

Combined Radiofrequency Ablation and Left Atrial Appendage Closure in Atrial Fibrillation and Systolic Heart Failure

 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Guideline-Directed Medical Therapies
2.3. A Combined Procedure of Catheter Ablation and LAAC
2.4. Post-Procedure Management and Follow-Up
2.5. Events Definition
2.6. Statistics
3. Results
3.1. Patient Demographics
3.2. Procedural and Index-Hospitalization Characteristics
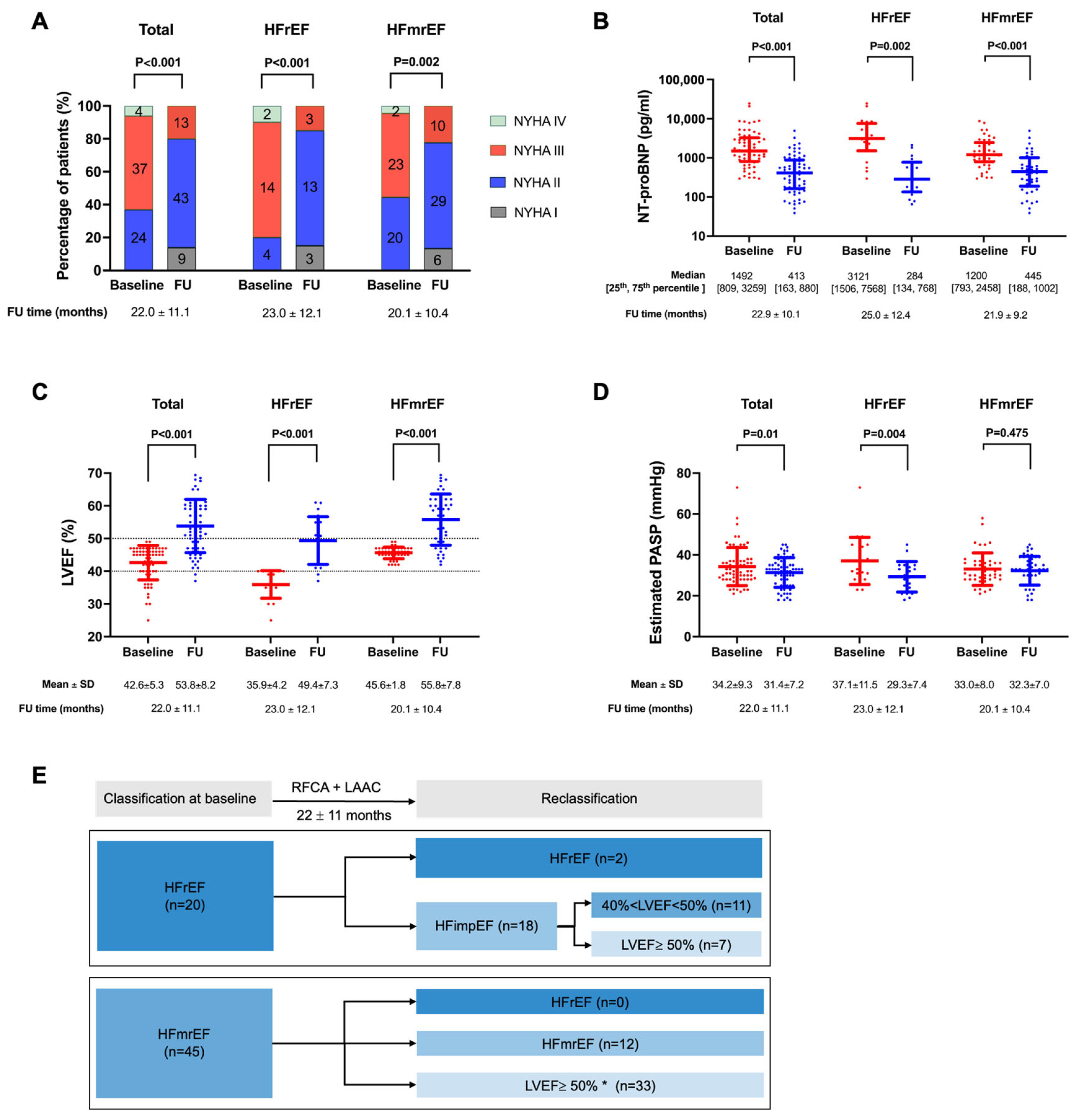
3.3. Post-Procedural Management and Evaluation
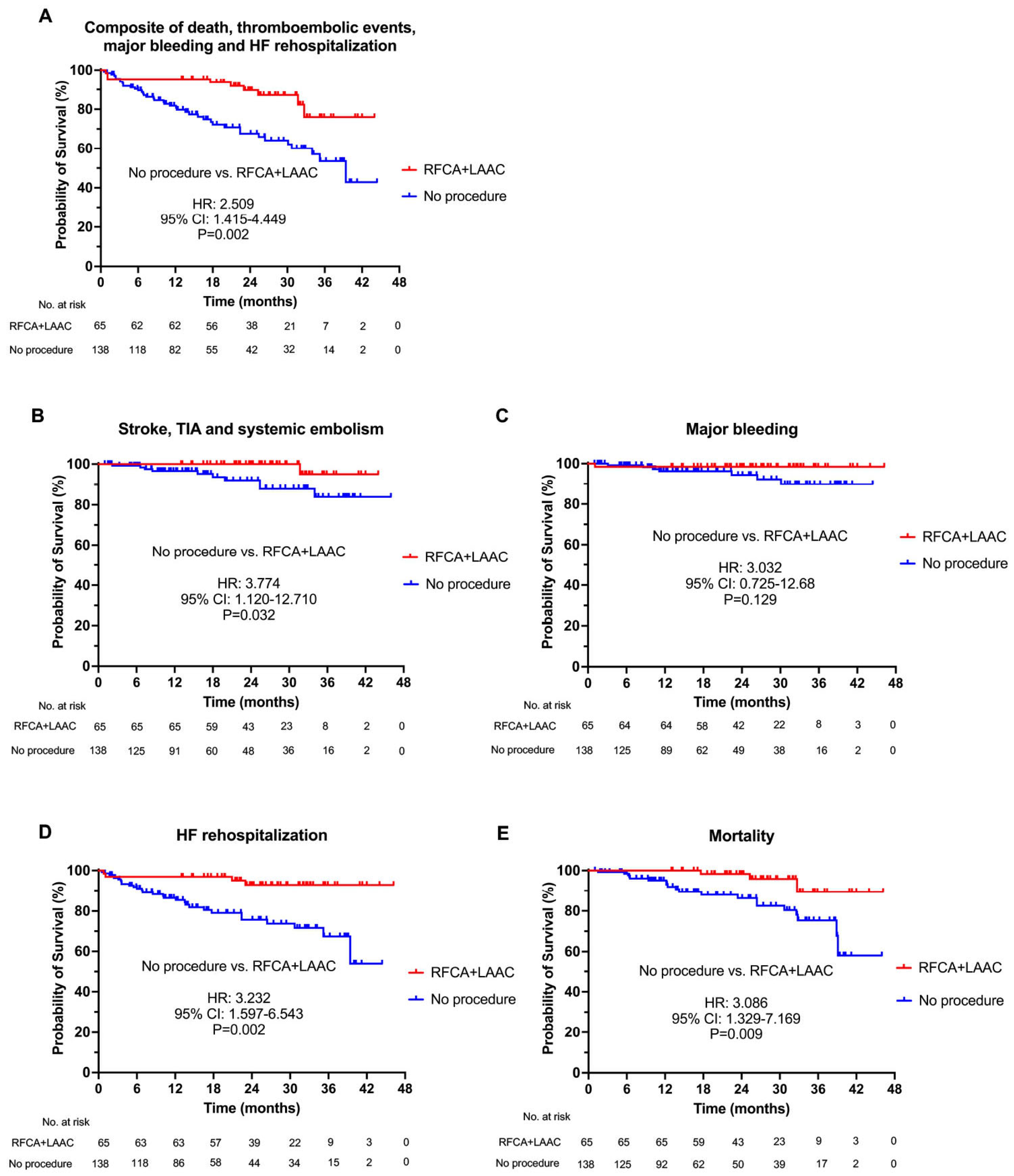
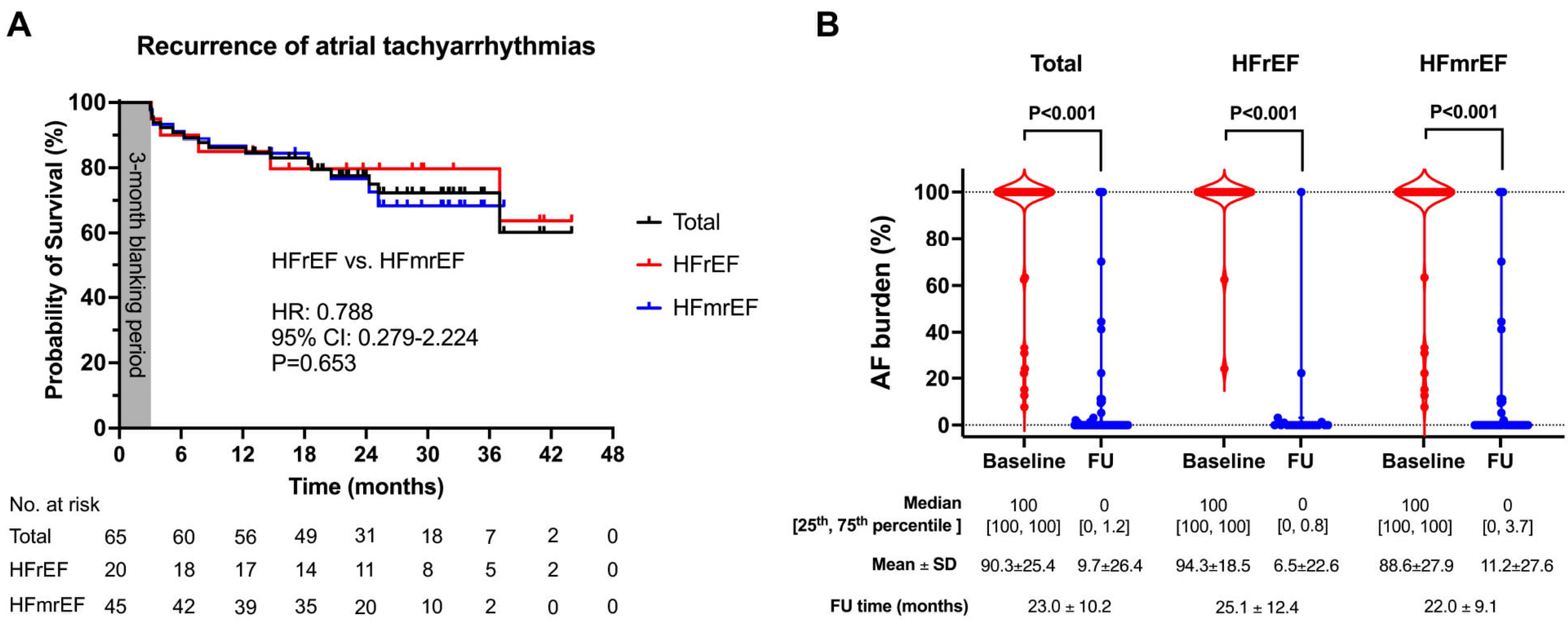
3.4. Events Follow-Up
4. Discussion
4.1. Main Findings
4.2. Effects of Catheter Ablation and Left Atrial Appendage Closure on Cardiac Function
4.3. The Combined Procedure on Stroke Prevention
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Santhanakrishnan, R.; Wang, N.; Larson, M.G.; Magnani, J.W.; McManus, D.D.; Lubitz, S.A.; Ellinor, P.T.; Cheng, S.; Vasan, R.S.; Lee, D.S.; et al. Atrial Fibrillation Begets Heart Failure and Vice Versa: Temporal Associations and Differences in Preserved Versus Reduced Ejection Fraction. Circulation 2016, 133, 484–492. [Google Scholar] [CrossRef] [PubMed]
- Roger, V.L.; Weston, S.A.; Redfield, M.M.; Hellermann-Homan, J.P.; Killian, J.; Yawn, B.P.; Jacobsen, S.J. Trends in heart failure incidence and survival in a community-based population. JAMA 2004, 292, 344–350. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Li, C.; Liao, P.; Cui, X.; Tian, W.; Wang, Q.; Sun, J.; Yang, M.; Luo, L.; Wu, H.; et al. Epidemiology, management, and outcomes of atrial fibrillation among 30 million citizens in Shanghai, China from 2015 to 2020: A medical insurance database study. Lancet Reg. Health West. Pac. 2022, 23, 100470. [Google Scholar] [CrossRef] [PubMed]
- Gopinathannair, R.; Chen, L.Y.; Chung, M.K.; Cornwell, W.K.; Furie, K.L.; Lakkireddy, D.R.; Marrouche, N.F.; Natale, A.; Olshansky, B.; Joglar, J.A.; et al. Managing Atrial Fibrillation in Patients With Heart Failure and Reduced Ejection Fraction: A Scientific Statement From the American Heart Association. Circ. Arrhythm. Electrophysiol. 2021, 14, HAE0000000000000078. [Google Scholar] [CrossRef] [PubMed]
- Di Biase, L.; Mohanty, P.; Mohanty, S.; Santangeli, P.; Trivedi, C.; Lakkireddy, D.; Reddy, M.; Jais, P.; Themistoclakis, S.; Dello Russo, A.; et al. Ablation Versus Amiodarone for Treatment of Persistent Atrial Fibrillation in Patients with Congestive Heart Failure and an Implanted Device: Results from the AATAC Multicenter Randomized Trial. Circulation 2016, 133, 1637–1644. [Google Scholar] [CrossRef] [PubMed]
