1. Background
Tuberculosis has received global attention and a political commitment to end TB by 2030 through the United Nations high-level meeting of the General Assembly on the fight against tuberculosis [
1]. India is one of the high TB burden countries and has committed to ending TB by 2025 through strategies envisaged in the “National Strategic Plan” with a focus on building and strengthening the health system for early detection and appropriate treatment [
2]. Early detection through high-sensitivity diagnostics and universal access to quality TB diagnosis is one of the key priority areas. The diagnostic network under the National TB Elimination Program (NTEP) has expanded, with molecular diagnostics at districts and sub-district level (5090 sites with Xpert/Truenat) and TB culture and drug-susceptibility testing facilities (83 Culture and Drug Susceptibility Testing (DST), 34 intermediate reference laboratories) with cutting-edge technologies at state and national levels (six national reference laboratories) [
3]. The diagnosis of Drug-Susceptible TB (DS-TB) and Drug-Resistant TB (DR-TB) requires sequential testing and these tests are available at different levels of the health system. At times, completing the diagnostic assessment of identified presumptive TB patients (PTBPs) could be a challenge and may result in the loss of patients along the care cascade [
4]. An incomplete diagnostic assessment could also lead to inappropriate treatment resulting in the amplification of drug resistance [
5].
The NTEPs diagnostic network and the strategies to increase access to diagnostic services have faced challenges, some of which are: (a) specimen collection and transportation from facilities to different laboratories; (b) the time taken to complete the diagnostic assessment tests required to rule out or detect drug resistance, which are carried out at different facilities at different locations; and (c) the provision of quality-assured diagnostic coverage for patients in the private sector [
2]. Though the program has strengthened the district and reference laboratories, running laboratories is resource intensive and requires the procurement of laboratory reagents, consumables, and test kits, maintenance, and calibration of equipment, sustaining human resources and their competencies, and implementing quality assurance measures [
6]. An option to engage private sector laboratories to complement and enhance the diagnostic services of the public sector is explored as part of the strategy [
7].
Private sector laboratories have demonstrated efficiencies through a person-centric approach for specimen collection, the transportation, testing, and reporting of results in the desired turnaround time (TAT) for a range of hematological and biochemical tests, operationalized through a hub-and-spoke model. Many of the private laboratories have been accredited by the National Accreditation Board for Testing and Calibration Laboratories (NABL) [
8]. The NTEP has also certified 14 laboratories for providing Line Probe Assay (LPA) and Culture DST diagnostic tests [
3]. The efficiency of private laboratories is harnessed using the “turn-key model” of the National AIDS Control Program (NACP), where specimens for viral load testing were collected from district sites and tested at a centralized laboratory and reports are shared in the desired TAT. Recently, the government has strategically engaged several private-sector laboratories for enhancing diagnostic services during the COVID-19 pandemic [
9].
Drawing from these experiences of private laboratory engagement in public health programs, and with the understanding that the TB diagnostic assessment involves multiple tests and the results of the preceding test determine the need for subsequent testing, the “One-Stop TB/DR-TB diagnostic solution” model was designed. This innovative model was conceptualized with the objectives to assess the feasibility, impact, and cost implications of the strategic purchase of TB testing services from a private laboratory for end-to-end operations—specimen collection, transportation, performing tests as per NTEP’s algorithm—and sharing results within the desired TAT. The article here outlines the model’s concept, implementation, and learnings, which could be transitioned into other high-burden TB countries.
1.1. The One-Stop TB Diagnostic Solution Model
The One-Stop TB Diagnostic Solution Model was implemented by the Infectious Disease Detection and Surveillance (IDDS) Project supported by the United States Agency for International Development (USAID) under the guidance of Central TB Division, Ministry of Health and Family Welfare, Government of India. In the model design, the healthcare providers (public/private) identify and refer the PTBPs/or diagnosed TB patients for assessment. The specimens are collected and transported from the point of collection to a centralized NTEP-certified private laboratory where requisite tests are performed. Along with the upfront Nucleic Acid Amplification Test (NAAT), the model offers first- and second-line Line Probe Assay (FL-LPA and SL-LPA) and Liquid Culture and Drug Susceptibility Testing (LC-DST), as per the NTEP’s diagnosed algorithm [
3]. The Chest X-ray (CXR) services for PTBPs are also offered through facilities that are engaged locally by the contracted private laboratory. Pre-treatment evaluation tests for diagnosed DR-TB patients are offered as part of the overall service delivery package. The PTBPs are registered at respective health facilities in the NTEP’s web portal (Ni-kshay) and test reports are updated as and when available. The results are also communicated to the program staff and the referring physician via email, for treatment decisions.
