


Image Quality and Quantitative PET Parameters of Low-Dose [18F]FDG PET in a Long Axial Field-of-View PET/CT Scanner

 , , , , , , , and
, , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Population
2.2. Imaging Protocol
2.3. Image Reconstruction
2.4. Image Analysis and Evaluation
2.5. Subjective PET Image Quality
2.6. Quantitative PET Analyses
2.7. Radiation Exposure
2.8. Statistical Analysis
3. Results
3.1. Overall PET Image Quality
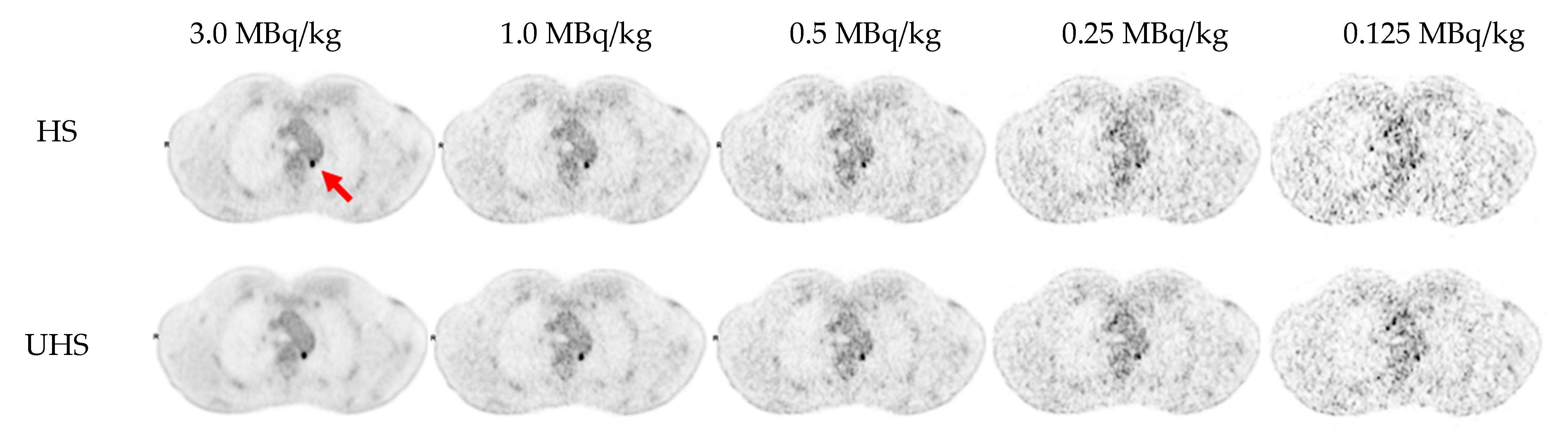
3.2. Detectability and Conspicuity of Suspected Pathological Lesions
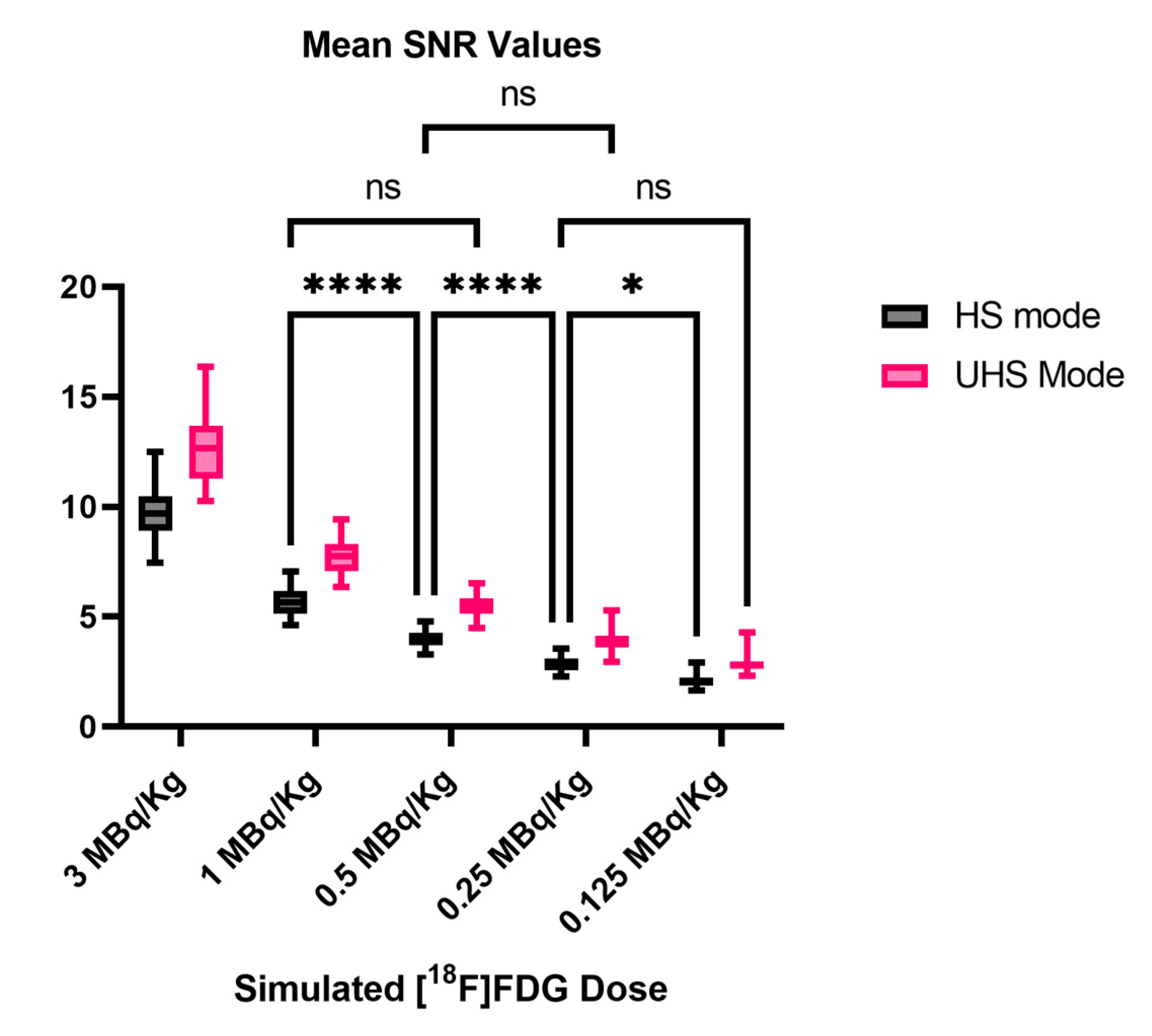
3.3. Image Noise
3.4. Quantitative PET Parameters
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Farsad, M. FDG PET/CT in the Staging of Lung Cancer. Curr. Radiopharm. 2020, 13, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Ayati, N.; Sadeghi, R.; Kiamanesh, Z.; Lee, S.T.; Zakavi, S.R.; Scott, A.M. The Value of 18F-FDG PET/CT for Predicting or Mon-itoring Immunotherapy Response in Patients with Metastatic Melanoma: A Systematic Review and Meta-Analysis. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 428–448. [Google Scholar] [CrossRef] [PubMed]
- Zanoni, L.; Bezzi, D.; Nanni, C.; Paccagnella, A.; Farina, A.; Broccoli, A.; Casadei, B.; Zinzani, P.L.; Fanti, S. PET/CT in Non-Hodgkin Lymphoma: An Update. Semin. Nucl. Med. 2023, 53, 320–351. [Google Scholar] [CrossRef]
- Nadig, V.; Herrmann, K.; Mottaghy, F.M.; Schulz, V. Hybrid Total-Body Pet Scanners—Current Status and Future Perspectives. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 445–459. [Google Scholar] [CrossRef] [PubMed]
- Alavi, A.; Saboury, B.; Nardo, L.; Zhang, V.; Wang, M.; Li, H.; Raynor, W.Y.; Werner, T.J.; Høilund-Carlsen, P.F.; Revheim, M.-E. Potential and Most Relevant Applications of Total Body PET/CT Imaging. Clin. Nucl. Med. 2022, 47, 43–55. [Google Scholar] [CrossRef]
- Alberts, I.; Hünermund, J.-N.; Prenosil, G.; Mingels, C.; Bohn, K.P.; Viscione, M.; Sari, H.; Vollnberg, B.; Shi, K.; Afshar-Oromieh, A.; et al. Clinical Performance of Long Axial Field of View PET/CT: A Head-to-Head Intra-Individual Comparison of the Bi-ograph Vision Quadra with the Biograph Vision PET/CT. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 2395–2404. [Google Scholar] [CrossRef]
