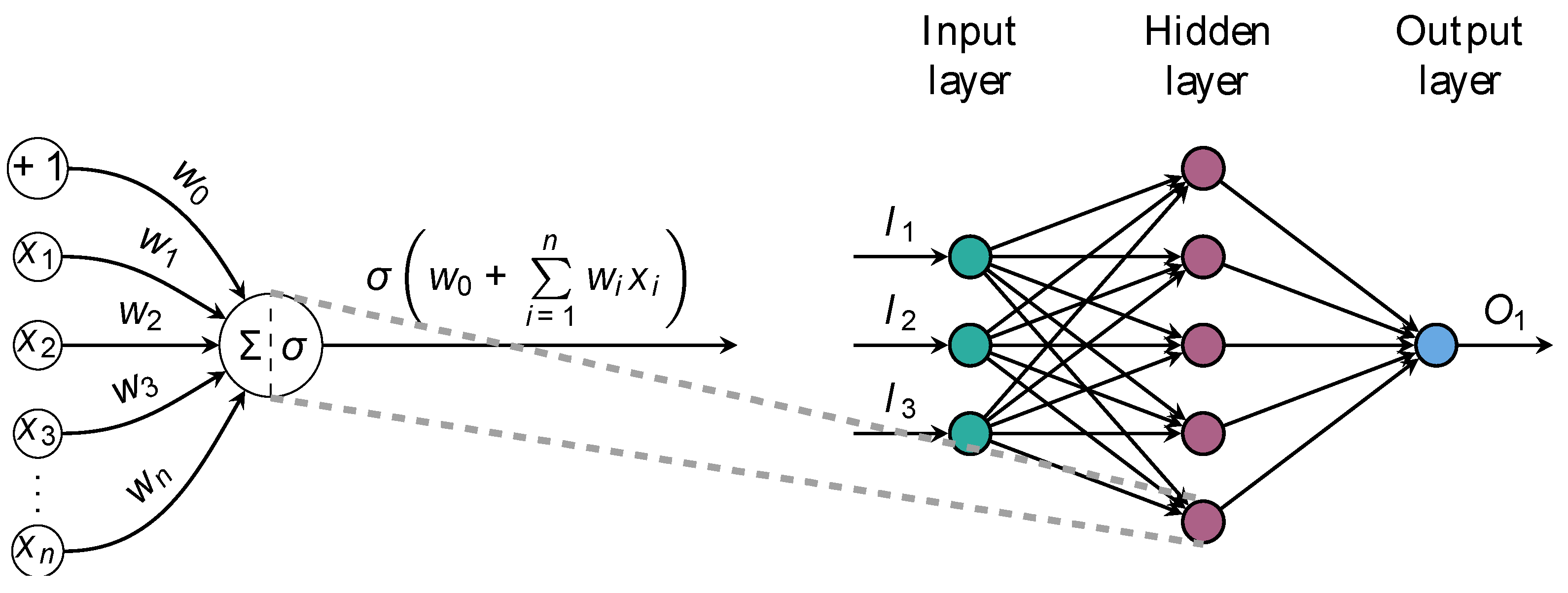
2. Concepts of AI
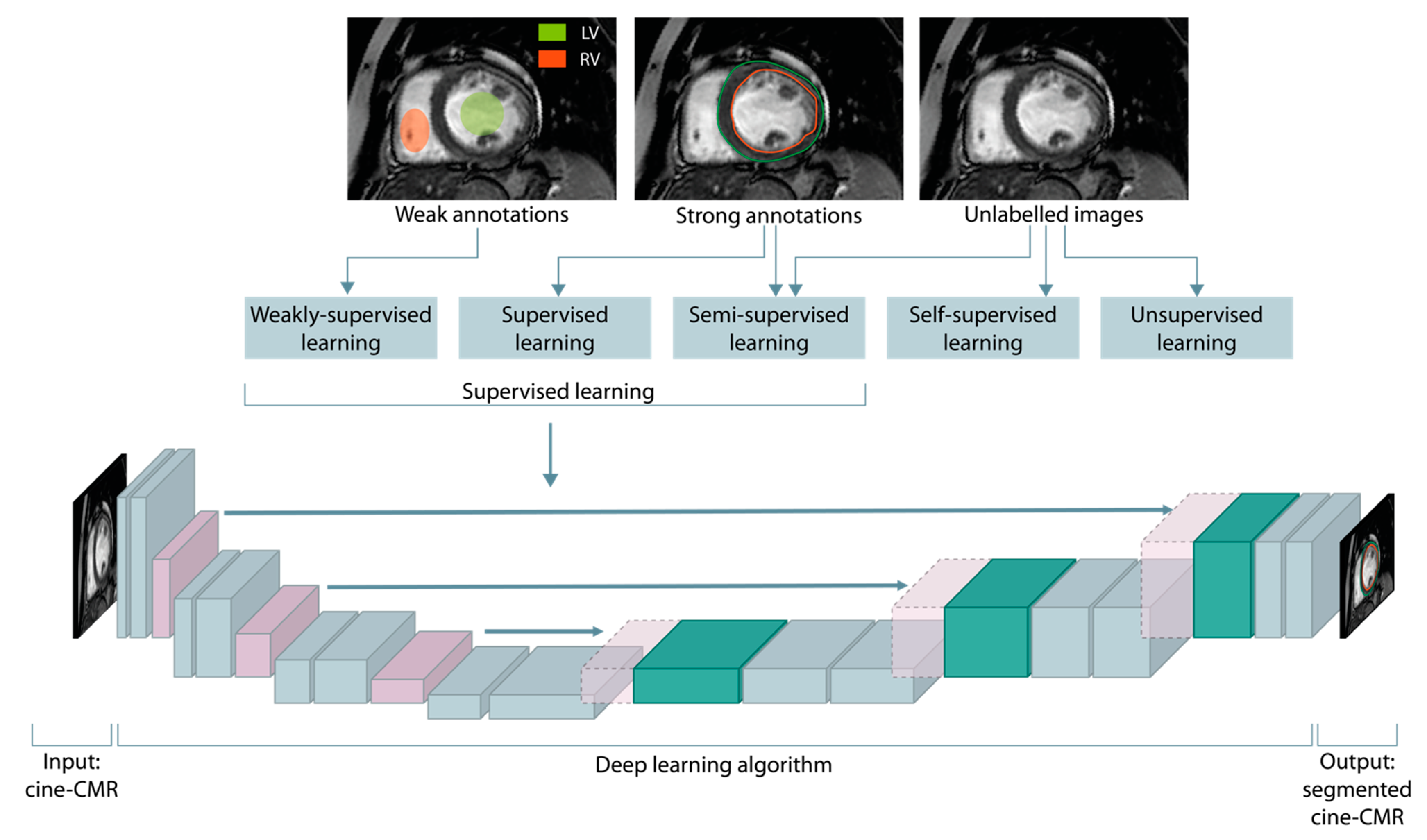
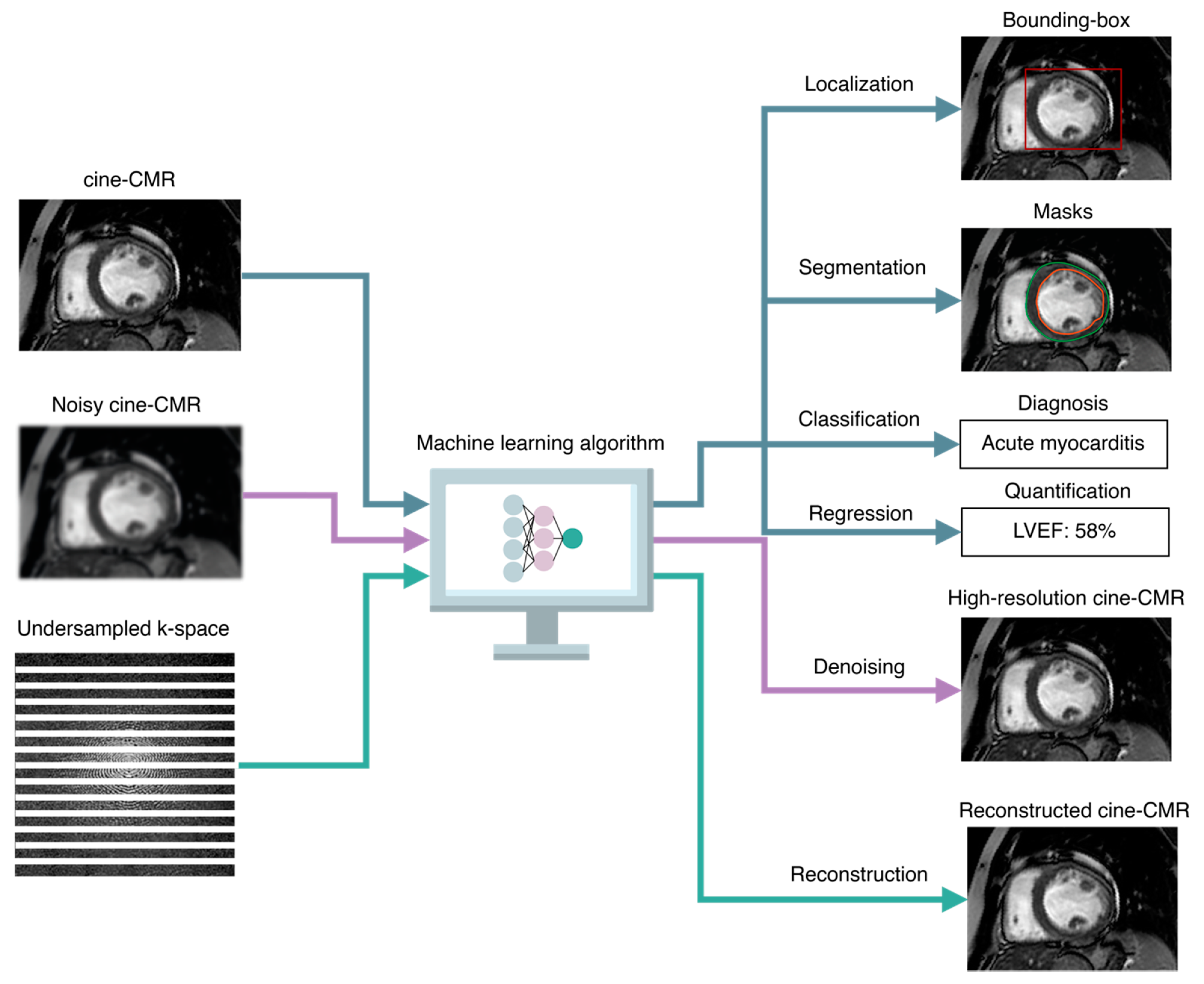
2.1. Taxonomy of ML Tasks
2.1.1. Supervised Learning
Taxonomy of Supervised Tasks
2.1.2. Unsupervised Learning
2.1.3. Hybrid Paradigms
2.2. Convolutional Neural Networks and the U-Net Architecture
2.3. AI-Based Diagnosis and Prognosis Prediction
3. AI Applications in Non-Contrast Cardiovascular Magnetic Resonance
3.1. Ischemic Cardiomyopathy
3.2. Non-Ischemic Cardiomyopathy
4. Current Limitations and Future Developments
4.1. Lack of Algorithms Transparency and Quality Control
4.2. Data Heterogeneity and Concerns with Validation and Testing
4.3. Ethical and Legal Issues
4.4. Future Development
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zeppenfeld, K.; Tfelt-Hansen, J.; de Riva, M.; Winkel, B.G.; Behr, E.R.; Blom, A.N.; Charron, P.; Corrado, D.; Dagres, N.; de Chillou, C.; et al. 2022 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: Developed by the task force for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur. Heart J. 2022, 43, 3997–4126. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contributio. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Cau, R.; Bassareo, P.P.; Mannelli, L.; Suri, J.S.; Saba, L. Imaging in COVID-19-related myocardial injury. Int. J. Cardiovasc. Imaging 2020, 37, 1349–1360. [Google Scholar] [CrossRef]
- Collet, J.-P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: The Task Force for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef]
- Matusik, P.S.; Bryll, A.; Matusik, P.T.; Popiela, T.J. Ischemic and non-ischemic patterns of late gadolinium enhancement in heart failure with reduced ejection fraction. Cardiol. J. 2021, 28, 67–76. [Google Scholar] [CrossRef] [Green Version]
- Vöhringer, M.; Mahrholdt, H.; Yilmaz, A.; Sechtem, U. Significance of late gadolinium enhancement in cardiovascular magnetic resonance imaging (CMR). Herz Kardiovaskuläre Erkrank. 2007, 32, 129–137. [Google Scholar] [CrossRef]
- Cau, R.; Muscogiuri, G.; Pisu, F.; Gatti, M.; Velthuis, B.; Loewe, C.; Cademartiri, F.; Pontone, G.; Montisci, R.; Guglielmo, M.; et al. Exploring the evolution in prognostic capability of multisequence cardiac magnetic resonance in patients affected by Takotsubo cardiomyopathy based on machine learning analysis design and rationale of the Evolution Study. J. Thorac. Imaging 2023, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Becker, M.A.; Cornel, J.H.; van de Ven, P.M.; van Rossum, A.C.; Allaart, C.P.; Germans, T. The prognostic value of late gadolinium-enhanced cardiac magnetic resonance imaging in nonischemic dilated cardiomyopathy: A Review and Meta-Analysis. JACC Cardiovasc. Imaging 2018, 11, 1274–1284. [Google Scholar] [CrossRef] [PubMed]
- Cau, R.; Solinas, C.; De Silva, P.; Lambertini, M.; Agostinetto, E.; Scartozzi, M.; Montisci, R.; Pontone, G.; Porcu, M.; Saba, L. Role of cardiac MRI in the diagnosis of immune checkpoint inhibitor-associated myocarditis. Int. J. Cancer 2022, 151, 1860–1873. [Google Scholar] [CrossRef]
- Kramer, C.M.; Barkhausen, J.; Flamm, S.D.; Kim, R.J.; Nagel, E. Standardized cardiovascular magnetic resonance (CMR) protocols 2013 update. J. Cardiovasc. Magn. Reson. 2013, 15, 91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kramer, C.M.; Barkhausen, J.; Bucciarelli-Ducci, C.; Flamm, S.D.; Kim, R.J.; Nagel, E. Standardized cardiovascular magnetic resonance imaging (CMR) protocols: 2020 update. J. Cardiovasc. Magn. Reson. 2020, 22, 17. [Google Scholar] [CrossRef] [PubMed]
