Abstract
Background and purpose: Dynamic 18F-FDG PET-CT scanning can accurately quantify 18F-FDG uptake and has been successfully applied in diagnosing and evaluating therapeutic effects in various malignant tumors. There is no conclusion as to whether it can accurately distinguish benign and malignant lymph nodes in nasopharyngeal cancer. The main purpose of this study is to reveal the diagnostic value of dynamic PET-CT in cervical lymph node metastasis of nasopharyngeal cancer through analysis. Method: We first searched for cervical lymph nodes interested in static PET-CT, measured their SUV-Max values, and found the corresponding lymph nodes in magnetic resonance images before and after treatment. The valid or invalid groups were included according to the changes in lymph node size before and after treatment. If the change in the product of the maximum diameter and maximum vertical transverse diameter of the lymph node before and after treatment was greater than or equal to 50%, they would be included in the valid group. If the change was less than 50%, they would be included in the invalid group. Their Ki values were measured on dynamic PET-CT and compared under different conditions. Then, we conducted a correlation analysis between various factors and Ki values. Finally, diagnostic tests were conducted to compare the sensitivity and specificity of Ki and SUV-Max. Result: We included 67 cervical lymph nodes from different regions of 51 nasopharyngeal cancer patients and divided them into valid and invalid groups based on changes before treatment. The valid group included 50 lymph nodes, while the invalid group included 17. There wer significant differences (p < 0.001) between the valid and the invalid groups in SUV-Max, Ki-Mean, and Ki-Max values. When the SUV-Max was ≤4.5, there was no significant difference in the Ki-Mean and Ki-Max between the two groups (p > 0.05). When the SUV-Max was ≤4.5 and pre-treatment lymph nodes were <1.0 cm, the valid group had significantly higher Ki-Mean (0.00910) and Ki-Maximum (0.01004) values than the invalid group (Ki-Mean = 0.00716, Ki-Max = 0.00767) (p < 0.05). When the SUV-Max was ≤4.5, the pre-treatment lymph nodes < 1.0 cm, and the EBV DNA replication normal, Ki-Mean (0.01060) and Ki-Max (0.01149) in the valid group were still significantly higher than the invalid group (Ki-Mean = 0.00670, Ki-Max = 0.00719) (p < 0.05). The correlation analysis between different factors (SUV-Max, T-stage, normal EB virus DNA replication, age, and pre-treatment lymph node < 1.0 cm) and the Ki value showed that SUV-Max and a pre-treatment lymph node < 1.0 cm were related to Ki-Mean and Ki-Max. Diagnostic testing was conducted; the AUC value of the SUV-Max value was 0.8259 (95% confidence interval: 0.7296–0.9222), the AUC value of the Ki-Mean was 0.8759 (95% confidence interval: 0.7950–0.9567), and the AUC value of the Ki-Max was 0.8859 (95% confidence interval: 0.8089–0.9629). After comparison, it was found that there was no significant difference in AUC values between Ki-Mean and SUV-Max (p = 0.220 > 0.05), and there was also no significant difference in AUC values between Ki max and SUV-Max (p = 0.159 > 0.05). By calculating the Youden index, we identified the optimal cut-off value. It was found that the sensitivity of SUV-Max was 100% and the specificity was 66%, the sensitivity of Ki-Mean was 100% and the specificity was 70%, and the sensitivity of Ki-Max was 100% and the specificity was 72%. After Chi-Square analysis, it was found that there was no significant difference in specificity between Ki-Mean and SUV-Max (p = 0.712), and there was also no significant difference in specificity between Ki-Max and SUV-Max (p = 0.755). Conclusion: Dynamic PET-CT has shown a significant diagnostic value in diagnosing cervical lymph node metastasis of nasopharyngeal cancer, especially for the small SUV value, and lymph nodes do not meet the metastasis criteria before treatment, and EBV DNA replication is normal. Although the diagnostic accuracy, sensitivity, and specificity of dynamic PET-CT were not significantly different from traditional static PET-CT, the dynamic PET-CT had a more accurate tendency.
1. Introduction
Nasopharyngeal cancer is a malignant tumor originating from nasopharyngeal mucosal epithelial cells. It is prevalent in southern China and Southeast Asia, and its incidence rate is 20–30/10,000/year [1]. Nasopharyngeal cancer has a hidden onset, and the early symptoms are not obvious. When apparent symptoms appear, it is already in the middle and late stages, and most patients only want to come to the hospital for the first time when they have touched the noticeable neck lumps [2]. It is essential to determine whether cervical lymph nodes are metastatic for nasopharyngeal cancer patients to clarify clinical staging, formulate treatment plans, and evaluate prognosis. Unlike other head and neck malignant tumors, nasopharyngeal cancer mainly adopts a comprehensive treatment plan based on radiation therapy, with local recurrence being the leading cause of treatment failure. Among them, 14–18% are cervical lymph node recurrence [3], mainly because the missed false negative lymph nodes were classified as low-dose areas during the planning process.
Previous studies have reported that 18F-fluorodeoxyglucose positron emission tomography-computed tomography (18F-FDG PET-CT) has shown significant functionality in detecting distant metastasis of nasopharyngeal cancer [4,5]. 18F-FDG PET-CT scanning is the most commonly used imaging method in clinical practice, which can reflect prognostic factors directly related to clinical outcomes, including maximum standardized uptake value (SUV-Max), metabolic tumor volume, and total lesion glycolysis [6]. 18FDG PET-CT combines the anatomical accuracy of CT and the details of PET molecular metabolism and has become an imaging method for molecular targets, providing an important basis for differential diagnosis and therapeutic evaluation of tumors [7]. However, static 18F-FDG PET-CT only displays the cumulative results after 60 min of tracer injection, ignoring the intermediate processes, including the transport of the tracer through blood flow, its exchange between blood vessels and tissues, and its binding and separation with the target [8]. SUV is an important diagnostic indicator for static PET imaging, a standard for given drug activity and weight, and a relative measurement value [9,10] and is influenced by many factors related to physical effects, hardware and software system specifications, tracer kinetics, motion, scanning protocol design, and limitations of current image derived PET indicators [11]. Meanwhile, the average SUV value changes due to voxel levels, making it sensitive to the definition of ROI (region of interest) and influenced by changes within and between observers [12]. Dynamic PET-CT scanning refers to starting data collection immediately after injection of a tracer, generating a time-activity-curve (TAC) based on the framing during the scanning process, and extracting parameters such as K1-K4, Ki, and glucose metabolism rate through dynamic modeling. It can avoid the influence of factors such as uptake kinetics, injection imaging time, and BMI, has better accuracy than SUVs, and can achieve a quantitative evaluation of tumor metabolism. In addition, dynamic studies have found that Ki can more sensitively identify early metastatic lymph nodes than SUVs [13]. For suspected metastases that SUVs cannot accurately identify, dynamic PET-CT scans can provide more information.