- Dimitrakopoulou-Strauss, A.; Pan, L.; Sachpekidis, C. Long Axial Field of View (LAFOV) PET-CT: Implementation in Static and Dynamic Oncological Studies. Eur. J. Nucl. Med. Mol. Imaging 2023, 50, 3354–3362. [Google Scholar] [CrossRef]
- Attarwala, A.A.; Molina-Duran, F.; Büsing, K.-A.; Schönberg, S.O.; Bailey, D.L.; Willowson, K.; Glatting, G. Quantitative and Qualitative Assessment of Yttrium-90 PET/CT Imaging. PLoS ONE 2014, 9, e110401. [Google Scholar] [CrossRef]
- Dryák, P.; Šolc, J. Measurement of the Branching Ratio Related to the Internal Pair Production of Y-90. Appl. Radiat. Isot. 2020, 156, 108942. [Google Scholar] [CrossRef]
- van Sluis, J.; Borra, R.; Tsoumpas, C.; van Snick, J.H.; Roya, M.; Ten Hove, D.; Brouwers, A.H.; Lammertsma, A.A.; Noordzij, W.; Dierckx, R.A.J.O.; et al. Extending the Clinical Capabilities of Short- and Long-Lived Positron-Emitting Radionuclides through High Sensitivity PET/CT. Cancer Imaging 2022, 22, 69. [Google Scholar] [CrossRef]
- Mohr, P.; van Sluis, J.; Providência, L.; van Snick, J.H.; Hooge, M.N.L.; Willemsen, A.T.; Glaudemans, A.W.J.M.; Boellaard, R.; Lammertsma, A.A.; Brouwers, A.H.; et al. Long Versus Short Axial Field of View Immuno-PET/CT: Semiquantitative Evalu-ation for 89Zr-Trastuzumab. J. Nucl. Med. 2023. [Google Scholar] [CrossRef]
- Lugat, A.; Bailly, C.; Chérel, M.; Rousseau, C.; Kraeber-Bodéré, F.; Bodet-Milin, C.; Bourgeois, M. Immuno-PET: Design Options and Clinical Proof-of-Concept. Front. Med. 2022, 9, 1026083. [Google Scholar] [CrossRef] [PubMed]
- Tan, H.; Sui, X.; Yin, H.; Yu, H.; Gu, Y.; Chen, S.; Hu, P.; Mao, W.; Shi, H. Total-Body PET/CT Using Half-Dose FDG and Compared with Conventional PET/CT Using Full-Dose FDG in Lung Cancer. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 1966–1975. [Google Scholar] [CrossRef] [PubMed]
- Sachpekidis, C.; Pan, L.; Kopp-Schneider, A.; Weru, V.; Hassel, J.C.; Dimitrakopoulou-Strauss, A. Application of the Long Axial Field-of-View PET/CT with Low-Dose [18F]FDG in Melanoma. Eur. J. Nucl. Med. Mol. Imaging 2023, 50, 1158–1167. [Google Scholar] [CrossRef] [PubMed]
- Surti, S.; Pantel, A.R.; Karp, J.S. Total Body PET: Why, How, What For? IEEE Trans. Radiat. Plasma Med. Sci. 2020, 4, 283–292. [Google Scholar] [CrossRef]