- Cau, R.; Cherchi, V.; Micheletti, G.; Porcu, M.; Mannelli, L.; Bassareo, P.; Suri, J.S.; Saba, L. Potential role of artificial intelligence in cardiac magnetic resonance imaging. J. Thorac. Imaging 2021, 36, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Muscogiuri, G.; Volpato, V.; Cau, R.; Chiesa, M.; Saba, L.; Guglielmo, M.; Senatieri, A.; Chierchia, G.; Pontone, G.; Dell’aversana, S.; et al. Application of AI in cardiovascular multimodality imaging. Heliyon 2022, 8, e10872. [Google Scholar] [CrossRef] [PubMed]
- Petersen, S.E.; Abdulkareem, M.; Leiner, T. Artificial intelligence will transform cardiac imaging—Opportunities and challenges. Front. Cardiovasc. Med. 2019, 6, 133. [Google Scholar] [CrossRef]
- Dey, D.; Slomka, P.J.; Leeson, P.; Comaniciu, D.; Shrestha, S.; Sengupta, P.P.; Marwick, T.H. Artificial intelligence in cardiovascular imaging: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2019, 73, 1317–1335. [Google Scholar] [CrossRef]
- Cau, R.; Faa, G.; Nardi, V.; Balestrieri, A.; Puig, J.; Suri, J.S.; SanFilippo, R.; Saba, L. Long-COVID diagnosis: From diagnostic to advanced AI-driven models. Eur. J. Radiol. 2022, 148, 110164. [Google Scholar] [CrossRef]
- Richardson, M.L.; Garwood, E.R.; Lee, Y.; Li, M.D.; Lo, H.S.; Nagaraju, A.; Nguyen, X.V.; Probyn, L.; Rajiah, P.; Sin, J.; et al. Noninterpretive uses of artificial intelligence in radiology. Acad. Radiol. 2020, 28, 1225–1235. [Google Scholar] [CrossRef]
- Xu, B.; Kocyigit, D.; Grimm, R.; Griffin, B.P.; Cheng, F. Applications of artificial intelligence in multimodality cardiovascular imaging: A state-of-the-art review. Prog. Cardiovasc. Dis. 2020, 63, 367–376. [Google Scholar] [CrossRef]
- Cau, R.; Flanders, A.; Mannelli, L.; Politi, C.; Faa, G.; Suri, J.S.; Saba, L. Artificial intelligence in computed tomography plaque characterization: A review. Eur. J. Radiol. 2021, 140, 109767. [Google Scholar] [CrossRef]
- Siegersma, K.R.; Leiner, T.; Chew, D.P.; Appelman, Y.; Hofstra, L.; Verjans, J.W. Artificial intelligence in cardiovascular imaging: State of the art and implications for the imaging cardiologist. Neth. Heart J. 2019, 27, 403–413. [Google Scholar] [CrossRef] [Green Version]
- Pecoraro, M.; Messina, E.; Bicchetti, M.; Carnicelli, G.; Del Monte, M.; Iorio, B.; La Torre, G.; Catalano, C.; Panebianco, V. The future direction of imaging in prostate cancer: MRI with or without contrast injection. Andrology 2021, 9, 1429–1443. [Google Scholar] [CrossRef]
- Azarfar, G.; Ko, S.-B.; Adams, S.J.; Babyn, P.S. Applications of deep learning to reduce the need for iodinated contrast media for CT imaging: A systematic review. Int. J. Comput. Assist. Radiol. Surg. 2023. [Google Scholar] [CrossRef]
- Adamou, A.; Beltsios, E.T.; Bania, A.; Gkana, A.; Kastrup, A.; Chatziioannou, A.; Politi, M.; Papanagiotou, P. Artificial intelligence-driven ASPECTS for the detection of early stroke changes in non-contrast CT: A systematic review and meta-analysis. J. NeuroInterventional Surg. 2022. [Google Scholar] [CrossRef]
- Pasquini, L.; Napolitano, A.; Pignatelli, M.; Tagliente, E.; Parrillo, C.; Nasta, F.; Romano, A.; Bozzao, A.; Di Napoli, A. Synthetic Post-contrast imaging through artificial intelligence: Clinical applications of virtual and augmented contrast media. Pharmaceutics 2022, 14, 2378. [Google Scholar] [CrossRef] [PubMed]
