
Advances in Biomarkers for Diagnosis and Treatment of ARDS

Abstract
:1. Introduction
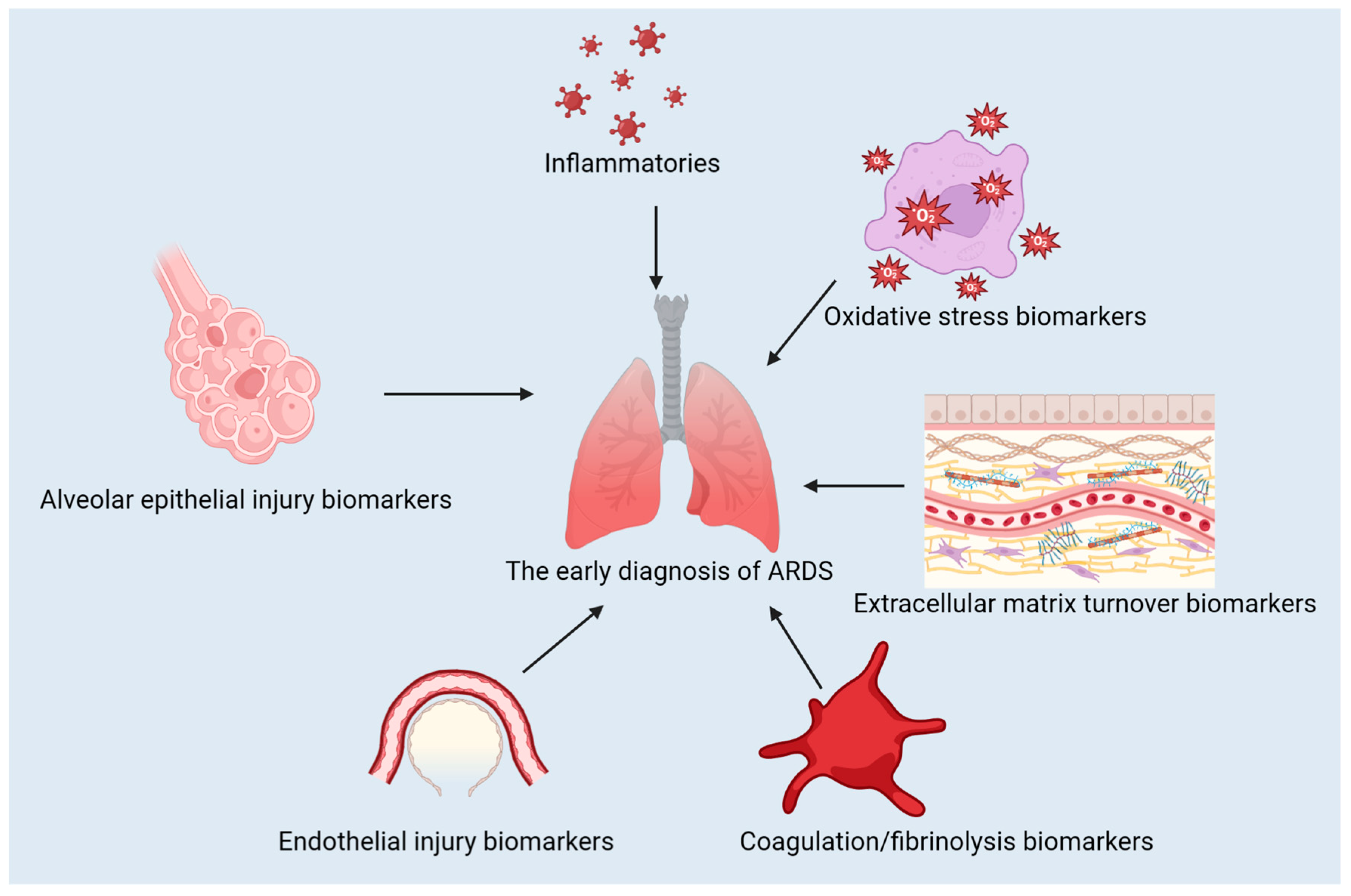
2. Classification of the Biomarkers Related to ARDS
2.1. Inflammatory Biomarkers
2.1.1. Interleukin-6 (IL-6)
2.1.2. Interleukin-8 (IL-8)
2.1.3. Tumor Necrosis Factor-Alpha (TNF-α)
2.1.4. The Neutrophil Response Index (NEUT-RI)
2.2. Alveolar Epithelial Injury Biomarkers
2.2.1. Receptor for Advanced Glycation End Products (RAGE)
2.2.2. Surfactant Protein-D (SP-D)
2.2.3. Clara Cell Secretory Protein (CCSP or CC16)
2.3. Endothelial Injury Biomarkers
2.3.1. Angiopoietin-2 (Ang-2)
2.3.2. Von Willebrand Factor (vWF)
2.3.3. Intercellular Adhesion Molecule-1 (ICAM-1)
2.4. Coagulation/Fibrinolysis Biomarkers
2.4.1. Plasminogen Activator Inhibitor-1 (PAI-1)
2.4.2. Thrombomodulin
2.4.3. D-Dimer
2.5. Extracellular Matrix Turnover Biomarkers
2.5.1. Matrix Metalloproteinase-9 (MMP-9)
2.5.2. Tissue Inhibitor of Metalloproteinase-1 (TIMP-1)
2.6. Oxidative Stress Biomarkers
Malondialdehyde (MDA)
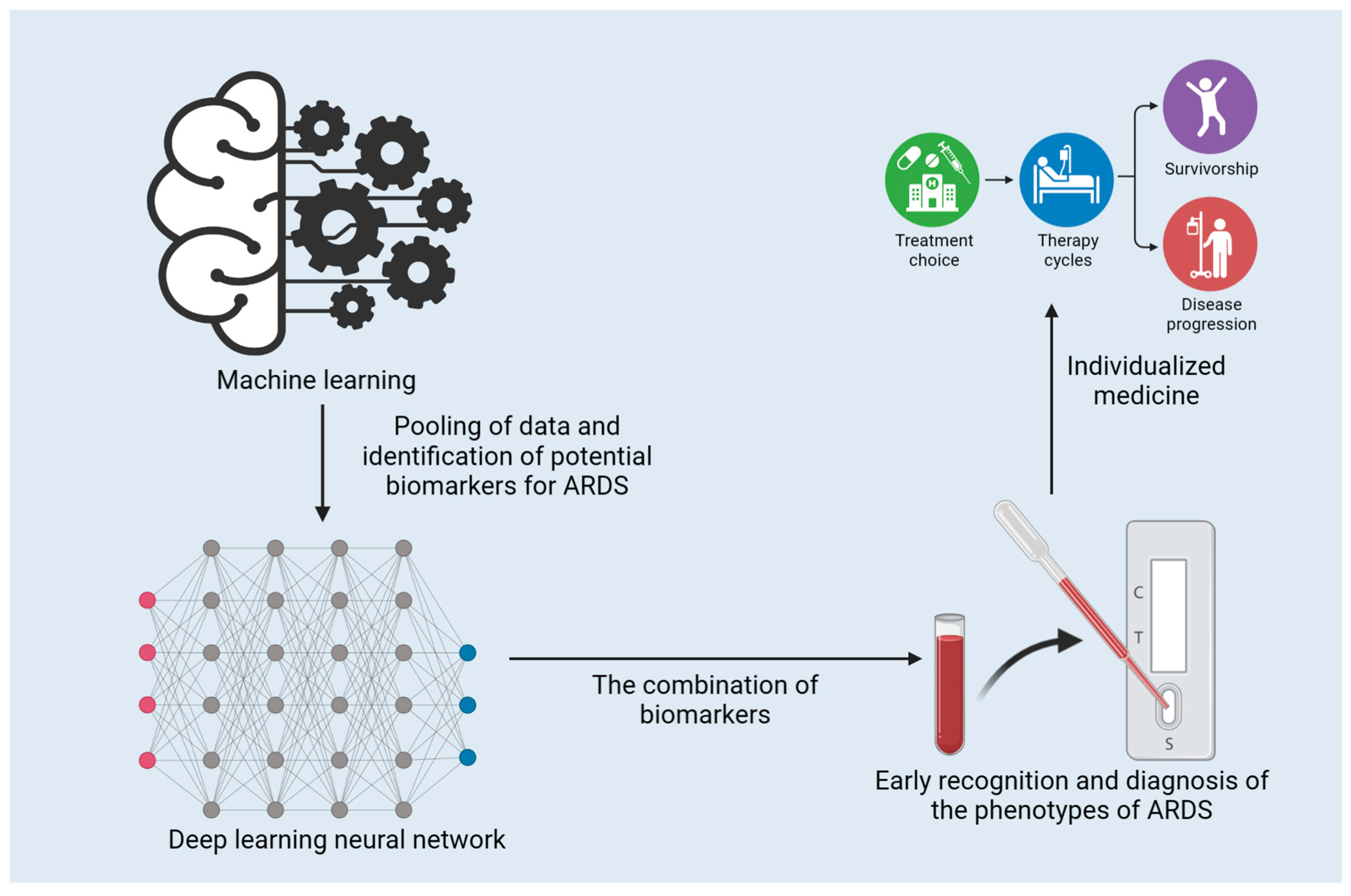
2.7. Machine Learning and ARDS Biomarkers
3. Challenges and Future Directions
3.1. Gaps between Biomarker Discovery and Clinical Utility
3.2. Possible Approaches for Further Research and Development
4. Conclusions
4.1. Summary of Advances in ARDS Biomarkers
4.2. Importance of Continued Research for Improving Diagnosis and Treatment of ARDS
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Matthay, M.A.; Zemans, R.L.; Zimmerman, G.A.; Arabi, Y.M.; Beitler, J.R.; Mercat, A.; Herridge, M.; Randolph, A.G.; Calfee, C.S. Acute respiratory distress syndrome. Nat. Rev. Dis. Primer 2019, 5, 18. [Google Scholar] [CrossRef] [PubMed]
- Gorman, E.A.; O’Kane, C.M.; McAuley, D.F. Acute respiratory distress syndrome in adults: Diagnosis, outcomes, long-term sequelae, and management. Lancet 2022, 400, 1157–1170. [Google Scholar] [CrossRef] [PubMed]
- Wick, K.D.; McAuley, D.F.; Levitt, J.E.; Beitler, J.R.; Annane, D.; Riviello, E.D.; Calfee, C.S.; Matthay, M.A. Promises and challenges of personalized medicine to guide ARDS therapy. Crit. Care Lond. Engl. 2021, 25, 404. [Google Scholar] [CrossRef]
- Wilson, J.G.; Calfee, C. ARDS Subphenotypes: Understanding a Heterogeneous Syndrome. Crit. Care 2020, 24. [Google Scholar] [CrossRef] [PubMed]
- Hu, Q.; Zhang, S.; Yang, Y.; Yao, J.-Q.; Tang, W.-F.; Lyon, C.J.; Hu, T.Y.; Wan, M.-H. Extracellular vesicles in the pathogenesis and treatment of acute lung injury. Mil. Med. Res. 2022, 9, 61. [Google Scholar] [CrossRef]
- Matthay, M.A.; Arabi, Y.M.; Siegel, E.R.; Ware, L.B.; Bos, L.D.J.; Sinha, P.; Beitler, J.R.; Wick, K.D.; Curley, M.A.Q.; Constantin, J.-M.; et al. Phenotypes and personalized medicine in the acute respiratory distress syndrome. Intensive Care Med. 2020, 46, 2136–2152. [Google Scholar] [CrossRef]
- Sathe, N.A.; Morrell, E.D.; Bhatraju, P.K.; Fessler, M.B.; Stapleton, R.D.; Wurfel, M.M.; Mikacenic, C. Alveolar Biomarker Profiles in Subphenotypes of the Acute Respiratory Distress Syndrome. Crit. Care Med. 2023, 51, e13–e18. [Google Scholar] [CrossRef]
- Broman, N.; Rantasärkkä, K.; Feuth, T.; Valtonen, M.; Waris, M.; Hohenthal, U.; Rintala, E.; Karlsson, A.; Marttila, H.; Peltola, V.; et al. IL-6 and other biomarkers as predictors of severity in COVID-19. Ann. Med. 2021, 53, 410–412. [Google Scholar] [CrossRef]
- Galván-Román, J.M.; Rodríguez-García, S.C.; Roy-Vallejo, E.; Marcos-Jiménez, A.; Sánchez-Alonso, S.; Fernández-Díaz, C.; Alcaraz-Serna, A.; Mateu-Albero, T.; Rodríguez-Cortes, P.; Sánchez-Cerrillo, I.; et al. IL-6 serum levels predict severity and response to tocilizumab in COVID-19: An observational study. J. Allergy Clin. Immunol. 2021, 147, 72–80.e8. [Google Scholar] [CrossRef]
- Gubernatorova, E.O.; Gorshkova, E.A.; Polinova, A.I.; Drutskaya, M.S. IL-6: Relevance for immunopathology of SARS-CoV-2. Cytokine Growth Factor Rev. 2020, 53, 13–24. [Google Scholar] [CrossRef]
- Mazzoni, A.; Salvati, L.; Maggi, L.; Capone, M.; Vanni, A.; Spinicci, M.; Mencarini, J.; Caporale, R.; Peruzzi, B.; Antonelli, A.; et al. Impaired immune cell cytotoxicity in severe COVID-19 is IL-6 dependent. J. Clin. Investig. 2020, 130, 4694–4703. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Li, M.; Zhou, Z.; Guan, X.; Xiang, Y. Can we use interleukin-6 (IL-6) blockade for coronavirus disease 2019 (COVID-19)-induced cytokine release syndrome (CRS)? J. Autoimmun. 2020, 111, 102452. [Google Scholar] [CrossRef] [PubMed]