- Cherry, S.R.; Jones, T.; Karp, J.S.; Qi, J.; Moses, W.W.; Badawi, R.D. Total-Body PET: Maximizing Sensitivity to Create New Opportunities for Clinical Research and Patient Care. J. Nucl. Med. 2018, 59, 3–12. [Google Scholar] [CrossRef]
- Prenosil, G.A.; Hentschel, M.; Weitzel, T.; Sari, H.; Shi, K.; Afshar-Oromieh, A.; Rominger, A. EARL Compliance Measure-ments on the Biograph Vision Quadra PET/CT System with a Long Axial Field of View. EJNMMI Phys. 2022, 9, 26. [Google Scholar] [CrossRef]
- Prenosil, G.A.; Sari, H.; Fürstner, M.; Afshar-Oromieh, A.; Shi, K.; Rominger, A.; Hentschel, M. Performance Characteristics of the Biograph Vision Quadra PET/CT System with a Long Axial Field of View Using the NEMA NU 2-2018 Standard. J. Nucl. Med. 2022, 63, 476–484. [Google Scholar] [CrossRef]
- Mingels, C.; Weidner, S.; Sari, H.; Buesser, D.; Zeimpekis, K.; Shi, K.; Alberts, I.; Rominger, A. Impact of the New Ultra-High Sensitivity Mode in a Long Axial Field-of-View PET/CT. Ann. Nucl. Med. 2023, 37, 310–315. [Google Scholar] [CrossRef]
- Boellaard, R.; Delgado-Bolton, R.; Oyen, W.J.G.; Giammarile, F.; Tatsch, K.; Eschner, W.; Verzijlbergen, F.J.; Barrington, S.F.; Pike, L.C.; Weber, W.A.; et al. FDG PET/CT: EANM Procedure Guidelines for Tumour Imaging: Version 2.0. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 328–354. [Google Scholar] [CrossRef]
- De Luca, G.M.R.; Habraken, J.B.A. Method to Determine the Statistical Technical Variability of SUV Metrics. EJNMMI Phys. 2022, 9, 40. [Google Scholar] [CrossRef] [PubMed]
- EFOMP Protocol for Quality Control in PET/CT and PET/MRI. Available online: https://www.efomp.org/index.php?r=news/view&id=277 (accessed on 22 May 2023).
- Mattsson, S.; Johansson, L.; Leide Svegborn, S.; Liniecki, J.; Noßke, D.; Riklund, K.Å.; Stabin, M.; Taylor, D.; Bolch, W.; Carlsson, S.; et al. Radiation Dose to Patients from Radiopharmaceuticals: A Compendium of Current Information Related to Frequently Used Substances. Ann. ICRP 2015, 44, 7–321. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Gu, Y.; Yu, H.; Wu, B.; Wang, S.; Tan, H.; Cao, Y.; Chen, S.; Sui, X.; Zhang, Y.; et al. Optimizing Acquisition Times for Total-Body Positron Emission Tomography/Computed Tomography with Half-Dose 18F-Fluorodeoxyglucose in Oncology Patients. EJNMMI Phys. 2022, 9, 45. [Google Scholar] [CrossRef] [PubMed]
