
Experience of “One Stop TB Diagnostic Solution” Model in Engaging a Private Laboratory for End-to-End Diagnostic Services in the National TB Elimination Program in Hisar, India


Abstract
:1. Background
1.1. The One-Stop TB Diagnostic Solution Model
1.2. Model Implementation
2. Methods
2.1. Data Source
2.2. Analysis and Statistics
- (a)
- Specimens with Xpert negative results are considered MTB negative and no further tests are conducted;
- (b)
- Specimens with Xpert positive results (MTB detected and rifampicin-sensitive) and FL-LPA (rifampicin and isoniazid-sensitive results) are considered DS-TB;
- (c)
- Specimens with the following Xpert results: MTB detected and rifampicin-resistant results; with FL-LPA (rifampicin and/or isoniazid-resistant results); SL-LPA (showing resistance to fluoroquinolones); and LC-DST (results showing resistance to any of the following drugs: moxifloxacin, linezolid, and pyrazinamide) are considered DR-TB. The analysis is presented in the result section as per the tests performed;
- (d)
- All specimens are tracked from the point of collection to the issuance of results, as mentioned above, for an analysis of turnaround time (TAT).
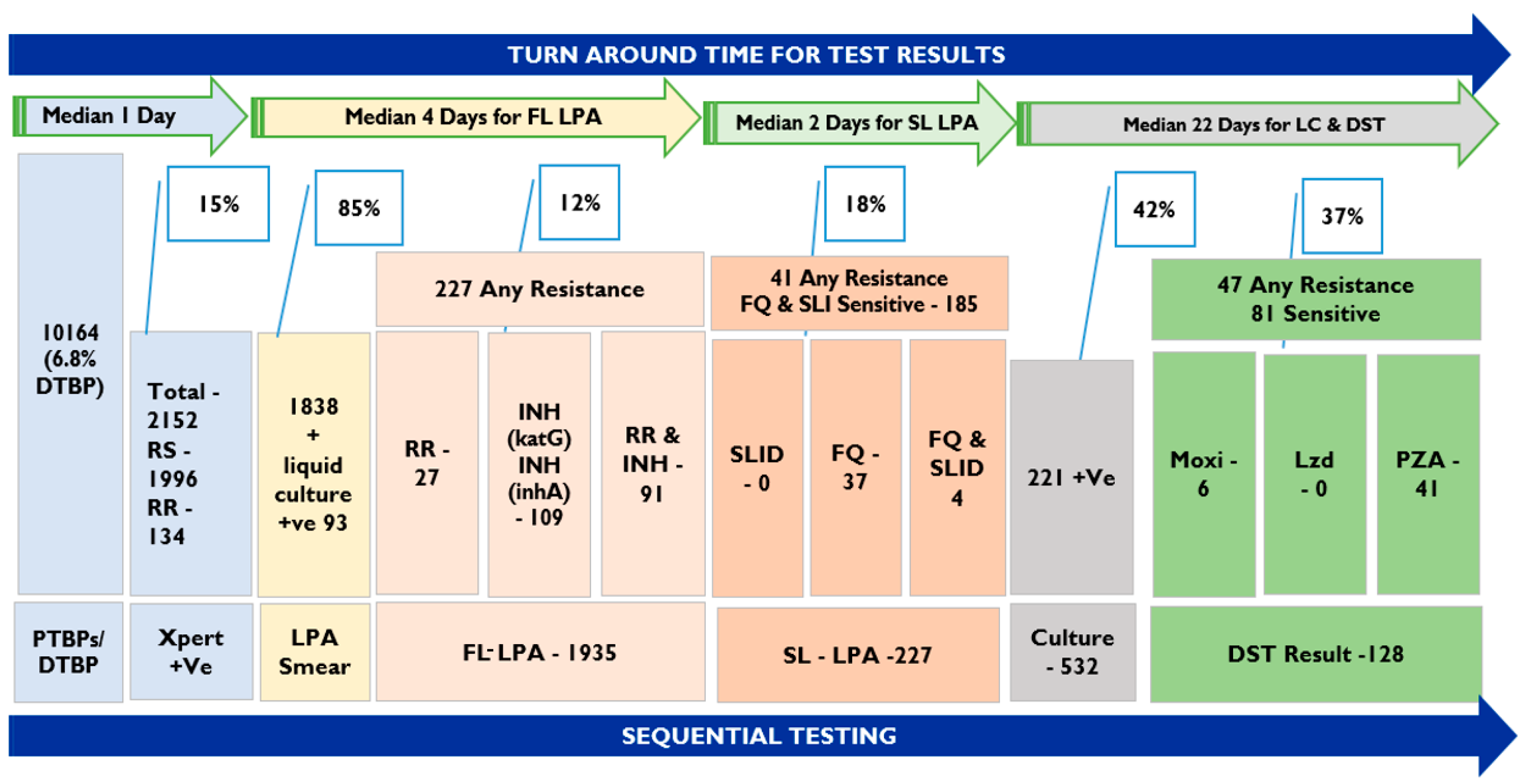
3. Results
3.1. Demographic and Clinical Profile of Patients
3.2. Completing TB Diagnostic Algorithm
3.3. Patients Completing Drug-Susceptible TB Diagnostic Algorithm
3.4. Patients Completing Drug-Resistant TB Diagnostic Algorithm
3.5. Turnaround Time for Completing Diagnostic Tests
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- UNGA. A/RES/73/3. Political Declaration of the High-Level Meeting of the General Assembly on the Fight against Tuberculosis; United Nations: New York, NY, USA, 2018. [Google Scholar]