- Marrouche, N.F.; Brachmann, J.; Andresen, D.; Siebels, J.; Boersma, L.; Jordaens, L.; Merkely, B.; Pokushalov, E.; Sanders, P.; Proff, J.; et al. Catheter Ablation for Atrial Fibrillation with Heart Failure. N. Engl. J. Med. 2018, 378, 417–427. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Purerfellner, H.; Meyer, C.; Acou, W.J.; Schratter, A.; Ling, Z.; Liu, S.; Yin, Y.; Martinek, M.; Kiuchi, M.G.; et al. Rhythm control for patients with atrial fibrillation complicated with heart failure in the contemporary era of catheter ablation: A stratified pooled analysis of randomized data. Eur. Heart J. 2020, 41, 2863–2873. [Google Scholar] [CrossRef]
- Lip, G.Y.; Nieuwlaat, R.; Pisters, R.; Lane, D.A.; Crijns, H.J. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: The euro heart survey on atrial fibrillation. Chest 2010, 137, 263–272. [Google Scholar] [CrossRef]
- Hsu, J.C.; Maddox, T.M.; Kennedy, K.F.; Katz, D.F.; Marzec, L.N.; Lubitz, S.A.; Gehi, A.K.; Turakhia, M.P.; Marcus, G.M. Oral Anticoagulant Therapy Prescription in Patients with Atrial Fibrillation Across the Spectrum of Stroke Risk: Insights from the NCDR PINNACLE Registry. JAMA Cardiol. 2016, 1, 55–62. [Google Scholar] [CrossRef]
- Saad, M.; Osman, M.; Hasan-Ali, H.; Abdel Ghany, M.; Alsherif, M.A.; Risha, O.; Sano, M.; Fink, T.; Heeger, C.H.; Vogler, J.; et al. Atrial appendage closure in patients with heart failure and atrial fibrillation: Industry-independent single-centre study. ESC Heart Fail. 2022, 9, 648–655. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.Y.; Kim, M.J.; Seo, J.; Cho, I.; Shim, C.Y.; Hong, G.R.; Kim, J.S.; Ha, J.W. Predictors of Subsequent Heart Failure after Left Atrial Appendage Closure. Circ. J. 2022, 86, 1129–1136. [Google Scholar] [CrossRef]
- Lin, A.Y.; Dinatolo, E.; Metra, M.; Sbolli, M.; Dasseni, N.; Butler, J.; Greenberg, B.H. Thromboembolism in Heart Failure Patients in Sinus Rhythm: Epidemiology, Pathophysiology, Clinical Trials, and Future Direction. JACC Heart Fail. 2021, 9, 243–253. [Google Scholar] [CrossRef]
- Dukkipati, S.R.; Kar, S.; Holmes, D.R.; Doshi, S.K.; Swarup, V.; Gibson, D.N.; Maini, B.; Gordon, N.T.; Main, M.L.; Reddy, V.Y. Device-Related Thrombus after Left Atrial Appendage Closure: Incidence, Predictors, and Outcomes. Circulation 2018, 138, 874–885. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Sun, J.Y.; Wu, L.D.; Hao, J.F.; Wang, R.X. The long-term efficacy and safety of combining ablation and left atrial appendage closure: A systematic review and meta-analysis. J. Cardiovasc. Electrophysiol. 2021, 32, 3068–3081. [Google Scholar] [CrossRef] [PubMed]