Recently, multiple studies have confirmed the important role of dynamic PET-CT in determining lymph node metastasis. Sun [14] et al. conducted a prospective cohort study on patients with non-small cell lung cancer and obtained some characteristic dynamic parameters such as V_Median, K3_Entropy, VB_Entropy, K1_Uniformity, and Ki_Uniformity. The results showed significant differences between benign and malignant lymph nodes, which were pathologically confirmed. The results showed significant differences in K3_Entropy, VB_Entropy, K1_Uniformity, and Ki_Uniformity. The Ki, VB, and K3 regression models could make good predictions for distinguishing between benign and malignant lymph nodes. Wumner [15] et al. analyzed 135 mediastinal and hilar lymph nodes from 29 lung cancer patients and confirmed pathologically that 49 were non-metastatic and 86 were metastatic. All patients completed dynamic PET-CT and obtained characteristic parameters. In addition to K3, dynamic metabolic parameters K1, K2, Ki, and Ki/K1 also performed well in the differential diagnosis of metastatic and non-metastatic lymph nodes (p < 0.05). However, the predictive role of dynamic PET-CT in cervical lymph node metastasis of nasopharyngeal carcinoma has not been reported.
Therefore, the primary purpose of this study is to clarify whether the Ki value in dynamic PET-CT can replace the SUV value in distinguishing cervical lymph node metastasis of nasopharyngeal cancer, which can be used as a reference for radiation oncologists when delineating the target area, and can improve tumor control rate, reduce recurrence rate, and obtain better efficacy and prognosis in clinical treatment.
2. Material and Method
2.1. Patients
A retrospective analysis was conducted on 51 newly diagnosed nasopharyngeal cancer patients who visited our department from 2020 to 2022. After the precise diagnosis, all patients received systematic treatment (radiotherapy, chemotherapy, or other anti-tumor treatments). All patients met the following criteria: (1) The pathological diagnosis was confirmed as nasopharyngeal cancer after the nasal endoscopic biopsy or multiple nasal endoscopic examinations could not diagnose nasopharyngeal cancer, but cervical lymph node biopsy was confirmed as metastatic squamous cell carcinoma and considered as the nasopharyngeal source, and there is evidence of nasopharyngeal malignancy on imaging. (2) No anti-tumor treatment was initiated before the PET-CT examination. (3) Before and after treatment, magnetic resonance imaging of the head and neck was performed, and there were measurable target lesions. (4) No other malignant tumors were present. (5) There was no severe cardio-cerebrovascular disease or diabetes, or mental disease.
2.2. Data Acquisition and Image Reconstruction
The patients fasted for at least 6 h before the examination, and their blood sugar was controlled at the normal level before the examination. Then, a uMI780 PET/CT scanner (Shanghai United Imaging Company, Shanghai, China) was used for scanning. Each patient underwent the low-dose transmission CT scan of the whole body, with a tube voltage of 120 KV and a tube current of 180 mA. The focus was on observing primary nasopharyngeal tumors and cervical lymph nodes. Then, immediately after injection of 18F-FDG (3.7 MBq/kg), a 60 min single bed dynamic PET image was collected, and an 18 × 5 s, 6 × 10 s, 5 × 30 s, 5 × 60 s, 8 × 150 s, 6 × 300 s frame protocol was divided into 48 image data [13]. Then, we used four beds (2 min each) for routine static whole-body PET scans and used the ordered subset expectation maximization (OSEM) iterative algorithm (parameter: 2 subsets, 20 iterations, 150 × 150 matrices) and reconstructed all dynamic PET data. Similarly, conventional static SUV images were reconstructed using the OSEM method (parameters: 2 subsets, 20 iterations, 128 × 128 matrices). All data were corrected according to isotope decay, scattering events, and random coincidence, and semi-maximum smoothing was performed using a standard Gaussian filter with a total width of 3 mm.
Our research used internally developed computer code for indirect parameter reconstruction processing [16,17]. Assuming irreversible uptake of 18F-FDG, the physiological parameters of voxel levels were estimated using the ordinary least squares (OLS) Patlak reconstruction regression method for 48 dynamic PET series based on a dual tissue compartment dynamics model [18]. We estimated the tracer concentration Cp(t) in the bleeding plasma and the tracer concentration C(t) in the tissue from the PET-CT images. In this study, we defined the input function Cp(t), derived non-invasively from dynamic PET data as the active concentration of the tracer in plasma. Specifically, VOI was drawn on the aortic arch of each patient, and then input functions derived from arterial images were extracted from all dynamic PET sequences. Then, by applying the OLS linear regression method to the following Patlak equation, the tracer uptake rate Ki at the voxel level could be calculated [18,19,20,21]. The specific block diagram was shown in Figure 1, and its equation was as follows: Ki-Mean was defined as the average Ki value at which the tracer was uptaken, and Ki-Max was the Ki value at which the uptake rate reached the highest value.
where t was the time when the vascular space and reversible tissue compartment reached relative equilibrium and Ki and V were the slopes and intercepts of linear regression, respectively.
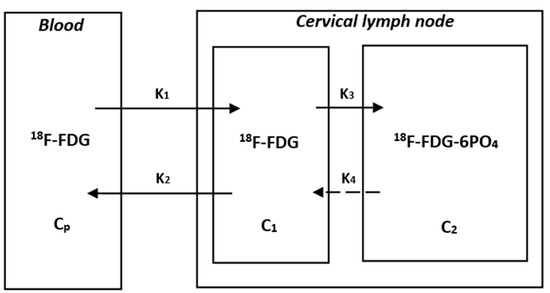
Figure 1.
The Patlak model of 18F-FDG catabolism. CP is the active concentration of 18F-FDG in plasma, while C1 and C2 are the concentrations of 18F-FDG-6PO4 in cervical lymph nodes. K1, K2, K3, and K4 are rate constants. K1 is the rate constant of blood to the cervical lymph node. K2 is the rate constant of the cervical lymph node to blood. K3 is the rate constant of 18F-FDG to 18F-FDG-6PO4. K4 is the rate constant of 18F-FDG-6PO4 to 18F-FDG. Due to the assumption of a unidirectional uptake of 18F-FDG in the Patlak analysis, the rate constant of 18F-FDG-6PO4 to 18F-FDG is negligible. The slope (Ki) and intercept (V) can be obtained from the graphical analysis and equation, where the slope Ki is equal to K1K3/(K2 + K3).
2.3. Delineation of VOIs
The delineation of VOIs (volumes of interest) mainly included cervical lymph nodes. Two experienced radiology doctors (Yang and Jiang) initially determined whether it was metastasis or reactive hyperplasia based on different lymph nodes’ size, shape, and SUV values in static PET-CT images and then measured the maximum SUV value (SUV-Max) of these suspicious lymph nodes and incorporated them into the following dynamic PET-CT image reconstruction software for analysis. Subsequently, the specific size changes of these lymph nodes before and after treatment were analyzed through comparison in magnetic resonance images, and data were recorded. The delineation of VOIs was performed by two radiation oncologists (Li and Xu). The Ki values of these lymph nodes were measured using Carisma software (version 2.0), which was used for comprehensive analysis with SUV values and changes in size before and after treatment.