- GOI. National Strategic Plan to End TB in India 2020–2025. June 2020. Available online: https://tbcindia.gov.in/index1.php?lang=1&level=1&sublinkid=5506&lid=3578 (accessed on 16 July 2023).
- GOI. India TB Report 2023 Leading the Way; Central TB Division, Ministry of Health and Family Welfare: New Delhi, India, 2023. [Google Scholar]
- Subbaraman, R.; Jhaveri, T.; Nathavitharana, R.R. Closing gaps in the tuberculosis care cascade: An action-oriented research agenda. J. Clin. Tuberc. Other Mycobact. Dis. 2020, 19, 100144. [Google Scholar] [CrossRef] [PubMed]
- Seung, K.J.; Keshavjee, S.; Rich, M.L. Multidrug-Resistant Tuberculosis and Extensively Drug-Resistant Tuberculosis. Cold Spring Harb. Perspect. Med. 2015, 5, a017863. [Google Scholar] [CrossRef]
- GOI. Report of The Joint Monitoring Mission: Revised National Tuberculosis Control Programme; Central TB Division, Ministry of Health and Family Welfare: New Delhi, India, 2019. [Google Scholar]
- GOI. Guidance Document on Partnerships. Revised National Tuberculosis Control Programme; Central TB Division, Ministry of Health and Family Welfare: New Delhi, India, 2019. [Google Scholar]
- Manchanda, O. Quality Medical Diagnostics: Making It Affordable and Accessible. 14 July 2020. Available online: https://timesofindia.indiatimes.com/blogs/voices/quality-medical-diagnostics-making-it-affordable-and-accessible/ (accessed on 16 July 2023).
- GOI. ICMR. 11 June 2020. Available online: https://www.icmr.gov.in/pdf/covid/labs/archive/COVID_Testing_Labs_11062020.pdf (accessed on 30 April 2023).
- GOI. National TB Prevalence Survey in India (2019–2021); Central TB Division, Ministry of Health and Family Welfare: New Delhi, India, 2021. [Google Scholar]
- Hisar District. Available online: https://commons.wikimedia.org/wiki/File:HaryanaHisar.png (accessed on 17 August 2023).