1.2. Model Implementation
The model was implemented in the Hisar district of Haryana in collaboration with the District Health Administration and District TB Office (
Figure 1). The district has an approximate population of two million with a mix of urban, semi-urban, and rural populations and an estimated TB prevalence of 465 (326–605) persons per 100,000 population [
10]. The district has one District TB Centre (DTC), eight TB Units (TUs), 20 designated microscopy centers, and two NAAT (GeneXpert and Truenat) facilities at the DTC and at the medical college. The average distance of the designated microscopy centers to the district headquarters is 28 km (min 7 km–max 59 km). The district is linked to the Intermediate Reference Laboratory (IRL) at Karnal (182 km) for FL-LPA, SL-LPA, and LC-DST, and to National Reference Laboratory at Delhi (118 km from Karnal) for LC-DST of certain second-line drugs.
An NTEP-certified private laboratory (Thyrocare Technologies Private Ltd., Mumbai, India) was selected through an open procurement process and was contracted for providing diagnostic services as envisaged in the model. In consultation with the district NTEP staff, route plans were prepared for specimen collection from public health facilities (tuberculosis units, designated microscopy centers, health and wellness centers, subcenters, and primary healthcare facilities) and private facilities (clinics and hospitals) and the CXR facilities engaged were also mapped (see
Supplementary Figure S1). The contracted laboratory deployed runners who covered nearly 80 facilities (36 public and 44 private) across the district. The runners reach each facility as scheduled daily to collect the specimens. Upon reaching the facility, staff hand over the collected specimens (two specimens for each patient) to runners along with test request forms (TRF) which have a Ni-kshay ID generated for the patient. The runners deposit the specimens at the district hub from where it is transported to the Xpert testing facility at Gurugram the same day (which is about 200 km from Hisar). Following an Xpert result of mycobacteria tuberculosis (MTB) being detected, the second specimen is flown the next day to the NTEP-certified laboratory based in Mumbai for FL-LPA, SL-LPA, and Liquid Culture Drug Susceptibility Test (LC DST) (see
Supplementary Figure S2). The tests are performed in compliance with the NTEP diagnostic algorithms [
3]. The test results are entered as and when they are available in the Ni-kshay portal against the IDs available in the TRF. The referring physicians at respective facilities in Hisar could view the results on the portal and initiate the treatment appropriately. In addition, the laboratory also shared reports via email with the health facilities at the district and sub-district levels.
3. Results
3.1. Demographic and Clinical Profile of Patients
A total of 10,164 patient specimens were collected and processed during the model implementation period, out of which 9468 (93%) specimens were collected from PTBPs for the diagnosis of TB and the remaining were from diagnosed TB patients for further assessment for drug resistance (
Table 1). More than 88% of the specimens collected were from public facilities and 11% were from private facilities. The private facilities provided specimens for >50% of the extrapulmonary specimens. The maximum number of specimens were collected from rural areas rather than urban areas and from male patients and from patients ≤ 60 years.