- Elahi, R.; Karami, P.; Heidary, A.H.; Esmaeilzadeh, A. An updated overview of recent advances, challenges, and clinical considerations of IL-6 signaling blockade in severe coronavirus disease 2019 (COVID-19). Int. Immunopharmacol. 2022, 105, 108536. [Google Scholar] [CrossRef] [PubMed]
- Zarrabi, M.; Shahrbaf, M.A.; Nouri, M.; Shekari, F.; Hosseini, S.-E.; Hashemian, S.-M.R.; Aliannejad, R.; Jamaati, H.; Khavandgar, N.; Alemi, H.; et al. Allogenic mesenchymal stromal cells and their extracellular vesicles in COVID-19 induced ARDS: A randomized controlled trial. Stem Cell Res. Ther. 2023, 14, 169. [Google Scholar] [CrossRef]
- McElvaney, O.J.; McEvoy, N.L.; Boland, F.; McElvaney, O.F.; Hogan, G.; Donnelly, K.; Friel, O.; Browne, E.; Fraughen, D.D.; Murphy, M.P.; et al. A randomized, double-blind, placebo-controlled trial of intravenous alpha-1 antitrypsin for ARDS secondary to COVID-19. Med 2022, 3, 233–248.e6. [Google Scholar] [CrossRef]
- Peng, W.; Chang, M.; Wu, Y.; Zhu, W.; Tong, L.; Zhang, G.; Wang, Q.; Liu, J.; Zhu, X.; Cheng, T.; et al. Lyophilized powder of mesenchymal stem cell supernatant attenuates acute lung injury through the IL-6-p-STAT3-p63-JAG2 pathway. Stem Cell Res. Ther. 2021, 12, 216. [Google Scholar] [CrossRef]
- Aisiku, I.; Yamal, J.-M.; Doshi, P.; Benoit, J.S.; Gopinath, S.; Goodman, J.; Robertson, C. Plasma cytokines IL-6, IL-8, and IL-10 are associated with the development of acute respiratory distress syndrome in patients with severe traumatic brain injury. Crit. Care 2016, 20. [Google Scholar] [CrossRef]
- Ronit, A.; Berg, R.M.G.; Bay, J.T.; Haugaard, A.K.; Ahlström, M.G.; Burgdorf, K.S.; Ullum, H.; Rørvig, S.B.; Tjelle, K.; Foss, N.B.; et al. Compartmental immunophenotyping in COVID-19 ARDS: A case series. J. Allergy Clin. Immunol. 2021, 147, 81–91. [Google Scholar] [CrossRef]
- Chen, L.; Wang, G.; Tan, J.; Cao, Y.; Long, X.; Luo, H.; Tang, Q.; Jiang, T.; Wang, W.; Zhou, J. Scoring cytokine storm by the levels of MCP-3 and IL-8 accurately distinguished COVID-19 patients with high mortality. Signal Transduct. Target. Ther. 2020, 5. [Google Scholar] [CrossRef]
- Li, L.; Li, J.; Gao, M.; Fan, H.; Wang, Y.; Xu, X.; Chen, C.; Liu, J.; Kim, J.T.; Aliyari, R.; et al. Interleukin-8 as a Biomarker for Disease Prognosis of Coronavirus Disease-2019 Patients. Front. Immunol. 2021, 11. [Google Scholar] [CrossRef]
- Ma, A.; Zhang, L.; Ye, X.; Chen, J.; Yu, J.; Zhuang, L.; Weng, C.; Petersen, F.; Wang, Z.; Yu, X. High Levels of Circulating IL-8 and Soluble IL-2R Are Associated With Prolonged Illness in Patients With Severe COVID-19. Front. Immunol. 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, R.; Leunig, A.; Pekayvaz, K.; Popp, O.; Joppich, M.; Polewka, V.; Escaig, R.; Anjum, A.; Hoffknecht, M.-L.; Gold, C.; et al. Self-sustaining IL-8 loops drive a prothrombotic neutrophil phenotype in severe COVID-19. JCI Insight 2021, 6, e150862. [Google Scholar] [CrossRef]
- Hashemian, S.-M.R.; Aliannejad, R.; Zarrabi, M.; Soleimani, M.; Vosough, M.; Hosseini, S.-E.; Hossieni, H.; Keshel, S.H.; Naderpour, Z.; Hajizadeh-Saffar, E.; et al. Mesenchymal stem cells derived from perinatal tissues for treatment of critically ill COVID-19-induced ARDS patients: A case series. Stem Cell Res. Ther. 2021, 12, 91. [Google Scholar] [CrossRef] [PubMed]
- Qin, M.; Qiu, Z. Changes in TNF-α, IL-6, IL-10 and VEGF in rats with ARDS and the effects of dexamethasone. Exp. Ther. Med. 2019, 17, 383–387. [Google Scholar] [CrossRef] [PubMed]
- Sun, R.; Jiang, K.; Zeng, C.; Zhu, R.; Chu, H.; Liu, H.; Du, J. Synergism of TNF-α and IFN-β triggers human airway epithelial cells death by apoptosis and pyroptosis. Mol. Immunol. 2023, 153, 160–169. [Google Scholar] [CrossRef] [PubMed]
- Karki, R.; Sharma, B.R.; Tuladhar, S.; Williams, E.P.; Zalduondo, L.; Samir, P.; Zheng, M.; Sundaram, B.; Banoth, B.; Malireddi, R.K.S.; et al. Synergism of TNF-α and IFN-γ triggers inflammatory cell death, tissue damage, and mortality in SARS-CoV-2 infection and cytokine shock syndromes. BioRxiv Prepr. Serv. Biol. 2020, 2020.10.29.361048. [Google Scholar] [CrossRef]
- Leija-Martínez, J.J.; Huang, F.; Del-Río-Navarro, B.E.; Sanchéz-Muñoz, F.; Muñoz-Hernández, O.; Giacoman-Martínez, A.; Hall-Mondragon, M.S.; Espinosa-Velazquez, D. IL-17A and TNF-α as potential biomarkers for acute respiratory distress syndrome and mortality in patients with obesity and COVID-19. Med. Hypotheses 2020, 144, 109935. [Google Scholar] [CrossRef]