- Tan, H.; Cai, D.; Sui, X.; Qi, C.; Mao, W.; Zhang, Y.; Liu, G.; Yu, H.; Chen, S.; Hu, P.; et al. Investigating Ultra-Low-Dose To-tal-Body [18F]-FDG PET/CT in Colorectal Cancer: Initial Experience. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 1002–1011. [Google Scholar] [CrossRef] [PubMed]
- Rausch, I.; Mannheim, J.G.; Kupferschläger, J.; la Fougère, C.; Schmidt, F.P. Image Quality Assessment along the One Metre Axial Field-of-View of the Total-Body Biograph Vision Quadra PET/CT System for 18F-FDG. EJNMMI Phys. 2022, 9, 87. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, F.P.; Mannheim, J.G.; Linder, P.; Will, P.; Kiefer, L.S.; Conti, M.; la Fougère, C.; Rausch, I. Impact of the maximum ring difference on image quality and noise characteristics of a total-body PET/CT scanner. Z. Med. Phys. 2023; in press. [Google Scholar] [CrossRef]
- van Sluis, J.; van Snick, J.H.; Brouwers, A.H.; Noordzij, W.; Dierckx, R.A.J.O.; Borra, R.J.H.; Slart, R.H.J.A.; Lammertsma, A.A.; Glaudemans, A.W.J.M.; Boellaard, R.; et al. EARL Compliance and Imaging Optimisation on the Biograph Vision Quadra PET/CT Using Phantom and Clinical Data. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 4652–4660. [Google Scholar] [CrossRef]
- Koopman, D.; van Osch, J.A.C.; Jager, P.L.; Tenbergen, C.J.A.; Knollema, S.; Slump, C.H.; van Dalen, J.A. Technical Note: How to Determine the FDG Activity for Tumour PET Imaging That Satisfies European Guidelines. EJNMMI Phys. 2016, 3, 22. [Google Scholar] [CrossRef]
- Lodge, M.A.; Chaudhry, M.A.; Wahl, R.L. Noise Considerations for PET Quantification Using Maximum and Peak Standard-ized Uptake Value. J. Nucl. Med. 2012, 53, 1041–1047. [Google Scholar] [CrossRef]
- Tsai, Y.-J.; Liu, C. Pitfalls on PET/CT Due to Artifacts and Instrumentation. Semin. Nucl. Med. 2021, 51, 646–656. [Google Scholar] [CrossRef]
- Alessio, A.M.; Stearns, C.W.; Tong, S.; Ross, S.G.; Kohlmyer, S.; Ganin, A.; Kinahan, P.E. Application and Evaluation of a Measured Spatially Variant System Model for PET Image Reconstruction. IEEE Trans. Med. Imaging 2010, 29, 938–949. [Google Scholar] [CrossRef]