3.2. Completing TB Diagnostic Algorithm
The specimens collected were processed using GeneXpert (Xpert MTB/rifampicin) for the diagnosis of TB and 21% of specimens resulted in MTB being detected (
Table 2). Excluding the specimens from diagnosed TB patients for further testing for drug resistance, MTB was detected in 1457 (15%) specimens from PTBPs (
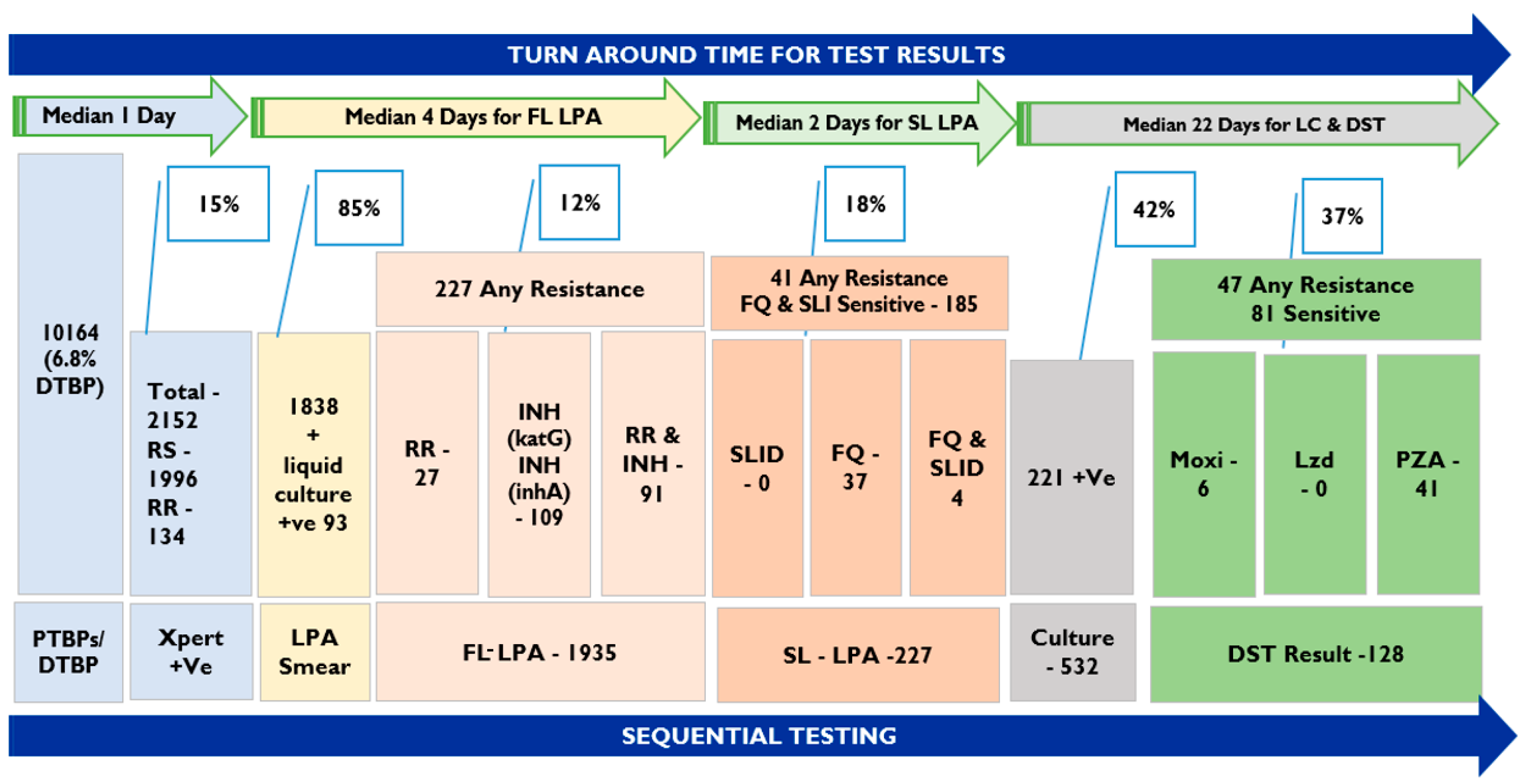
Table 2). Rifampicin resistance (RR) was detected in 5.7% of PTBP MTB positive specimens (84 patients) and 7% of specimens from diagnosed TB patients. Almost 100% of Xpert MTB specimens were subjected to FL-LPA. There were 13 specimens with insufficient quantity for processing that were requested for repeat samples for further testing and were not received. Out of the total of 2136 specimens, 1838 were smear-positive and 298 were smear-negative prior to performing FL-LPA tests (
Figure 2). All smear-negative specimens were inoculated for Liquid Culture and 93 showed growth (31%). A total of 227 specimen results showed resistance to one of the first-line drugs (rifampicin/isoniazid).
Following the NTEP diagnostic algorithm, 227 specimens were processed for SL-LPA. The results showed that 37 specimens were resistant to fluoroquinolones and 4 specimens were found to be resistant to fluoroquinolones (FQ) and second-line injectable drugs (SLID). The remaining 186 specimens were sensitive to both FQ and SLID. All 227 specimens were processed for LC in a Mycobacteria Growth Indicator Tube (MGIT 960); out of these 133 showed growth and the DST results for 128 specimens were available. The results for the remaining specimens are expected shortly, at the time of manuscript preparation. A total of 11 specimens showed resistance to moxifloxacin, 2 specimens were resistant to linezolid, and 41 were resistant to pyrazinamide. Resistance to moxifloxacin and pyrazinamide is seen in five specimens and resistance to linezolid and pyrazinamide was seen in two specimens.