2.4. Efficacy Evaluation
Due to the inability to perform needle biopsies on all cervical lymph nodes of all patients, we performed needle biopsies to determine the benign and malignant nature of cervical lymph nodes only when the patient had the following conditions, such as patients had obvious cervical masses, suspected metastatic lymph nodes on imaging, or multiple biopsies from the nasopharynx could not determine the diagnosis. Only a few patients underwent needle biopsies of cervical lymph nodes. For most patients, we mainly identified the possibility of malignancy through changes in size on MRI before and after treatment. According to the World Health Organization (WHO) efficacy evaluation criteria, clinical efficacy was evaluated [22]. Based on the definitions of partial remission (PR) and complete remission (CR), we considered these two situations more likely for the lymph node to be malignant. That is to say, we supposed that the product value of the lymph node’s maximum diameter and maximum vertical transverse diameter changed more than or equal to 50% before and after treatment. In that case, treatment was considered valid, indicating a tendency towards malignancy. Treatment was considered invalid if it was less than 50%, indicating a greater likelihood of benign.
2.5. Data Analysis
Two radiation oncologists (Li and Xu) accurately recorded all data, performed the normality distribution test on all data, and used Pearson or Spearman tests to analyze the correlation between different factors and Ki values based on the normal distribution. For sensitivity and specificity detection of diagnosis, we drew ROC curves, calculated the area under the curve, and found the optimal cutoff point. If the data followed the normal distribution, the t-test was used to analyze the Ki values under different conditions (SUV-Max value, lymph node size before and after treatment, and EB virus DNA expression). Conversely, the Mann–Whitney U test was used, and all tests were bilateral tests, with the p-value < 0.05 indicating meaningful results. All statistical analyses were plotted and analyzed using GraphPad PRISM version 9.0 and SPSS software version 27.0.
3. Result
3.1. Patients
Ultimately, we screened 51 patients with confirmed pathological diagnoses of nasopharyngeal cancer, including 36 male and 15 female patients. All patients received comprehensive treatment, such as radiotherapy and chemotherapy. All patients underwent MRI examinations before and after treatment, and some patients underwent cervical lymph node biopsy before treatment, and their benign or malignant nature was consistent with the degree of change in the MRI before and after treatment. The clinical characteristics of these 51 patients are shown in Table 1. The median age of all patients was 48 years (range: 26–63). In TNM staging, there were 7 patients with T1, 9 with T2, 28 with T3, and 7 with T4. There were 21 patients with stage N1, 27 with stage N2, and 3 with stage N3. There were 3 patients with stage M0, 44 with stage M0, and 4 with stage M1. Among all clinical stages, there were no patients belonging to stage I, while there were 8 patients in stage II, 27 in stage III, and 42 in stage IV. One patient had the TNM stage of T3N1Mx, and it was impossible to determine whether the clinical stage was stage III or IV. Therefore, the patient was included in the unclear staging group. After grouping based on the expression of EBV-DNA, it was found that 23 patients had higher than normal expression levels, while 28 patients had normal expression levels.

Table 1.
The characteristics of NPC patients.
3.2. Comparison of SUVmax, Ki-Mean, and Ki-Max Values between the Valid and Invalid Groups
We identified 67 cervical lymph nodes from different regions from the PET CT images of the 51 patients, measured their static SUV-Max values and dynamic Ki-Mean and Ki-Max values, and combined them with magnetic resonance images before and after treatment to determine their size changes. Finally, they were included in the valid and invalid groups based on the degree of change. After the normal distribution test, it was found that the data did not conform to the normal distribution, so the Mann–Whitney U test was used for all comparative analyses.
From Table 2 and Figure 2, it could be seen that the average SUV-Max value of the valid group was 7.2, the average Ki-Mean was 0.01323, and the average Ki-Max was 0.01510, which were significantly higher than the invalid group (SUV-Max = 4.3, Ki-Mean = 0.00978, and Ki-Max value = 0.01077, p < 0.001) (Table 2 and Figure 1).
Table 2.
Comparison of SUV-Max, Ki-Mean, and Ki-Max between the valid and invalid groups.
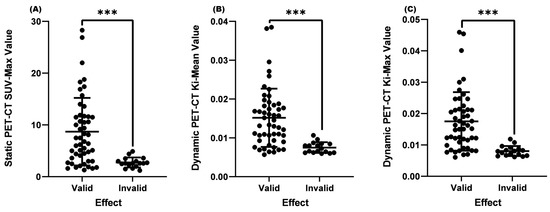
Figure 2.
Comparison of SUV-Max, Ki-Mean, and Ki-Max between the valid and invalid groups. (A) Comparison of SUV-Max between the valid and invalid groups (p < 0.001). (B) Comparison of the Ki-Mean between the valid and invalid groups (p < 0.001). (C) Comparison of the valid Ki-Max between the valid and invalid groups (p < 0.001). *** means p < 0.001.
3.3. Comparison of Ki-Mean and Ki-Max Values between Valid and Invalid Groups When SUV-Max ≤ 4.5
Matsubara [23] found in their study that when the SUV-Max of cervical lymph nodes was greater than 4.5, it was confirmed by biopsy pathology as metastatic lymph nodes. However, for lymph nodes with an SUV-Max less than or equal to 4.5, it was difficult to distinguish whether they were malignant or benign. Based on the results of this study, we set the case where the SUV-Max was less than or equal to 4.5 in this study. The results showed that there was no significant difference between the Ki-Mean (p = 0.151 > 0.05) and Ki-Max (p = 0.075 > 0.05) between the two groups (Table 3 and Figure 3).
Table 3.
Comparison of Ki-Mean and Ki-Max values between valid and invalid groups when the SUV-Max was ≤4.5.
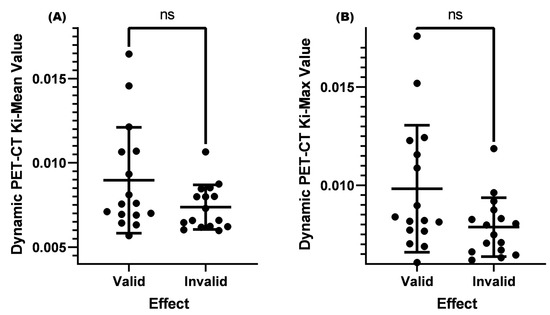
Figure 3.
Comparison of Ki-Mean and Ki-Max values between valid and invalid groups when the SUV-Max was ≤4.5. (A) Comparison of the Ki-Mean between the valid and invalid groups when the SUV-Max was ≤4.5 (p = 0.151 > 0.05). (B) Comparison of the Ki-Max between the valid and invalid groups when the SUV-Max was ≤4.5 (p = 0.075 > 0.05). ns means not significant.