- Mallio, C.A.; Radbruch, A.; Deike-Hofmann, K.; van der Molen, A.J.; Dekkers, I.A.; Zaharchuk, G.; Parizel, P.M.; Beomonte Zobel, B.; Quattrocchi, C.C. Artificial intelligence to reduce or eliminate the need for gadolinium-based contrast agents in brain and cardiac MRI: A literature review. Investig. Radiol. 2023. Available online: https://journals.lww.com/investigativeradiology/Fulltext/9900/Artificial_Intelligence_to_Reduce_or_Eliminate_the.114.aspx (accessed on 25 May 2023). [CrossRef]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef]
- Leiner, T.; Rueckert, D.; Suinesiaputra, A.; Baeßler, B.; Nezafat, R.; Išgum, I.; Young, A.A. Machine learning in cardiovascular magnetic resonance: Basic concepts and applications. J. Cardiovasc. Magn. Reson. 2019, 21, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oscanoa, J.A.; Middione, M.J.; Alkan, C.; Yurt, M.; Loecher, M.; Vasanawala, S.S.; Ennis, D.B. Deep learning-based reconstruction for cardiac MRI: A Review. Bioengineering 2023, 10, 334. [Google Scholar] [CrossRef] [PubMed]
- Ramachandram, D.; Taylor, G.W. Deep multimodal learning: A survey on recent advances and trends. IEEE Signal Process. Mag. 2017, 34, 96–108. [Google Scholar] [CrossRef]
- Anastasopoulos, C.; Yang, S.; Pradella, M.; D’antonoli, T.A.; Knecht, S.; Cyriac, J.; Reisert, M.; Kellner, E.; Achermann, R.; Haaf, P.; et al. Atri-U: Assisted image analysis in routine cardiovascular magnetic resonance volumetry of the left atrium. J. Cardiovasc. Magn. Reson. 2021, 23, 133. [Google Scholar] [CrossRef]
- Ronneberger, O.; Fischer, P.; Brox, T. U-Net: Convolutional Networks for Biomedical Image Segmentation BT–Medical Image Computing and Computer-Assisted Intervention–MICCAI 2015; Navab, N., Hornegger, J., Wells, W.M., Frangi, A.F., Eds.; Springer International Publishing: Berlin/Heidelberg, Germany, 2015; pp. 234–241. [Google Scholar]
- Van Smeden, M.; Reitsma, J.B.; Riley, R.D.; Collins, G.S.; Moons, K.G. Clinical prediction models: Diagnosis versus prognosis. J. Clin. Epidemiol. 2021, 132, 142–145. [Google Scholar] [CrossRef] [PubMed]
- Marcos-Garcés, V.; Perez, N.; Gavara, J.; Lopez-Lereu, M.P.; Monmeneu, J.V.; Rios-Navarro, C.; de Dios, E.; Merenciano-González, H.; Gabaldon-Pérez, A.; Cànoves, J.; et al. Risk score for early risk prediction by cardiac magnetic resonance after acute myocardial infarction. Int. J. Cardiol. 2021, 349, 150–154. [Google Scholar] [CrossRef] [PubMed]
- Isaak, A.; Bratz, J.; Kravchenko, D.; Mesropyan, N.; Eckardt, I.; Bischoff, L.M.; Weinhold, L.; Kuetting, D.; Pieper, C.C.; Attenberger, U.; et al. A novel and simple cardiac magnetic resonance score (PE2RT) predicts outcome in takotsubo syndrome. Eur. Radiol. 2023. [Google Scholar] [CrossRef]
- Pezel, T.; Sanguineti, F.; Garot, P.; Unterseeh, T.; Champagne, S.; Toupin, S.; Morisset, S.; Hovasse, T.; Faradji, A.; Ah-Sing, T.; et al. Machine-Learning Score Using Stress CMR for Death Prediction in Patients with Suspected or Known CAD. JACC Cardiovasc. Imaging 2022, 15, 1900–1913. [Google Scholar] [CrossRef]
- Eichhorn, C.; Greulich, S.; Bucciarelli-Ducci, C.; Sznitman, R.; Kwong, R.Y.; Gräni, C. Multiparametric cardiovascular magnetic resonance approach in diagnosing, monitoring, and prognostication of myocarditis. JACC Cardiovasc. Imaging 2022, 15, 1325–1338. [Google Scholar] [CrossRef]
- Kotanidis, C.P.; Bazmpani, M.-A.; Haidich, A.-B.; Karvounis, C.; Antoniades, C.; Karamitsos, T.D. Diagnostic accuracy of cardiovascular magnetic resonance in acute myocarditis: A systematic review and meta-Analysis. JACC Cardiovasc. Imaging 2018, 11, 1583–1590. [Google Scholar] [CrossRef]