- Barra, S.; Narayanan, K.; Boveda, S.; Primo, J.; Goncalves, H.; Baran, J.; Agarwal, S.; Marijon, E.; Providencia, R. Atrial Fibrillation Ablation and Reduction of Stroke Events: Understanding the Paradoxical Lack of Evidence. Stroke 2019, 50, 2970–2976. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Sun, J.; Li, W.; Zhang, P.P.; Zhang, R.; Mo, B.F.; Yang, M.; Wang, Q.S.; Li, Y.G. Sex Differences in the Combined Ablation and Left Atrial Appendage Closure: Results from LAACablation Registry. JACC Asia 2023, 3, 138–149. [Google Scholar] [CrossRef]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2022, 79, e263–e421. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Jin, Q.; Kong, D.; Jiang, Y.; Chen, S.; Chen, D.; Hou, C.R.; Zhang, L.; Pan, C.; Zhou, D.; et al. Comparison of fluoroscopy and transesophageal echocardiogram for intra-procedure device surveillance assessment during implantation of Watchman. Int. J. Cardiol. 2021, 324, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Pocock, S.J.; Ariti, C.A.; McMurray, J.J.; Maggioni, A.; Kober, L.; Squire, I.B.; Swedberg, K.; Dobson, J.; Poppe, K.K.; Whalley, G.A.; et al. Predicting survival in heart failure: A risk score based on 39,372 patients from 30 studies. Eur. Heart J. 2013, 34, 1404–1413. [Google Scholar] [CrossRef]
- Friberg, L.; Rosenqvist, M.; Lip, G.Y. Evaluation of risk stratification schemes for ischaemic stroke and bleeding in 182,678 patients with atrial fibrillation: The Swedish Atrial Fibrillation cohort study. Eur. Heart J. 2012, 33, 1500–1510. [Google Scholar] [CrossRef]
- Holmes, D.R.; Reddy, V.Y.; Turi, Z.G.; Doshi, S.K.; Sievert, H.; Buchbinder, M.; Mullin, C.M.; Sick, P.; Investigators, P.A. Percutaneous closure of the left atrial appendage versus warfarin therapy for prevention of stroke in patients with atrial fibrillation: A randomised non-inferiority trial. Lancet 2009, 374, 534–542. [Google Scholar] [CrossRef] [PubMed]
- Holmes, D.R., Jr.; Kar, S.; Price, M.J.; Whisenant, B.; Sievert, H.; Doshi, S.K.; Huber, K.; Reddy, V.Y. Prospective randomized evaluation of the Watchman Left Atrial Appendage Closure device in patients with atrial fibrillation versus long-term warfarin therapy: The PREVAIL trial. J. Am. Coll. Cardiol. 2014, 64, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Osmancik, P.; Herman, D.; Neuzil, P.; Hala, P.; Taborsky, M.; Kala, P.; Poloczek, M.; Stasek, J.; Haman, L.; Branny, M.; et al. Left Atrial Appendage Closure Versus Direct Oral Anticoagulants in High-Risk Patients with Atrial Fibrillation. J. Am. Coll. Cardiol. 2020, 75, 3122–3135. [Google Scholar] [CrossRef]