- Schmidt, E.P.; Yang, Y.; Janssen, W.J.; Gandjeva, A.; Perez, M.J.; Barthel, L.; Zemans, R.L.; Bowman, J.C.; Koyanagi, D.E.; Yunt, Z.X.; et al. The pulmonary endothelial glycocalyx regulates neutrophil adhesion and lung injury during experimental sepsis. Nat. Med. 2012, 18, 1217–1223. [Google Scholar] [CrossRef]
- Chen, D.; Chen, C.; Xiao, X.; Huang, Z.; Huang, X.; Yao, W. TNF-α Induces Neutrophil Apoptosis Delay and Promotes Intestinal Ischemia-Reperfusion-Induced Lung Injury through Activating JNK/FoxO3a Pathway. Oxid. Med. Cell. Longev. 2021, 2021, 1–13. [Google Scholar] [CrossRef]
- Mortaz, E.; Tabarsi, P.; Jamaati, H.; Dalil Roofchayee, N.; Dezfuli, N.K.; Hashemian, S.M.; Moniri, A.; Marjani, M.; Malekmohammad, M.; Mansouri, D.; et al. Increased Serum Levels of Soluble TNF-α Receptor Is Associated With ICU Mortality in COVID-19 Patients. Front. Immunol. 2021, 12, 592727. [Google Scholar] [CrossRef]
- Pooladanda, V.; Thatikonda, S.; Bale, S.; Pattnaik, B.; Sigalapalli, D.K.; Bathini, N.B.; Singh, S.B.; Godugu, C. Nimbolide protects against endotoxin-induced acute respiratory distress syndrome by inhibiting TNF-α mediated NF-κB and HDAC-3 nuclear translocation. Cell Death Dis. 2019, 10, 81. [Google Scholar] [CrossRef] [PubMed]
- Kowalska-Kępczyńska, A.; Mleczko, M.; Domerecka, W.; Krasowska, D.; Donica, H. Assessment of Immune Cell Activation in Pemphigus. Cells 2022, 11, 1912. [Google Scholar] [CrossRef] [PubMed]
- Domerecka, W.; Kowalska-Kępczyńska, A.; Homa-Mlak, I.; Michalak, A.; Mlak, R.; Mazurek, M.; Cichoż-Lach, H.; Małecka-Massalska, T. The Usefulness of Extended Inflammation Parameters and Systemic Inflammatory Response Markers in the Diagnostics of Autoimmune Hepatitis. Cells 2022, 11, 2554. [Google Scholar] [CrossRef] [PubMed]
- Dennison, D.; Al Khabori, M.; Al Mamari, S.; Aurelio, A.; Al Hinai, H.; Al Maamari, K.; Alshekaili, J.; Al Khadouri, G. Circulating activated neutrophils in COVID-19: An independent predictor for mechanical ventilation and death. Int. J. Infect. Dis. 2021, 106, 155–159. [Google Scholar] [CrossRef]
- Kwiecień, I.; Rutkowska, E.; Kulik, K.; Kłos, K.; Plewka, K.; Raniszewska, A.; Rzepecki, P.; Chciałowski, A. Neutrophil Maturation, Reactivity and Granularity Research Parameters to Characterize and Differentiate Convalescent Patients from Active SARS-CoV-2 Infection. Cells 2021, 10, 2332. [Google Scholar] [CrossRef]
- Kim, H.J.; Jeong, M.; Jang, S. Molecular Characteristics of RAGE and Advances in Small-Molecule Inhibitors. Int. J. Mol. Sci. 2021, 22, 6904. [Google Scholar] [CrossRef]
- Chiappalupi, S.; Salvadori, L.; Donato, R.; Riuzzi, F.; Sorci, G. Hyperactivated RAGE in Comorbidities as a Risk Factor for Severe COVID-19—The Role of RAGE-RAS Crosstalk. Biomolecules 2021, 11, 876. [Google Scholar] [CrossRef]
- Bonda, W.L.M.; Fournet, M.; Zhai, R.; Lutz, J.; Blondonnet, R.; Bourgne, C.; Leclaire, C.; Saint-Béat, C.; Theilliere, C.; Belville, C.; et al. Receptor for Advanced Glycation End-Products Promotes Activation of Alveolar Macrophages through the NLRP3 Inflammasome/TXNIP Axis in Acute Lung Injury. Int. J. Mol. Sci. 2022, 23, 11659. [Google Scholar] [CrossRef]
- Lim, A.; Radujkovic, A.; Weigand, M.; Merle, U. Soluble receptor for advanced glycation end products (sRAGE) as a biomarker of COVID-19 disease severity and indicator of the need for mechanical ventilation, ARDS and mortality. Ann. Intensive Care 2021, 11. [Google Scholar] [CrossRef]
- Jabaudon, M.; Blondonnet, R.; Pereira, B.; Cartin-Ceba, R.; Lichtenstern, C.; Mauri, T.; Determann, R.M.; Drabek, T.; Hubmayr, R.D.; Gajic, O.; et al. Plasma sRAGE is independently associated with increased mortality in ARDS: A meta-analysis of individual patient data. Intensive Care Med. 2018, 44, 1388–1399. [Google Scholar] [CrossRef]
- Singh, H.; Agrawal, D. Therapeutic potential of targeting the receptor for advanced glycation end products (RAGE) by small molecule inhibitors. Drug Dev. Res. 2022, 83, 1257–1269. [Google Scholar] [CrossRef]
- Xiong, X.; Dou, J.; Shi, J.; Ren, Y.; Wang, C.; Zhang, Y.; Cui, Y. RAGE inhibition alleviates lipopolysaccharides-induced lung injury via directly suppressing autophagic apoptosis of type II alveolar epithelial cells. Respir. Res. 2023, 24, 24. [Google Scholar] [CrossRef] [PubMed]