- Shanbhag, S.M.; Greve, A.M.; Aspelund, T.; Schelbert, E.B.; Cao, J.J.; Danielsen, R.; Þorgeirsson, G.; Sigurðsson, S.; Eiríksdóttir, G.; Harris, T.B.; et al. Prevalence and prognosis of ischaemic and non-ischaemic myocardial fibrosis in older adults. Eur. Heart J. 2019, 40, 529–538. [Google Scholar] [CrossRef]
- Cau, R.; Bassareo, P.; Suri, J.S.; Pontone, G.; Saba, L. The emerging role of atrial strain assessed by cardiac MRI in different cardiovascular settings: An up-to-date review. Eur. Radiol. 2022, 32, 4384–4394. [Google Scholar] [CrossRef]
- Hor, K.N.; Taylor, M.D.; Al-Khalidi, H.R.; Cripe, L.H.; Raman, S.V.; Jefferies, J.L.; O’donnell, R.; Benson, D.W.; Mazur, W. Prevalence and distribution of late gadolinium enhancement in a large population of patients with Duchenne muscular dystrophy: Effect of age and left ventricular systolic function. Magn. Reson. 2013, 15, 107. [Google Scholar] [CrossRef] [Green Version]
- Aquaro, G.D.; Habtemicael, Y.G.; Camastra, G.; Monti, L.; Dellegrottaglie, S.; Moro, C.; Lanzillo, C.; Scatteia, A.; Di Roma, M.; Pontone, G.; et al. Prognostic value of repeating cardiac magnetic resonance in patients with acute myocarditis. J. Am. Coll. Cardiol. 2019, 74, 2439–2448. [Google Scholar] [CrossRef]
- Cau, R.; Bassareo, P.; Caredda, G.; Suri, J.S.; Esposito, A.; Saba, L. Atrial strain by feature-tracking cardiac magnetic resonance imaging in Takotsubo cardiomyopathy. Features, feasibility, and reproducibility. Can. Assoc. Radiol. J. 2021, 73, 573–580. [Google Scholar] [CrossRef] [PubMed]
- Peretto, G.; Sala, S.; Lazzeroni, D.; Palmisano, A.; Gigli, L.; Esposito, A.; De Cobelli, F.; Camici, P.G.; Mazzone, P.; Basso, C.; et al. Septal late gadolinium enhancement and arrhythmic risk in genetic and acquired non-ischaemic cardiomyopathies. Heart Lung Circ. 2020, 29, 1356–1365. [Google Scholar] [CrossRef] [PubMed]
- Souto, A.L.M.; Souto, R.M.; Teixeira, I.C.R.; Nacif, M.S. Myocardial viability on cardiac magnetic resonance. Arq. Bras. Cardiol. 2017, 108, 458–469. [Google Scholar] [CrossRef]
- Burrage, M.K.; Ferreira, V.M. Cardiovascular magnetic resonance for the differentiation of left ventricular hypertrophy. Curr. Heart Fail. Rep. 2020, 17, 192–204. [Google Scholar] [PubMed]
- Weng, Z.; Yao, J.; Chan, R.H.; He, J.; Yang, X.; Zhou, Y.; He, Y. Prognostic value of LGE-CMR in HCM: A meta-analysis. JACC Cardiovasc. Imaging 2016, 9, 1392–1402. [Google Scholar] [CrossRef]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Socie. Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [CrossRef] [Green Version]
- Naruse, Y.; Sato, A.; Kasahara, K.; Makino, K.; Sano, M.; Takeuchi, Y.; Nagasaka, S.; Wakabayashi, Y.; Katoh, H.; Satoh, H.; et al. The clinical impact of late gadolinium enhancement in Takotsubo cardiomyopathy: Serial analysis of cardiovascular magnetic resonance images. J. Cardiovasc. Magn. Reson. 2011, 13, 67. [Google Scholar] [CrossRef] [Green Version]
- Patel, A.R.; Kramer, C.M. Role of cardiac magnetic resonance in the diagnosis and prognosis of nonischemic cardiomyopathy. JACC Cardiovasc. Imaging 2017, 10, 1180–1193. [Google Scholar] [CrossRef]
- Kuruvilla, S.; Adenaw, N.; Katwal, A.B.; Lipinski, M.J.; Kramer, C.M.; Salerno, M. Late gadolinium enhancement on cardiac magnetic resonance predicts adverse cardiovascular outcomes in nonischemic cardiomyopathy. Circ. Cardiovasc. Imaging 2014, 7, 250–258. [Google Scholar] [CrossRef] [Green Version]
- Lee, E.; Ibrahim, E.-S.H.; Parwani, P.; Bhave, N.; Stojanovska, J. Practical guide to evaluating myocardial disease by cardiac MRI. Am. J. Roentgenol. 2020, 214, 546–556. [Google Scholar] [CrossRef]