- Phan, Q.T.; Shin, S.Y.; Cho, I.S.; Lee, W.S.; Won, H.; Sharmin, S.; Lee, D.Y.; Kim, T.H.; Kim, C.J.; Kim, S.W. Impact of left atrial appendage closure on cardiac functional and structural remodeling: A difference-in-difference analysis of propensity score matched samples. Cardiol. J. 2019, 26, 519–528. [Google Scholar] [CrossRef] [PubMed]
- Herman, D.; Osmancik, P.; Neuzil, P.; Hala, P.; Lekesova, V.; Benesova, K.; Hozman, M.; Jarkovsky, J.; Novackova, M.; Widimsky, P.; et al. The effect of left atrial appendage closure on heart failure biomarkers: A PRAGUE-17 trial subanalysis. J. Cardiovasc. Electrophysiol. 2021, 32, 2645–2654. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.G.; Gong, C.Q.; Zhao, M.Z.; Sun, J.; Wang, Q.S.; Zhang, P.P.; Feng, X.F.; Yu, Y.; Yu, Y.C.; Liang, B.E.; et al. Determinants of postoperative left atrial structural reverse remodeling in patients undergoing combined catheter ablation of atrial fibrillation and left atrial appendage closure procedure. J. Cardiovasc. Electrophysiol. 2019, 30, 1868–1876. [Google Scholar] [CrossRef] [PubMed]
- Healey, J.S.; Baranchuk, A.; Crystal, E.; Morillo, C.A.; Garfinkle, M.; Yusuf, S.; Connolly, S.J. Prevention of atrial fibrillation with angiotensin-converting enzyme inhibitors and angiotensin receptor blockers: A meta-analysis. J. Am. Coll. Cardiol. 2005, 45, 1832–1839. [Google Scholar] [CrossRef] [PubMed]
- Fujimoto, H.; Doi, N.; Okayama, S.; Naito, M.; Kobori, A.; Kaitani, K.; Inoue, K.; Kurotobi, T.; Morishima, I.; Yamaji, H.; et al. Long-term prognosis of patients undergoing radiofrequency catheter ablation for atrial fibrillation: Comparison between heart failure subtypes based on left ventricular ejection fraction. Europace 2022, 24, 576–586. [Google Scholar] [CrossRef]
- Prochaska, J.H.; Gobel, S.; Nagler, M.; Knopfler, T.; Eggebrecht, L.; Lamparter, H.; Panova-Noeva, M.; Keller, K.; Coldewey, M.; Bickel, C.; et al. Sustained atrial fibrillation increases the risk of anticoagulation-related bleeding in heart failure. Clin. Res. Cardiol. 2018, 107, 1170–1179. [Google Scholar] [CrossRef]
- MacDonald, M.R.; Connelly, D.T.; Hawkins, N.M.; Steedman, T.; Payne, J.; Shaw, M.; Denvir, M.; Bhagra, S.; Small, S.; Martin, W.; et al. Radiofrequency ablation for persistent atrial fibrillation in patients with advanced heart failure and severe left ventricular systolic dysfunction: A randomised controlled trial. Heart 2011, 97, 740–747. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | Total (n = 65) | HFrEF (n = 20) | HFmrEF (n = 45) | p-Value |
