
Inverse Problem Algorithm-Based Time-Resolved Imaging of Head and Neck Computed Tomography Angiography Contrast Kinetics with Clinical Testification


 and
and
Abstract
:1. Introduction
2. Methodology
2.1. Stage 1
2.1.1. Basics of the Inverse Problem Algorithm
2.1.2. IPA Derivation of the 29-Term Formula
2.1.3. CTA Number of LA and Seven Risk Factors
2.2. Stage 2
Extreme Values of CMmax and CMmin
3. Results
3.1. Raw Data Normalization
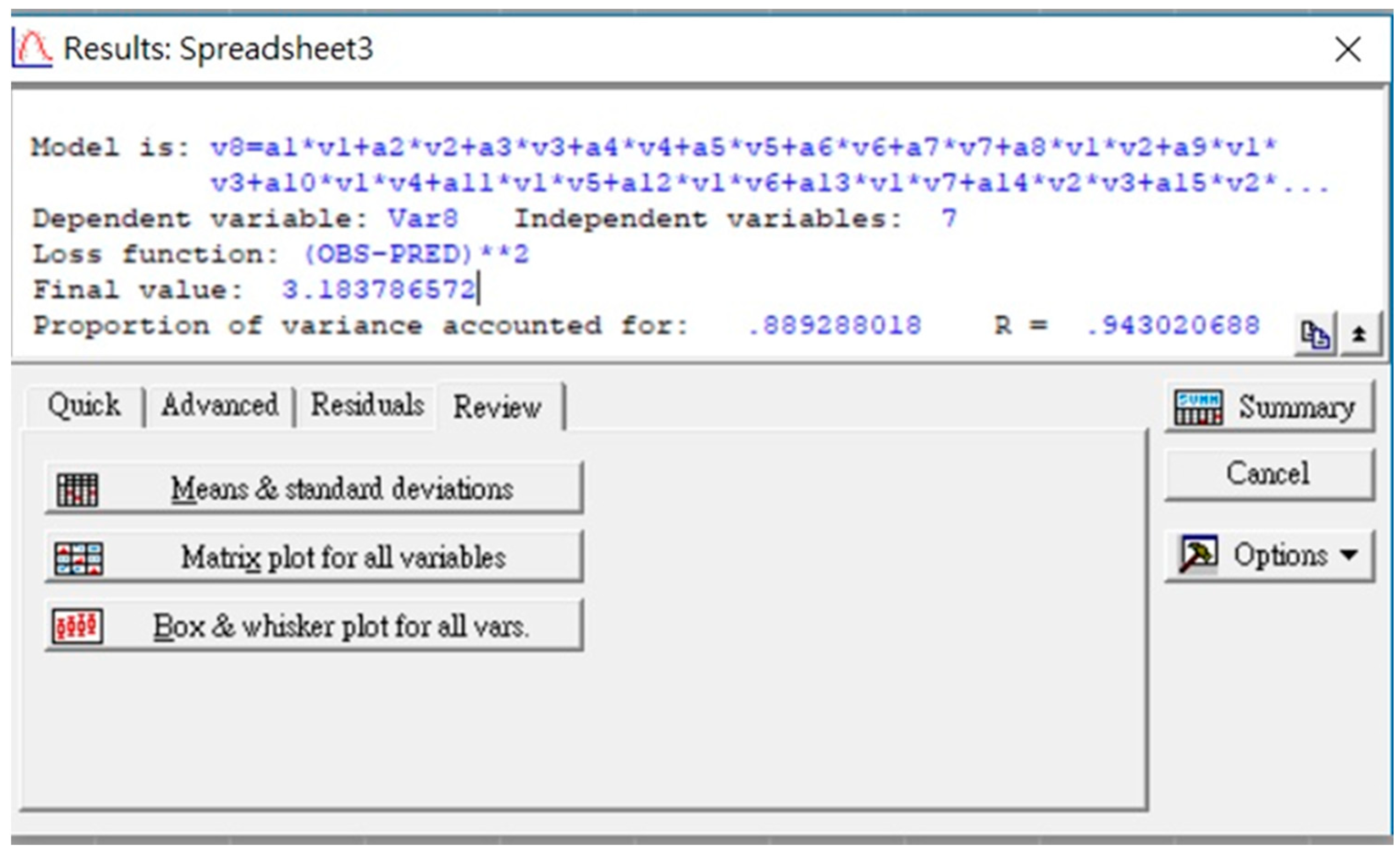
3.2. Calculation Procedure and Program Performance of the Customized IPA Algorithm
4. Discussion
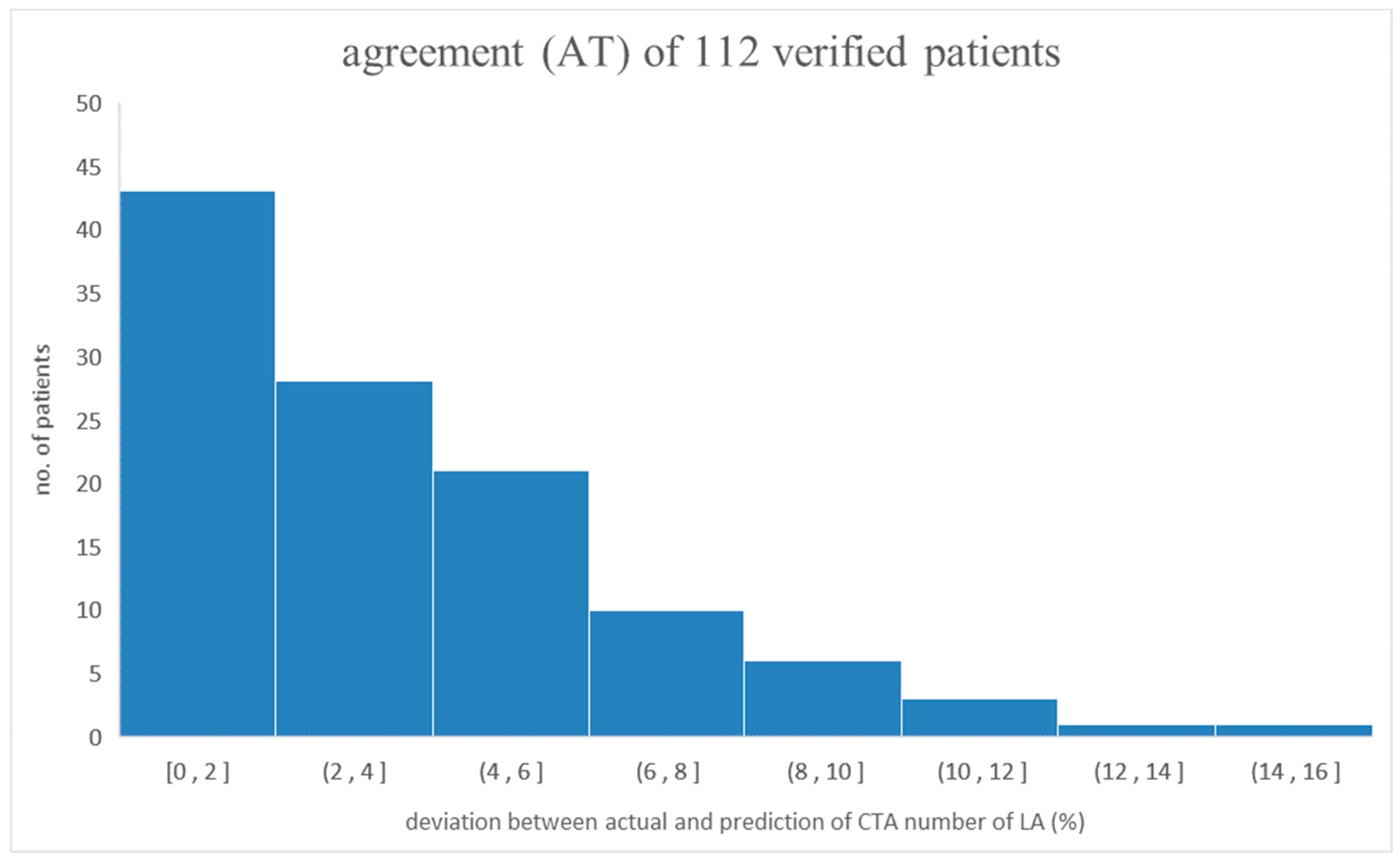
4.1. Verifying the Predicted CTA Number of LA by the Derived Semi-Empirical Formula
4.2. Interpreting the Dominant Factors Controlling the Prediction of the CTA Number of LA
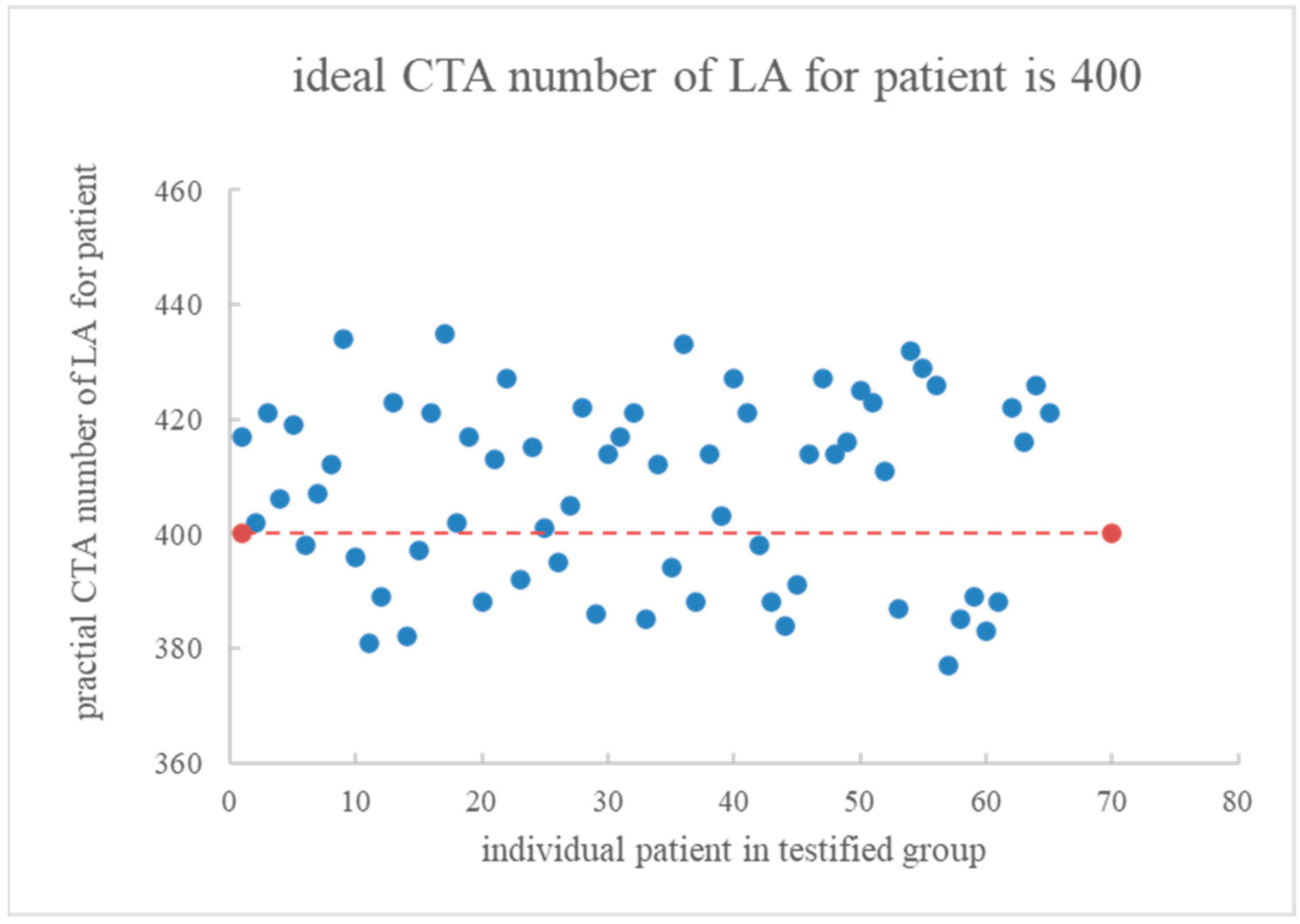
4.3. In Vivo Testification of 65 Patients
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Computation via STATISTICA 7.0

References
- Ma, G.; Yu, Y.; Duan, H.; Jia, Y.; Zhang, X.; Yang, C.; Chen, X.; Han, D.; Guo, C.; He, T. Subtraction CT angiography in head and neck with low radiation and contrast dose dual-energy spectral CT using rapid kV-switching technique. Br. J. Radiol. 2018, 91, 20170631. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Chen, Y.; Wang, Y.; Xue, H.; Jin, Z.; Kong, L.; Cao, J.; Li, S. Feasibility of low-dose contrast medium high pitch CT angiography for the combined evaluation of coronary, head and neck arteries. PLoS ONE 2014, 9, e90268. [Google Scholar] [CrossRef] [PubMed]
- Benz, D.C.; Grani, C.; Moch, B.H.; Mikulicic, F.; Vontobel, J.; Fuchs, T.A.; Stehli, J.; Clerc, O.; Possner, M.; Pazhenkottil, A.P.; et al. A low-dose and an ultra-low-dose contrast agent protocol for coronary CT angiography in a clinical setting: Quantitative and qualitative comparison to a standard dose protocol. Br. J. Radiol. 2017, 90, 20160933. [Google Scholar] [CrossRef] [PubMed]