3.4. Comparison of Ki-Mean and Ki-Max between the Valid and Invalid Groups with an SUV-Max ≤ 4.5 and Lymph Nodes < 1.0 cm before Treatment
The current guidelines and consensus often use a cervical lymph node short longitude ≥ 1.0 cm as a standard for lymph node metastasis, and it is necessary to combine the shape, density, number, and other factors of lymph nodes to assist in diagnosis and treatment [24]. The role of dynamic PET-CT in distinguishing benign and malignant cervical lymph nodes is not yet clear when the cervical lymph node is <1.0 cm. In this study, two conditions were set: (1) SUV-Max was less than or equal to 4.5, (2) cervical lymph node size was <1.0 cm. After analysis, it was found that the Ki-Mean (0.00910) and Ki-Max (0.01004) of the valid group were both higher than those of the invalid group (Ki-Mean = 0.00716 and Ki-Max = 0.00767, p < 0.05) (Table 4 and Figure 4).
Table 4.
Comparison of Ki-Mean and Ki-Max values between the valid and invalid groups with an SUV-Max ≤ 4.5 and a lymph node < 1.0 cm before treatment.
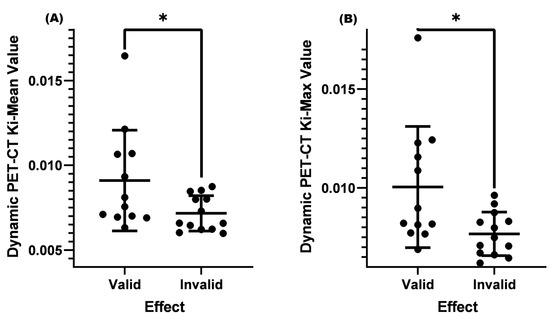
Figure 4.
Comparison of Ki-Mean and Ki-Max values between the valid and invalid groups with an SUV-Max ≤ 4.5 and a lymph node < 1.0 cm before treatment. (A) Comparison of Ki-Mean between the valid and invalid groups when the SUV-Max was ≤4.5 and the cervical lymph node < 1.0 cm before treatment (p = 0.0457 < 0.05). (B) Comparison of Ki-Max between the valid and invalid groups when the SUV was ≤4.5 and the cervical lymph node < 1.0 cm before treatment (p = 0.0298 < 0.05). * means p < 0.05.
We selected two patients who underwent dynamic and static PET/CT scans and cervical lymph node biopsies before treatment and completed MRI examinations before and after treatment. The relevant results were shown in Figure 5. These two patients’ cervical lymph nodes were <1.0 cm in size before treatment, and both showed low metabolism (SUV-Max = 1.6) on static PET-CT. Without biopsies, their benign and malignant status could not be determined, and from the results in Figure 4, one of the individuals had a positive cervical lymph node biopsy result. From the MRI images before and after treatment, there was a significant change in the size of the cervical lymph node (>50%). The Ki-Mean was 0.01065, the Ki-Max was 0.01156, and the metabolism was elevated in dynamic PET CT images. On the contrary, the biopsy result of another patient was negative, and there was almost no change in the cervical lymph node before and after treatment. The Ki-Mean was 0.00658, the Ki-Max was 0.00749, and the metabolism was not obvious in dynamic PET-CT images. The Ki values of the malignant lymph node were significantly greater than that of the benign lymph node. This result indirectly indicated that dynamic PET-CT could be the best choice for low SUV values and sizes < 1.0 cm, which could not determine the nature of cervical lymph nodes.
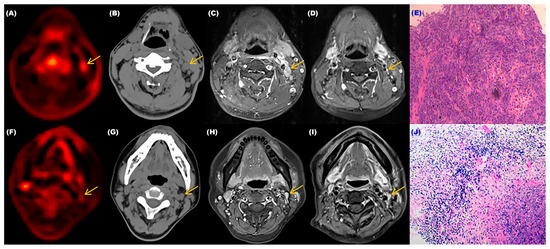
Figure 5.
The relevant examination results of two patients with different cervical lymph nodes. (A) Dynamic PET-CT image of the patient with the malignant cervical lymph node. (B) CT image of the patient with the malignant cervical lymph node. (C,D) MRI images of the patient with the malignant cervical lymph node before and after treatment. (E) Pathological image of the patient’s lymph node which was confirmed as malignant. (F) Dynamic PET-CT image of the patient with the benign cervical lymph node. (G) CT image of the patient with the benign cervical lymph node. (H,I) MRI images of the patient with the benign cervical lymph node before and after treatment. (J) Pathological image of the patient’s lymph node that was confirmed as benign.
3.5. Comparison of Ki-Mean and Ki-Max between the Valid and Invalid Groups with an SUV-Max ≤ 4.5 and a Lymph Node < 1.0 cm and a Normal EBV-DNA Replication before Treatment
Epstein–Barr virus DNA (EBV-DNA) is often used as an important indicator for efficacy monitoring [25,26], tumor recurrence [27], and lymph node metastasis [28] in clinical diagnosis and treatment. If the EBV-DNA level continues to rise, it often indicates a poor prognosis and the possibility of cervical lymph node metastasis. We continued to add EBV-DNA conditions based on an SUV-Max less than or equal to 4.5 and a cervical lymph node less than 1.0 cm before treatment. When EBV-DNA replication was at the normal level, the Ki-Mean (0.01060) and Ki-Max (0.01149) of the valid group were both more significant than those of the invalid group (Ki-Mean = 0.00670 and Ki-Max = 0.00719, p < 0.01) (Table 5 and Figure 6).
Table 5.
Comparison of Ki-Mean and Ki-Max values between the valid and invalid groups with an SUV-Max ≤ 4.5 and a lymph node < 1.0 cm and a normal EBV-DNA replication before treatment.
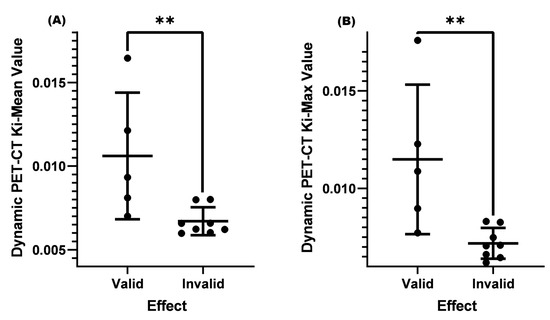
Figure 6.
Comparison of Ki-Mean and Ki-Max values between the valid and invalid groups with an SUV-Max ≤ 4.5 and a lymph node < 1.0 cm and a normal EBV-DNA replication before treatment. (A) Comparison of Ki-Mean between the valid and invalid groups when the SUV-Max was ≤4.5 and the cervical lymph node was <1.0 cm and there was the normal EBV-DNA replication before treatment (p = 0.0062 < 0.01). (B) Comparison of Ki-Max between the valid and invalid groups when the SUV-Max was ≤4.5 and the cervical lymph node was <1.0 cm and there was the normal EBV-DNA replication before treatment (p = 0.0062 < 0.01). ** means p < 0.01.