|---|---|---|---|---|
| Age | 67.3 ± 7.5 | 67.3 ± 9.8 | 67.3 ± 6.4 | 0.967 |
| Age < 65 y | 17 (26.2) | 4 (20.0) | 13 (28.9) | 0.551 |
| 65 y ≤ age < 75 y | 36 (55.4) | 11 (55.0) | 25 (55.6) | 0.967 |
| Age ≥ 75 y | 12 (18.5) | 5 (25.0) | 7 (15.5) | 0.490 |
| Female | 18 (27.7) | 6 (30.0) | 12 (26.6) | 0.782 |
| BMI (kg/m2) | 25.7 ± 3.4 | 25.1 ± 4.2 | 26.0 ± 3.1 | 0.339 |
| AF types | ||||
| Paroxysmal | 10 (15.4) | 3 (15.0) | 7 (15.6) | >0.999 |
| Persistent/long-standing persistent | 55 (84.6) | 17 (85.0) | 38 (84.4) | >0.999 |
| CHA2DS2-VASc score | 3.9 ± 1.2 | 3.6 ± 1.3 | 4.0 ± 1.1 | 0.225 |
| HAS-BLED score | 2.7 ± 1.0 | 2.7 ± 1.3 | 2.8 ± 1.0 | 0.848 |
| MAGGIC score * | 20.1 ± 4.9 | 22.6 ± 5.1 | 19.0 ± 4.4 | 0.006 |
| NYHA class | ||||
| NYHA class II | 24 (36.9) | 4 (20.0) | 20 (44.4) | 0.094 |
| NYHA class III | 37 (56.9) | 14 (70.0) | 23 (51.1) | 0.156 |
| Ambulatory NYHA class IV | 4 (6.2) | 2 (10.0) | 2 (4.4) | >0.999 |
| Hypertension | 51 (78.5) | 16 (80.0) | 35 (77.8) | >0.999 |
| Diabetes mellites | 15 (23.1) | 3 (15.0) | 12 (26.7) | 0.359 |
| Myocardial infarction | 2 (3.1) | 0 (0) | 2 (4.4) | >0.999 |
| Cardiac revascularization † | 6 (9.2) | 1 (5.0) | 5 (11.1) | 0.657 |
| Hypertrophic cardiomyopathy | 4 (6.2) | 2 (10.0) | 2 (4.4) | 0.581 |
| Left ventricular non-compaction cardiomyopathy | 2 (3.1) | 0 (0) | 2 (4.4) | >0.999 |
| Obstructive sleep apnea | 4 (6.2) | 3 (15.0) | 1 (2.2) | 0.083 |
| Chronic obstructive pulmonary disease | 3 (4.6) | 2 (10.0) | 1 (2.2) | 0.222 |
| History of strokes/TIAs/SE | 13 (20.0) | 2 (10.0) | 11 (24.4) | 0.314 |
| History of LAA thrombus | 6 (9.2) | 2 (10.0) | 4 (8.9) | >0.999 |
| History of major bleeding | 11 (16.9) | 4 (20.0) | 7 (15.6) | 0.726 |
| History of malignant tumor | 4 (6.2) | 1 (5.0) | 3 (6.7) | >0.999 |
| History of chemotherapy | 3 (4.6) | 1 (5.0) | 2 (4.4) | >0.999 |
| Pacemaker implantation | 3 (4.6) | 1 (5.0) | 2 (4.4) | >0.999 |
| ICD/RT-D implantation | 2 (3.1) | 1 (5.0) | 1 (2.2) | 0.524 |
| Current smoker | 23 (35.4) | 9 (45.0) | 14 (31.1) | 0.400 |
| Echocardiographic parameters | ||||
| LVEF (%) | 42.6 ± 5.3 | 35.9 ± 4.2 | 45.6 ± 1.8 | <0.001 |
| Left atrial diameter (mm) | 47.1 ± 5.0 | 46.5 ± 5.5 | 47.4 ± 4.9 | 0.532 |
| LVEDD (mm) | 57.0 ± 6.6 | 60.0 ± 8.5 | 55.7 ± 5.2 | 0.016 |
| LVESD (mm) | 44.1 ± 6.6 | 48.9 ± 8.1 | 42.0 ± 4.5 | <0.001 |
| Estimated PASP (mmHg) | 34.3 ± 9.3 | 37.1 ± 11.5 | 33.0 ± 8.0 | 0.106 |
| Pericardial effusion, mm ‡ | 2.6 ± 1.2 | 2.9 ± 1.1 | 2.5 ± 1.3 | 0.222 |
| NT-proBNP (pg/mL) | 1492 [809, 3259] | 3121 [1506, 7568] | 1200 [793, 2458] | 0.006 |