- Saade, C.; Bourne, R.; Wilkinson, M.; Evanoff, M.; Brennan, P. A reduced contrast volume acquisition regimen based on cardiovascular dynamics improves visualisation of head and neck vasculature with carotid MDCT angiography. Eur. J. Radiol. 2013, 82, e64–e69. [Google Scholar] [PubMed]
- Xia, W.; Wu, J.T.; Yin, X.R.; Wang, Z.J.; Wu, H.T. CT angiography of the neck: Value of contrast medium dose reduction with low tube voltage and high tube current in a 64-detector row CT. Clin. Radiol. 2014, 69, e183–e189. [Google Scholar] [CrossRef]
- Zhang, W.L.; Li, M.; Zhang, B.; Geng, H.Y.; Liang, Y.Q.; Xu, K.; Li, S.B. CT Angiography of the head-and-neck vessels acquired with low tube voltage, low iodine, and iterative image reconstruction: Clinical evaluation of radiation dose and image quality. PLoS ONE 2013, 8, e81486. [Google Scholar] [CrossRef]
- Shen, Y.; Hu, X.; Zou, X.; Zhu, D.; Li, Z.; Hu, D. Did low tube voltage CT combined with low contrast media burden protocols accomplish the goal of “double low” for patients? An overview of applications in vessels and abdominal parenchymal organs over the past 5 years. Int. J. Clin. Pract. 2016, 70, B5–B15. [Google Scholar] [CrossRef]
- Lin, C.S.; Chen, Y.F.; Deng, J.; Yang, D.H.; Chen, M.H.; Lin, Y.H.; Pan, L.K. Taguchi-based optimization of head and neck CT angiography: In-vivo enhanced triggered timing for 600 patients. J. Mech. Med. Biol. 2021, 21, 2140041. [Google Scholar] [CrossRef]
- Liang, C.C.; Pan, L.F.; Chen, M.H.; Deng, J.; Yang, D.H.; Lin, C.S.; Pan, L.K. Timing optimization of head and neck CT angiography via the inverse problem algorithm: In-vivo survey for 1001 patients in 2020–2021. J. Mech. Med. Biol. 2021, 21, 2140055. [Google Scholar] [CrossRef]