3.6. The Correlation between Different Factors and Ki-Mean and Ki-Max
We conducted a correlation study to explore the correlation between different factors (SUV-Max, T-stage, normal EBV-DNA replication, age, and a cervical lymph node < 1.0 cm) and Ki-Mean and Ki-Max values. Because the data did not conform to the normal distribution, we used the Spearman test to determine correlations. The results showed the correlation between SUV-Max and a cervical lymph node < 1.0 cm and Ki-Mean and Ki-Max (p < 0.0001). The r coefficient of the SUV Max and Ki-Mean was 0.8450, and the r coefficient of the Ki-Max was 0.8498. There were significant positive correlations (Table 6 and Figure 7).
Table 6.
Correlation between different factors and Ki-Mean values and Ki-Max.
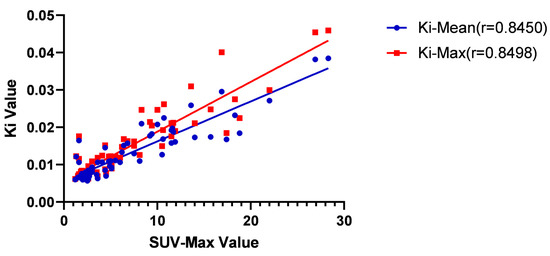
Figure 7.
Correlation between SUV-Max and Ki-Mean values and Ki-Max. The r coefficient of the SUV Max and Ki-Mean was 0.8450 (p < 0.01), and the r coefficient of the Ki-Max was 0.8498 (p < 0.01).
3.7. Diagnostic Accuracy of SUV-Max and Ki for Cervical Lymph Node Metastasis in Nasopharyngeal Cancer
We plotted ROC curves to evaluate the diagnostic accuracy of SUV-Max and Ki for cervical lymph node metastasis. The AUC value of the SUV-Max value was 0.8259 (95% confidence interval: 0.7296–0.9222), the AUC value of the Ki-Mean was 0.8759 (95% confidence interval: 0.7950–0.9567), and the AUC value of the Ki-Max was 0.8859 (95% confidence interval: 0.8089–0.9629). After comparison, it was found that there was no significant difference in AUC values between Ki-Mean and SUV-Max (p = 0.220 > 0.05), and there was also no significant difference in AUC values between Ki-Max and SUV-Max (p = 0.159 > 0.05). To calculate the sensitivity and specificity of each index, we first calculated Youden’s index. The calculation formula was: Youden’s index = Sensitivity + Specificity − 1. When Youden’s index was the largest, its cut-off value was the best [29]. After calculation, the sensitivity of SUV-Max was 100% and the specificity was 66%. The sensitivity of the Ki-Mean was 100% and the specificity was 70%; the sensitivity of the Ki-Max was 100% and the specificity was 72%. After Chi-Square analysis, it was found that there was no significant difference in specificity between Ki-Mean and SUV-Max (p = 0.712), and there was also no significant difference in specificity between Ki-Max and SUV-Max (p = 0.755) (Figure 8).
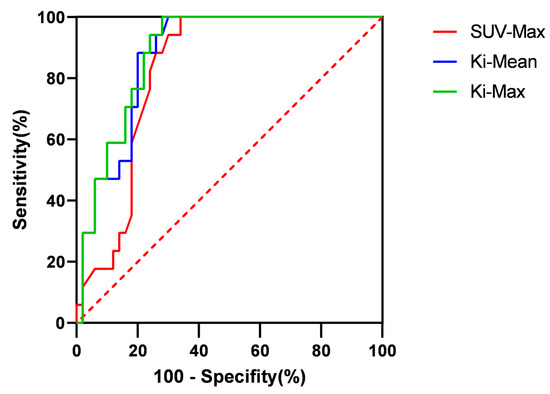
Figure 8.
The ROC curves of SUV-Max, Ki-Mean, and Ki-Max.
4. Discussion
In the first diagnosis, 70~80% of nasopharyngeal cancer patients have enlarged cervical lymph nodes [30]. The location of metastatic lymph nodes is related to the lymphatic drainage area of the primary tumor. The cervical lymph node metastasis of nasopharyngeal cancer mainly occurs bilaterally, commonly around the jugular vein chain. Currently, the treatment of nasopharyngeal cancer mainly relies on radiation therapy as a comprehensive treatment. With the development of radiation therapy technology, although intensity-modulated radiation therapy (IMRT) can provide excellent dose coverage for tumors, better protect surrounding normal tissues, improve local control, and long-term survival [31,32], 7% to 18% of patients still have residual or recurrent cervical lymph nodes after the first round of radiation therapy [33,34]. Therefore, determining whether neck lymph nodes are metastatic is crucial for accurate staging, selection of treatment plans, delineation of radiotherapy targets, and evaluation of the prognosis of nasopharyngeal cancer.
PET imaging for cancer metabolic assessment has been widely used in clinical medicine. The commonly used method is to evaluate the energy consumption of tumors by injecting 18F-fluorodeoxyglucose and detecting the maximum glucose metabolism (SUV-Max) [35]. However, many factors, such as uptake kinetics, body mass index, or post-injection time, can affect the results of SUV values [36]. As a new imaging technology in nuclear medicine, dynamic PET-CT images collect continuous frames through long-term scanning compared with static PET-CT images. Therefore, the degree of drug metabolism and histopathological activity is dynamically reflected [35]. The diagnostic value of dynamic PET-CT has been supported by data in non-small cell lung cancer and primary tumors of nasopharyngeal cancer [13,37], but there is no research report on whether it can differentiate cervical lymph node metastasis in nasopharyngeal cancer.
In our study, we first searched for cervical lymph nodes of interest on PET-CT images and then found the corresponding lymph nodes on magnetic resonance images. Then, according to the latest version of WHO solid tumor evaluation standards, we measured the maximum diameters and maximum vertical transverse diameters of lymph nodes before and after treatment and calculated the product size of the two. If the change before and after treatment exceeded 50%, it was included in the valid group; if it was less than 50%, it was included in the invalid group. Due to the inability to perform a needle biopsy on each cervical lymph node to determine its nature, we could only speculate on its potential for malignancy based on changes before and after treatment. It would likely be malignant if the change was greater than 50%. If the change was less than 50%, it was considered more likely to be benign. Through analysis, we found that the SUV-Max, Ki-Mean, and Ki-Max of the valid group were significantly higher than those of the invalid group (p < 0.001). This result might indicate that glucose metabolism’s degree and metabolic rate in general metastatic lymph nodes are significantly higher than in benign lymph nodes.