| Troponin I (ng/mL) | 0.019 [0.009, 0.033] | 0.028 [0.009, 0.054] | 0.018 [0.009, 0.029] | 0.313 |
| Hemoglobin, g/L | 136 ± 14 | 138 ± 16 | 135 ± 14 | 0.398 |
| Creatine, mmol/L | 76 ± 19 | 76 ± 16 | 76 ± 20 | 0.903 |
| Characteristics | Total (n = 65) | HFrEF (n = 20) | HfmrEF (n = 45) | p-Value |
|---|---|---|---|---|
| Ablation phase | ||||
| PVI (total) | 65 (100) | 20 (100.0) | 45 (100) | >0.999 |
| PVI only | 3 (4.6) | 1 (5.0) | 2 (4.4) | >0.999 |
| LA roof line | 50 (76.9) | 15 (75.0) | 35 (77.7) | >0.999 |
| LA posterior and/or inferior lines | 33 (50.8) | 9 (45.0) | 24 (53.3) | 0.535 |
| Posterior wall isolation | 27 (41.5) | 7 (35.0) | 20 (44.4) | 0.476 |
| Anterior septal line | 41 (63.1) | 12 (60.0) | 29 (64.4) | 0.785 |
| Mitral isthmus line | 35 (53.8) | 5 (25.0) | 30 (66.6) | 0.003 |
| CS and GCV musculature ablation | 10 (15.4) | 1 (5.0) | 9 (20.0) | 0.156 |
| VOM ethanol infusion | 10 (15.4) | 2 (10.0) | 8 (17.7) | 0.711 |
| LAA isolation | 5 (7.7) | 1 (5.0) | 4 (8.9) | >0.999 |
| Cavo-tricuspid line | 48 (73.8) | 12 (60.0) | 36 (80.0) | 0.127 |
| Superior vena cava isolation | 3 (4.6) | 1 (10.0) | 2 (4.4) | >0.999 |
| CFAE ablation | 39 (60.0) | 11 (55.0) | 27 (60.0) | 0.706 |
| Ganglionated plexi ablation | 1 (1.5) | 0 (0) | 1 (2.2) | >0.999 |
| Intracardiac cardioversion | 20 (30.8) | 7 (35.0) | 13 (28.8) | 0.622 |
| Intraprocedural sinus rhythm restoration | 65 (100.0) | 20 (100.0) | 45 (100) | >0.999 |
| LAAC phase | ||||
| LAA morphology types | ||||
| Chicken wing | 17 (26.2) | 8 (40.0) | 9 (20.0) | 0.090 |
| Windsock | 5 (7.7) | 1 (5.0) | 4 (8.9) | >0.999 |
| Cauliflower | 40 (61.5) | 10 (50.0) | 30 (66.7) | 0.202 |
| Cactus | 3 (4.6) | 1 (5.0) | 2 (4.4) | >0.999 |
| LAA ostium, mm | 23.8 ± 3.5 | 24.1 ± 3.9 | 23.7 ± 3.3 | 0.648 |
| Device size for WATCHMAN | ||||
| 21 mm | 4 (6.2) | 2 (10.0) | 2 (4.4) | 0.581 |
| 24 mm | 11 (16.9) | 2 (10.0) | 9 (20.0) | 0.480 |
| 27 mm | 16 (24.6) | 6 (30.0) | 10 (22.2) | 0.502 |
| 30 mm | 12 (18.5) | 2 (10.0) | 10 (22.2) | 0.315 |
| 33 mm | 22 (33.8) | 8 (40.0) | 14 (31.1) | 0.485 |
| Total procedure time, min | 196 ± 50 | 183 ± 55 | 203 ± 46 | 0.133 |
| Ablation time, min | 62 ± 27 | 56 ± 26 | 64 ± 27 | 0.269 |
| Fluoroscopy time, min | 8.4 ± 4.5 | 8.1 ± 4.7 | 8.6 ± 4.1 | 0.666 |
| Irrigation fluid volume, ml | 1103 ± 423 | 1035 ± 432 | 1147 ± 417 | 0.303 |
| Procedural complications (total) | 6 (9.2) | 2 (10.0) | 4 (8.8) | >0.999 |
| Acute decompensated heart failure | 4 (6.2) | 2 (10.0) | 2 (4.4) | 0.581 |
| Cardiac tamponade | 0 (0) | 0 (0) | 0 (0) | >0.999 |
| Pericardial effusion not requiring pericardiocentesis | 1 (1.5) | 0 (0) | 1 (2.2) | >0.999 |