- Peukert, K.; Seeliger, B.; Fox, M.; Feuerborn, C.; Sauer, A.; Schuss, P.; Schneider, M.; David, S.; Welte, T.; Putensen, C.; et al. SP-D Serum Levels Reveal Distinct Epithelial Damage in Direct Human ARDS. J. Clin. Med. 2021, 10, 737. [Google Scholar] [CrossRef] [PubMed]
- Agustama, A.; Surgean Veterini, A.; Utariani, A. Correlation of Surfactant Protein-D (SP-D) Serum Levels with ARDS Severity and Mortality in Covid-19 Patients in Indonesia. Acta Medica Acad. 2022, 51, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Jayadi; Airlangga, P.; Kusuma, E.; Waloejo, C.; Salinding, A.; Lestari, P. Correlation between serum surfactant protein-D level with respiratory compliance and acute respiratory distress syndrome in critically ill COVID-19 Patients: A retrospective observational study. Int. J. Crit. Illn. Inj. Sci. 2022, 12, 204. [Google Scholar] [CrossRef] [PubMed]
- Attias Cohen, S.; Kingma, P.S.; Whitsett, J.A.; Goldbart, R.; Traitel, T.; Kost, J. SP-D loaded PLGA nanoparticles as drug delivery system for prevention and treatment of premature infant’s lung diseases. Int. J. Pharm. 2020, 585, 119387. [Google Scholar] [CrossRef]
- García-Mouton, C.; Hidalgo, A.; Arroyo, R.; Echaide, M.; Cruz, A.; Pérez-Gil, J. Pulmonary Surfactant and Drug Delivery: An Interface-Assisted Carrier to Deliver Surfactant Protein SP-D Into the Airways. Front. Bioeng. Biotechnol. 2020, 8, 613276. [Google Scholar] [CrossRef]
- Ghati, A.; Dam, P.; Tasdemir, D.; Kati, A.; Sellami, H.; Sezgin, G.C.; Ildiz, N.; Franco, O.L.; Mandal, A.K.; Ocsoy, I. Exogenous pulmonary surfactant: A review focused on adjunctive therapy for severe acute respiratory syndrome coronavirus 2 including SP-A and SP-D as added clinical marker. Curr. Opin. Colloid Interface Sci. 2021, 51, 101413. [Google Scholar] [CrossRef]
- Salvioni, L.; Testa, F.; Sulejmani, A.; Pepe, F.; Giorgio Lovaglio, P.; Berta, P.; Dominici, R.; Leoni, V.; Prosperi, D.; Vittadini, G.; et al. Surfactant protein D (SP-D) as a biomarker of SARS-CoV-2 infection. Clin. Chim. Acta Int. J. Clin. Chem. 2022, 537, 140–145. [Google Scholar] [CrossRef]
- Tiezzi, M.; Morra, S.; Seminerio, J.; Van Muylem, A.; Godefroid, A.; Law-Weng-Sam, N.; Van Praet, A.; Corbière, V.; Orte Cano, C.; Karimi, S.; et al. SP-D and CC-16 Pneumoproteins’ Kinetics and Their Predictive Role During SARS-CoV-2 Infection. Front. Med. 2021, 8, 761299. [Google Scholar] [CrossRef]
- Almuntashiri, S.; Chase, A.; Sikora, A.; Zhang, D. Validation of Prognostic Club Cell Secretory Protein (CC16) Cut-point in an Independent ALTA Cohort. Biomark. Insights 2023, 18, 11772719231156308. [Google Scholar] [CrossRef] [PubMed]
- Greven, J.; Vollrath, J.T.; Bläsius, F.; He, Z.; Bolierakis, E.; Horst, K.; Störmann, P.; Nowak, A.J.; Simic, M.; Marzi, I.; et al. Club cell protein (CC)16 as potential lung injury marker in a porcine 72 h polytrauma model. Eur. J. Trauma Emerg. Surg. Off. Publ. Eur. Trauma Soc. 2022, 48, 4719–4726. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Zhu, Y.; Almuntashiri, S.; Wang, X.; Somanath, P.R.; Owen, C.A.; Zhang, D. Extracellular vesicle-encapsulated CC16 as novel nanotherapeutics for treatment of acute lung injury. Mol. Ther. 2023, 31, 1346–1364. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.-J.; Li, Y.; Wang, D.-Y.; Yuan, H.-T. ARB might be superior to ACEI for treatment of hypertensive COVID-19 patients. J. Cell. Mol. Med. 2021, 25, 11031–11034. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Q.; Huang, G.; Li, S.; Wen, F. Diagnostic and prognostic value of Ang-2 in ARDS: A systemic review and meta-analysis. Expert Rev. Respir. Med. 2023, 1–10. [Google Scholar] [CrossRef]
- Rosenberger, C.M.; Wick, K.D.; Zhuo, H.; Wu, N.; Chen, Y.; Kapadia, S.B.; Guimaraes, A.; Chang, D.; Choy, D.F.; Chen, H.; et al. Early plasma angiopoietin-2 is prognostic for ARDS and mortality among critically ill patients with sepsis. Crit. Care 2023, 27, 234. [Google Scholar] [CrossRef]
- Morganstein, T.; Haidar, Z.; Trivlidis, J.; Azuelos, I.; Huang, M.J.; Eidelman, D.H.; Baglole, C.J. Involvement of the ACE2/Ang-(1-7)/MasR Axis in Pulmonary Fibrosis: Implications for COVID-19. Int. J. Mol. Sci. 2021, 22, 12955. [Google Scholar] [CrossRef]
- Cheng, H.; Wang, Y.; Wang, G.-Q. Organ-protective effect of angiotensin-converting enzyme 2 and its effect on the prognosis of COVID-19. J. Med. Virol. 2020, 92, 726–730. [Google Scholar] [CrossRef]