- Shankar, S.U.; Kumar, A.M.V.; Venkateshmurthy, N.S.; Nair, D.; Kingsbury, R.; Padmesha, R.; Velu, M.; Suganthi, P.; Gupta, J.; Ahmed, J.; et al. Implementation of the new integrated algorithm for diagnosis of drug-resistant tuberculosis in Karnataka State, India: How well are we doing? PLoS ONE 2021, 16, e0244785. [Google Scholar] [CrossRef]
- Vatsyayan, V.; Pattery, T.; Sayyad, K.; Williams, J.; Pal, A.; Panibatla, V.; Khanna, A. DOST” Model to Link and Support Drug Resistant TB Patients from Private Sector: An Experience from Delhi, India. Front. Public Health 2022, 10, 835055. [Google Scholar] [CrossRef]
- Pai, M.; Dewan, P.K.; Swaminathan, S. Transforming tuberculosis diagnosis. Nat. Microbiol. 2023, 8, 756–759. [Google Scholar] [CrossRef] [PubMed]
- GOI. Guidelines for Progammatic Management of Drug Resistance Tuberculosis in India; Central TB Division, Ministry of Health and Family Welfare: New Delhi, India, 2021. [Google Scholar]



{kind=link}
{kind=link}
| Variable | Number | Percentage |
|---|---|---|
| Total Specimens in the Model | 10,164 | |
| Type of patient | ||
| PTBPs | 9468 | 93.2% |
| Diagnosed TB Patients | 696 | 6.8% |
| Type of Referring Facility | ||
| Public | 9005 | 88.6% |
| Private | 1159 | 11.4% |
| Type of Specimen | ||
| Pulmonary | 9924 | 97.6% |
| Extra Pulmonary | 240 | 2.4% |
| Geography | ||
| Rural | 6660 | 65.5% |
| Urban | 3504 | 34.5% |
| Gender | ||
| Male | 6663 | 65.5% |
| Female | 3500 | 34.4% |
| Transgender | 1 | |
| Age (years) | ||
| ≤ 14 | 284 | 2.8% |
| 15–29 | 2249 | 22.1% |
| 30–44 | 2309 | 22.7% |
| 45–59 | 2411 | 23.7% |
| ≥ 60 | 2911 | 28.6% |
| Xpert Result for MTB | Number | Percentages |
|---|---|---|
| MTB Detected | 2152 | 21.2% |
| MTB Not Detected | 8012 | 78.8% |
| Rifampicin Status Xpert | ||
| Rif-Resistant | 134 | 6.2% |
| Rif-Sensitive | 1996 | 92.7% |
| Rif Indeterminate | 22 | 1.0% |
| Rifampicin-Sensitive (RS) TB Diagnostic Algorithm | One-Stop TB Model | ||
|---|---|---|---|
| sl no. | Particulars | Number | Percentage |
| 1 | Number of RS TB Patients diagnosed using Xpert | 1996 | |
| 2 | Number of samples that reached the reference lab and were eligible | 1996 | 100% |
| 3 | FL-LPA carried out with results | 1806 | 90% |
| a | H- and R-Sensitive | 1692 | 94% |
| b | H-Resistant and R-Sensitive | 108 | 6% |
| c | R-Resistant only | 1 | <1% |
| d | H- and R-Resistant | 5 | <1% |
| 4 | FL-LPA not done | 2 | |
| 5 | SL-LPA done | 114 | 100% |
| 6 | SL-LPA not done | 0 | 0 |
| i | FQ- and SLI-Sensitive | 99 | 87% |
| ii | FQ- and/or SLI-Resistant | 15 | 13% |
| 7 | Liquid Culture—DST done | 114 | 100% |
| 8 | Result anticipated for LC-DST (Moxi, PZA, Lzd) | 6 | 5% |
| 9 | Result for LC-DST (Moxi, PZA, Lzd) | Moxi (3/108), Lzd (1/108), PZA (14/108). | |
| 10 | Number of Rifampicin-Sensitive patients completing the diagnostic algorithm | 1985 | 99% |
| Rifampicin-Resistant TB Diagnostic Algorithm | One-Stop TB Model | ||