Previous studies have shown that when the SUV value of the lymph node is greater than 4.5, pathological biopsy confirms it as metastasis. However, for SUV values ≤ 4.5, it is difficult to distinguish between benign and malignant [23,38]. Given this result, we also set the same conditions in this study and found no significant difference in the Ki-Mean and Ki-Max between the two groups (p > 0.05). However, it could be seen from the results that the p-value of the Ki-Max was very close to 0.05. Due to the small sample size of this study, no positive results were obtained. Increasing the sample size further might result in better research results. According to the current results, when the SUV-Max was ≤4.5, the Ki-Mean and Ki-Max could not effectively distinguish between metastatic or benign lymph nodes.
The lymph node size is often an important indicator for diagnosing metastasis. In clinical practice, a cervical lymph node size ≥ 1.0 cm is an important criterion for cervical lymph node metastasis. For lymph nodes < 1.0 cm, it is often necessary to consider specific situations, such as whether there is central necrosis, cluster distribution, obvious enhancement, and so on. In our study, it was found that when the SUV-Max was ≤4.5, and the cervical lymph node < 1.0 cm before treatment, it could be seen that the Ki-Mean and Ki-Max of the valid group were greater than those of the invalid group (p < 0.05). The average Ki-Mean and Ki-Max values of the valid group were 0.00910 and 0.01004, and both were close to 0.01. This result indicates that dynamic PET-CT can often distinguish between benign and malignant lymph nodes when the SUV-Max is small and the cervical lymph node size does not meet the standards.
Epstein–Barr (EB) is the γ herpesvirus [39] and is closely related to the occurrence and development of nasopharyngeal cancer. In recent years, research has found that EB virus DNA (EBV-DNA) plays an important role in the efficacy monitoring and prognosis evaluation of nasopharyngeal cancer patients, especially in the clinical significance of changes in EBV-DNA concentration before and after treatment for distant metastasis and local recurrence in nasopharyngeal cancer patients [40]. Current research shows a positive correlation between EBV-DNA content in the blood of nasopharyngeal cancer patients and the volume of cervical lymph node metastasis [41], and EBV is closely associated with lymph node metastasis in nasopharyngeal cancer [28]. To further explore whether dynamic PET-CT can identify cervical lymph node metastasis when the level of EBV-DNA replication was normal, we analyzed it. The results showed that when the SUV-Max was ≤4.5, the pre-treatment lymph node < 1.0 cm, and EBV-DNA replication was normal the Ki-Mean and Ki-Max in the valid group were significantly higher than those in the invalid group (p < 0.05). Moreover, the valid group’s Ki-Mean and Ki-Max were greater than 0.01. Dynamic PET-CT can identify metastatic cervical lymph nodes when the EBV-DNA replication is normal, meanwhile, the SUV-Max is small and the lymph nodes do not meet the standards.
Many factors, such as age, T-stage, and SUV-Max, are related to parameters in dynamic PET-CT. Through analysis, it was found that SUV-Max and pre-treatment lymph nodes < 1.0 cm were associated with Ki-Mean and Ki-Max. A strong linear correlation existed between SUV-Max and Ki-Mean and Ki-Max. After further diagnostic testing, it was found that the AUC value of both the Ki-Mean and Ki-Max were greater than those of the SUV-Max. Generally speaking, the larger the AUC value, the higher its diagnostic or exclusion value [42]. However, in our study, it was found that there was no significant difference in AUC values between Ki-Mean and SUV-Max (p = 0.220 > 0.05), and there was also no significant difference in AUC values between Ki-Max and SUV-Max (p = 0.159 > 0.05). In terms of sensitivity, the sensitivity of SUV-Max, Ki-Mean, and Ki-Max could all reach 100%. However, regarding specificity, there was no significant difference between Ki-Mean and Ki-Max compared to SUV-Max (p > 0.05). The above results may indicate that dynamic PET-CT has the more accurate tendency, and due to sample size limitations, no positive conclusion has been drawn. This positive conclusion may be confirmed in large sample data in the future.
Some issues need to be addressed in our research. (1) We could only speculate on the possibility of cervical lymph node metastasis based on the changes in MRI before and after treatment, without pathological results to support it. There might be misdiagnoses and errors in the conclusions. (2) Some studies yielded nearly positive results, but a positive conclusion could not be reached due to insufficient sample size and could only be treated as negative. (3) In our study, some nasopharyngeal cancer patients only received partial treatment, and the follow-up time after treatment was insufficient. Some cervical lymph nodes might not have shown significant changes and had been included in the invalid group. (4) The sample difference between the valid and invalid groups was large, and the data did not conform to the normal distribution, affecting the results’ authenticity.
5. Conclusions
Compared with traditional static PET-CT, dynamic PET-CT has shown advantages in the diagnosis of cervical metastasis of nasopharyngeal cancer, especially for the cervical lymph nodes with small SUV values on static PET-CT, the lymph nodes’ size does not meet the criteria for judging metastasis, and the patient’s serum EBV-DNA replication before treatment is normal. Although our diagnostic test did not yield positive results, it could be seen from this result that dynamic PET-CT has the more accurate tendency. In the future, we need to combine pathology further and increase the sample size to verify everything based on this study.
Author Contributions
Methodology, G.L.; Software, S.Y.; Validation, S.W.; Formal analysis, G.L.; Data curation, R.J.; Writing—original draft, G.L.; Writing—review & editing, G.L.; Visualization, X.X.; Supervision, X.X.; Project administration, X.X. All authors contributed equally to the work. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of The Fifth Affiliated Hospital of Sun Yat-sen University (protocol code: K68-1 and date of approval: 24 September 2020).
Informed Consent Statement
Informed consents were obtained from all subjects involved in the study. Written informed consents have been obtained from the patients to publish this paper.