- STATISTICA 13.3.721. Available online: https://statistica.software.informer.com (accessed on 9 February 2023).
- Lin, M.C.; Tseng, V.S.; Lin, C.S.; Chiu, S.W.; Pan, L.K.; Pan, L.F. Quantitative prediction of SYNTAX score for cardiovascular artery disease patients via the inverse problem algorithm technique as artificial intelligence assessment in diagnostics. Diagnostics 2022, 12, 3180. [Google Scholar] [CrossRef]
- Huang, S.H.; Peng, B.R.; Lin, C.S.; Tsai, H.C.; Pan, L.F.; Pan, L.K. Potential risk quantification from multiple biological factors via the inverse problem algorithm as an artificial intelligence tool in clinical diagnosis. Technol. Health Care 2023, 31, S69–S79. [Google Scholar] [CrossRef]
- Cademartiri, F.; Mollet, N.R.; Lemos, P.A.; Saia, F.; Midiri, M.; Feyter, P.J.; Krestin, G.P. Higher intracoronary attenuation improves diagnostic accuracy in MDCT coronary angiography. AJR 2006, 187, W430–W433. [Google Scholar] [CrossRef] [PubMed]
- Cademartiri, F.; Maffei, E.; Palumbo, A.A.; Malago, R.; Crutta, L.L.; Meiijboom, W.B.; Aldrovandi, A.; Fusaro, M.; Vignali, L.; Menozzi, A.; et al. Influence of intra-coronary enhancement on diagnostic accuracy with 64-slice CT coronary angiography. Eur. Radiol. 2008, 18, 576–583. [Google Scholar] [CrossRef] [PubMed]
- Lembcke, A.; Schwenke, C.; Hein, P.A.; Knobloch, G.; Durmus, T.; Hamm, B.; Huppertz, A. High-pitch dual-source CT coronary angiography with low volumes of contrast medium. Eur. Radiol. 2013, 24, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Orimadegun, A.E.; Omisanjo, A.O. Evaluation of five formulas for estimating body surface area of Nigerian children. Ann. Med. Health Sci. Res. 2014, 4, 889–898. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, S.; Sekine, A.; Baba, T.; Yamanka, Y.; Sadoyama, S.; Yamakawa, H.; Oda, T.; Okuda, R.; Kitamura, H.; Okudela, K.; et al. Low body surface area predicts hepatotoxicity of nintedanib in patients with idiopathic pulmonary fibrosis. Sci. Rep. 2015, 7, 10811. [Google Scholar] [CrossRef] [PubMed]