- Buteau, J.P.; Martin, A.J.; Emmett, L.; Iravani, A.; Sandhu, S.; Joshua, A.M.; Francis, R.J.; Zhang, A.Y.; Scott, A.M.; Lee, S.-T.; et al. PSMA and FDG-PET as Predictive and Prognostic Biomarkers in Patients given [177Lu]Lu-PSMA-617 versus Cabazitaxel for Metastatic Castration-Resistant Prostate Cancer (TheraP): A Biomarker Analysis from a Randomised, Open-Label, Phase 2 Trial. Lancet Oncol. 2022, 23, 1389–1397. [Google Scholar] [CrossRef] [PubMed]
- Alberts, I.; Schepers, R.; Zeimpekis, K.; Sari, H.; Rominger, A.; Afshar-Oromieh, A. Combined [68 Ga]Ga-PSMA-11 and Low-Dose 2-[18F]FDG PET/CT Using a Long-Axial Field of View Scanner for Patients Referred for [177Lu]-PSMA-Radioligand Therapy. Eur. J. Nucl. Med. Mol. Imaging 2023, 50, 951–956. [Google Scholar] [CrossRef] [PubMed]
- Reichkendler, M.; Andersen, F.L.; Borgwardt, L.; Nygaard, U.; Albrecht-Beste, E.; Andersen, K.F.; Ljunggren, A.; Abraham-sen, N.; Loft, A.; Højgaard, L.; et al. A Long Axial Field of View Enables PET/CT in Toddler Without Sedation. J. Nucl. Med. 2022, 63, 1962. [Google Scholar] [CrossRef] [PubMed]
- Sekine, T.; Delso, G.; Zeimpekis, K.G.; de Galiza Barbosa, F.; Ter Voert, E.E.G.W.; Huellner, M.; Veit-Haibach, P. Reduction of 18F-FDG Dose in Clinical PET/MR Imaging by Using Silicon Photomultiplier Detectors. Radiology 2018, 286, 249–259. [Google Scholar] [CrossRef]
- Mannheim, J.G.; Rausch, I.; Conti, M.; la Fougère, C.; Schmidt, F.P. Characterization of the Partial Volume Effect along the Axial Field-of-View of the Biograph Vision Quadra Total-Body PET/CT System for Multiple Isotopes. EJNMMI Phys. 2023, 10, 33. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Score | Image Quality | Lesion Conspicuity | Image Noise |
|---|---|---|---|
| 5 | state-of-the-art quality | well-defined | near-imperceptible noise |
| 4 | superior to the average | fairly defined | lower than regular image of daily practice |
| 3 | regular quality of daily practice | hazy, recognizable | similar to regular image of daily practice |
| 2 | barely diagnostic | ill-defined, impairing diagnostic confidence | increased noise, slightly worse than regular image of daily practice |
| 1 | non-diagnostic | un-recognizable | excessive noise |