Data Availability Statement
All data have been included in this article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Chen, Y.-P.; Chan, A.T.C.; Le, Q.-T.; Blanchard, P.; Sun, Y.; Ma, J. Nasopharyngeal carcinoma. Lancet 2019, 394, 64–80. [Google Scholar] [CrossRef] [PubMed]
- Ho, F.C.; Tham, I.W.; Earnest, A.; Lee, K.M.; Lu, J.J. Patterns of regional lymph node metastasis of nasopharyngeal carcinoma: A meta-analysis of clinical evidence. BMC Cancer 2012, 12, 98. [Google Scholar] [CrossRef]
- Wei, W.I.; Chan, J.Y.W.; Ng, R.W.M.; Ho, W.K. Surgical salvage of persistent or recurrent nasopharyngeal carcinoma with maxillary swing approach—Critical appraisal after 2 decades. Head Neck 2011, 33, 969–975. [Google Scholar] [CrossRef]
- Liu, F.-Y.; Lin, C.-Y.; Chang, J.T.; Ng, S.-H.; Chin, S.-C.; Wang, H.-M.; Liao, C.-T.; Chan, S.-C.; Yen, T.-C. 18F-FDG PET Can Replace Conventional Work-up in Primary M Staging of Nonkeratinizing Nasopharyngeal Carcinoma. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2007, 48, 1614–1619. [Google Scholar] [CrossRef] [PubMed]
- Tang, L.-Q.; Chen, Q.-Y.; Fan, W.; Liu, H.; Zhang, L.; Guo, L.; Luo, D.-H.; Huang, P.-Y.; Zhang, X.; Lin, X.-P.; et al. Prospective Study of Tailoring Whole-Body Dual-Modality [18F]Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography With Plasma Epstein-Barr Virus DNA for Detecting Distant Metastasis in Endemic Nasopharyngeal Carcinoma at Initial Staging. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2013, 31, 2861–2869. [Google Scholar] [CrossRef]
- De Jaeghere, E.A.; Laloo, F.; Lippens, L.; Van Bockstal, M.; De Man, K.; Naert, E.; Van Dorpe, J.; Van de Vijver, K.; Tummers, P.; Makar, A.; et al. Splenic 18F-FDG uptake on baseline PET/CT is associated with oncological outcomes and tumor immune state in uterine cervical cancer. Gynecol. Oncol. 2020, 159, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Furlow, B. PET-CT Cancer Imaging. Radiol. Technol. 2018, 90, 149CT–170CT. [Google Scholar]
- Yang, D.M.; Palma, D.; Louie, A.; Malthaner, R.; Fortin, D.; Rodrigues, G.; Yaremko, B.; Laba, J.; Gaede, S.; Warner, A.; et al. Assessment of tumor response after stereotactic ablative radiation therapy for lung cancer: A prospective quantitative hybrid (18) F-fluorodeoxyglucose-positron emission tomography and CT perfusion study. J. Med. Imaging Radiat. Oncol. 2019, 63, 94–101. [Google Scholar] [CrossRef]
- Devriese, J.; Beels, L.; Maes, A.; Van De Wiele, C.; Gheysens, O.; Pottel, H. Review of clinically accessible methods to determine lean body mass for normalization of standardized uptake values. Q. J. Nucl. Med. Mol. Imaging 2016, 60, 1–11. [Google Scholar]
- Wang, Z.; Wu, Y.; Li, X.; Bai, Y.; Chen, H.; Ding, J.; Shen, C.; Hu, Z.; Liang, D.; Liu, X.; et al. Comparison between a dual-time-window protocol and other simplified protocols for dynamic total-body 18F-FDG PET imaging. EJNMMI Phys. 2022, 9, 63. [Google Scholar] [CrossRef]
- Zaidi, H.; Karakatsanis, N. Towards enhanced PET quantification in clinical oncology. Br. J. Radiol. 2018, 91, 20170508. [Google Scholar] [CrossRef] [PubMed]
- Adams, M.C.; Turkington, T.G.; Wilson, J.M.; Wong, T.Z. A Systematic Review of the Factors Affecting Accuracy of SUV Measurements. AJR Am. J. Roentgenol. 2010, 195, 310–320. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Lin, Z.; Xu, Z.; Li, D.; Lv, W.; Yang, S.; Liu, Y.; Cao, Y.; Cao, Q.; Jin, H. Influx rate constant of 18F-FDG increases in metastatic lymph nodes of non-small cell lung cancer patients. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 1198–1208. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Xiao, L.; Wang, Y.; Liu, C.; Cao, L.; Zhai, W.; Wang, B.; Yu, S.; Xin, J. Diagnostic value of dynamic 18F-FDG PET/CT imaging in non-small cell lung cancer and FDG hypermetabolic lymph nodes. Quant. Imaging Med. Surg. 2023, 13, 2556–2567. [Google Scholar] [CrossRef]
- Wumener, X.; Zhang, Y.; Wang, Z.; Zhang, M.; Zang, Z.; Huang, B.; Liu, M.; Huang, S.; Huang, Y.; Wang, P.; et al. Dynamic FDG-PET imaging for differentiating metastatic from non-metastatic lymph nodes of lung cancer. Front. Oncol. 2022, 12, 1005924. [Google Scholar] [CrossRef]
- Zhuang, M.; Karakatsanis, N.A.; Dierckx, R.A.J.O.; Zaidi, H. Impact of Tissue Classification in MRI-Guided Attenuation Correction on Whole-Body Patlak PET/MRI. Mol. Imaging Biol. 2019, 21, 1147–1156. [Google Scholar] [CrossRef]
- Zhuang, M.; Karakatsanis, N.A.; Dierckx, R.; Zaidi, H. Quantitative Analysis of Heterogeneous [18F]FDG Static (SUV) vs. Patlak (Ki) Whole-body PET Imaging Using Different Segmentation Methods: A Simulation Study. Mol. Imaging Biol. 2019, 21, 317–327. [Google Scholar] [CrossRef]
- van Sluis, J.; van Snick, J.H.; Brouwers, A.H.; Noordzij, W.; Dierckx, R.A.J.O.; Borra, R.J.H.; Lammertsma, A.A.; Glaudemans, A.W.J.M.; Slart, R.H.J.A.; Yaqub, M.; et al. Shortened duration whole body 18F-FDG PET Patlak imaging on the Biograph Vision Quadra PET/CT using a population-averaged input function. EJNMMI Phys. 2022, 9, 74. [Google Scholar] [CrossRef]
- Karakatsanis, N.A.; Lodge, M.A.; Zhou, Y.; Wahl, R.L.; Rahmim, A. Dynamic whole-body PET parametric imaging: II. Task-oriented statistical estimation. Phys. Med. Biol. 2013, 58, 7419–7445. [Google Scholar] [CrossRef]
- Karakatsanis, N.A.; Lodge, M.A.; Tahari, A.K.; Zhou, Y.; Wahl, R.L.; Rahmim, A. Dynamic whole-body PET parametric imaging: I. Concept, acquisition protocol optimization and clinical application. Phys. Med. Biol. 2013, 58, 7391–7418. [Google Scholar] [CrossRef]
- Lv, W.; Yang, M.; Zhong, H.; Wang, X.; Yang, S.; Bi, L.; Xian, J.; Pei, X.; He, X.; Wang, Y.; et al. Application of Dynamic 18F-FDG PET/CT for Distinguishing Intrapulmonary Metastases from Synchronous Multiple Primary Lung Cancer. Mol. Imaging 2022, 2022, 8081299. [Google Scholar] [CrossRef] [PubMed]