- Olive, D.J. Linear Regression, 1st ed.; Springer: Carbondale, IL, USA, 2017; ISBN 978-3-319-55250-7. [Google Scholar]
- Pan, L.F.; Chiang, C.Y.; Huang, C.C.; Kao, H.T.; Chen, C.F.; Peng, B.R.; Pan, L.K. Thyroid biokinetics for radioactive I-131 in twelve thyroid cancer patients via the refined nine-compartmental model. Appl. Sci. 2022, 12, 5538. [Google Scholar] [CrossRef]
- Giavarina, D. Understanding bland altman analysis. Biochem. Medica 2015, 25, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Weiskopf, N.G.; Weng, C. Methods and dimensions of electronic health record data quality assessment: Enabling reuse for clinical research. J. Am. Med. Inform. Assoc. 2013, 20, 144–151. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Risk Factor | Case No. and Variation Range | Parameters of Derived Data | |||
|---|---|---|---|---|---|
| Case No./Max. | Case No./Min. | Mean | Median | St. Dev | |
| Age (yr) | 162/90 | 383/24 | 56 | 58 | 13.3 |
| Tube voltage (kVp) | 142/140 | 151/70 | 100 | 100 | 19.0 |
| BSA (m2) | 142/2.70 | 135/1.27 | 1.75 | 1.73 | 0.20 |
| HR (#/min) | 367/139 | 170/45 | 72.1 | 70.0 | 12.8 |
| CO (L/min) | 142/11.11 | 367/4.18 | 6.32 | 6.10 | 1.06 |
| CM (c.c.) | 89/75.0 | 268/17.0 | 36.7 | 34.5 | 11.5 |
| DTT (s) | 95/5.13 | 360/2.00 | 3.08 | 3.00 | 0.53 |
| CT number of LA/400 | 270/2.17 | 170/0.61 | 1.13 | 1.11 | 0.20 |
| Risk Factor | Normalized Range | Normalized Data Parameters | |||
|---|---|---|---|---|---|
| Case No./Max. | Case No./Min. | Mean | Median | St. Dev | |
| Age (yr) | 162/+1 | 383/−1 | −0.02 | 0.03 | 0.40 |