| Device embolism | 0 (0) | 0 (0) | 0 (0) | >0.999 |
| Stroke/TIA/systemic embolism | 0 (0) | 0 (0) | 0 (0) | >0.999 |
| Air embolism | 1 (1.5) | 0 (0) | 1 (2.2) | >0.999 |
| Major bleeding | 0 (0) | 0 (0) | 0 (0) | >0.999 |
| Death | 0 (0) | 0 (0) | 0 (0) | >0.999 |
| Total hospital stay, days | 10.0 ± 4.1 | 11.8 ± 5.2 | 9.2 ± 3.3 | 0.022 |
| Pre-procedural hospital stay, days | 5.6 ± 2.4 | 6.6 ± 2.4 | 5.1 ± 2.3 | 0.026 |
| Post-procedural hospital stay, days | 4.4 ± 3.0 | 5.2 ± 4.7 | 5.2 ± 4.7 | 0.173 |
| Post-Procedural Imaging | Total (n = 65) | HFrEF (n = 20) | HFmrEF (n = 45) | p-Value |
|---|---|---|---|---|
| TEE evaluation, n | 46 (70.8) | 15 (75.0) | 31 (68.9) | 0.770 |
| Compression ratio, % | 15.4 ± 2.3 | 16.0 ± 2.4 | 15.2 ± 2.2 | 0.216 |
| DRT | 3 (6.5) | 1 (6.7) | 2 (6.5) | >0.999 |
| No PDL † | 33 (71.7) | 12 (80.0) | 21 (67.7) | 0.497 |
| PDL ≤ 5 mm | 13 (28.3) | 3 (0.2) | 10 (32.3) | 0.497 |
| PDL > 5 mm | 0 (0) | 0 (0) | 0 (0) | >0.999 |
| Satisfactory seal | 46 (100) | 15 (100) | 31 (100) | >0.999 |
| Cardiac CT evaluation, n | 37 (56.9) | 12 (60.0) | 25 (55.6) | 0.738 |
| LAA—no contrast filling ‡ | 12 (32.4) | 4 (33.3) | 8 (32.0) | >0.999 |
| LAA—contrast filling | 25 (67.6) | 8 (66.7) | 17 (68.0) | >0.999 |
| Contrast filling with visible PDL | 19(51.4) | 5 (41.7) | 13 (52.0) | >0.999 |
| Contrast filling without PDL | 6 (16.2) | 2(17.7) | 4(16.0) | >0.999 |
| Oral Medications | HFrEF (n = 20) | HFmrEF (n = 45) | ||||
|---|---|---|---|---|---|---|
| Before | 1-Year | p-Value | Before | 1-Year | p-Value | |
| Antithrombotic regimen | ||||||
| Oral anticoagulants | 17 (85.0) | 3 (15.0) | <0.001 | 39 (86.7) | 5 (11.1) | <0.001 |
| Warfarin | 6 (30.0) | 0 (0) | 0.020 | 11 (24.4) | 1 (2.2) | 0.004 |
| NOAC | 11 (55.0) | 3 (15.0) | 0.019 | 28 (62.2) | 4 (8.9) | <0.001 |
| Antiplatelets | 2 (10.0) | 14 (70.0) | <0.001 | 5 (11.1) | 32 (71.1) | <0.001 |
| Dual antiplatelets | 1 (5.0) | 0 (0) | >0.999 | 2 (4.4) | 1 (2.2) | >0.999 |
| Single antiplatelet | 1 (5.0) | 14 (70.0) | <0.001 | 3 (6.7) | 31 (68.9) | <0.001 |
| None | 1 (5.0) | 3 (15.0) | 0.605 | 1 (2.2) | 8 (17.8) | 0.030 |
| Antiarrhythmic drugs | 8 (40.0) | 3 (15.0) | >0.999 | 6 (13.3) | 3 (6.7) | 0.485 |
| Class I * | 0 (0) | 0 (0) | >0.999 | 0 (0) | 0 (0) | >0.999 |
| Amiodarone | 8 (40.0) | 2 (10.0) | 0.065 | 5 (11.1) | 3 (6.7) | 0.714 |
| Other Class III † | 0 (0) | 0 (0) | >0.999 | 1 (2.2) | 0 (0) | >0.999 |
| Class IV | 0 (0) | 0 (0) | >0.999 | 0 (0) | 0 (0) | >0.999 |
| Medications for heart failure | ||||||
| Beta-blocker | 19 (95.0) | 19 (95.0) | >0.999 | 28 (62.2) | 33 (73.3) | 0.259 |