- Huang, W.; Cao, Y.; Liu, Y.; Ping, F.; Shang, J.; Zhang, Z.; Li, Y. Activating Mas receptor protects human pulmonary microvascular endothelial cells against LPS-induced apoptosis via the NF-kB p65/P53 feedback pathways. J. Cell. Physiol. 2019, 234, 12865–12875. [Google Scholar] [CrossRef]
- Collins, K.L.; Younis, U.S.; Tanyaratsrisakul, S.; Polt, R.; Hay, M.; Mansour, H.M.; Ledford, J.G. Angiotensin-(1-7) Peptide Hormone Reduces Inflammation and Pathogen Burden during Mycoplasma pneumoniae Infection in Mice. Pharmaceutics 2021, 13, 1614. [Google Scholar] [CrossRef]
- Li, F.; Yin, R.; Guo, Q. Circulating angiopoietin-2 and the risk of mortality in patients with acute respiratory distress syndrome: A systematic review and meta-analysis of 10 prospective cohort studies. Ther. Adv. Respir. Dis. 2020, 14, 1753466620905274. [Google Scholar] [CrossRef]
- Parke, R.; Bihari, S.; Dixon, D.-L.; Gilder, E.; Cavallaro, E.; McGuinness, S.; Bersten, A.D. Fluid resuscitation associated with elevated angiopoietin-2 and length of mechanical ventilation after cardiac surgery. Crit. Care Resusc. J. Australas. Acad. Crit. Care Med. 2018, 20, 198–208. [Google Scholar] [CrossRef]
- Osburn, W.; Smith, K.; Yanek, L.; Amat-Alcaron, N.; Thiemann, D.; Cox, A.; Leucker, T.; Lowenstein, C. Markers of endothelial cell activation are associated with the severity of pulmonary disease in COVID-19. PLoS ONE 2022, 17. [Google Scholar] [CrossRef] [PubMed]
- Seibert, F.S.; Blazquez-Navarro, A.; Hölzer, B.; Doevelaar, A.A.N.; Nusshag, C.; Merle, U.; Morath, C.; Zgoura, P.; Dittmer, R.; Schneppenheim, S.; et al. Effect of plasma exchange on COVID-19 associated excess of von Willebrand factor and inflammation in critically ill patients. Sci. Rep. 2022, 12, 4801. [Google Scholar] [CrossRef] [PubMed]
- Tóth, E.; Beinrohr, L.; Gubucz, I.; Szabó, L.; Tenekedjiev, K.; Nikolova, N.; Nagy, A.; Hidi, L.; Sótonyi, P.; Szikora, I.; et al. Fibrin to von Willebrand factor ratio in arterial thrombi is associated with plasma levels of inflammatory biomarkers and local abundance of extracellular DNA. Thromb. Res. 2021, 209, 8–15. [Google Scholar] [CrossRef]
- Wibowo, A.; Pranata, R.; Lim, M.; Akbar, M.R.; Martha, J.W. Endotheliopathy marked by high von Willebrand factor (vWF) antigen in COVID-19 is associated with poor outcome: A systematic review and meta-analysis. Int. J. Infect. Dis. 2021, 117, 267–273. [Google Scholar] [CrossRef]
- Gaudet, A.; Portier, L.; Mathieu, D.; Hureau, M.; Tsicopoulos, A.; Lassalle, P.; De Freitas Caires, N. Cleaved endocan acts as a biologic competitor of endocan in the control of ICAM-1-dependent leukocyte diapedesis. J. Leukoc. Biol. 2020, 107, 833–841. [Google Scholar] [CrossRef]
- Williams, J.G.; Jones, R.L.; Yunger, T.L.; Lahni, P.M.; Yehya, N.; Varisco, B.M. Comparison of 16 Pediatric Acute Respiratory Distress Syndrome-Associated Plasma Biomarkers With Changing Lung Injury Severity. Pediatr. Crit. Care Med. 2023; Ahead of Print. [Google Scholar] [CrossRef]
- Li, G.; Jiang, X.; Liang, X.; Hou, Y.; Zang, J.; Zhu, B.; Jia, C.; Niu, K.; Liu, X.; Xu, X.; et al. BAP31 regulates the expression of ICAM-1/VCAM-1 via MyD88/NF-κB pathway in acute lung injury mice model. Life Sci. 2023, 313, 121310. [Google Scholar] [CrossRef]
- He, B.; Geng, S.; Zhou, W.; Rui, Y.; Mu, X.; Zhang, C.; You, Q.; Su, X. MMI-0100 ameliorates lung inflammation in a mouse model of acute respiratory distress syndrome by reducing endothelial expression of ICAM-1. Drug Des. Devel. Ther. 2018, 12, 4253–4260. [Google Scholar] [CrossRef]
- Su, L.; Sun, Q.; Cai, W.; Qi, Y. Influenced CD cells and ICAM-1 by pulmonary surfactant combined with high-frequency oscillatory ventilation and its effects on immune function in children with neonatal respiratory distress syndrome. Cell. Mol. Biol. Noisy--Gd. Fr. 2020, 66, 32–38. [Google Scholar] [CrossRef]
- Yao, M.-Y.; Zhang, W.-H.; Ma, W.-T.; Liu, Q.-H.; Xing, L.-H.; Zhao, G.-F. Long non-coding RNA MALAT1 exacerbates acute respiratory distress syndrome by upregulating ICAM-1 expression via microRNA-150-5p downregulation. Aging 2020, 12, 6570–6585. [Google Scholar] [CrossRef] [PubMed]
- Spadaro, S.; Fogagnolo, A.; Campo, G.; Zucchetti, O.; Verri, M.; Ottaviani, I.; Tunstall, T.; Grasso, S.; Scaramuzzo, V.; Murgolo, F.; et al. Markers of endothelial and epithelial pulmonary injury in mechanically ventilated COVID-19 ICU patients. Crit. Care 2020, 25. [Google Scholar] [CrossRef] [PubMed]