| Tube voltage (kVp) | 142/+1 | 151/−1 | −0.13 | −0.14 | 0.56 |
| BSA (m2) | 142/+1 | 135/−1 | −0.33 | −0.36 | 0.28 |
| HR (#/min) | 367/+1 | 170/−1 | −0.42 | −0.47 | 0.27 |
| CO (L/min) | 142/+1 | 367/−1 | −0.38 | −0.45 | 0.31 |
| CM (c.c.) | 89/+1 | 268/−1 | −0.32 | −0.40 | 0.40 |
| DTT (s) | 95/+1 | 360/−1 | −0.31 | −0.36 | 0.34 |
| CT number of LA/400 | 270/+1 | 170/−1 | −0.335 | −0.357 | 1.524 |
| Biological Index | Factor | Coefficient | After Normalization | |
|---|---|---|---|---|
| Value | Rank | |||
| AGE | A | a1 | 0.165404 | 24 |
| Tube voltage | B | a2 | −0.626781 | 7 |
| BSA | C | a3 | −0.438880 | 10 |
| HR | D | a4 | −0.181944 | 23 |
| CO | E | a5 | 0.231918 | 21 |
| CM | F | a6 | 0.348170 | 17 |
| DTT | G | a7 | −0.377270 | 14 |
| Age × Tube voltage | A × B | a8 | −0.578918 | 9 |
| Age × BSA | A × C | a9 | 0.131548 | 25 |
| Age × HR | A × D | a10 | 0.255888 | 19 |
| Age × CO | A × E | a11 | −0.035711 | 29 |
| Age × CM | A × F | a12 | 0.255385 | 20 |
| Age × DT | A × G | a13 | −0.358334 | 16 |
| Tube voltage × BSA | B × C | a14 | 1.366192 | 2 |
| Tube voltage × HR | B × D | a15 | 0.127896 | 26 |
| Tube voltage × CO | B × E | a116 | −1.453575 | 1 |
| Tube voltage × CM | B × F | a17 | −0.291472 | 18 |
| Tube voltage × DTT | B × G | a18 | 0.198130 | 22 |
| BSA × HR | C × D | a19 | 0.372922 | 15 |
| BSA × CO | C × E | a20 | 0.437779 | 11 |
| BSA × CM | C × F | a21 | −0.661009 | 6 |
| BSA × DTT | C × G | a22 | 0.734438 | 4 |
| HR × CO | D × E | a23 | 0.068061 | 28 |
| HR × CM | D × F | a24 | −0.678175 | 5 |
| HR × DTT | D × G | a25 | 0.109320 | 27 |
| CO × CM | E × F | a26 | 0.417461 | 13 |
| CO × DTT | E × G | a27 | −0.803023 | 3 |
| CM × DTT | F × G | a28 | −0.590657 | 8 |
| Constant | a29 | −0.419399 | 29 | |
| Factor | Range | Derived Data | |||
|---|---|---|---|---|---|