3.3. Patients Completing Drug-Susceptible TB Diagnostic Algorithm
The specimens with Xpert results of being MTB positive and rifampicin-sensitive (RS) were eligible to be tested for FL-LPA. Prior to FL-LPA tests, smear tests were performed. The results of smear tests determined whether the specimen was to be processed directly for LPA or indirectly following LC (MGIT 960). Out of the 1996 eligible for FL-LPA, 1715 (86%) had smear-positive results and 267 (13%) were smear-negative. The smear-negative specimens were subjected to LC and 12 specimens were rejected for insufficient specimen quantity and 2 repeat specimens were not received. Including the culture-positive samples (89/267, 33%), 1806 specimens were tested for FL-LPA (including two smear-negative and culture-negative samples processed for LPA). The tests were not conducted for 174 specimens with culture-negative results and 14 specimens for which repeat specimens were not received (
Table 3). Among the specimens tested for FL-LPA, 93% were sensitive to both rifampicin and isoniazid and were declared as DS-TB. The specimens resistant to isoniazid, rifampicin, and both isoniazid and rifampicin were 108 (6%), 1 (<1%), and 5 (4%), respectively, and these 114 specimens were subjected for SL-LPA and LC-DST as per the algorithm.
Out of the 114 specimens eligible for SL-LPA, 99 (87%) were sensitive to FQ and SLID. About 13% of the specimens were resistant to either FQ or SLID. The culture DST results were available for 108 specimens and results were anticipated for 6 specimens while the manuscript was being prepared. The LC-DST results showed resistance to moxifloxacin (3/108, 3%) linezolid (1/108, 1%), and pyrazinamide (14/108, 13%). Two specimens were resistant to both moxifloxacin and pyrazinamide and one specimen was resistant to linezolid and pyrazinamide. None of the specimens were resistant to both fluoroquinolone and linezolid. Almost 99% of the cohort of patient specimens with MTB positive/RS Xpert test results completed the diagnostic algorithm.
3.4. Patients Completing Drug-Resistant TB Diagnostic Algorithm
Out of the total 134 RR TB specimens, 109 were smear-positive and processed for FL-LPA directly, and the remaining 23 were subjected to LC (2 specimens were excluded, 1 repeat specimen and 1 for insufficient quantity). Two specimens with culture-positive results were processed for FL-LPA. Among the total 111 specimens processed for FL-LPA, isoniazid and rifampicin resistance was seen in 81 (73%), and rifampicin resistance was seen in 26 (23%) specimens (
Table 4).
A total of 107 specimens resistant to either isoniazid or rifampicin following the FL-LPA results were tested for SL-LPA. Among the specimens tested, 81 (76%) were sensitive to FQ and SLIDs and 26 (24%) specimens were resistant to either of the drugs. In the model, all those specimens (107 specimens) with any drug-resistant results were subjected to LC-DST. The LC results for three specimens were still under process. The results were available for 104 specimens, which showed 8% resistance to moxifloxacin (8/104), 1% to linezolid (1/104), and 25% to pyrazinamide (26/104). The resistance to both moxifloxacin and pyrazinamide was seen in three specimens and one specimen showed resistance to both linezolid and pyrazinamide. Overall, 96% of patient specimens completed the DR-TB diagnostic algorithm in the model.
3.5. Turnaround Time for Completing Diagnostic Tests
The TAT analysis included the time interval between the day of specimen collection to the issuance of results. The TAT is shown for respective tests along the diagnostic care cascade (
Table 5). The median number of days for reporting results for Xpert, FL-LPA, SL-LPA, and LC-DST was 1 day, 5 days, 7 days, and 45 days, respectively. For specimens with smear-negative results requiring liquid culture prior to LPA, the results were shared within 30 days.
The TAT for RS and/or DS-TB specimens with smear-positive results was about 4–6 days, including results for FL-LPA. For RR and/or DR-TB patients, the TAT was in the range of 6–9 days, including SL-LPA. However, with the inclusion of LC for smear-negative and LC-DST for certain drugs of DR-TB patients, the median TAT for completing the NTEP diagnostic algorithm up to pyrazinamide susceptibility testing was 45 days. For all liquid cultures, negative results were declared within 42 days, as per the protocol for declaring results in MGIT 960.