- Morrow, G.B.; Mutch, N.J. Past, Present, and Future Perspectives of Plasminogen Activator Inhibitor 1 (PAI-1). Semin. Thromb. Hemost. 2023, 49, 305–313. [Google Scholar] [CrossRef]
- Jiang, S.; Wang, Y.; Chen, L.; Mu, H.; Meaney, C.; Fan, Y.; Pillay, J.; Wang, H.; Zhang, J.; Pan, S.; et al. PAI-1 genetic polymorphisms influence septic patients’ outcomes by regulating neutrophil activity. Chin. Med. J. 2023. [Google Scholar] [CrossRef]
- Han, M.; Pandey, D. ZMPSTE24 Regulates SARS-CoV-2 Spike Protein-enhanced Expression of Endothelial PAI-1. Am. J. Respir. Cell Mol. Biol. 2021, 65, 300–308. [Google Scholar] [CrossRef]
- Liu, B.; Wu, Y.; Wang, Y.; Cheng, Y.; Yao, L.; Liu, Y.; Qian, H.; Yang, H.; Shen, F. NF-κB p65 Knock-down inhibits TF, PAI-1 and promotes activated protein C production in lipopolysaccharide-stimulated alveolar epithelial cells type II. Exp. Lung Res. 2018, 44, 241–251. [Google Scholar] [CrossRef]
- Suzuki, K.; Okada, H.; Takemura, G.; Takada, C.; Tomita, H.; Yano, H.; Muraki, I.; Zaikokuji, R.; Kuroda, A.; Fukuda, H.; et al. Recombinant thrombomodulin protects against LPS-induced acute respiratory distress syndrome via preservation of pulmonary endothelial glycocalyx. Br. J. Pharmacol. 2020, 177, 4021–4033. [Google Scholar] [CrossRef]
- Kono, H.; Hosomura, N.; Amemiya, H.; Kawaida, H.; Furuya, S.; Shoda, K.; Akaike, H.; Kawaguchi, Y.; Ichikawa, D. Recombinant Human Thrombomodulin Reduces Mortality and Acute Lung Injury Caused by Septic Peritonitis in Rats. ImmunoHorizons 2023, 7, 159–167. [Google Scholar] [CrossRef]
- Liu, Z.; Li, Y.; Zhao, Q.; Kang, Y. Association and predictive value of soluble thrombomodulin with mortality in patients with acute respiratory distress syndrome: Systematic review and meta-analysis. Ann. Transl. Med. 2023, 11, 181. [Google Scholar] [CrossRef]
- Monteiro, A.C.C.; Flori, H.; Dahmer, M.K.; Sim, M.S.; Quasney, M.W.; Curley, M.A.Q.; Matthay, M.A.; Sapru, A.; BALI Study Investigators of the Pediatric Acute Lung Injury and Sepsis Investigators (PALISI) Network. Thrombomodulin is associated with increased mortality and organ failure in mechanically ventilated children with acute respiratory failure: Biomarker analysis from a multicenter randomized controlled trial. Crit. Care Lond. Engl. 2021, 25, 271. [Google Scholar] [CrossRef]
- Hirata, N.; Ngo, D.T.; Phan, P.H.; Ainai, A.; Phung, T.T.B.; Ta, T.A.; Takasaki, J.; Kawachi, S.; Nunoi, H.; Nakajima, N.; et al. Recombinant human thrombomodulin for pneumonia-induced severe ARDS complicated by DIC in children: A preliminary study. J. Anesth. 2021, 35, 638–645. [Google Scholar] [CrossRef] [PubMed]
- Huang, I.; Pranata, R.; Lim, M.A.; Oehadian, A.; Alisjahbana, B. C-reactive protein, procalcitonin, D-dimer, and ferritin in severe coronavirus disease-2019: A meta-analysis. Ther. Adv. Respir. Dis. 2020, 14, 1753466620937175. [Google Scholar] [CrossRef] [PubMed]
- Nasif, W.A.; El-Moursy Ali, A.S.; Hasan Mukhtar, M.; Alhuzali, A.M.H.; Yahya Alnashri, Y.A.; Ahmed Gadah, Z.I.; Edrees, E.A.A.; Albarakati, H.A.M.; Muhji Aloufi, H.S. Elucidating the Correlation of D-Dimer Levels with COVID-19 Severity: A Scoping Review. Anemia 2022, 2022, 9104209. [Google Scholar] [CrossRef] [PubMed]
- Vidali, S.; Morosetti, D.; Cossu, E.; Luisi, M.L.E.; Pancani, S.; Semeraro, V.; Consales, G. D-dimer as an indicator of prognosis in SARS-CoV-2 infection: A systematic review. ERJ Open Res. 2020, 6, 00260–02020. [Google Scholar] [CrossRef]
- Ye, W.; Chen, G.; Li, X.; Lan, X.; Ji, C.; Hou, M.; Zhang, D.; Zeng, G.; Wang, Y.; Xu, C.; et al. Dynamic changes of D-dimer and neutrophil-lymphocyte count ratio as prognostic biomarkers in COVID-19. Respir. Res. 2020, 21, 169. [Google Scholar] [CrossRef]
- Tóth, K.; Fresilli, S.; Paoli, N.; Maiucci, G.; Salvioni, M.; Kotani, Y.; Katzenschlager, S.; Weigand, M.A.; Landoni, G. D-dimer levels in non-COVID-19 ARDS and COVID-19 ARDS patients: A systematic review with meta-analysis. PLoS ONE 2023, 18, e0277000. [Google Scholar] [CrossRef]
- Yovchevska, I.P.; Trenovski, A.B.; Atanasova, M.H.; Georgiev, M.N.; Tafradjiiska-Hadjiolova, R.K.; Lazarov, S.D.; Yovchevski, P.H. Platelet Distribution Width and Increased D-Dimer at Admission Predicts Subsequent Development of ARDS in COVID-19 Patients. Pathophysiol. Off. J. Int. Soc. Pathophysiol. 2022, 29, 233–242. [Google Scholar] [CrossRef]