- Weinreb, J.C.; Rodby, R.A.; Yee, J.; Wang, C.L.; Fine, D.; McDonald, R.J.; Perazella, M.A.; Dillman, J.R.; Davenport, M.S. Use of intravenous gadolinium-based contrast media in patients with kidney disease: Consensus Statements from the American College of Radiology an the National Kidney Foundation. Radiology 2020, 298, 28–35. [Google Scholar] [CrossRef]
- Ferreira, V.M.; Schulz-Menger, J.; Holmvang, G.; Kramer, C.M.; Carbone, I.; Sechtem, U.; Kindermann, I.; Gutberlet, M.; Cooper, L.T.; Liu, P.; et al. Cardiovascular magnetic resonance in nonischemic myocardial inflammation: Expert recommendations. J. Am. Coll. Cardiol. 2018, 72, 3158–3176. [Google Scholar] [CrossRef]
- Luetkens, J.A.; Faron, A.; Isaak, A.; Dabir, D.; Kuetting, D.; Feisst, A.; Schmeel, F.; Sprinkart, A.M.; Thomas, D. Comparison of original and 2018 Lake Louise Criteria for diagnosis of acute myocarditis: Results of a validation cohort. Radiol. Cardiothorac. Imaging 2019, 1, e190010. [Google Scholar] [CrossRef]
- Cau, R.; Bassareo, P.; Deidda, M.; Caredda, G.; Suri, J.S.; Pontone, G.; Saba, L. Could CMR tissue-tracking and parametric mapping distinguish between Takotsubo syndrome and acute myocarditis? A Pilot Study. Acad. Radiol. 2021, 29, S33–S39. Available online: http://www.sciencedirect.com/science/article/pii/S1076633221000155 (accessed on 25 May 2023). [CrossRef]
- Liu, X.; Hou, J.L.; Yang, Z.G.; Xia, C.C.; Xie, L.J.; Ye, P.F.; Peng, W.L.; Li, L.; Yang, M.X.; Guo, Y.K. Native T1 mapping for characterization of acute and chronic myocardial infarction in swine: Comparison with contrast-enhanced MRI. J. Magn. Reason. Imaging 2018, 47, 1406–1414. [Google Scholar] [CrossRef]
- Dastidar, A.G.; Harries, I.; Pontecorboli, G.; Bruno, V.D.; De Garate, E.; Moret, C.; Baritussio, A.; Johnson, T.W.; McAlindon, E.; Bucciarelli-Ducci, C. Native T1 mapping to detect extent of acute and chronic myocardial infarction: Comparison with late gadolinium enhancement technique. Int. J. Cardiovasc. Imaging 2019, 35, 517–527. [Google Scholar] [CrossRef] [Green Version]
- Popescu, I.A.; Werys, K.; Zhang, Q.; Puchta, H.; Hann, E.; Lukaschuk, E.; Ferreira, V.M.; Piechnik, S.K. Standardization of T1-mapping in cardiovascular magnetic resonance using clustered structuring for benchmarking normal ranges. Int. J. Cardiol. 2020, 326, 220–225. [Google Scholar] [CrossRef]
- Baessler, B.; Mannil, M.; Oebel, S.; Maintz, D.; Alkadhi, H.; Manka, R. Subacute and chronic left ventricular myocardial scar: Accuracy of texture analysis on nonenhanced cine MR images. Radiology 2018, 286, 103–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avard, E.; Shiri, I.; Hajianfar, G.; Abdollahi, H.; Kalantari, K.R.; Houshmand, G.; Kasani, K.; Bitarafan-Rajabi, A.; Deevband, M.R.; Oveisi, M.; et al. Non-contrast Cine Cardiac Magnetic Resonance image radiomics features and machine learning algorithms for myocardial infarction detection. Comput. Biol. Med. 2022, 141, 105145. [Google Scholar] [CrossRef] [PubMed]
- Larroza, A.; Materka, A.; López-Lereu, M.P.; Monmeneu, J.V.; Bodí, V.; Moratal, D. Differentiation between acute and chronic myocardial infarction by means of texture analysis of late gadolinium enhancement and cine cardiac magnetic resonance imaging. Eur. J. Radiol. 2017, 92, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Larroza, A.; López-Lereu, M.P.; Monmeneu, J.V.; Gavara, J.; Chorro, F.J.; Bodí, V.; Moratal, D. Texture analysis of cardiac cine magnetic resonance imaging to detect nonviable segments in patients with chronic myocardial infarction. Med. Phys. 2018, 45, 1471–1480. [Google Scholar] [CrossRef] [PubMed]