- Minocha, J.; Lewandowski, R.J. Assessing Imaging Response to Therapy. Radiol. Clin. N. Am. 2015, 53, 1077–1088. [Google Scholar] [CrossRef] [PubMed]
- Matsubara, R.; Kawano, S.; Chikui, T.; Kiyosue, T.; Goto, Y.; Hirano, M.; Jinno, T.; Nagata, T.; Oobu, K.; Abe, K.; et al. Clinical Significance of Combined Assessment of the Maximum Standardized Uptake Value of F-18 FDG PET with Nodal Size in the Diagnosis of Cervical Lymph Node Metastasis of Oral Squamous Cell Carcinoma. Acad. Radiol. 2012, 19, 708–717. [Google Scholar] [CrossRef] [PubMed]
- Vogl, T.; Bisdas, S. Lymph node staging. Top. Magn. Reson. Imaging 2007, 18, 303–316. [Google Scholar] [CrossRef] [PubMed]
- Tsao, S.W.; Tsang, C.M.; Lo, K.W. Epstein-Barr virus infection and nasopharyngeal carcinoma. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2017, 372, 20160270. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Tsai, M.-H.; Shumilov, A.; Baccianti, F.; Tsao, S.W.; Poirey, R.; Delecluse, H.-J. Epstein-Barr virus ncRNA from a nasopharyngeal carcinoma induces an inflammatory response that promotes virus production. Nat. Microbiol. 2019, 4, 2475–2486. [Google Scholar] [CrossRef]
- Vasudevan, H.N.; Yom, S.S. Nasopharyngeal Carcinoma and Its Association with Epstein-Barr Virus. Hematol. Oncol. Clin. N. Am. 2021, 35, 963–971. [Google Scholar] [CrossRef]
- Zhao, C.-X.; Zhu, W.; Ba, Z.-Q.; Xu, H.-J.; Liu, W.-D.; Zhu, B.; Wang, L.; Song, Y.-J.; Yuan, S.; Ren, C.-P. The regulatory network of nasopharyngeal carcinoma metastasis with a focus on EBV, lncRNAs and miRNAs. Am. J. Cancer Res. 2018, 8, 2185–2209. [Google Scholar]
- Otrante, A.; Bounafaa, A.; Berrougui, H.; Essamadi, A.-K.; Nguyen, M.; Fülöp, T.; Khalil, A. Small Dense LDL Level and LDL/HDL Distribution in Acute Coronary Syndrome Patients. Biomedicines 2023, 11, 1198. [Google Scholar] [CrossRef]
- Wang, X.S.; Yan, C.; Hu, C.S.; Ying, H.M.; He, X.Y.; Zhou, Z.R.; Ding, J.H. Study of the medial group retropharyngeal node metastasis from nasopharyngeal carcinoma based on 3100 newly diagnosed cases. Oral Oncol. 2014, 50, 1109–1113. [Google Scholar] [CrossRef]
- Fang, F.M.; Tsai, W.L.; Chen, H.C.; Hsu, H.C.; Hsiung, C.Y.; Chien, C.Y.; Ko, S.F. Intensity-modulated or conformal radiotherapy improves the quality of life of patients with nasopharyngeal carcinoma: Comparisons of four radiotherapy techniques. Cancer 2007, 109, 313–321. [Google Scholar] [CrossRef]
- Lu, H.; Peng, L.; Yuan, X.; Hao, Y.; Lu, Z.; Chen, J.; Chang, J.; Geng, S.; Gu, J.; Pang, Q.; et al. Concurrent chemoradiotherapy in locally advanced nasopharyngeal carcinoma: A treatment paradigm also applicable to patients in Southeast Asia. Cancer Treat. Rev. 2009, 35, 345–353. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Luo, T.; Jin, T.; Zhang, J.; Xiang, Z.; Yan, R.; Xie, L.; Wu, X.; Zhang, H.; Wang, F.; et al. Advantages of using reduced-volume intensity modulated radiation therapy for the treatment of nasopharyngeal carcinoma: A retrospective paired study. BMC Cancer 2019, 19, 554. [Google Scholar] [CrossRef]
- Paiar, F.; Di Cataldo, V.; Zei, G.; Pasquetti, E.M.; Cecchini, S.; Meattini, I.; Mangoni, M.; Agresti, B.; Iermano, C.; Bonomo, P.; et al. Role of chemotherapy in nasopharyngeal carcinoma. Oncol. Rev. 2012, 6, e1. [Google Scholar] [CrossRef] [PubMed]
- Muzi, M.; O’Sullivan, F.; Mankoff, D.A.; Doot, R.K.; Pierce, L.A.; Kurland, B.F.; Linden, H.M.; Kinahan, P.E. Quantitative assessment of dynamic PET imaging data in cancer imaging. Magn. Reson. Imaging 2012, 30, 1203–1215. [Google Scholar] [CrossRef]
- Laffon, E.; de Clermont, H.; Begueret, H.; Vernejoux, J.-M.; Thumerel, M.; Marthan, R.; Ducassou, D. Assessment of dual-time-point 18F-FDG-PET imaging for pulmonary lesions. Nucl. Med. Commun. 2009, 30, 455–461. [Google Scholar] [CrossRef]
- Huang, X.; Zhuang, M.; Yang, S.; Wang, Y.; Liu, Q.; Xu, X.; Xiao, M.; Peng, Y.; Jiang, P.; Xu, W.; et al. The valuable role of dynamic 18F FDG PET/CT-derived kinetic parameter Ki in patients with nasopharyngeal carcinoma prior to radiotherapy: A prospective study. Radiother. Oncol. 2023, 179, 109440. [Google Scholar] [CrossRef]
- Kojima, I.; Takanami, K.; Ogawa, T.; Ishikawa, K.; Morishita, Y.; Ishii, R.; Ohkoshi, A.; Nakanome, A.; Odagiri, H.; Iikubo, M. High diagnostic accuracy for lymph node metastasis of oral squamous cell carcinoma using PET/CT with a silicon photomultiplier. Oral Radiol. 2022, 38, 540–549. [Google Scholar] [CrossRef]
- Luzuriaga, K.; Sullivan, J.L. Infectious mononucleosis. N. Engl. J. Med. 2010, 362, 1993–2000. [Google Scholar] [CrossRef]
- Kim, K.Y.; Le, Q.-T.; Yom, S.S.; Ng, R.H.; Chan, K.A.; Bratman, S.V.; Welch, J.J.; Divi, R.L.; Petryshyn, R.A.; Conley, B.A. Clinical Utility of Epstein-Barr Virus DNA Testing in the Treatment of Nasopharyngeal Carcinoma Patients. Int. J. Radiat. Oncol. Biol. Phys. 2017, 98, 996–1001. [Google Scholar] [CrossRef]
- Hsu, C.-L.; Chang, K.-P.; Lin, C.-Y.; Chang, H.-K.; Wang, C.-H.; Lin, T.-L.; Liao, C.-T.; Tsang, N.-M.; Lee, L.-Y.; Chan, S.-C.; et al. Plasma epstein-barr virus DNA concentration and clearance rate as novel prognostic factors for metastatic nasopharyngeal carcinoma. Head Neck 2012, 34, 1064–1070. [Google Scholar] [CrossRef] [PubMed]
- Duffy, M.J.; Sturgeon, C.; Lamerz, R.; Haglund, C.; Holubec, V.L.; Klapdor, R.; Nicolini, A.; Topolcan, O.; Heinemann, V. Tumor markers in pancreatic cancer: A European Group on Tumor Markers (EGTM) status report. Ann. Oncol. 2010, 21, 441–447. [Google Scholar] [CrossRef] [PubMed]








Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).