|---|---|---|---|
| sl no. | Particulars | Number | Percentage |
| 1 | Number of RR-TB patients diagnosed on Xpert testing | 134 | |
| 2 | Number whose samples reached the C-DST lab for further cascade testing | 134 | |
| i | FL-LPA carried out | 111 | 100% |
| ii | H- and R-Sensitive | 4 | 3% |
| iii | R-Resistant | 26 | 23% |
| iv | H- and R-Resistant | 81 | 73% |
| 3 | FL-LPA not carried out | 2 | 1% |
| 4 | Liquid Culture carried out | 23 | 17% |
| Liquid Culture positive (included into FL-LPA tests) | 2 | 8% | |
| 5 | SL-LPA carried out | 107 | 96% |
| i | FQ- and SLI-sensitive | 81 | 76% |
| ii | FQ- and/or SLI-Resistant | 26 | 24% |
| 6 | SL-LPA Not carried out | 2 | 2% |
| 7 | Liquid Culture DST carried out | 107 | 100% |
| i | Results anticipated for Liquid Culture DST | 3 | 5% |
| ii | Result for LC-DST (Moxi, PZA, Lzd) | Moxi (8/104) Lzd (1/104) PZA (26/104). | |
| 8 | Number of Rifampicin-Resistant patients completing the diagnostic algorithm | 132 | 98% |
| Test Name * | Pre-Lab TAT | Lab TAT | Total TAT |
|---|---|---|---|
| Xpert test | 1 | 1 | 1 (1–1) |
| FL-LPA | n.a | 4 (3–5) | 4 (3–5) |
| SL-LPA | n.a | 2 (1–4) | 2 (1–4) |
| LC-DST ** | n.a | 22 (17–32) | 22 (17–32) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raju, R.; Prasad, B.M.; Alavadi, U.; Saini, S.; Sabharwal, M.; Duhan, A.; Anand, S.; Lal, M.; Kaur, H.; Arora, N.; et al. Experience of “One Stop TB Diagnostic Solution” Model in Engaging a Private Laboratory for End-to-End Diagnostic Services in the National TB Elimination Program in Hisar, India. Diagnostics 2023, 13, 2823. https://doi.org/10.3390/diagnostics13172823
Raju R, Prasad BM, Alavadi U, Saini S, Sabharwal M, Duhan A, Anand S, Lal M, Kaur H, Arora N, et al. Experience of “One Stop TB Diagnostic Solution” Model in Engaging a Private Laboratory for End-to-End Diagnostic Services in the National TB Elimination Program in Hisar, India. Diagnostics. 2023; 13(17):2823. https://doi.org/10.3390/diagnostics13172823
Chicago/Turabian StyleRaju, Rajesh, Banuru Muralidhara Prasad, Umesh Alavadi, Sanjeev Saini, Mukesh Sabharwal, Akshay Duhan, Sridhar Anand, Manohar Lal, Harpreet Kaur, Neerja Arora, and et al. 2023. "Experience of “One Stop TB Diagnostic Solution” Model in Engaging a Private Laboratory for End-to-End Diagnostic Services in the National TB Elimination Program in Hisar, India" Diagnostics 13, no. 17: 2823. https://doi.org/10.3390/diagnostics13172823
APA StyleRaju, R., Prasad, B. M., Alavadi, U., Saini, S., Sabharwal, M., Duhan, A., Anand, S., Lal, M., Kaur, H., Arora, N., Jaju, J., Moore, M., Ramachandran, R., Kumar, N., & Joshi, R. P. (2023). Experience of “One Stop TB Diagnostic Solution” Model in Engaging a Private Laboratory for End-to-End Diagnostic Services in the National TB Elimination Program in Hisar, India. Diagnostics, 13(17), 2823. https://doi.org/10.3390/diagnostics13172823