- Zhang, N.; Yang, G.; Gao, Z.; Xu, C.; Zhang, Y.; Shi, R.; Keegan, J.; Xu, L.; Zhang, H.; Fan, Z.; et al. Deep learning for diagnosis of chronic myocardial infarction on nonenhanced Cardiac Cine MRI. Radiology 2019, 291, 606–617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Q.; Burrage, M.K.; Shanmuganathan, M.; Gonzales, R.; Lukaschuk, E.; Thomas, K.E.; Mills, R.; Pelado, J.L.; Nikolaidou, C.; Popescu, I.A.; et al. Artificial intelligence for contrast-free MRI: Scar assessment in myocardial infarction using deep learning–based virtual native enhancement. Circulation 2022, 146, 1492–1503. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Shi, J.; Pommier, T.; Cottin, Y.; Salomon, M.; Decourselle, T.; Lalande, A.; Couturier, R. Prediction of myocardial infarction from patient features with machine learning. Front. Cardiovasc. Med. 2022, 9, 754609. [Google Scholar] [CrossRef] [PubMed]
- Goldfarb, J.W.; Craft, J.; Cao, J.J. Water-fat separation and parameter mapping in cardiac MRI via deep learning with a convolutional neural network. J. Magn. Reson. Imaging 2019, 50, 655–665. [Google Scholar] [CrossRef]
- Xu, C.; Xu, L.; Gao, Z.; Zhao, S.; Zhang, H.; Zhang, Y.; Du, X.; Zhao, S.; Ghista, D.; Liu, H.; et al. Direct delineation of myocardial infarction without contrast agents using a joint motion feature learning architecture. Med. Image Anal. 2018, 50, 82–94. [Google Scholar] [CrossRef]
- Xu, C.; Howey, J.; Ohorodnyk, P.; Roth, M.; Zhang, H.; Li, S. Segmentation and quantification of infarction without contrast agents via spatiotemporal generative adversarial learning. Med. Image Anal. 2020, 59, 101568. [Google Scholar] [CrossRef]
- Abdulkareem, M.; Kenawy, A.A.; Rauseo, E.; Lee, A.M.; Sojoudi, A.; Amir-Khalili, A.; Lekadir, K.; Young, A.A.; Barnes, M.R.; Barckow, P.; et al. Predicting post-contrast information from contrast agent free cardiac MRI using machine learning: Challenges and methods. Front. Cardiovasc. Med. 2022, 9, 894503. [Google Scholar] [CrossRef]
- Zhang, Q.; Burrage, M.K.; Lukaschuk, E.; Shanmuganathan, M.; Popescu, I.A.; Nikolaidou, C.; Mills, R.; Werys, K.; Hann, E.; Barutcu, A.; et al. Toward replacing late gadolinium enhancement with artificial intelligence virtual native enhancement for gadolinium-free cardiovascular magnetic resonance tissue characterization in hypertrophic cardiomyopathy. Circulation 2021, 144, 589–599. [Google Scholar] [CrossRef]
- Baeßler, B.; Mannil, M.; Maintz, D.; Alkadhi, H.; Manka, R. Texture analysis and machine learning of non-contrast T1-weighted MR images in patients with hypertrophic cardiomyopathy-Preliminary results. Eur. J. Radiol. 2018, 102, 61–67. [Google Scholar] [CrossRef]
- Fahmy, A.S.; Rausch, J.; Neisius, U.; Chan, R.H.; Maron, M.S.; Appelbaum, E.; Menze, B.; Nezafat, R. Automated Cardiac MR Scar Quantification in Hypertrophic Cardiomyopathy Using Deep Convolutional Neural Networks. JACC Cardiovasc. Imaging 2018, 1112, 1917–1918. [Google Scholar] [CrossRef] [PubMed]
- Cau, R.; Pisu, F.; Porcu, M.; Cademartiri, F.; Montisci, R.; Bassareo, P.; Muscogiuri, G.; Amadu, A.; Sironi, S.; Esposito, A.; et al. Machine learning approach in diagnosing Takotsubo cardiomyopathy: The role of the combined evaluation of atrial and ventricular strain, and parametric mapping. Int. J. Cardiol. 2022, 373, 124–133. [Google Scholar] [CrossRef] [PubMed]