| [18F]FDG MBq/kg | Sensitivity Mode | Number of Lesions Detected | Lesion Detection Rate in % |
|---|---|---|---|
| 3.0 | UHS | 82 | 100% |
| 3.0 | HS | 82 | 100% |
| 1.0 | UHS | 82 | 100% |
| 1.0 | HS | 82 | 100% |
| 0.5 | UHS | 80 | 98% |
| 0.5 | HS | 78 | 95% |
| 0.25 | UHS | 68 | 83% |
| 0.25 | HS | 58 | 71% |
| 0.125 | UHS | 49 | 60% |
| 0.125 | HS | 40 | 49% |
| [18F]FDG MBq/kg | Sensitivity Mode | Mean CoV and STD in % | Mean SNR and STD |
|---|---|---|---|
| 3.0 | UHS | 7.9 ± 1.0 | 12.8 ± 1.6 |
| 3.0 | HS | 10.4 ± 1.2 | 9.7 ± 1.1 |
| 1.0 | UHS | 13.0 ± 1.3 | 7.8 ± 0.8 |
| 1.0 | HS | 17.9 ± 2.0 | 5.7 ± 0.6 |
| 0.5 | UHS | 18.3 ± 1.8 | 5.5 ± 0.5 |
| 0.5 | HS | 25.3 ± 2.6 | 4.0 ± 0.4 |
| 0.25 | UHS | 26.0 ± 3.3 | 3.9 ± 0.5 |
| 0.25 | HS | 35.5 ± 4.0 | 2.9 ± 0.3 |
| 0.125 | UHS | 35.7 ± 4.5 | 2.9 ± 0.4 |
| 0.125 | HS | 49.0 ± 6.3 | 2.1 ± 0.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calderón, E.; Schmidt, F.P.; Lan, W.; Castaneda-Vega, S.; Brendlin, A.S.; Trautwein, N.F.; Dittmann, H.; la Fougère, C.; Kiefer, L.S. Image Quality and Quantitative PET Parameters of Low-Dose [18F]FDG PET in a Long Axial Field-of-View PET/CT Scanner. Diagnostics 2023, 13, 3240. https://doi.org/10.3390/diagnostics13203240
Calderón E, Schmidt FP, Lan W, Castaneda-Vega S, Brendlin AS, Trautwein NF, Dittmann H, la Fougère C, Kiefer LS. Image Quality and Quantitative PET Parameters of Low-Dose [18F]FDG PET in a Long Axial Field-of-View PET/CT Scanner. Diagnostics. 2023; 13(20):3240. https://doi.org/10.3390/diagnostics13203240
Chicago/Turabian StyleCalderón, Eduardo, Fabian P. Schmidt, Wenhong Lan, Salvador Castaneda-Vega, Andreas S. Brendlin, Nils F. Trautwein, Helmut Dittmann, Christian la Fougère, and Lena Sophie Kiefer. 2023. "Image Quality and Quantitative PET Parameters of Low-Dose [18F]FDG PET in a Long Axial Field-of-View PET/CT Scanner" Diagnostics 13, no. 20: 3240. https://doi.org/10.3390/diagnostics13203240
APA StyleCalderón, E., Schmidt, F. P., Lan, W., Castaneda-Vega, S., Brendlin, A. S., Trautwein, N. F., Dittmann, H., la Fougère, C., & Kiefer, L. S. (2023). Image Quality and Quantitative PET Parameters of Low-Dose [18F]FDG PET in a Long Axial Field-of-View PET/CT Scanner. Diagnostics, 13(20), 3240. https://doi.org/10.3390/diagnostics13203240