- Guizani, I.; Fourti, N.; Zidi, W.; Feki, M.; Allal-Elasmi, M. SARS-CoV-2 and pathological matrix remodeling mediators. Inflamm. Res. 2021, 70, 847–858. [Google Scholar] [CrossRef]
- D’Avila-Mesquita, C.; Couto, A.E.; Campos, L.C.; Vasconcelos, T.F.; Michelon-Barbosa, J.; Corsi, C.; Mestriner, F.; Petroski-Moraes, B.C.; Garbellini-Diab, M.J.; Couto, D.M.S.; et al. MMP-2 and MMP-9 levels in plasma are altered and associated with mortality in COVID-19 patients. Biomed. Pharmacother. 2021, 142, 112067. [Google Scholar] [CrossRef]
- Ueland, T.; Holter, J.; Holten, A.; Müller, K.; Lind, A.; Bekken, G.K.; Dudman, S.; Aukrust, P.; Dyrhol-Riise, A.; Heggelund, L. Distinct and early increase in circulating MMP-9 in COVID-19 patients with respiratory failure. J. Infect. 2020, 81, e41–e43. [Google Scholar] [CrossRef] [PubMed]
- Lerum, T.V.; Maltzahn, N.; Aukrust, P.; Trøseid, M.; Henriksen, K.N.; Kåsine, T.; Dyrhol-Riise, A.; Stiksrud, B.; Haugli, M.; Blomberg, B.; et al. Persistent pulmonary pathology after COVID-19 is associated with high viral load, weak antibody response, and high levels of matrix metalloproteinase-9. Sci. Rep. 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- da Silva-Neto, P.V.; do Valle, V.B.; Fuzo, C.; Fernandes, T.M.; Toro, D.M.; Fraga-Silva, T.F.C.; Basile, P.A.; de Carvalho, J.C.S.; Pimentel, V.E.; Pérez, M.; et al. Matrix Metalloproteinases on Severe COVID-19 Lung Disease Pathogenesis: Cooperative Actions of MMP-8/MMP-2 Axis on Immune Response through HLA-G Shedding and Oxidative Stress. Biomolecules 2022, 12, 604. [Google Scholar] [CrossRef] [PubMed]
- Almuntashiri, S.; Jones, T.W.; Wang, X.; Sikora, A.; Zhang, D. Plasma TIMP-1 as a sex-specific biomarker for acute lung injury. Biol. Sex Differ. 2022, 13. [Google Scholar] [CrossRef]
- Chernikov, I.V.; Staroseletz, Y.; Tatarnikova, I.; Sen’kova, A.; Savin, I.; Markov, A.; Logashenko, E.; Chernolovskaya, E.; Zenkova, M.; Vlassov, V. siRNA-Mediated Timp1 Silencing Inhibited the Inflammatory Phenotype during Acute Lung Injury. Int. J. Mol. Sci. 2023, 24, 1641. [Google Scholar] [CrossRef]
- Toufekoula, C.; Papadakis, V.; Tsaganos, T.; Routsi, C.; Orfanos, S.E.; Kotanidou, A.; Carrer, D.-P.; Raftogiannis, M.; Baziaka, F.; Giamarellos-Bourboulis, E.J. Compartmentalization of lipid peroxidation in sepsis by multidrug-resistant gram-negative bacteria: Experimental and clinical evidence. Crit. Care 2013, 17, R6. [Google Scholar] [CrossRef]
- Ma, A.; Feng, Z.; Li, Y.; Wu, Q.; Xiong, H.; Dong, M.; Cheng, J.; Wang, Z.; Yang, J.; Kang, Y. Ferroptosis-related signature and immune infiltration characterization in acute lung injury/acute respiratory distress syndrome. Respir. Res. 2023, 24, 154. [Google Scholar] [CrossRef]
- Liu, P.; Feng, Y.; Li, H.; Chen, X.; Wang, G.; Xu, S.; Li, Y.; Zhao, L. Ferrostatin-1 alleviates lipopolysaccharide-induced acute lung injury via inhibiting ferroptosis. Cell. Mol. Biol. Lett. 2020, 25, 10. [Google Scholar] [CrossRef]
- Li, J.; Deng, S.; Li, J.; Li, L.; Zhang, F.; Zou, Y.; Wu, D.; Xu, Y. Obacunone alleviates ferroptosis during lipopolysaccharide-induced acute lung injury by upregulating Nrf2-dependent antioxidant responses. Cell. Mol. Biol. Lett. 2022, 27, 29. [Google Scholar] [CrossRef]
- Bhattarai, S.; Gupta, A.; Ali, E.; Ali, M.; Riad, M.; Adhikari, P.; Mostafa, J.A. Can Big Data and Machine Learning Improve Our Understanding of Acute Respiratory Distress Syndrome? Cureus 2021, 13, e13529. [Google Scholar] [CrossRef]
- Lam, C.; Thapa, R.; Maharjan, J.; Rahmani, K.; Tso, C.F.; Singh, N.P.; Casie Chetty, S.; Mao, Q. Multitask Learning With Recurrent Neural Networks for Acute Respiratory Distress Syndrome Prediction Using Only Electronic Health Record Data: Model Development and Validation Study. JMIR Med. Inform. 2022, 10, e36202. [Google Scholar] [CrossRef] [PubMed]
- Maddali, M.V.; Churpek, M.; Pham, T.; Rezoagli, E.; Zhuo, H.; Zhao, W.; He, J.; Delucchi, K.; Wang, C.; Wickersham, N.; et al. Validation and utility of ARDS subphenotypes identified by machine-learning models using clinical data: An observational, multicohort, retrospective analysis. Lancet Respir. Med. 2022. [CrossRef] [PubMed]
- Sinha, P.; Churpek, M.; Calfee, C. Machine Learning Classifier Models Can Identify Acute Respiratory Distress Syndrome Phenotypes Using Readily Available Clinical Data. 2020. Available online: https://www.semanticscholar.org/paper/3a5c4e49255647b55f75fc0e1d162b81983501ff (accessed on 3 March 2023).