| Case No./Max. | Case No./Min. | Mean | Median | St. Dev | |
| Age (yr) | 9/88 | 34/31 | 55.0 | 55.0 | 13.9 |
| Tube voltage (kVp) | 3/120 | 71/100 | 118.4 | 120.0 | 5.5 |
| BSA (m2) | 68/2.39 | 25/1.25 | 1.81 | 1.81 | 0.19 |
| HR (#/min) | 85/103 | 36/45 | 72.3 | 70.0 | 12.2 |
| CO (L/min) | 68/9.6 | 25/4.5 | 6.45 | 6.42 | 0.77 |
| CM (c.c.) | 19/68 | 30/32 | 54.4 | 56.6 | 8.9 |
| DTT (s) | 81/4.61 | 102/2.37 | 3.86 | 3.88 | 0.32 |
| CT number of LA/400 | 25/1.58 | 44/0.88 | 1.12 | 1.11 | 0.14 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, C.-S.; Peng, B.-R.; Ma, H.-B.; Chen, K.-L.; Lin, T.-H.; Pan, L.-K.; Lin, Y.-H. Inverse Problem Algorithm-Based Time-Resolved Imaging of Head and Neck Computed Tomography Angiography Contrast Kinetics with Clinical Testification. Diagnostics 2023, 13, 3354. https://doi.org/10.3390/diagnostics13213354
Lin C-S, Peng B-R, Ma H-B, Chen K-L, Lin T-H, Pan L-K, Lin Y-H. Inverse Problem Algorithm-Based Time-Resolved Imaging of Head and Neck Computed Tomography Angiography Contrast Kinetics with Clinical Testification. Diagnostics. 2023; 13(21):3354. https://doi.org/10.3390/diagnostics13213354
Chicago/Turabian StyleLin, Chih-Sheng, Bing-Ru Peng, Hong-Bing Ma, Ke-Lin Chen, Tsung-Han Lin, Lung-Kwang Pan, and Ya-Hui Lin. 2023. "Inverse Problem Algorithm-Based Time-Resolved Imaging of Head and Neck Computed Tomography Angiography Contrast Kinetics with Clinical Testification" Diagnostics 13, no. 21: 3354. https://doi.org/10.3390/diagnostics13213354
APA StyleLin, C.-S., Peng, B.-R., Ma, H.-B., Chen, K.-L., Lin, T.-H., Pan, L.-K., & Lin, Y.-H. (2023). Inverse Problem Algorithm-Based Time-Resolved Imaging of Head and Neck Computed Tomography Angiography Contrast Kinetics with Clinical Testification. Diagnostics, 13(21), 3354. https://doi.org/10.3390/diagnostics13213354