- Eckstein, J.; Moghadasi, N.; Körperich, H.; Valdés, E.W.; Sciacca, V.; Paluszkiewicz, L.; Burchert, W.; Piran, M. A Machine learning challenge: Detection of cardiac amyloidosis based on bi-atrial and right ventricular strain and cardiac function. Diagnostics 2022, 12, 2693. [Google Scholar] [CrossRef]
- Krebs, J.; Mansi, T.; Delingette, H.; Bin Lou, B.; Lima, J.A.C.; Tao, S.; Ciuffo, L.A.; Norgard, S.; Butcher, B.; Lee, W.H.; et al. CinE cardiac magnetic resonance to predict ventricular arrhythmia (CERTAINTY). Sci. Rep. 2021, 11, 22683. [Google Scholar] [CrossRef] [PubMed]
- Leiner, T.; Bogaert, J.; Friedrich, M.G.; Mohiaddin, R.; Muthurangu, V.; Myerson, S.; Powell, A.J.; Raman, S.V.; Pennell, D.J. SCMR Position Paper (2020) on clinical indications for cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. 2020, 22, 76. [Google Scholar]
- Lee, S.-A.; Yoon, Y.E.; Kim, J.-E.; Park, J.J.; Oh, I.-Y.; Yoon, C.-H.; Suh, J.-W.; Kim, J.-S.; Chun, E.J.; Cho, Y.-S.; et al. Long-term prognostic value of late gadolinium-enhanced magnetic resonance imaging in patients with and without left ventricular dysfunction undergoing coronary artery bypass grafting. Am. J. Cardiol. 2016, 118, 1647–1654. [Google Scholar] [CrossRef] [PubMed]
- Garcia, M.J.; Kwong, R.Y.; Scherrer-Crosbie, M.; Taub, C.C.; Blankstein, R.; Lima, J.; Bonow, R.O.; Eshtehardi, P.; Bois, J.P. State of the Art: Imaging for myocardial viability: A Scientific Statement from the American Heart Association. Circ. Cardiovasc. Imaging. Circ. Cardiovasc. Imaging 2020, 13, e000053. [Google Scholar] [CrossRef]
- Löffler, A.I.; Kramer, C.M. Myocardial viability testing to guide coronary revascularization. Interv. Cardiol. Clin. 2018, 7, 355–365. [Google Scholar] [CrossRef]
- Antoniades, C.; Oikonomou, E.K. Artificial intelligence in cardiovascular imaging—Principles, expectations, and limitations. Eur. Heart J. 2021, ehab678. [Google Scholar] [CrossRef]
- Molinaro, A.M.; Simon, R.; Pfeiffer, R.M. Prediction error estimation: A comparison of resampling methods. Bioinformatics 2005, 21, 3301–3307. [Google Scholar] [CrossRef] [Green Version]
- Leighton, S.P.; Upthegrove, R.; Krishnadas, R.; Benros, E.M.; Broome, M.R.; Gkoutos, G.V.; Liddle, P.F.; Singh, S.P.; Everard, L.; Jones, P.B.; et al. Development and validation of multivariable prediction models of remission, recovery, and quality of life outcomes in people with first episode psychosis: A machine learning approach. Lancet Digit. Health 2019, 1, e261–e270. [Google Scholar] [CrossRef]
- Radanliev, P.; De Roure, D. Epistemological and Bibliometric Analysis of Ethics and Shared Responsibility—Health Policy and IoT Systems. Sustainability 2021, 13, 8533. [Google Scholar] [CrossRef]
- Murphy, K.; Di Ruggiero, E.; Upshur, R.; Willison, D.J.; Malhotra, N.; Cai, J.C.; Malhotra, N.; Lui, V.; Gibson, J. Artificial intelligence for good health: A scoping review of the ethics literature. BMC Med. Ethics. 2021, 22, 14. [Google Scholar] [CrossRef] [PubMed]
- Benjamens, S.; Dhunnoo, P.; Meskó, B. The state of artificial intelligence-based FDA-approved medical devices and algorithms: An online database. npj Digit. Med. 2020, 3, 118. [Google Scholar] [CrossRef]
- Allen, A.; Szabo, L.; Kaiser Health News. NIH “Very Concerned” about Serious Side Effect in Coronavirus Vaccine Trial [Internet]. Scientic American. 2020. Available online: https://www.scientificamerican.com/article/nih-very-concerned-about-serious-side-effect-in-c (accessed on 25 May 2023).