4. Discussion
The salient features of the innovative “One-Stop TB diagnostic solution model” are: (a) the staff at the health facility generated a Ni-kshay ID for all PTBPs and two specimens were collected for testing; (b) the runners reached facilities as scheduled along the designated route maps covering rural and urban areas to collect the specimen and deposit it at the district hub, from where the logistic team shipped them to the Xpert lab and NTEP-certified culture-DST lab of the contracted private laboratory; (c) the NTEP diagnostic algorithm was followed and the results were updated as and when they were available in the portal, which could be accessed by referring to the facility; (d) a one-time specimen is collected and it is ensured that all tests are performed as per the algorithm; (e) the results are issued as per the NTEP-prescribed TAT for respective tests; and (f) the laboratory services in the public sector continued to perform Xpert and other tests, complementing the diagnostic services for the district.
The findings from the model could be referred to two studies from India. A cohort study conducted by Uma Shankar et al. in Karnataka involved a review of program records and the mapping of sequential testing [
12]. In Uma Shankar’s study, patients with Xpert MTB-detected results were traced to a reference laboratory and the results showed that FL-LPA reports were available for 71% of patients. However, SL-LPA reports were available for 20% of eligible and culture results for 40% of patients. Overall, 95% of patients with Xpert RS results completed the algorithm. In the same study, for those with RR specimens, FL-LPA reports were available for 55%, SL-LPA for 31%, and 49% completed the diagnostic algorithm. Comparing these results with the Hisar model, 99% of specimens with RS and 98% RR completed the diagnostic algorithm (a comparative table with the model is available in
Supplementary Tables S1 and S2). The “DOST” intervention model in Delhi was designed to strengthen the patient care pathway, collected 9331 specimens of patients from private providers, and transported them to Xpert sites in public facilities through an interface agency [
13]. The Xpert results showed 382 specimens were RR and 198 (52%) specimens were subjected to SL- LPA, out of which 134 (68%) completed the tests. The LPA tests were also performed in the IRL of the NTEP. Both studies were conducted in routine programmatic settings with the involvement of public health laboratories. However, in the one-stop diagnostic solution model, the services were provided by a contracted private laboratory.
A complete TB diagnostic assessment is critical for a clinician to decide on an appropriate treatment regimen. Empirical treatment regimens, due to the non-availability of certain test results, may cause an amplification of drug resistance, treatment failures, and the continued transmission of infection [
14]. Along with completing the diagnostic assessment, it is equally important to obtain results within the stipulated TAT. The model has demonstrated that one-time specimens collected from patients, and issuing results within the stipulated TAT, would reduce the need for multiple visits to the same/different providers or visits to higher centers. The availability of timely test results and prompt initiation of appropriate treatment could also reduce transmission. The indicated TAT for various tests includes collection, performing the tests, and issuing the results of the program, and is 1–2 days for Xpert and 2–4 days for LPA [
15]. In the model, these TATs were achieved, which were much lower compared to other studies from Delhi—2.6 days for Xpert, 26 days for LPA—and for the study from Karnataka—1 day for Xpert, 5 days for LPA (see
Supplementary Table S3 for a comparison of the TAT of NTEP with the studies and model) [
12].
The pre-treatment evaluation (PTE) of diagnosed DR-TB patients was part of the overall diagnostic service package included in the model. The diagnosed DR-TB patients were counseled and assessed by the nodal officer who prescribed the evaluation tests. All the tests were reported within a day to the medical officer for the initiation of the appropriate treatment regimen. In the model, sequential testing was also completed for twenty-two specimens with Xpert Rifampicin Indeterminant results (see
Supplementary Table S4).
The model has demonstrated the fact that diagnostic and operational efficiencies could be incorporated into routine programmatic settings to strengthen diagnostic services. The runner concept could facilitate ensuring specimens are picked and reach the facility as scheduled and in a timely manner, and the services could be bundled along with other laboratory services for sustainability. The laboratory operations could be extended beyond regular timings with a 6/8 hourly shift basis for laboratory technicians to provide results on the same day and to ship specimens to higher centers for further testing. The program may also explore the purchase of services from private laboratories, as demonstrated in the model.
Overall, the model is designed to complete the diagnostic care cascade and no efforts were made for additional case finding. This is one of the limitations of the model and others worth mentioning are: (a) the CXR services included in the model had a negligible role in the diagnostic care cascade; and (b), though the runners were available for transport, repeat specimens were not available for 14 patients, and the team coordinated with the program and other partners to trace the patients. However, these were lost to follow-up due to multiple reasons. Limited efforts were made by the private laboratory to address the discordant results for ten specimens between FL-LPA and Xpert by performing a third test on Xpert for RR status. However, this discordance was resolved for four specimens.






{kind=link}
{kind=link}