| Initiation dosage | 15 (75.0) | 7 (35.0) | 0.025 | 22 (48.9) | 24 (53.3) | 0.673 |
| Up-titration | 4 (20.0) | 12 (60.0) | 0.010 | 6 (13.3) | 9 (20.0) | 0.396 |
| ACEi/ARB/ARNi ‡ | 16 (80.0) | 18 (90.0) | 0.661 | 27 (60.0) | 26 (57.8) | >0.999 |
| Initiation dosage | 15 (75.0) | 7 (35.0) | 0.010 | 24 (53.3) | 21 (46.7) | 0.527 |
| Up-titration | 1 (5.0) | 11 (55.0) | 0.001 | 3 (6.7) | 5 (11.1) | 0.288 |
| MRA | 18 (90.0) | 17 (85.0) | >0.999 | 24 (53.3) | 23 (51.1) | >0.999 |
| Initiation dosage | 16 (80.0) | 15 (75.0) | >0.999 | 23 (51.1) | 21 (46.7) | 0.673 |
| Up-titration | 2 (10.0) | 2 (10.0) | >0.999 | 1 (2.2) | 2 (4.4) | >0.999 |
| SGLT2i § | 1 (5.0) | 3 (15.0) | 0.605 | 2 (4.4) | 4 (8.9) | 0.677 |
| Combination of GDMT ¶ | ||||||
| No therapy | 0 (0) | 0 (0) | >0.999 | 4 (8.9) | 3 (6.7) | >0.999 |
| Single therapy | 0 (0) | 0 (0) | >0.999 | 15 (33.3) | 11 (24.4) | 0.352 |
| Double therapy | 7 (35.0) | 4 (20.0) | 0.480 | 12 (26.7) | 18 (40.0) | 0.180 |
| Triple therapy | 12 (60.0) | 15 (75.0) | 0.501 | 14 (31.1) | 13 (28.9) | 0.929 |
| Quadruple therapy | 1 (5.0) | 1 (5.0) | >0.999 | 0 (0) | 0 (0) | >0.999 |
| Diuretics | 18 (90.0) | 17 (85.0) | >0.999 | 32 (71.1) | 28 (62.2) | 0.371 |
| Digitalis | 10 (50.0) | 3 (20.0) | 0.041 | 13 (28.9) | 4 (8.9) | 0.029 |
| Ivabradine | 0 (0) | 0 (0) | >0.999 | 0 (0) | 1 (2.2) | >0.999 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sun, J.; Zhang, R.; Yang, M.; Li, W.; Zhang, P.-P.; Mo, B.-F.; Wang, Q.-S.; Chen, M.; Li, Y.-G. Combined Radiofrequency Ablation and Left Atrial Appendage Closure in Atrial Fibrillation and Systolic Heart Failure. Diagnostics 2023, 13, 3325. https://doi.org/10.3390/diagnostics13213325
Sun J, Zhang R, Yang M, Li W, Zhang P-P, Mo B-F, Wang Q-S, Chen M, Li Y-G. Combined Radiofrequency Ablation and Left Atrial Appendage Closure in Atrial Fibrillation and Systolic Heart Failure. Diagnostics. 2023; 13(21):3325. https://doi.org/10.3390/diagnostics13213325
Chicago/Turabian StyleSun, Jian, Rui Zhang, Mei Yang, Wei Li, Peng-Pai Zhang, Bin-Feng Mo, Qun-Shan Wang, Mu Chen, and Yi-Gang Li. 2023. "Combined Radiofrequency Ablation and Left Atrial Appendage Closure in Atrial Fibrillation and Systolic Heart Failure" Diagnostics 13, no. 21: 3325. https://doi.org/10.3390/diagnostics13213325
APA StyleSun, J., Zhang, R., Yang, M., Li, W., Zhang, P.-P., Mo, B.-F., Wang, Q.-S., Chen, M., & Li, Y.-G. (2023). Combined Radiofrequency Ablation and Left Atrial Appendage Closure in Atrial Fibrillation and Systolic Heart Failure. Diagnostics, 13(21), 3325. https://doi.org/10.3390/diagnostics13213325