- Van Kolfschooten, H. EU regulation of artificial intelligence: Challenges for patients’ rights. Common Mark. Law Rev. 2022, 59, 81–112. [Google Scholar] [CrossRef]
- Dendumrongsup, T.; Plumb, A.A.; Halligan, S.; Fanshawe, T.R.; Altman, D.G.; Mallett, S. Multi-reader multi-case studies using the area under the receiver operator characteristic curve as a measure of diagnostic accuracy: Systematic review with a focus on quality of data reporting. PLoS ONE 2014, 9, e116018. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Authors | Years | Number of Patients | Variables | Results |
|---|---|---|---|---|
| Baessler et al. [59] | 2018 | 120 | Radiomics features of cine-CMR images | The model demonstrated an AUC of 0.93 and 0.092 to diagnose large and small myocardial infarction on cine-CMR. |
| Avard et al. [60] | 2022 | 72 | Radiomics features of cine-CMR images | The authors reported optimal performance for the logistic regression model with an AUC of 0.93 ± 0.03, an accuracy of 0.86 ± 0.05, a recall of 0.87 ± 0.1, a precision of 0.93 ± 0.03, an F1 Score = 0.90 ± 0.04, and for the support vector machine model with an AUC of 0.92 ± 0.05, an accuracy of 0.85 ± 0.04, a recall of 0.92 ± 0.01, a precision of 0.88 ± 0.04, and an F1 Score of 0.90 ± 0.02, respectively. |
| Larroza et al. [61] | 2017 | 44 | Radiomics features of cine-CMR images | Radiomics analysis of cine-CMR images achieved an AUC of 0.82 ± 0.06 with a sensitivity of 0.79 ± 0.10, and specificity of 0.80 ± 0.10 for differentiation of acute myocardial infarction from chronic myocardial infarction. |
| Larroza et al. [62] | 2018 | 50 | Radiomics features of cine-CMR images | The model demonstrated an AUC of 0.849, and a sensitivity of 92% to detect nonviable segments, 72% to detect viable segments, and 85% to detect remote segments. |
| Zhang et al. [63] | 2019 | 212 | Cine-CMR | The DL model showed a sensitivity of 89.8% and a specificity of 99.1%, with an AUC of 0.94. |
| Zhang et al. [64] | 2022 | 843 | Cine-CMR images, T1 mapping images | Virtual native enhancement demonstrated a strong correlation with LGE in quantifying scar size (R, 0.89; intraclass correlation coefficient, 0.94) and transmurality (R, 0.84; intraclass correlation coefficient, 0.90), achieving an accuracy of 84% for detecting scars with a specificity of 100% and sensitivity of 77%, and excellent visuospatial agreement with the histopathological porcine model. |
| Chen et al. [65] | 2022 | 150 | Physiological, clinical, and paraclinical features | The proposed model demonstrated a mean error of 0.056 and 0.012 for the quantification, and 88.67 and 77.33% for the classification accuracy of the state of the myocardium. |
| Goldfarb et al. [66] | 2019 | 90 | CMR water–fat separation and parametric mapping | The DL model could visualize myocardial fat deposition in chronic myocardial infarction and intramyocardial hemorrhage in acute myocardial infarction. |
| Xu et al. [67] | 2020 | 165 | Cine-CMR images | The proposed AI-based model achieved a pixel classification accuracy of 96.98%, and the mean absolute error of the infarction size was 17.15 mm2. |
| Xu et al. [68] | 2018 | 165 | Cine-CMR images | The proposed framework for the pixel-wise delineation of the myocardial infarction area achieved an accuracy of 95.03% and optimal consistency (Kappa statistic: 0.91; Dice: 89.87%) in comparison to the ground truths manually segmented LGE images. |
| Abdulkareem et al. [69] | 2022 | 272 | Cine-CMR images | The SVM model achieved accuracy, F1, and precision scores of 0.68, 0.69, and 0.64, respectively. Conversely, the DT models achieved accuracy, F1, and precision scores of 0.62, 0.63, and 0.72, respectively. |
| Zhang et al. [70] | 2021 | 1196 | Cine-CMR images, T1 mapping images | The authors reported high agreement between virtual native enhancement and LGE in the visuospatial distribution and quantification of lesions. |
| Baeßler et al. [71] | 2018 | 32 | Radiomics features of T1 mapping images | The proposed ML model achieved an AUC of 0.95 with a diagnostic sensitivity of 91% and a specificity of 93%. |
| Fahmy et al. [72] | 2022 | 759 | Radiomics features of cine-CMR | The DL model using radiomics data of cine-CMR images correctly identified 43% and 28% of HCM patients without scars in the internal and external datasets. |
| Cau et al. [73] | 2022 | 43 | CMR parameters, demographics data | The model showed a sensitivity of 92% (95% CI 78–100), specificity of 86% (95% CI 80–92), and AUC of 0.94 (95% CI 0.90–0.99) in diagnosing Takotsubo cardiomyopathy. |
| Eckstein et al. [74] | 2022 | 96 | CMR strain and function parameters | The supervised ML model demonstrated an accuracy of 90.9% (0.996; precision = 94%; sensitivity = 100%; F1 Score = 97%) to identify cardiac amiloidosis patients. |
| Krebs et al. [75] | 2021 | 350 | Cine-CMR images | The proposed score remained significantly associated with ventricular arrhythmia after adjustment in multivariable regression analysis. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cau, R.; Pisu, F.; Suri, J.S.; Mannelli, L.; Scaglione, M.; Masala, S.; Saba, L. Artificial Intelligence Applications in Cardiovascular Magnetic Resonance Imaging: Are We on the Path to Avoiding the Administration of Contrast Media? Diagnostics 2023, 13, 2061. https://doi.org/10.3390/diagnostics13122061
Cau R, Pisu F, Suri JS, Mannelli L, Scaglione M, Masala S, Saba L. Artificial Intelligence Applications in Cardiovascular Magnetic Resonance Imaging: Are We on the Path to Avoiding the Administration of Contrast Media? Diagnostics. 2023; 13(12):2061. https://doi.org/10.3390/diagnostics13122061
Chicago/Turabian StyleCau, Riccardo, Francesco Pisu, Jasjit S. Suri, Lorenzo Mannelli, Mariano Scaglione, Salvatore Masala, and Luca Saba. 2023. "Artificial Intelligence Applications in Cardiovascular Magnetic Resonance Imaging: Are We on the Path to Avoiding the Administration of Contrast Media?" Diagnostics 13, no. 12: 2061. https://doi.org/10.3390/diagnostics13122061
APA StyleCau, R., Pisu, F., Suri, J. S., Mannelli, L., Scaglione, M., Masala, S., & Saba, L. (2023). Artificial Intelligence Applications in Cardiovascular Magnetic Resonance Imaging: Are We on the Path to Avoiding the Administration of Contrast Media? Diagnostics, 13(12), 2061. https://doi.org/10.3390/diagnostics13122061