- Afshar, M.; Joyce, C.; Oakey, A.; Formanek, P.; Yang, P.; Churpek, M.; Cooper, R.; Price, R.; Zelisko, S.; Dligach, D. A Computable Phenotype for Acute Respiratory Distress Syndrome Using Natural Language Processing and Machine Learning. AMIA Annu. Symp. Proc. AMIA Symp. 2018, 2018, 157–165. [Google Scholar] [PubMed]
- Gattinoni, L.; Chiumello, D.; Caironi, P.; Busana, M.; Romitti, F.; Brazzi, L.; Camporota, L. COVID-19 pneumonia: Different respiratory treatments for different phenotypes? Intensive Care Med. 2020, 46, 1099–1102. [Google Scholar] [CrossRef] [PubMed]
- Bai, Y.; Xia, J.; Huang, X.; Chen, S.; Zhan, Q. Using machine learning for the early prediction of sepsis-associated ARDS in the ICU and identification of clinical phenotypes with differential responses to treatment. Front. Physiol. 2022, 13, 1050849. [Google Scholar] [CrossRef]
- Calabrese, F.; Pezzuto, F.; Fortarezza, F.; Boscolo, A.; Lunardi, F.; Giraudo, C.; Cattelan, A.; Del Vecchio, C.; Lorenzoni, G.; Vedovelli, L.; et al. Machine learning-based analysis of alveolar and vascular injury in SARS-CoV-2 acute respiratory failure. J. Pathol. 2021, 254, 173–184. [Google Scholar] [CrossRef]
- Levine, A.R.; Shanholtz, C.B. I, DOCTOR: The role of machine learning in phenotyping ARDS. EBioMedicine 2022, 75, 103770. [Google Scholar] [CrossRef]
- McNicholas, B.; Madden, M.G.; Laffey, J.G. Machine Learning Classifier Models: The Future for Acute Respiratory Distress Syndrome Phenotyping? Am. J. Respir. Crit. Care Med. 2020, 202, 919–920. [Google Scholar] [CrossRef]
- Bime, C.; Camp, S.; Casanova, N.; Oita, R.; Ndukum, J.; Lynn, H.; Garcia, J.G.N. The acute respiratory distress syndrome biomarker pipeline: Crippling gaps between discovery and clinical utility. Transl. Res. 2020, 226, 105–115. [Google Scholar] [CrossRef]
- Hernández-Beeftink, T.; Guillen-Guio, B.; Villar, J.; Flores, C. Genomics and the Acute Respiratory Distress Syndrome: Current and Future Directions. Int. J. Mol. Sci. 2019, 20, 4004. [Google Scholar] [CrossRef]
- Reilly, J.; Christie, J.; Meyer, N. Fifty Years of Research in ARDS. Genomic Contributions and Opportunities. Am. J. Respir. Crit. Care Med. 2017, 196, 1113–1121. [Google Scholar] [CrossRef] [PubMed]
- van der Zee, P.A.; Rietdijk, W.; Somhorst, P.; Endeman, H.; Gommers, D. A systematic review of biomarkers multivariately associated with acute respiratory distress syndrome development and mortality. Crit. Care 2020, 24. [Google Scholar] [CrossRef] [PubMed]
- Bime, C.; Casanova, N.G.; Nikolich-Zugich, J.; Knox, K.S.; Camp, S.M.; Garcia, J.G.N. Strategies to DAMPen COVID-19-mediated lung and systemic inflammation and vascular injury. Transl. Res. J. Lab. Clin. Med. 2021, 232, 37–48. [Google Scholar] [CrossRef] [PubMed]
- Capelozzi, V.; Allen, T.; Beasley, M.; Cagle, P.; Guinee, D.; Hariri, L.; Husain, A.; Jain, D.; Lantuejoul, S.; Larsen, B.T.; et al. Molecular and Immune Biomarkers in Acute Respiratory Distress Syndrome: A Perspective From Members of the Pulmonary Pathology Society. Arch. Pathol. Lab. Med. 2017, 141, 1719–1727. [Google Scholar] [CrossRef] [PubMed]
- Lynn, H.; Sun, X.; Casanova, N.; Gonzales-Garay, M.; Bime, C.; Garcia, J.G.N. Genomic and Genetic Approaches to Deciphering Acute Respiratory Distress Syndrome Risk and Mortality. Antioxid. Redox Signal. 2019. [Google Scholar] [CrossRef] [PubMed]
- Bime, C.; Casanova, N.; Oita, R.; Ndukum, J.; Lynn, H.; Camp, S.; Lussier, Y.; Abraham, I.; Carter, D.; Miller, E.; et al. Development of a biomarker mortality risk model in acute respiratory distress syndrome. Crit. Care 2019, 23. [Google Scholar] [CrossRef]
- Quijada, H.; Bermudez, T.; Kempf, C.L.; Valera, D.; Garcia, A.N.; Camp, S.; Song, J.H.; Franco, E.; Burt, J.K.; Sun, B.L.; et al. Endothelial eNAMPT amplifies pre-clinical acute lung injury: Efficacy of an eNAMPT-neutralising monoclonal antibody. Eur. Respir. J. 2020, 57. [Google Scholar] [CrossRef]
- Sun, X.; Sun, B.L.; Babicheva, A.; Vanderpool, R.; Oita, R.; Casanova, N.; Tang, H.; Gupta, A.; Lynn, H.; Gupta, G.; et al. Direct eNAMPT Involvement in Pulmonary Hypertension and Vascular Remodeling: Transcriptional Regulation by SOX and HIF2α. Am. J. Respir. Cell Mol. Biol. 2020. [Google Scholar] [CrossRef]
- Oita, R.C.; Camp, S.M.; Ma, W.; Ceco, E.; Harbeck, M.; Singleton, P.; Messana, J.; Sun, X.; Wang, T.; Garcia, J.G.N. Novel Mechanism for Nicotinamide Phosphoribosyltransferase Inhibition of TNF-α-mediated Apoptosis in Human Lung Endothelial Cells. Am. J. Respir. Cell Mol. Biol. 2018, 59, 36–44. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Routinely Tested | Commonly Tested | Less Frequently Tested | Research-Specific | |
|---|---|---|---|---|
| Inflammatory biomarkers | IL-6, IL-8, TNF-α | ICAM-1 | ||
| Alveolar epithelial injury biomarkers | SP-D, CCSP | RAGE | ||
| Endothelial injury biomarkers | vWF | Ang-2 | ||
| Coagulation/fibrinolysis biomarkers | D-dimer | PAI-1, Thrombomodulin | ||
| Extracellular matrix turnover biomarkers | MMP-9, TIMP-1 | |||
| Oxidative stress biomarkers | MDA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ge, R.; Wang, F.; Peng, Z. Advances in Biomarkers for Diagnosis and Treatment of ARDS. Diagnostics 2023, 13, 3296. https://doi.org/10.3390/diagnostics13213296
Ge R, Wang F, Peng Z. Advances in Biomarkers for Diagnosis and Treatment of ARDS. Diagnostics. 2023; 13(21):3296. https://doi.org/10.3390/diagnostics13213296
Chicago/Turabian StyleGe, Ruiqi, Fengyun Wang, and Zhiyong Peng. 2023. "Advances in Biomarkers for Diagnosis and Treatment of ARDS" Diagnostics 13, no. 21: 3296. https://doi.org/10.3390/diagnostics13213296
APA StyleGe, R., Wang, F., & Peng, Z. (2023). Advances in Biomarkers for Diagnosis and Treatment of ARDS. Diagnostics, 13(21), 3296. https://doi.org/10.3390/diagnostics13213296